Comparison of the Effects of Brazil Nut Oil and Soybean Oil on the Cardiometabolic Parameters of Patients with Metabolic Syndrome: A Randomized Trial

 ,
,
Abstract
1. Introduction
2. Materials and Methods
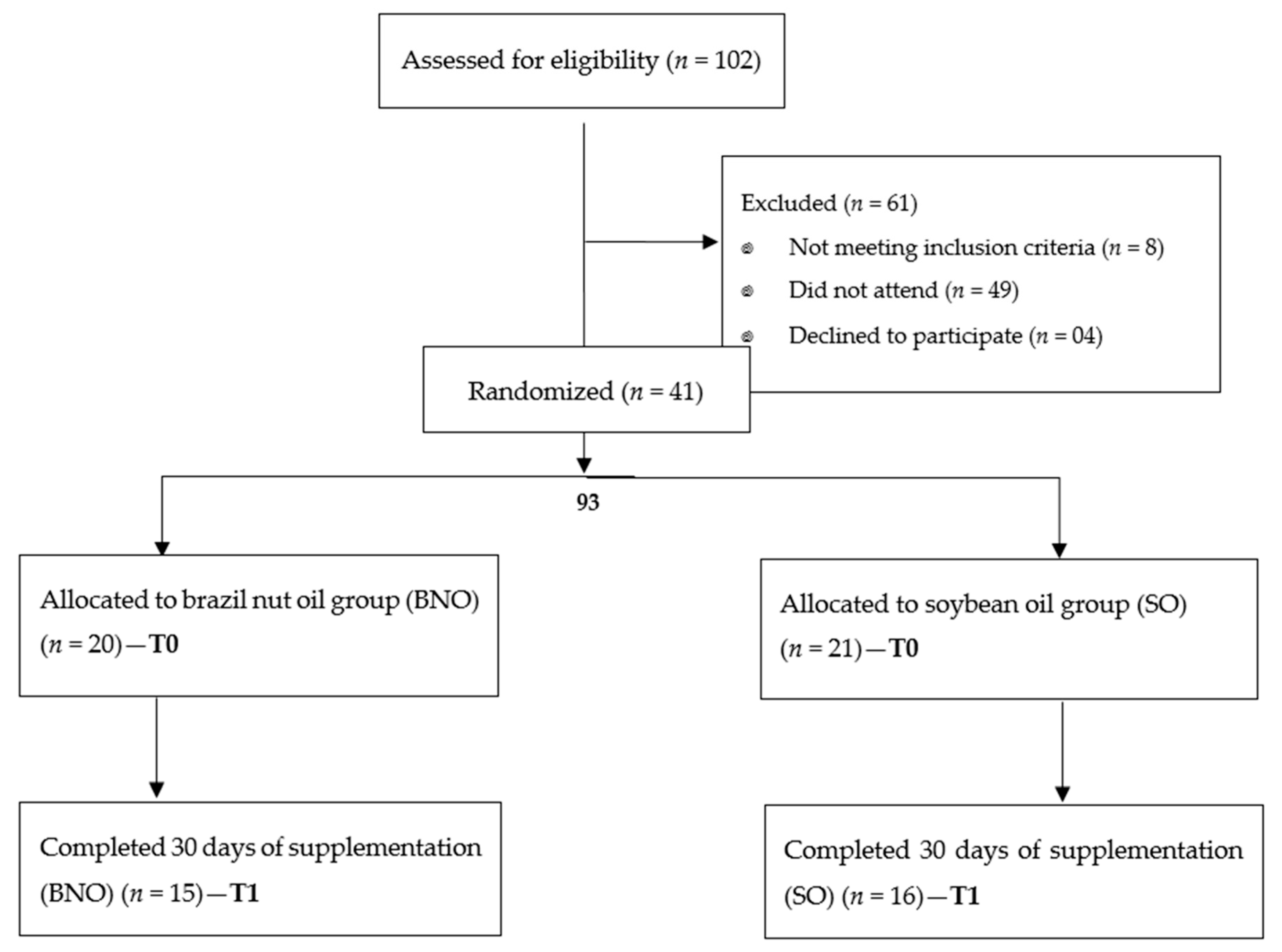
2.1. Participants
2.2. Experimental Design
2.3. Oils
Determination of the Fatty Acid Profile of Brazil Nut Oil
2.4. Assessments
2.4.1. Body Composition and Blood Pressure Parameters
2.4.2. Biochemical Parameters
2.4.3. Oxidative Parameters
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohamed, S. Functional foods against metabolic syndrome (obesity, diabetes, hypertension and dyslipidemia) and cardiovasular disease. Trends Food Sci. Technol. 2014, 35, 114–128. [Google Scholar] [CrossRef]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; de Koning, L.; Delgado-Lista, J.; Díaz-Lopez, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef]
- Minich, D.M.; Bland, J.S. Dietary management of the metabolic syndrome beyond macronutrients. Nutr. Rev. 2008, 66, 429–444. [Google Scholar] [CrossRef]
- Abete, I.; Astrup, A.; Martinez, J.A.; Thorsdottir, I.; Zulet, M.A. Obesity and the metabolic syndrome: Role of different dietary macronutrient distribution patterns and specific nutritional components on weight loss and maintenance. Nutr. Rev. 2010, 68, 214–231. [Google Scholar] [CrossRef]
- Keane, D.; Kelly, S.; Healy, N.P.; McArdle, M.A.; Holohan, K.; Roche, H.M. Diet and metabolic syndrome: An overview. Curr. Vasc. Pharmacol. 2013, 11, 842–857. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care 2013, 36, 3821–3842. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations. Fats and Fatty Acids in Human Nutrition; Food and Agriculture Organization of the United Nations: Rome, Italy, 2010; ISBN 978-92-5-106733-8. [Google Scholar]
- Aranceta, J.; Pérez-Rodrigo, C. Recommended dietary reference intakes, nutritional goals and dietary guidelines for fat and fatty acids: A systematic review. Br. J. Nutr. 2012, 107, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.D.; Gagliardi, A.C.M.; Xavier, H.T.; Magnoni, C.D.; Cassani, R.; Lottenberg, A.M.; Casella, F.A.; Araújo, D.B.; Cesena, F.Y.; Alves, R.J.; et al. First guidelines on fat consumption and cardiovascular health [Article in Portuguese]. Arq. Bras. Cardiol. 2013, 100 (Suppl. 3), 1–40. [Google Scholar] [CrossRef]
- Siró, I.; Kápolna, E.; Kápolna, B.; Lugasi, A. Functional food. Product development, marketing and consumer acceptance—A review. Appetite 2008, 51, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, A.; Tsang, C.; Tiss, A.; Bahorun, T.; Arefanian, H.; Barake, R.; Khadir, A.; Tuomilehto, J. Functional foods and lifestyle approaches for diabetes prevention and management. Nutrients 2017, 9, 1310. [Google Scholar] [CrossRef]
