Clinical Characteristics and Outcomes of S. Aureus Bacteremia in Patients Receiving Total Parenteral Nutrition

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
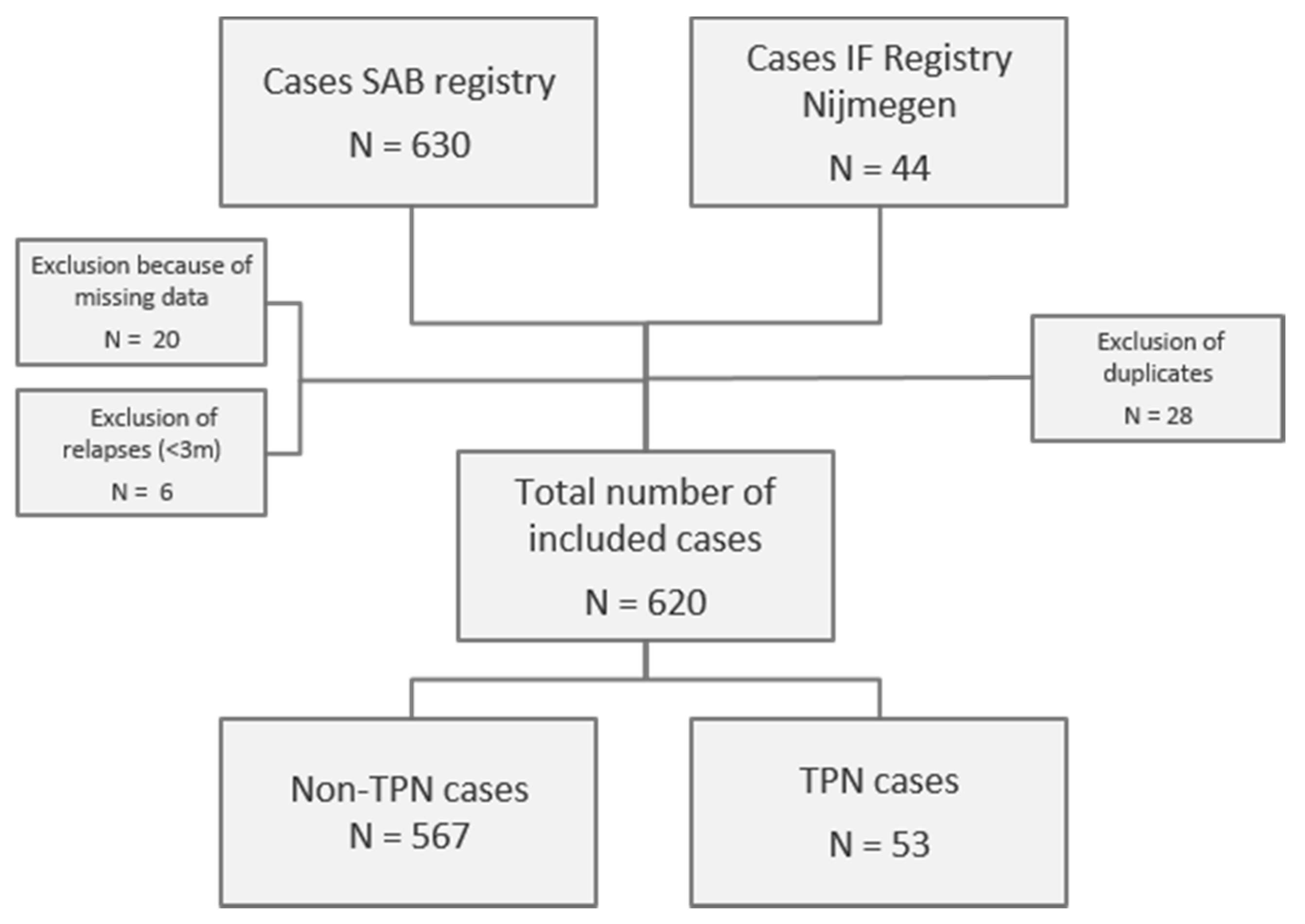
2.1. Study Design and Setting
2.2. Data Collection
2.3. Ethical Consideration
2.4. Management of Central Line Sepsis and S. aureus Bacteremia in Patients with TPN Support
2.5. Outcomes and Definitions
2.6. Statistical Methods
3. Results
3.1. Comparison of Patient Characteristics
3.2. Clinical Characteristics of S. aureus Bacteremia
3.3. Antibiotic Treatment
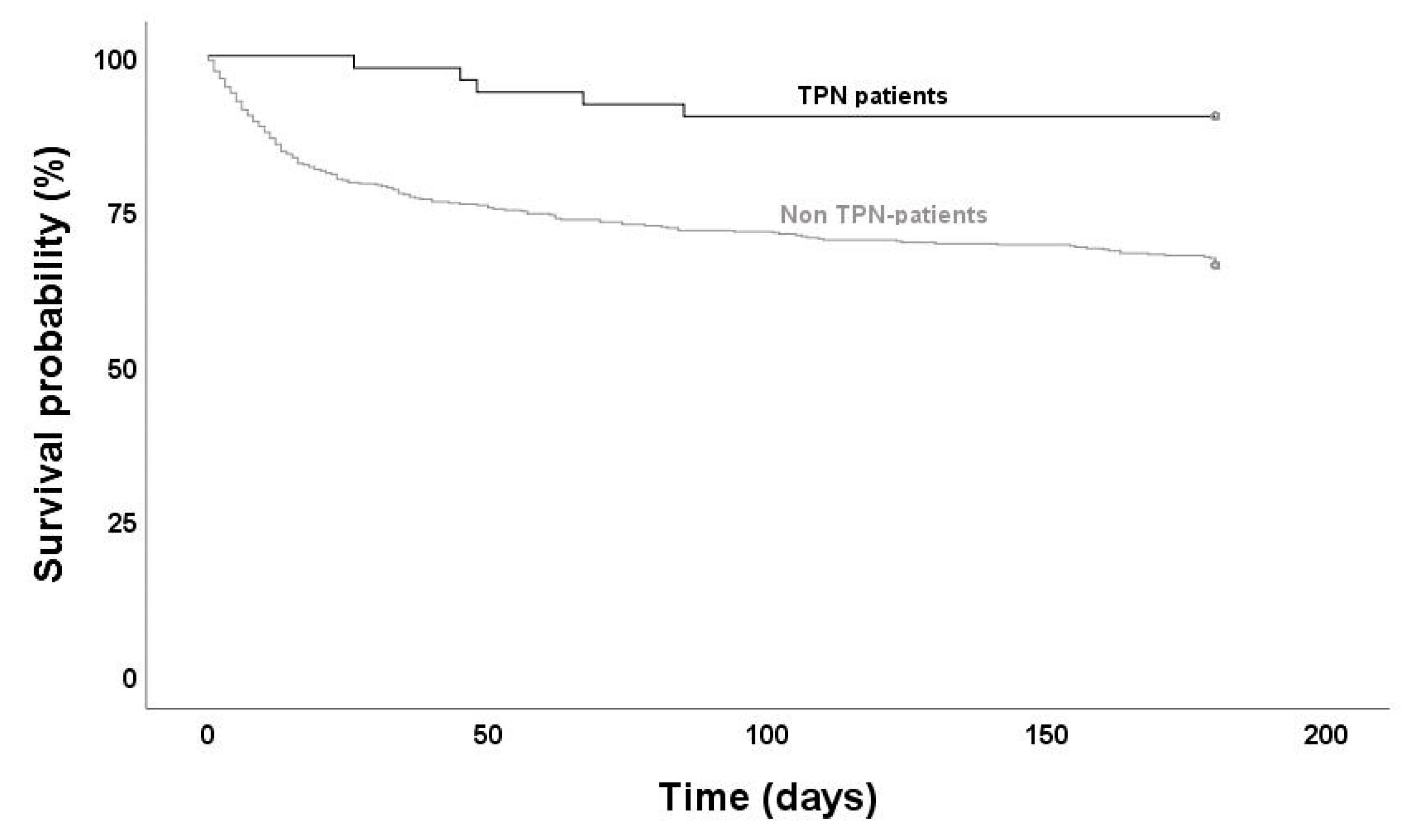
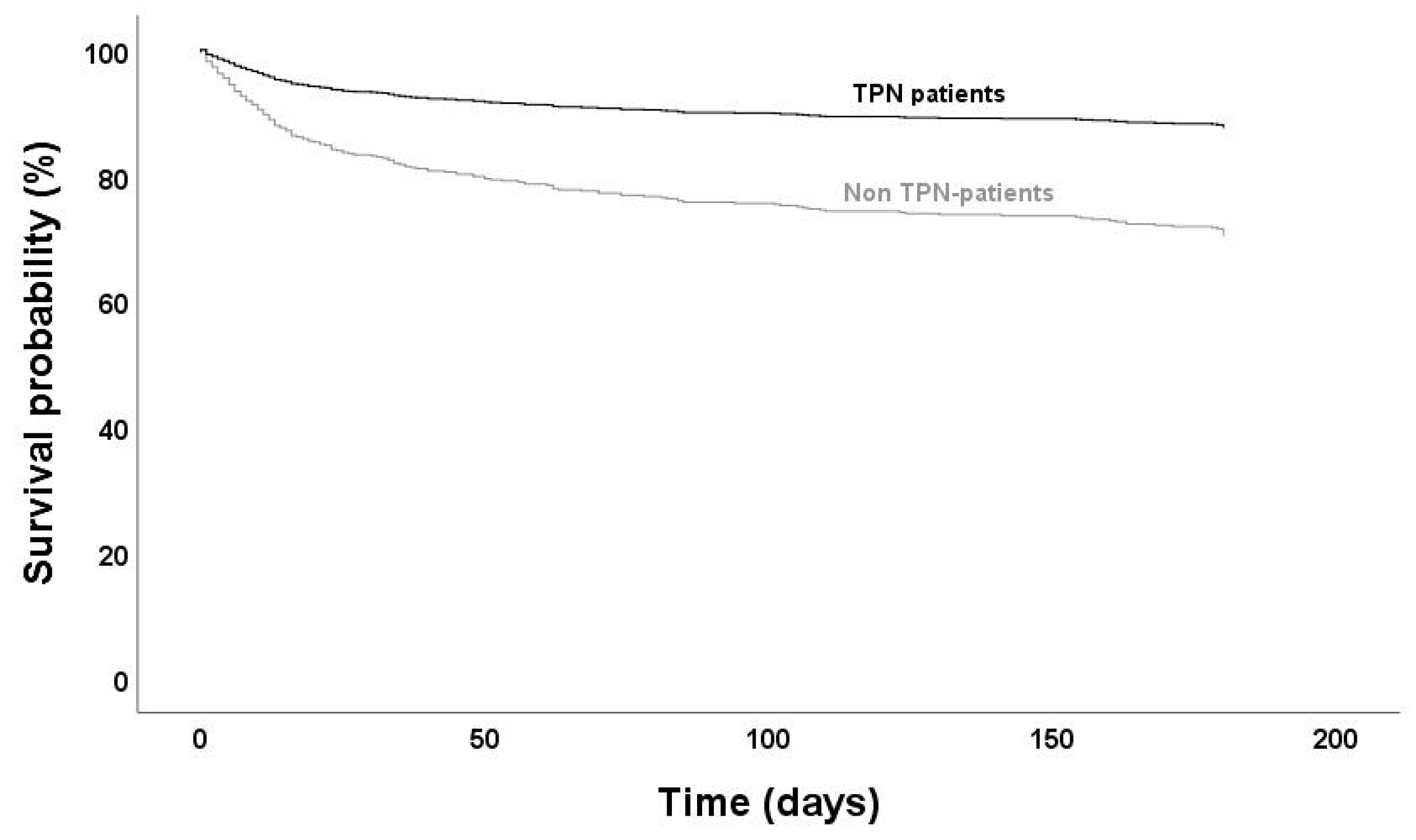
3.4. Mortality and Multivariate Survival Analyses
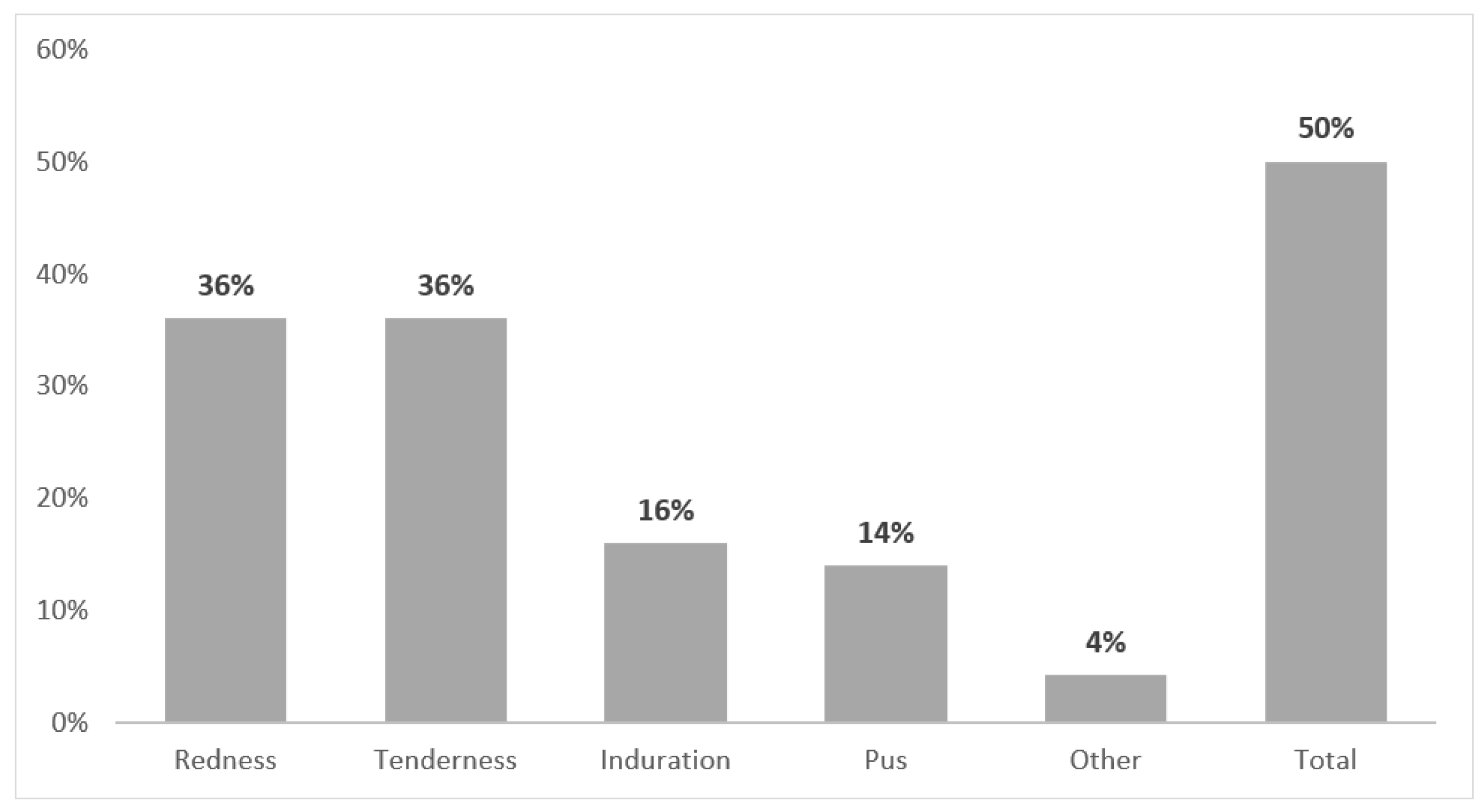
3.5. Clinical Characteristics of Complicated SAB in Patients Receiving TPN
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A: Clinical Characteristics and Outcomes of S. aureus Bacteremia in Patients Receiving Total Parenteral Nutrition

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Central Line Associated Blood Stream Infection (CLABSI) | According to the Centers for Disease control and Prevention (CDC) [29] |
| Community acquisition of SAB | SAB cases were community-acquired in all cases that did not meet the definition of healthcare associated SAB or hospital acquired SAB, thus infection in a patient who has had no contact with the health care system within the last 90 days. |
| Complicated SAB | Presence of any of the following [14]: - infective endocarditis; - metastatic infection; - non-retainable infected foreign body material; - relapse <3 months |
| Contamination | Contamination was defined as only one positive blood culture and no clinical signs of infection. |
| Exit site infection | An exit site infection is defined as an infection at the catheter exit site, with local erythema, induration and/or tenderness around the catheter exit site, and/or purulent discharge from the catheter exit site. When an exit site culture was performed and it was positive for S. aureus, it was labeled ‘definite’. Without an exit site culture, it was labeled ‘probable’ [22] |
