An Exploratory Analysis of Changes in Mental Wellbeing Following Curcumin and Fish Oil Supplementation in Middle-Aged and Older Adults



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Procedures
2.2.1. Mood States
2.2.2. Subjective Memory Complaints
2.2.3. General Health Perception (Quality of Life)
2.2.4. APOE4 Analysis
2.3. Investigational Product and Intervention
- FO group: active fish oil capsules (Blackmores Omega Brain™: 400 mg EPA and 2000 mg DHA/day) with placebo curcumin capsules (maltodextrin with yellow food colouring);
- CUR group: active curcumin capsules (Blackmores Brain Active™: 800 mg Longvida® containing 160 mg curcumin/day) with placebo fish oil capsules (mix of corn and olive oil with 20 mg of fish oil to match odour);
- FO + CUR group: active fish oil and active curcumin capsules;
- PL group: placebo fish oil and placebo curcumin capsules.
2.4. Statistical Analysis
- Fish oil (FO and FO + CUR group) vs. no fish oil (CUR and PL group);
- Curcumin (CUR and FO + CUR group) vs. no curcumin (FO and PL group).
3. Results
3.1. Participant Disposition and Baseline Characteristics
3.2. Effects of Treatment on Mental Wellbeing Measures
3.3. Effects of Treatment on Quality of Life
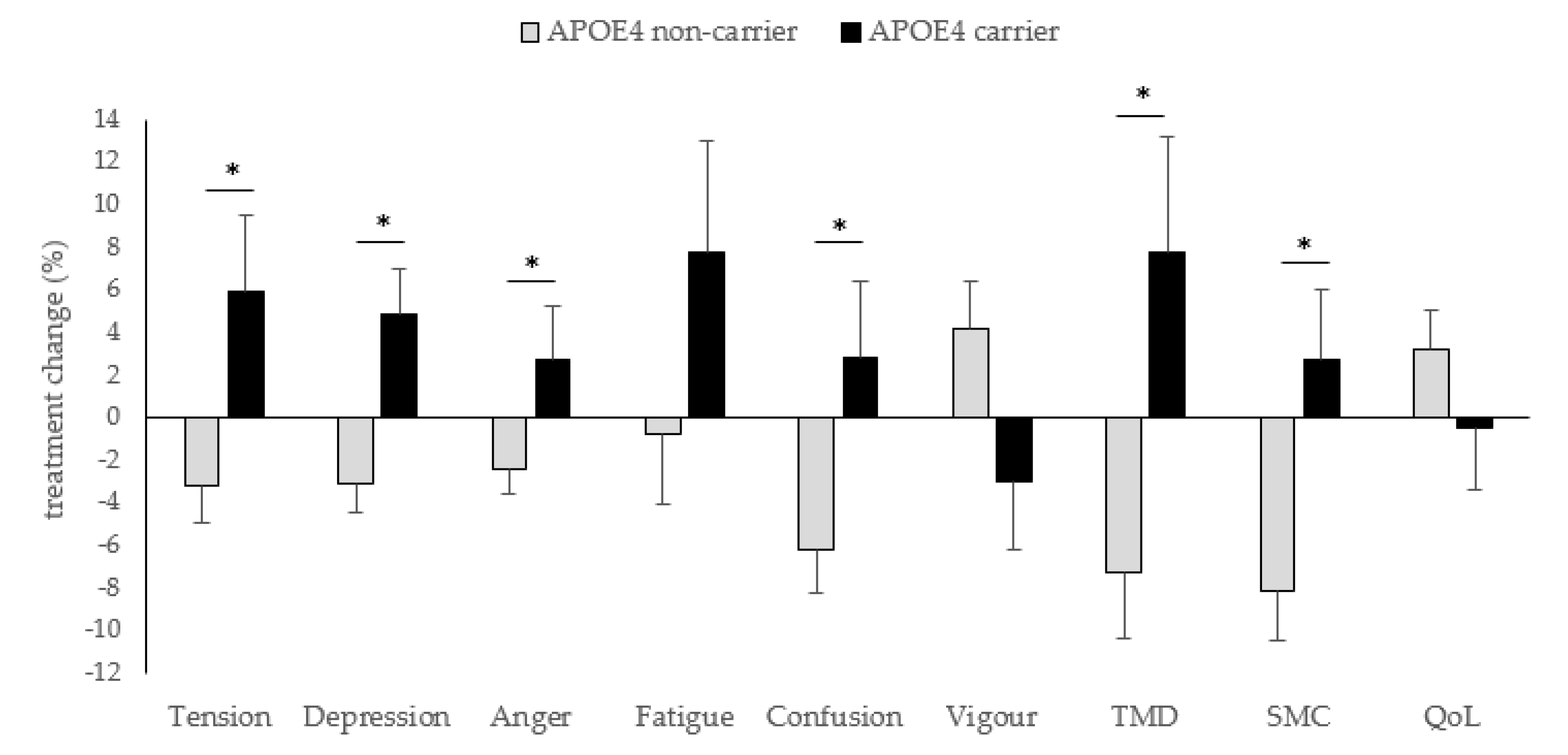
3.4. Influence of APOE4 Status
3.5. Subanalysis in APOE4 Non-Carriers
4. Discussion
4.1. Curcumin Supplementation
4.2. Effects of Fish oil Supplementation Influenced by APOE4 Status
4.3. Combination of Fish Oil and Curcumin
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Farioli-Vecchioli, S.; Sacchetti, S.; di Robilant, N.V.; Cutuli, D. The Role of Physical Exercise and Omega-3 Fatty Acids in Depressive Illness in the Elderly. Curr. Neuropharmacol. 2018, 16, 308–326. [Google Scholar] [CrossRef] [PubMed]
- Barua, A.; Ghosh, M.K.; Kar, N.; Basilio, M.A. Prevalence of depressive disorders in the elderly. Ann. Saudi Med. 2011, 31, 620–644. [Google Scholar] [CrossRef] [PubMed]
- Okereke, O.I.; Reynolds, C.F., 3rd; Mischoulon, D.; Chang, G.; Cook, N.R.; Copeland, T.; Friedenberg, G.; Buring, J.E.; Manson, J.E. The VITamin D and OmegA-3 TriaL-Depression Endpoint Prevention (VITAL-DEP): Rationale and design of a large-scale ancillary study evaluating vitamin D and marine omega-3 fatty acid supplements for prevention of late-life depression. Contemp. Clin. Trials 2018, 68, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Balash, Y.; Mordechovich, M.; Shabtai, H.; Giladi, N.; Gurevich, T.; Korczyn, A.D. Subjective memory complaints in elders: Depression, anxiety, or cognitive decline? Acta Neurol. Scand. 2013, 127, 344–350. [Google Scholar] [CrossRef]