- Santos, O.V.; Corrêa, N.C.F.; Soares, F.A.S.M.; Gioelli, L.A.; Costa, C.E.F.; Lannes, S.C.S. Chemical evaluation and thermal behavior of Brazil nut oil obtained by different. Food Res. Int. 2012, 47, 253–258. [Google Scholar] [CrossRef]
- Kocygit, A.; Koylu, A.A.; Keles, H. Effects of pistachio nuts consumption on plasma lipid profile and oxidative status in healthy volunteers. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Ros, E. Nuts and novel biomarkers of cardiovascular disease. Am. J. Clin. Nutr. 2009, 89, 1649–1656. [Google Scholar] [CrossRef]
- Ros, E.; Nunez, I.; Perez-Heras, A.; Serra, M.; Gilabert, R.; Casals, E.; Deulofeu, R. A walnut diet improves endothelial function in hypercholesterolemic subjects: A randomized crossover trial. Circulation 2004, 109, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Mataix, J. Fatty acid composition of nuts–implications for cardiovascular health. Br. J. Nutr. 2006, 96, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Yang, J. Brazil nuts and associated health benefits: A review. LWT Food Sci. Technol. 2009, 42, 1573–1580. [Google Scholar] [CrossRef]
- NCEP; Adult Treatment Panel III. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Rodrigues, A.M.C.; Darnetb, S.; Silva, L.H.M. Fatty Acid Profiles and Tocopherol Contents of Buriti (Mauritia flexuosa), Patawa (Oenocarpus bataua), Tucuma (Astrocaryum vulgare), Mari (Poraqueiba paraensis) and Inaja (Maximiliana maripa) Fruits. J. Braz. Chem. Soc. 2010, 21, 2000–2004. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1988; ISBN 978-087-322-121-4. [Google Scholar]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry—Report of a WHO Expert Committee; WHO Technical Report Series No. 854; World Health Organization: Geneva, Switzerland, 1995; ISBN 924-120-854-6. [Google Scholar]
- Veiga, E.V.; Nogueira, M.S.; Cárnio, E.C.; Marques, S.; Lavrador, M.A.; De Moraes, S.A.; Souza, L.A.C.; Lima, N.K.C.; Nobre, F. Assessment of the techniques of blood pressure measurement by health professionals [Article in Portuguese]. Arq. Bras. Cardiol. 2003, 80, 89–93. [Google Scholar] [CrossRef]
- Friedwald, W.; Levy, A.L.; Frederickson, D.S. Estimation of concentrations of low-density cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–4502. [Google Scholar]
- Miller, N.; Rice-Evans, C.; Davies, M.; Gopinathan, V.; Milner, A. A novel method for measuring antioxidant capacity and its application to monitoring the antioxidant status in premature neonates. Clin. Sci. (Lond.) 1993, 84, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Re, R.; Pellegrini, R.; Protegente, A.; Pannala, A.; Yang, M.; Rice-Evans, C. Antioxidant activity applying an improved ABTS radical cation decolorizaton assay. Free Radic. Biol. Med. 1999, 26, 1231–1237. [Google Scholar] [CrossRef]