| Healthcare associated SAB | SAB cases were healthcare-associated when patients were receiving home and/or ambulatory intravenous therapy, chemotherapy, hemodialysis, when patients were admitted in a hospital for at least 48 h within the last 90 days; and patients residing in a nursing home or long-term care facility [30]. |
| Hospital acquired SAB | SAB cases were labeled hospital-acquired if patients had been admitted for at least 48 h before the first positive blood culture. |
| Onset of SAB | The first positive blood culture was defined as the onset of SAB. |
| Portal of entry for SAB | The site that was most likely responsible for entry of S. aureus into the bloodstream, based on clinical signs, microbiological cultures and imaging results. |
| Staphylococcus aureus bacteremia (SAB) | At least one positive blood culture for Staphylococcus aureus combined with clinical signs of infection. |
| Time of delay between onset of SAB and adequate treatment | The onset of clinical symptoms (fever, chills) was used to define the time of delay between onset of SAB and starting of adequate treatment. |
References
- Howard, L.; Ashley, C. Management of complications in patients receiving home parenteral nutrition. Gastroenterology 2003, 124, 1651–1661. [Google Scholar] [CrossRef]
- O’Keefe, S.J.; Burnes, J.U.; Thompson, R.L. Recurrent sepsis in home parenteral nutrition patients: An analysis of risk factors. JPEN J. Parenter Enter. Nutr. 1994, 18, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Mariani, L.; Bertinet, D.B.; Chiavenna, G.; Crose, N.; De Cicco, M.; Gigli, G.; Micklewright, A.; Moreno Villares, J.M.; Orban, A.; et al. Central venous catheter complications in 447 patients on home parenteral nutrition: An analysis of over 100.000 catheter days. Clin. Nutr. 2002, 21, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Reitzel, R.A.; Rosenblatt, J.; Chaftari, A.M.; Raad, I.I. Epidemiology of infectious and noninfectious catheter complications in patients receiving home parenteral nutrition: A systematic review and meta-analysis. JPEN J. Parenter Enter. Nutr. 2019, 43, 832–851. [Google Scholar] [CrossRef] [PubMed]
- Wanten, G.; Calder, P.C.; Forbes, A. Managing adult patients who need home parenteral nutrition. BMJ 2011, 342, d1447. [Google Scholar] [CrossRef] [PubMed]