- Glodzik-Sobanska, L.; Reisberg, B.; De Santi, S.; Babb, J.S.; Pirraglia, E.; Rich, K.E.; Brys, M.; de Leon, M.J. Subjective memory complaints: Presence, severity and future outcome in normal older subjects. Dement. Geriatr. Cogn. Disord. 2007, 24, 177–184. [Google Scholar] [CrossRef]
- Jessen, F.; Wiese, B.; Bachmann, C.; Eifflaender-Gorfer, S.; Haller, F.; Kölsch, H.; Luck, T.; Mösch, E.; van den Bussche, H.; Wagner, M.; et al. Prediction of dementia by subjective memory impairment: Effects of severity and temporal association with cognitive impairment. Arch. Gen. Psychiatry 2010, 67, 414–422. [Google Scholar] [CrossRef]
- Kaup, A.R.; Nettiksimmons, J.; LeBlanc, E.S.; Yaffe, K. Memory complaints and risk of cognitive impairment after nearly 2 decades among older women. Neurology 2015, 85, 1852–1858. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Vozza, L.; Gabbiadini, A.; Vanella, A.; Concas, I.; Tinacci, S.; Petralia, A.; Signorelli, M.S.; Aguglia, E. Curcumin for depression: A meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 60, 2643–2653. [Google Scholar] [CrossRef]
- Cox, K.H.; Pipingas, A.; Scholey, A.B. Investigation of the effects of solid lipid curcumin on cognition and mood in a healthy older population. J. Psychopharmacol. 2015, 29, 642–651. [Google Scholar] [CrossRef]
- Cox, K.H.M.; White, D.J.; Pipingas, A.; Poorun, K.; Scholey, A. Further Evidence of Benefits to Mood and Working Memory from Lipidated Curcumin in Healthy Older People: A 12-Week, Double-Blind, Placebo-Controlled, Partial Replication Study. Nutrients 2020, 12, 1678. [Google Scholar] [CrossRef]
- Abdolahi, M.; Sarraf, P.; Javanbakht, M.H.; Honarvar, N.M.; Hatami, M.; Soveyd, N.; Tafakhori, A.; Sedighiyan, M.; Djalali, M.; Jafarieh, A.; et al. A Novel Combination of ω-3 Fatty Acids and Nano-Curcumin Modulates Interleukin-6 Gene Expression and High Sensitivity C-reactive Protein Serum Levels in Patients with Migraine: A Randomized Clinical Trial Study. CNS Neurol. Disord. Drug Targets 2018, 17, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Larrieu, T.; Layé, S. Food for Mood: Relevance of Nutritional Omega-3 Fatty Acids for Depression and Anxiety. Front. Physiol. 2018, 9, 1047. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Kim, Y.; Je, Y. Fish consumption and risk of depression: Epidemiological evidence from prospective studies. Asia Pac. Psychiatry 2018, 10, e12335. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.H.; Kim, G. Systematic review and meta-analysis of omega-3-fatty acids in elderly patients with depression. Nutr. Res. 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Grenyer, B.F.; Crowe, T.; Meyer, B.; Owen, A.J.; Grigonis-Deane, E.M.; Caputi, P.; Howe, P.R. Fish oil supplementation in the treatment of major depression: A randomised double-blind placebo-controlled trial. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 1393–1396. [Google Scholar] [CrossRef]