- Vasconcelos, S.M.L.; Goulart, M.O.F.; Moura, J.B.F.; Manfredini, V.; Benfato, M.S.; Kubota, L.T. Reactive oxygen and nitrogen species, antioxidants and markers of oxidative damage in human blood: Main analytical methods for their determination [Article in Portuguese]. Chem. Nova 2007, 30, 1323–1338. [Google Scholar] [CrossRef]
- Khonn, H.I.; Liversedge, M. On a new aerobic metabolite whose production by brain is inhibited by apomorphine, methine, ergotamine, epinephrine and menadione. J. Pharmacol. Exp. Ther. 1944, 83, 292–300. [Google Scholar]
- Percário, S.; Vital, A.; Jablonka, F. Malondialdehyde dosage [Article in Portuguese]. Newslab 1994, 2, 46–50. [Google Scholar]
- Mayne, S.T. Antioxidant nutrients and chronic disease: Use of biomarkers of exposure and oxidative stress status in epidemiologic research. J. Nutr. 2003, 133, 933–940. [Google Scholar] [CrossRef]
- Ayres, M.; Ayres, M., Jr.; Ayres, D.L.; Santos, A.A.S. BioEstat 5.3: Aplicações Estatísticas Nas Áreas das Ciências Biológicas e Médicas, 5th ed.; Publicações Avulsas do Mamirauá: Belém, Brazil, 2007; p. 361. [Google Scholar]
- Zaunschirm, M.; Pignitter, M.; Kienesberger, J.; Hernler, N.; Riegger, C.; Eggersdorfer, M.; Somoza, V. Contribution of the ratio of tocopherol homologs to the oxidative stability of commercial vegetable oils. Molecules 2018, 23, 206. [Google Scholar] [CrossRef]
- Martin, C.A.; Visentainer, J.V.; de Oliveira, A.N.; de Oliveira, C.C.; Matsushita, M.; de Souza, N.E. Fatty acid contents of Brazilian soybean oils with emphasis on trans-fatty acids. J. Braz. Chem. Soc. 2008, 19, 117–122. [Google Scholar] [CrossRef]
- Muniz, M.A.P.; Santos, M.N.F.; Costa, C.E.F.; Morais, L.; Lamarão, M.L.N.; Ribeiro-Costa, R.M.; Silva-Junior, O.C. Physicochemical characterization, fatty acid composition, and thermal analysis of Bertholletia excelsa HBK oil. Pharmacogn. Mag. 2015, 11, 147–151. [Google Scholar] [CrossRef]
- Keys, A.; Kimura, N.; Kusukawa, A.; Bonte-Stewart, B.; Larsen, N.; Keys, M.H. Lessons from serum cholesterol studies in Japan, Hawaii and Los Angeles. Ann. Intern. Med. 1958, 48, 83–94. [Google Scholar] [CrossRef]
- Connor, S.L.; Gustafson, J.R.; Artaud-Wild, S.M.; Flavell, D.P.; Classick-Kohn, C.J.; Hatcher, L.F.; Connor, W.E. The cholesterol/saturated-fat index: An indication of the hypercholesterolaemic and atherogenic potential of food. Lancet 1986, 1, 1229–1232. [Google Scholar] [CrossRef]
- Lands, B. A critique of paradoxes in current advice on dietary lipids. Prog. Lipid Res. 2008, 47, 77–106. [Google Scholar] [CrossRef] [PubMed]
- Pilar, B.C.; Güllich, A.P.C.; Ströher, D.J.; Zuravski, L.; Mezzomo, J.; Coelho, R.P.; Faoro, D.; Piccoli, J.D.; Manfredini, V. 28-days dietary supplementation with golden flaxseed improves biochemical and oxidative parameters in patients with metabolic syndrome. J. Funct. Foods 2014, 10, 232–242. [Google Scholar] [CrossRef]