- Dreesen, M.; Foulon, V.; Spriet, I.; Goossens, G.A.; Hiele, M.; De Pourcq, L.; Willems, L. Epidemiology of catheter-related infections in adult patients receiving home parenteral nutrition: A systematic review. Clin. Nutr. 2013, 32, 16–26. [Google Scholar] [CrossRef]
- Gillanders, L.; Angstmann, K.; Ball, P.; O’Callaghan, M.; Thomson, A.; Wong, T.; Thomas, M. A prospective study of catheter-related complications in HPN patients. Clin. Nutr. 2012, 31, 30–34. [Google Scholar] [CrossRef]
- Ross, V.M.; Guenter, P.; Corrigan, M.L.; Kovacevich, D.; Winkler, M.F.; Resnick, H.E.; Norris, T.L.; Robinson, L.; Steiger, E. Central venous catheter infections in home parenteral nutrition patients: Outcomes from Sustain: American society for parenteral and enteral nutrition’s national patient registry for nutrition care. Am. J. Infect. Control 2016, 44, 1462–1468. [Google Scholar] [CrossRef]
- Santarpia, L.; Buonomo, A.; Pagano, M.C.; Alfonsi, L.; Foggia, M.; Mottola, M.; Marinosci, G.Z.; Contaldo, F.; Pasanisi, F. Central venous catheter related bloodstream infections in adult patients on home parenteral nutrition: Prevalence, predictive factors, therapeutic outcome. Clin. Nutr. 2016, 35, 1394–1398. [Google Scholar] [CrossRef]
- Lowy, F.D. Staphylococcus aureus infections. N. Engl. J. Med. 1998, 339, 520–532. [Google Scholar] [CrossRef]
- Cosgrove, S.E.; Sakoulas, G.; Perencevich, E.N.; Schwaber, M.J.; Karchmer, A.W.; Carmeli, Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: A meta-analysis. Clin. Infect. Dis. 2003, 36, 53–59. [Google Scholar] [CrossRef]
- Kaasch, A.J.; Barlow, G.; Edgeworth, J.D.; Fowler, V.G., Jr.; Hellmich, M.; Hopkins, S.; Kern, W.V.; Llewelyn, M.J.; Rieg, S.; Rodriguez-Baño, J.; et al. Staphylococcus aureus bloodstream infection: A pooled analysis of five prospective, observational studies. J. Infect. 2014, 68, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Kern, W.V. Management of Staphylococcus aureus bacteremia and endocarditis: Progresses and challenges. Curr. Opin. Infect. Dis. 2010, 23, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G., Jr.; Olsen, M.K.; Corey, G.R.; Woods, C.W.; Cabell, C.H.; Reller, L.B.; Cheng, A.C.; Dudley, T.; Oddone, E.Z. Clinical identifiers of complicated Staphylococcus aureus bacteremia. Arch. Int. Med. 2003, 163, 2066–2072. [Google Scholar] [CrossRef]