- Meyer, B.J.; Grenyer, B.F.; Crowe, T.; Owen, A.J.; Grigonis-Deane, E.M.; Howe, P.R. Improvement of major depression is associated with increased erythrocyte DHA. Lipids 2013, 48, 863–868. [Google Scholar] [CrossRef]
- Giltay, E.J.; Geleijnse, J.M.; Kromhout, D. Effects of n-3 fatty acids on depressive symptoms and dispositional optimism after myocardial infarction. Am. J. Clin. Nutr. 2011, 94, 1442–1450. [Google Scholar] [CrossRef]
- Sinn, N.; Milte, C.M.; Street, S.J.; Buckley, J.D.; Coates, A.M.; Petkov, J.; Howe, P.R. Effects of n-3 fatty acids, EPA v. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: A 6-month randomised controlled trial. Br. J. Nutr. 2012, 107, 1682–1693. [Google Scholar] [CrossRef]
- Van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Hoefnagels, W.H.; Beekman, A.T.; de Groot, L.C. Effect of fish-oil supplementation on mental well-being in older subjects: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2008, 88, 706–713. [Google Scholar] [CrossRef]
- Minihane, A.M. Impact of Genotype on EPA and DHA Status and Responsiveness to Increased Intakes. Nutrients 2016, 8, 123. [Google Scholar] [CrossRef]
- Minihane, A.M.; Khan, S.; Leigh-Firbank, E.C.; Talmud, P.; Wright, J.W.; Murphy, M.C.; Griffin, B.A.; Williams, C.M. ApoE polymorphism and fish oil supplementation in subjects with an atherogenic lipoprotein phenotype. Arter. Thromb. Vasc. Biol. 2000, 20, 1990–1997. [Google Scholar] [CrossRef] [PubMed]
- Pontifex, M.; Vauzour, D.; Minihane, A.M. The effect of APOE genotype on Alzheimer’s disease risk is influenced by sex and docosahexaenoic acid status. Neurobiol. Aging 2018, 69, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Small, G.W.; Siddarth, P.; Li, Z.; Miller, K.J.; Ercoli, L.; Emerson, N.D.; Martinez, J.; Wong, K.P.; Liu, J.; Merrill, D.A.; et al. Memory and Brain Amyloid and Tau Effects of a Bioavailable Form of Curcumin in Non-Demented Adults: A Double-Blind, Placebo-Controlled 18-Month Trial. Am. J. Geriatr. Psychiatry 2018, 26, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Kuszewski, J.C.; Wong, R.H.X.; Wood, L.G.; Howe, P.R.C. Effects of fish oil and curcumin supplementation on cerebrovascular function in older adults: A randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 625–633. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Wyrwich, K.W.; Yu, H. Validation of POMS questionnaire in postmenopausal women. Qual. Life Res. 2011, 20, 1111–1121. [Google Scholar] [CrossRef]