- Harris, M.; Hutchins, A.; Fryda, L. The impact of virgin coconut oil and high-oleic safflower oil on body composition, lipids, and inflammatory markers in postmenopausal women. J. Med. Food 2017, 20, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Paschos, G.K.; Magkos, F.; Panagiotakos, D.B.; Votteas, V.; Zampelas, A. Dietary supplementation with flaxseed oil lowers blood pressure in dyslipidaemic patients. Eur. J. Clin. Nutr. 2007, 61, 1201–1206. [Google Scholar] [CrossRef] [PubMed]
- Amir, K.; Watanabe, M.; Yokotsuka, M.; Kobayashi, Y. Changes in serum fatty acids and effects of metabolic syndrome induced by intermittent flaxseed-oil supplementation. Ningen Dock 2011, 26, 927–934. [Google Scholar] [CrossRef]
- Hensler, M.; Bardova, K.; Jilkova, Z.M.; Wahli, W.; Meztger, D.; Chambon, P.; Kopecky, J.; Flachs, P. The inhibition of fat cell proliferation by n-3 fatty acids in dietary obese mice. Lipids Health Dis. 2011, 10, 2–7. [Google Scholar] [CrossRef]
- Miller, M.; Sorkin, J.D.; Mastella, L.; Sutherland, A.; Rhyne, J.; Donnelly, P.; Simpson, K.; Goldberg, A.P. Poly is more effective than mono-unsaturated fat for dietary management in the metabolic syndrome: The muffin study. J. Clin. Lipidol. 2016, 10, 996–1003. [Google Scholar] [CrossRef]
- Tripodi, A.; Loria, P.; Dilengite, M.A.; Carulli, N. Effect of fish oil and coconut oil diet on the LDL receptor activity of rat liver plasma membranes. Biochim. Biophys. Acta 1991, 1083, 298–304. [Google Scholar] [CrossRef]
- Fernandez, M.L.; McNamar, D.J. Dietary fat-mediated changes in hepatic apoprotein B/E receptor in the guinea pig: Effect of polyunsaturated, monounsaturated, and saturated fat. Metabolism 1989, 38, 1094–1102. [Google Scholar] [CrossRef]
- Spritz, N.; Mishkel, M.A. Effects of dietary fats on plasma lipids and lipoproteins: A hypothesis for the lipid-lowering effect of unsaturated fatty acids. J. Clin. Investig. 1969, 48, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Cederbaum, A.I.; Zhang, Y.L.; Ginsberg, H.N.; Williams, K.J.; Fisher, E.A. Lipid peroxidation and oxidant stress regulate hepatic apolipoprotein B degradation and VLDL production. J. Clin. Investig. 2004, 113, 1277–1287. [Google Scholar] [CrossRef] [PubMed]