- Yilmaz, M.; Elaldi, N.; Balkan, İ.İ.; Arslan, F.; Batırel, A.A.; Bakıcı, M.Z.; Gozel, M.G.; Alkan, S.; Çelik, A.D.; Yetkin, M.A.; et al. Mortality predictors of Staphylococcus aureus bacteremia: A prospective multicenter study. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- El Zakhem, A.; Chaftari, A.M.; Bahu, R.; El Helou, G.; Shelburne, S.; Jiang, Y.; Hachem, R.; Raad, I. Central line-associated bloodstream infections caused by Staphylococcus aureus in cancer patients: Clinical outcome and management. Ann. Med. 2014, 46, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.Y.; MacDonald, B.B.; Peacock, J.E., Jr.; Musher, D.M.; Triplett, P.; Mylotte, J.M.; O’Donnell, A.; Wagener, M.M.; Yu, V.L. A prospective multicenter study of Staphylococcus aureus bacteremia: Incidence of endocarditis, risk factors for mortality, and clinical impact of methicillin resistance. Medicine 2003, 82, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Dibb, M.J.; Abraham, A.; Chadwick, P.R.; Shaffer, J.L.; Teubner, A.; Carlson, G.L.; Lal, S. Central venous catheter salvage in home parenteral nutrition catheter-related bloodstream infections: Long-term safety and efficacy data. JPEN J. Parenter Enter. Nutr. 2016, 40, 699–704. [Google Scholar] [CrossRef]
- Fowler, V.G., Jr.; Justice, A.; Moore, C.; Benjamin, D.K., Jr.; Woods, C.W.; Campbell, S.; Reller, L.B.; Corey, G.R.; Day, N.P.; Peacock, S.J. Risk factors for hematogenous complications of intravascular catheter-associated Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2005, 40, 695–703. [Google Scholar] [CrossRef]
- Nambiar, K.; Seifert, H.; Rieg, S.; Kern, W.V.; Scarborough, M.; Gordon, N.C.; Kim, H.B.; Song, K.H.; Tilley, R.; Gott, H.; et al. Survival following Staphylococcus aureus bloodstream infection: A prospective multinational cohort study assessing the impact of place of care. J. Infect. 2018, 77, 516–525. [Google Scholar] [CrossRef]