- Butterworth, P.; Crosier, T. The validity of the SF-36 in an Australian National Household Survey: Demonstrating the applicability of the Household Income and Labour Dynamics in Australia (HILDA) Survey to examination of health inequalities. BMC Public Health 2004, 4, 44. [Google Scholar] [CrossRef]
- Mishra, G.; Schofield, M.J. Norms for the physical and mental health component summary scores of the SF-36 for young, middle-aged and older Australian women. Qual. Life Res. 1998, 7, 215–220. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Treatment allocation by minimisation. BMJ 2005, 330, 843. [Google Scholar] [CrossRef]
- Gota, V.S.; Maru, G.B.; Soni, T.G.; Gandhi, T.R.; Kochar, N.; Agarwal, M.G. Safety and pharmacokinetics of a solid lipid curcumin particle formulation in osteosarcoma patients and healthy volunteers. J. Agric. Food Chem. 2010, 58, 2095–2099. [Google Scholar] [CrossRef]
- Cassiday, L. Sink or swim: Fish oil supplements and human health. INFORM 2016, 27, 6–13. [Google Scholar] [CrossRef]
- Luo, X.D.; Feng, J.S.; Yang, Z.; Huang, Q.T.; Lin, J.D.; Yang, B.; Su, K.P.; Pan, J.Y. High-dose omega-3 polyunsaturated fatty acid supplementation might be more superior than low-dose for major depressive disorder in early therapy period: A network meta-analysis. BMC Psychiatry 2020, 20, 248. [Google Scholar] [CrossRef] [PubMed]
- Hafkemeijer, A.; Altmann-Schneider, I.; Oleksik, A.M.; van de Wiel, L.; Middelkoop, H.A.; van Buchem, M.A.; van der Grond, J.; Rombouts, S.A. Increased functional connectivity and brain atrophy in elderly with subjective memory complaints. Brain Connect. 2013, 3, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Mol, M.; Carpay, M.; Ramakers, I.; Rozendaal, N.; Verhey, F.; Jolles, J. The effect of perceived forgetfulness on quality of life in older adults; a qualitative review. Int. J. Geriatr. Psychiatry 2007, 22, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Mitchell, J.; Arnold, R.; Dawson, K.; Nestor, P.J.; Hodges, J.R. Memory complaints in mild cognitive impairment, worried well, and semantic dementia patients. Alzheimer Dis. Assoc. Disord. 2008, 22, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Adjibade, M.; Assmann, K.E.; Julia, C.; Galan, P.; Hercberg, S.; Kesse-Guyot, E. Prospective association between adherence to the MIND diet and subjective memory complaints in the French NutriNet-Santé cohort. J. Neurol. 2019, 266, 942–952. [Google Scholar] [CrossRef]
- Zhu, J.; Shi, R.; Chen, S.; Dai, L.; Shen, T.; Feng, Y.; Gu, P.; Shariff, M.; Nguyen, T.; Ye, Y.; et al. The Relieving Effects of BrainPower Advanced, a Dietary Supplement, in Older Adults with Subjective Memory Complaints: A Randomized, Double-Blind, Placebo-Controlled Trial. Evid. Based Complement. Altern. Med. 2016, 2016, 7898093. [Google Scholar] [CrossRef]