- Reaven, P.; Parthasarathy, S.; Grasse, B.J.; Miller, E.; Almazan, F.; Mattson, F.H.; Khoo, J.C.; Steinberg, D.; Witztum, J.L. Feasibility of using an oleate-rich diet to reduce the susceptibility of low-density lipoprotein to oxidative modification in humans. Am. J. Clin. Nutr. 1991, 54, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M. George Lyman Duff Memorial Lecture. Multifactorial etiology of hypercholesterolemia. Implications for prevention of coronary heart disease. Arterioscler. Thromb. 1991, 11, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.J.H.; Lichtenstein, A.H.; Schaefer, E.J.; Namchuk, G.L. Effect of dietary fat selection on plasma cholesterol synthesis in older, moderately hypercholesterolemic humans. Arterioscler. Thromb. 1994, 14, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Niazi, S.; Mirmiran, P.; Fallah-Ghohroudi, A.; Azizi, F. Combined effect of unsaturated fatty acids and saturated fatty acids on the metabolic syndrome: Tehran lipid and glucose study. J. Health Popul. Nutr. 2015, 33, 5. [Google Scholar] [CrossRef]
- Faludi, A.A.; Izar, M.C.O.; Saraiva, J.F.K.; Chacra, A.P.M.; Bianco, H.T.; Afiune Neto, A.; Bertolami, A.; Pereira, A.C.; Lottenberg, A.M.; Sposito, A.C.; et al. Atualização da Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose [Article in Portuguese]. Arq. Bras. Cardiol. 2017, 109 (Suppl. 1), 1–76. [Google Scholar] [CrossRef]
- Zibaeenezhad, M.J.; Farhadi, P.; Attar, A.; Mosleh, A.; Amirmoezi, F.; Azimi, A. Effects of walnut oil on lipid profiles in hyperlipidemic type 2 diabetic patients: A randomized, double-blind, placebo-controlled trial. Nutr. Diabetes 2017, 7, 259. [Google Scholar] [CrossRef]
- Shen, T.; Xing, G.; Zhu, J.; Zhang, S.; Cai, Y.; Li, D.; Xu, G.; Xing, E.; Rao, J.; Shi, R. Effects of 12-week supplementation of marine Omega-3 PUFA-based formulation Omega3Q10 in older adults with prehypertension and/or elevated blood cholesterol. Lipids Health Dis. 2017, 16, 253. [Google Scholar] [CrossRef]
- Oliveira-de-Lira, L.; Santos, E.M.C.; de Souza, R.F.; Matos, R.J.B.; Silva, M.C.D.; Oliveira, L.D.S.; Nascimento, T.G.D.; Schemly, P.A.L.S.; Souza, S.L. Supplementation-dependent effects of vegetable oils with varying fatty acid compositions on anthropometric and biochemical parameters in obese women. Nutrients 2018, 10, 932. [Google Scholar] [CrossRef]
- Hodson, L.; Skeaff, C.M.; Chisholm, W.A. The effect of replacing dietary saturated fat with polyunsaturated or monounsaturated fat on plasma lipids in free-living young adults. Eur. J. Clin. Nutr. 2001, 55, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Tierney, A.C.; McMonagle, J.; Shaw, D.I.; Gulseth, H.L.; Helal, O.; Saris, W.H.; Paniagua, J.A.; Gołąbek-Leszczyñska, I.; Defoort, C.; Williams, C.M.; et al. Effects of dietary fat modification on insulin sensitivity and on other risk factors of the metabolic syndrome—LIPGENE: A European randomized dietary intervention study. Int. J. Obes. (Lond.) 2011, 35, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A. Yogurt and dairy product consumption to prevent cardiometabolic diseases: Epidemiologic and experimental studies. Am. J. Clin. Nutr. 