- Chu, V.H.; Crosslin, D.R.; Friedman, J.Y.; Reed, S.D.; Cabell, C.H.; Griffiths, R.I.; Masselink, L.E.; Kaye, K.S.; Corey, G.R.; Reller, L.B.; et al. Staphylococcus aureus bacteremia in patients with prosthetic devices: Costs and outcomes. Am. J. Med. 2005, 118, 1416. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Farr, B.M.; Sherertz, R.J.; Raad, I.I.; O’Grady, N.; Harris, J.S.; Craven, D.E. Guidelines for the management of intravascular catheter-related infections. Clin. Infect. Dis. 2001, 24, 180–205. [Google Scholar]
- Mylotte, J.M.; Tayara, A. Staphylococcus aureus bacteremia: Predictors of 30-day mortality in a large cohort. Clin. Infect. Dis. 2000, 31, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Wouters, Y.; Vissers, R.K.; Groenewoud, H.; Kievit, W.; Wanten, G.J.A. Repair of damaged central venous catheters is safe and doubles catheter survival: A home parenteral nutrition patient cohort study. Clin. Nutr. 2019, 38, 1692–1699. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Berrevoets, M.A.H.; Kouijzer, I.J.E.; Aarntzen, E.H.J.G.; Janssen, M.; De Geus-Oei, L.F.; Wertheim, H.; Kullberg, B.J.; Oever, J.T.; Oyen, W.; Bleeker-Rovers, C.P. 18F-FDG PET/CT optimizes treatment in Staphylococcus aureus bacteremia and is associated with reduced mortality. J. Nucl. Med. 2017, 58, 1504–1510. [Google Scholar] [CrossRef]
- Pironi, L.; Boeykens, K.; Bozzetti, F.; Joly, F.; Klek, S.; Lal, S.; Lichota, M.; Mühlebach, S.; Van Gossum, A.; Wanten, G.; et al. ESPEN guideline on home parenteral nutrition. Clin. Nutr. 2020, 39, 1645–1666. [Google Scholar] [CrossRef] [PubMed]
- Olthof, E.D.; Versleijen, M.W.; Huisman-de Waal, G.; Feuth, T.; Kievit, W.; Wanten, G.J. Taurolidine lock is superior to heparin lock in the prevention of catheter related bloodstream infections and occlusions. PLoS ONE. 2014, 7, e111216. [Google Scholar] [CrossRef]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Infectious diseases society of america. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 1, e18–e55. [Google Scholar] [CrossRef]
- Durack, D.T.; Lukes, A.S.; Bright, D.K. New criteria for diagnosis of infective endocarditis: Utilization of specific echocardiographic findings. Duke Endocarditis Service. Am. J. Med. 1994, 96, 200–209. [Google Scholar] [CrossRef]
- Dutch Working Party on Antibiotic Policy (SWAB). Guidelines for Antibacterial Therapy of Adult Patients with Sepsis. Available online: https://swab.nl/en/sepsis-general-information (accessed on 13 October 2020).