- Firth, J.; Gangwisch, J.E.; Borisini, A.; Wootton, R.E.; Mayer, E.A. Food and mood: How do diet and nutrition affect mental wellbeing? BMJ 2020, 369, m2382. [Google Scholar] [CrossRef]
- Gardner, M.P.; Wansink, B.; Kim, J.; Park, S. Better moods for better eating? How mood influences food choice. J. Consum. Psychol. 2014, 24, 320–335. [Google Scholar] [CrossRef]
- Huang, T.L.; Zandi, P.P.; Tucker, K.L.; Fitzpatrick, A.L.; Kuller, L.H.; Fried, L.P.; Burke, G.L.; Carlson, M.C. Benefits of fatty fish on dementia risk are stronger for those without APOE epsilon4. Neurology 2005, 65, 1409–1414. [Google Scholar] [CrossRef]
- Whalley, L.J.; Deary, I.J.; Starr, J.M.; Wahle, K.W.; Rance, K.A.; Bourne, V.J.; Fox, H.C. n-3 Fatty acid erythrocyte membrane content, APOE varepsilon4, and cognitive variation: An observational follow-up study in late adulthood. Am. J. Clin. Nutr. 2008, 87, 449–454. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | PL (n = 36) | FO (n = 39) | CUR (n = 38) | FO + CUR (n = 39) |
|---|---|---|---|---|
| Sex (female %) | 50 | 56 | 55 | 56 |
| Age (years) | 65.4 ± 1.3 | 65.4 ± 1.2 | 65.4 ± 1.2 | 66.2 ± 1.3 |
| BMI (kg/m2) | 31.0 ± 0.7 | 31.0 ± 0.7 | 30.5 ± 0.7 | 30.9 ± 0.6 |
| Depressive symptoms (%) | 13.4 ± 1.9 | 14.0 ± 1.7 | 17.0 ± 2.1 | 15.4 ± 2.4 |
| Mood states (POMS) | ||||
| Tension (%) | 16.0 ± 2.2 | 16.8 ± 2.2 | 23.1 ± 2.9 | 23.7 ± 3.1 * |
| Depression (%) | 5.6 ± 1.1 | 7.9 ± 1.8 | 9.6 ± 1.9 | 10.6 ± 2.1 |
| Anger (%) | 7.0 ± 1.0 | 7.1 ± 1.4 | 10.7 ± 2.0 | 10.5 ± 1.7 |
| Fatigue (%) | 28.1 ± 4.1 | 28.1 ± 4.6 | 30.4 ± 3.9 | 28.3 ± 3.5 |
| Confusion (%) | 23.8 ± 2.9 | 23.9 ± 3.1 | 28.6 ± 3.3 | 24.5 ± 2.8 |
| Vigour (%) | 56.2 ± 2.8 | 50.5 ± 3.0 | 49.2 ± 2.8 | 52.5 ± 3.5 |
| TMD a (%) | −40.1 ± 3.6 | −33.7 ± 4.6 | −28.7 ± 4.2 | −33.0 ± 5.0 |
| Subjective memory complaints (%) | 37.5 ± 4.1 | 33.7 ± 4.1 | 35.7 ± 3.9 | 39.4 ± 4.5 |
| Quality of Life (%) | 70.4 ± 2.4 | 72.5 ± 1.9 | 67.1 ± 2.5 | 69.4 ± 2.4 |
| PL (n = 32) | FO (n = 31) | CUR (n = 30) | FO + CUR (n = 30) | |
|---|---|---|---|---|
| Tension (%) | 0.4 ± 1.5 | −0.5 ± 2.1 | 0.0 ± 2.1 | −0.8 ± 2.5 |
| Depression (%) | −0.6 ± 1.3 | −1.6 ± 1.8 | −1.8 ± 2.1 | −0.1 ± 1.6 |
| Anger (%) | −2.1 ± 1.2 | 0.2 ± 1.5 | −2.1 ± 2.1 | −2.2 ± 1.7 |
| Fatigue (%) | −3.1 ± 4.0 | 0.1 ± 4.0 | −1.5 ± 3.5 | 3.8 ± 3.9 |
| Confusion (%) | −3.1 ± 2.4 | −3.4 ± 2.8 | −7.6 ± 3.1 | −3.8 ± 2.4 |
| Vigour (%) | −3.7 ± 2.6 | 1.5 ± 2.9 | 3.5 ± 2.0 * | 2.5 ± 2.4 |
| TMD a (%) | 2.0 ± 3.8 | −2.6 ± 4.2 | −6.1 ± 3.3 | −3.1 ± 3.7 |
| Subjective memory complaints (%) | −1.8 ± 2.5 | −2.6 ± 2.4 | −6.7 ± 2.7 | −8.9 ± 3.1 |