- O’Grady, N.P.; Alexander, M.; Dellinger, E.P.; Gerberding, J.L.; Heard, S.O.; Maki, D.G.; Masur, H.; McCormick, R.D.; Mermel, L.A.; Pearson, M.L.; et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm. Rep. 2002, 51, 1–29. [Google Scholar] [PubMed]
- Bishara, J.; Goldberg, E.; Leibovici, L.; Samra, Z.; Shaked, H.; Mansur, N.; Paul, M. Healthcare-associated vs. hospital-acquired Staphylococcus aureus bacteremia. Int. J. Infect. Dis. 2012, 16, e457–e463. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, A.M.; Rosdahl, V.T.; Espersen, F.; Frimodt-Møller, N.; Skinhøj, P.; Bentzon, M.W. Catheter-related Staphylococcus aureus infections. J. Hosp. Infect. 1993, 23, 123–131. [Google Scholar] [CrossRef]
- van Hal, S.J.; Jensen, S.O.; Vaska, V.L.; Espedido, B.A.; Paterson, D.L.; Gosbell, I.B. Predictors of mortality in Staphylococcus aureus Bacteremia. Clin. Microbiol. Rev. 2012, 25, 362–386. [Google Scholar] [CrossRef]
- Ghanem, G.A.; Boktour, M.; Warneke, C.; Pham-Williams, T.; Kassis, C.; Bahna, P.; Aboufaycal, H.; Hachem, R.; Raad, I. Catheter-related Staphylococcus aureus bacteremia in cancer patients: High rate of complications with therapeutic implications. Medicine 2007, 86, 54–60. [Google Scholar] [CrossRef]
- Engemann, J.J.; Friedman, J.Y.; Reed, S.D.; Griffiths, R.I.; Szczech, L.A.; Kaye, K.S.; Stryjewski, M.E.; Reller, L.B.; Schulman, K.A.; Corey, G.R.; et al. Clinical outcomes and costs due to Staphylococcus aureus bacteremia among patients receiving long-term hemodialysis. Infect. Control Hosp. Epidemiol. 2005, 26, 534–539. [Google Scholar] [CrossRef]
- Fitzgerald, S.F.; O’Gorman, J.; Morris-Downes, M.M.; Crowley, R.K.; Donlon, S.; Bajwa, R.; Smyth, E.G.; Fitzpatrick, F.; Conlon, P.J.; Humphreys, H. A 12-year review of Staphylococcus aureus bloodstream infections in haemodialysis patients: More work to be done. J. Hosp. Infect. 2011, 79, 218–221. [Google Scholar] [CrossRef]
- Blot, S.I.; Vandewoude, K.H.; Hoste, E.A.; Colardyn, F.A. Outcome and attributable mortality in critically Ill patients with bacteremia involving methicillin-susceptible and methicillin-resistant Staphylococcus aureus. Arch. Intern. Med. 2002, 162, 2229–2235. [Google Scholar] [CrossRef]
- Tong, S.Y.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G., Jr. Staphylococcus aureus infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 2015, 28, 603–661. [Google Scholar] [CrossRef]
- Krishnan, A.; Irani, K.; Swaminathan, R.; Boan, P. A retrospective study of tunnelled haemodialysis central line-associated bloodstream infections. J. Chemother. 2019, 31, 132–136. [Google Scholar] [CrossRef]
- Chaudry, M.S.; Gislason, G.H.; Kamper, A.L.; Rix, M.; Dahl, A.; Østergaard, L.; Fosbøl, E.L.; Lauridsen, T.K.; Oestergaard, L.B.; Hassager, C.; et al. The impact of hemodialysis on mortality risk and cause of death in Staphylococcus aureus endocarditis. BMC Nephrol. 2018, 19, 216. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G., Jr.; Sanders, L.L.; Sexton, D.J.; Kong, L.; Marr, K.A.; Gopal, A.K.; Gottlieb, G.; McClelland, R.S.; Corey, G.R. Outcome of Staphylococcus aureus bacteremia according to compliance with recommendations of infectious diseases specialists: Experience with 244 patients. Clin. Infect. Dis. 1998, 27, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Libman, H.; Arbeit, R.D. Complications associated with Staphylococcus aureus bacteremia. Arch. Intern. Med. 1984, 144, 541–545. [Google Scholar] [CrossRef]
- Vos, F.J.; Bleeker-Rovers, C.P.; Sturm, P.D.; Krabbe, P.F.; van Dijk, A.P.; Cuijpers, M.L.; Adang, E.M.; Wanten, G.J.; Kullberg, B.J.; Oyen, W.J. 18F-FDG PET/CT for detection of metastatic infection in gram-positive bacteremia. J. Nucl. Med. 2010, 51, 1234–1240. [Google Scholar] [CrossRef] [PubMed]
- Horino, T.; Sato, F.; Hosaka, Y.; Hoshina, T.; Tamura, K.; Nakaharai, K.; Kato, T.; Nakazawa, Y.; Yoshida, M.; Hori, S. Predictive factors for metastatic infection in patients with bacteremia caused by methicillin-sensitive Staphylococcus aureus. Am. J. Med. Sci. 2015, 349, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Dugdale, D.C.; Ramsey, P.G. Staphylococcus aureus bacteremia in patients with Hickman catheters. Am. J. Med. 1990, 89, 137–141. [Google Scholar] [CrossRef]
- Malanoski, G.J.; Samore, M.H.; Pefanis, A.; Karchmer, A.W. Staphylococcus aureus catheter-associated bacteremia. Minimal effective therapy and unusual infectious complications associated with arterial sheath catheters. Arch. Intern. Med. 1995, 155, 1161–1166. [Google Scholar] [CrossRef]
- Gold, H.S.; Karchmer, A.W. Catheter-associated Staphylococcus aureus bacteremia. Hosp. Pract. 1996, 31, 133–150. [Google Scholar] [CrossRef]




| Patient Characteristics | All Patients n = 604 | TPN Patients n = 41 | Non-TPN Patients n = 563 | p-Value |
|---|---|---|---|---|
| Age, mean (SD) | 62.5 (16.7) | 53.4 (16.0) | 63.2 (16.6) | <0.001 |
| Female (%) | 237 (39.2) | 28 (68.3) | 209 (37.1) | <0.001 |
| Presence of CVC (%) | 110 (18.2) | 41 (100) | 69 (12.2) | <0.001 |
| Foreign body (%) | 229 (37.9) | 8 (19.5) | 221 (39.3) | 0.012 |
| Joint prosthesis | 70 (11.6) | 1 (2.4) | 69 (12.3) | 0.073 * |
| Pacemaker/ICD | 47 (7.8) | 2 (4.9) | 45 (8.0) | 0.761 * |
| Prosthetic heart valve | 52 (8.6) | 2 (4.9) | 50 (8.9) | 0.565 * |
| Vascular prosthesis | 50 (8.3) | 4 (9.8) | 46 (8.2) | 0.766 * |
| Other 1 | 54 (8.9) | 3 (7.3) | 51 (9.1) | 1.00 |
| Charlson comorbidity index, mean (SD) | 3.52 (2.33) | 1.90 (1.88) | 3.64 (2.32) | <0.001 |
| Immunocompromised 2 (%) | 139 (23.3) | 9 (22.0) | 130 (23.4) | 0.834 |
| Risk factors for endocarditis 3 (%) | 63 (10.4) | 3 (7.3) | 60 (10.7) | 0.790 * |
| Allergy to antibiotics (%) | 78 (12.9) | 10 (24.4) | 68 (12.1) | 0.024 |
| Clinical Characteristics | All Cases n = 620 | TPN Cases n = 53 | Non-TPN Cases n = 567 | p-Value |
|---|---|---|---|---|
| MRSA (%) | 13 (2.1) | 1 (1.9) | 12 (2.1) | 1.00 * |
| Mode of acquisition (%) | ||||
| Community acquired | 206 (33.2) | 0 | 206 (36.3) | <0.001 |
| Healthcare associated | 195 (31.5) | 44 (83) | 151 (26.6) | |
| Hospital acquired | 219 (35.3) | 9 (17) | 210 (37) | |
| Portal of entry (%) | <0.001 | |||
| Skin | 194 (31.6) | 3 (5.7) | 191 (34) | |
| Central venous line | 103 (16.8) | 48 (90.6) | 55 (9.8) | |
| Peripheral venous line | 97 (15.8) | 1 (1.9) | 96 (17.1) | |
| Lungs | 14 (2.3) | 0 | 14 (2.5) | |
| Other 1 | 36 (5.9) | 0 | 36 (6.4) | |
| Unknown | 170 (27.7) | 1 (1.9) | 169 (30.1) | |
| Fever at onset (%) | 490 (84.6) | 41 (83.7) | 449 (84.7) | 0.83 |
| Persistent fever >72 h treatment (%) | 180 (31.9) | 7 (17.5) | 173 (33) | 0.04 |
| Follow-up blood cultures performed (%) | 552 (90.8) | 45 (95.7) | 507 (90.4) | 0.22 |
| Positive at 48 h | 152 (24.5) | 13 (24.5) | 139 (24.5) | 1.00 |
| CRP at onset mg/l, mean (SD) | 161 (127) | 74.6 (67.9) | 169 (128) | <0.001 |
| Creatinine at onset umol/l, mean (SD) | 121 (104) | 113 (66.4) | 121 (107) | 0.58 |
| 18FDG-PET/CT scan performed (%) | 334 (55) | 37 (72.5) | 297 (52.8) | <0.01 |
| Metastatic infection | 233 (70.6) | 20 (54.1) | 213 (72.7) | 0.02 |
| Spondylodiscitis | 50 (8.1) | 1 (1.9) | 49 (8.6) | 0.11 |
| Endocarditis | 34 (5.5) | 1 (1.9) | 33 (5.8) | 0.35 |
| Skin/soft tissue | 85 (13.7) | 3 (5.7) | 82 (14.5) | 0.09 |
| Spleen | 3 (0.5) | 0 | 3 (0.5) | 1.00 * |
| Liver/bile system | 4 (0.6) | 0 | 4 (0.7) | 1.00 * |
| Psoas muscle | 18 (2.9) | 1 (1.9) | 17 (3) | 1.00 * |
| Non-vertebral osteomyelitis | 21 (3.4) | 1 (1.9) | 20 (3.5) | 1.00 * |
| Arthritis | 56 (9) | 3 (5.7) | 53 (9.3) | 0.46 * |
| Brain | 4 (0.6) | 0 | 4 (0.7) | 1.00 * |
| Endovascular | 54 (8.7) | 10 (18.9) | 44 (7.8) | <0.01 |
| Lung | 61 (9.8) | 15 (28.3) | 46 (8.1) | <0.001 |
| Other | 64 (10.3) | 0 | 64 (11.3) | <0.01 * |
| Endocarditis 2 (%) | 63 (10.2) | 2 (3.8) | 61 (10.8) | 0.15 * |
| ID bedside consultation (%) | 473 (78.7) | 37 (88.1) | 436 (78) | 0.12 |
| Onset treatment # (%) | 0.98 | |||
| <24 h | 284 (49) | 26 (51) | 258 (48.8) | |
| 24–48 h | 88 (15.2) | 7 (13.7) | 81 (15.3) | |
| 48 h–72 h | 63 (10.9) | 5 (9.8) | 58 (11) | |