| Quality of Life (%) | 0.3 ± 1.8 | 2.4 ± 1.8 | 2.0 ± 2.1 | 2.1 ± 2.4 |
| APOE4 Non-Carrier (n = 48) | APOE4 Carrier (n = 17) | p-Value | |
|---|---|---|---|
| Sex (female %) | 52 | 53 | |
| Age (years) | 66.3 ± 1.2 | 64.0 ± 1.8 | 0.298 |
| BMI (kg/m2) | 31.5 ± 0.6 | 29.3 ± 0.7 | 0.052 |
| Depressive symptoms (%) | 15.2 ± 1.8 | 15.4 ± 4.2 | 0.953 |
| EPA (%) | 1.06 ± 0.37 | 1.04 ± 0.44 | 0.807 |
| DHA (%) | 5.49 ± 1.36 | 5.73 ± 1.31 | 0.527 |
| Tension (%) | 20.9 ± 2.3 | 25.5 ± 5.3 | 0.356 |
| Depression (%) | 10.4 ± 1.8 | 9.7 ± 3.4 | 0.855 |
| Anger (%) | 8.5 ± 1.4 | 12.2 ± 3.1 | 0.214 |
| Fatigue (%) | 30.3 ± 4.1 | 23.3 ± 3.9 | 0.219 |
| Confusion (%) | 26.8 ± 2.8 | 22.3 ± 4.0 | 0.388 |
| Vigour (%) | 49.4 ± 2.7 | 52.2 ± 5.7 | 0.619 |
| TMD a (%) | −30.0 ± 4.2 | −33.6 ± 8.0 | 0.671 |
| Subjective memory complaints (%) | 41.9 ± 3.8 | 30.6 ± 6.5 | 0.137 |
| Quality of life (%) | 69.5 ± 2.0 | 72.7 ± 3.4 | 0.430 |
| PL (n = 32) | FO (n = 22) | CUR (n = 30) | FO + CUR (n = 22) | |
|---|---|---|---|---|
| Tension (%) | 0.4 ± 1.5 | −3.6 ± 1.8 | 0.0 ± 2.1 | −2.7 ± 3.0 |
| Depression (%) | −0.6 ± 1.3 | −4.4 ± 1.9 | −1.8 ± 2.1 | −1.7 ± 1.9 |
| Anger (%) | −2.1 ± 1.2 | −1.8 ± 1.3 | −2.1 ± 2.1 | −2.9 ± 2.0 |
| Fatigue (%) | −3.1 ± 4.0 | −3.8 ± 4.4 | −1.5 ± 3.5 | 2.3 ± 4.8 |
| Confusion (%) | −3.1 ± 2.4 | −7.9 ± 2.7 | −7.6 ± 3.1 | −4.4 ± 3.1 |
| Vigour (%) | −3.7 ± 2.6 | 4.8 ± 3.3 * | 3.5 ± 2.0 * | 3.6 ± 3.1 |
| TMD a (%) | 2.0 ± 3.8 | −9.1 ± 4.0 * | −6.1 ± 3.3 | −5.4 ± 4.8 |
| Subjective memory complaints (%) | −1.8 ± 2.5 | −6.1 ± 2.6 | −6.7 ± 2.7 | −11.0 ± 3.9 * |
| Quality of life (%) | 0.3 ± 1.8 | 4.6 ± 2.0 | 2.0 ± 2.1 | 1.8 ± 2.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuszewski, J.C.; Howe, P.R.C.; Wong, R.H.X. An Exploratory Analysis of Changes in Mental Wellbeing Following Curcumin and Fish Oil Supplementation in Middle-Aged and Older Adults. Nutrients 2020, 12, 2902. https://doi.org/10.3390/nu12102902
Kuszewski JC, Howe PRC, Wong RHX. An Exploratory Analysis of Changes in Mental Wellbeing Following Curcumin and Fish Oil Supplementation in Middle-Aged and Older Adults. Nutrients. 2020; 12(10):2902. https://doi.org/10.3390/nu12102902
Chicago/Turabian StyleKuszewski, Julia C., Peter R. C. Howe, and Rachel H. X. Wong. 2020. "An Exploratory Analysis of Changes in Mental Wellbeing Following Curcumin and Fish Oil Supplementation in Middle-Aged and Older Adults" Nutrients 12, no. 10: 2902. https://doi.org/10.3390/nu12102902
APA StyleKuszewski, J. C., Howe, P. R. C., & Wong, R. H. X. (2020). An Exploratory Analysis of Changes in Mental Wellbeing Following Curcumin and Fish Oil Supplementation in Middle-Aged and Older Adults. Nutrients, 12(10), 2902. https://doi.org/10.3390/nu12102902