| >72 h | 145 (25) | 13 (25.5) | 132 (25) | |
| Antibiotic therapy (%) | 0.13 | |||
| Flucloxacillin | 523 (85.5) | 43 (84.3) | 480 (85.6) | |
| Cefazolin | 32 (5.2) | 3 (5.9) | 29 (5.2) | |
| Vancomycin/teicoplanin | 19 (3.1) | 4 (7.8) | 15 (2.7) | |
| Other | 38 (6.2) | 1 (2.0) | 37 (6.6) | |
| Duration of therapy (%) ## | 0.04 | |||
| <2 weeks | 40 (6.5) | 2 (3.8) | 38 (6.7) | |
| 2–4 weeks | 192 (31.2) | 22 (41.5) | 170 (30.2) | |
| 4–6 weeks | 71 (11.5) | 5 (9.4) | 66 (11.7) | |
| >6 weeks | 179 (29.1) | 16 (30.2) | 163 (29) | |
| Died during therapy | 115 (18.7) | 4 (7.5) | 111 (19.7) | |
| Switch to oral therapy (%) | 191 (32.4) | 5 (10.4) | 186 (34.4) | <0.001 * |
| Intensive care admission (%) | 173 (28.1) | 12 (23.1) | 161 (28.6) | 0.40 |
| Duration hospital admission, mean (SD) ### | 21.3 (20.7) | 26 23) | 20.8 (20.5) | 0.05 |
| All Cases n = 620 | TPN Cases n = 53 | Non-TPN Cases n = 551 | p-Value | Missing Values TPN/Non-TPN | |
|---|---|---|---|---|---|
| In-hospital death | 103 (17.1) | 2 (3.8) | 101 (18.3) | 0.004 | 0/16 |
| 1 month | |||||
| Death | 111 (18.4) | 1 (1.9) | 110 (20) | <0.001 | 0/16 |
| 3 months | |||||
| Death | 152 (25.2) | 5 (9.4) | 147 (26.7) | 0.004 | 0/16 |
| Relapse | 9 (1.5) | 2 (3.8) | 7 (1.3) | 0.18 | 0/16 |
| Overall mortality a | 181 (31.8) | 5 (9.8) | 176 (34) | <0.001 | 2/49 |
| SAB attributable mortality | 93 (15) | 1 (1.9) | 92 (17) | 0.002 | 2/36 |
| Complicated SAB b | 246 (39.7) | 22 (41.5) | 224 (39.5) | 0.78 | 0/0 |
| Univariate Analysis a | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Gender (ref.: female) | 1.06 | 0.78–1.43 | 0.71 | |||
| Charlson com. index (per point) | 1.28 | 1.19–1.37 | <0.001 | 1.32 | 1.24–1.4 | <0.001 |
| Immunocompromised (ref.: no) | 1.29 | 0.93–1.78 | 0.13 | |||
| Foreign body material (ref.: no) | 1.01 | 0.75–1.38 | 0.93 | |||
| Risk factors for endocarditis (ref.: no) | 1.63 | 1.08–2.45 | 0.02 | 1.74 | 1.15–2.62 | <0.01 |
| TPN support (ref.: no) | 0.25 | 0.10–0.60 | <0.01 | 0.38 | 0.16–0.93 | 0.03 |
| Total TPN Cases n = 53 (%) | Complicated SAB n = 22 (%) | Non-Complicated SAB n = 31 (%) | p-Value | Missing Values | |
|---|---|---|---|---|---|
| Healthcare-associated onset | 44 (83) | 21 (95) | 23 (74) | 0.04 | 0 |
| Fever at onset | 41 (77) | 17 (77) | 24 (77) | 0.27 * | 4 |
| Inflammation at CVC insertion | 25 (47) | 12 (55) | 13 (42) | 0.31 | 15 |
| Previous problems with CVC # | 12 (22) | 9 (41) | 3 (10) | 0.02 * | 15 |
| CRP, mean (SD) | 75 (68) | 99 (66) | 54 (64) | 0.02 | 5 |
| Therapy onset <24 h ## | 26 (49) | 4 (18) | 22 (71) | <0.001 * | 2 |
| CVC removed | 51 (96) | 21 (95) | 30 (97) | 0.24 | 1 |
| Persistent fever >72 h | 7 (13) | 4 (18) | 3 (10) | 0.69 * | 13 |
| Positive follow-up BC | 13 (25) | 10 (45) | 3 (10) | <0.01 * | 0 |
| SAB in medical history | 14 (26) | 5 (23) | 9 (29) | 0.51 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gompelman, M.; Tuinte, R.A.M.; Berrevoets, M.A.H.; Bleeker-Rovers, C.P.; Wanten, G.J.A. Clinical Characteristics and Outcomes of S. Aureus Bacteremia in Patients Receiving Total Parenteral Nutrition. Nutrients 2020, 12, 3131. https://doi.org/10.3390/nu12103131
Gompelman M, Tuinte RAM, Berrevoets MAH, Bleeker-Rovers CP, Wanten GJA. Clinical Characteristics and Outcomes of S. Aureus Bacteremia in Patients Receiving Total Parenteral Nutrition. Nutrients. 2020; 12(10):3131. https://doi.org/10.3390/nu12103131
Chicago/Turabian StyleGompelman, Michelle, Renée A. M. Tuinte, Marvin A. H. Berrevoets, Chantal P. Bleeker-Rovers, and Geert J. A. Wanten. 2020. "Clinical Characteristics and Outcomes of S. Aureus Bacteremia in Patients Receiving Total Parenteral Nutrition" Nutrients 12, no. 10: 3131. https://doi.org/10.3390/nu12103131
APA StyleGompelman, M., Tuinte, R. A. M., Berrevoets, M. A. H., Bleeker-Rovers, C. P., & Wanten, G. J. A. (2020). Clinical Characteristics and Outcomes of S. Aureus Bacteremia in Patients Receiving Total Parenteral Nutrition. Nutrients, 12(10), 3131. https://doi.org/10.3390/nu12103131