2014, 99, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, M.; Vasudevan, D.M.; Sundaram, K.R.; Krishnan, S.; Vaidyanathan, K.; Nandakumar, S.; Chandrasekhar, R.; Mathew, N. A randomized study of coconut oil versus sunflower oil on cardiovascular risk factors in patients with stable coronary heart disease. Indian Heart J. 2016, 68, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Karupaiah, T.; Chuah, K.; Chinna, K.; Matsuoka, R.; Masuda, Y.; Sundram, K.; Michihiro, S. Comparing effects of soybean oil- and palm olein-based mayonnaise consumption on the plasma lipid and lipoprotein profiles in human subjects: A double-blind randomized controlled trial with cross-over design. Lipids Health Dis. 2016, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.K.; Yoon, S. Relation of serum total antioxidant status with metabolic syndrome risk factors in Korean adults. Nutr. Res. Pract. 2007, 1, 335–340. [Google Scholar] [CrossRef][Green Version]
- Demirbag, R.; Yilmaz, R.; Kunt, A.S.; Gur, M.; Ulucay, A.; Unlu, D. Relationship between plasma total antioxidant capacity and thoracic aortic intima-media thickness. Echocardiography 2006, 23, 183–188. [Google Scholar] [CrossRef]
- Kitabchi, E.; McDaniel, K.A.; Wan, J.Y.; Tylavsky, F.A.; Jacovino, C.A.; Sands, C.W.; Nyenwe, E.A.; Stentz, F.B. Effects of high-protein versus high-carbohydrate diets on markers of β-cell function, oxidative stress, lipid peroxidation, proinflammatory cytokines, and adipokines in obese, premenopausal women without diabetes: A randomized control trial. Diabetes Care 2013, 36, 1919–1925. [Google Scholar] [CrossRef]
- Yuzefovych, L.V.; Musiyenko, S.I.; Wilson, G.L.; Rachek, L.I. Mitochondrial DNA damage and dysfunction, and oxidative stress are associated with endoplasmic reticulum stress, protein degradation and apoptosis in high fat diet-induced insulin resistance mice. PLoS ONE 2013, 8, 540–559. [Google Scholar] [CrossRef]
- Tan, B.L.; Norhaizan, M.E.; Liew, W. Nutrients and Oxidative Stress: Friend or Foe? Oxid. Med. Cell. Longev. 2018, 2018, 9719584. [Google Scholar] [CrossRef]
- Scalbert, A.; Manach, C.; Morand, C.; Rémésy, C.; Jiménez, L. Dietary polyphenols and the prevention of diseases. Crit. Rev. Food Sci. Nutr. 2005, 287–306. [Google Scholar] [CrossRef] [PubMed]
- Scalbert, A.; Williamson, G. Dietary intake and bioavailability of polyphenols. J. Nutr. 2000, 130, 2073–2085. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.R.; Gonçalves, L.A. Quantificação de tocoferóis em óleos de milho, soja, castanha-do-pará e castanha de caju por cromatografia líquida de alta eficiência em fase reversa. Alim. Nutr. Araraquara 1997, 8, 65–73. [Google Scholar]
- Silveira, C.S. Caracterização Físico-Química e Avaliação Biológica de Produtos da Castanha-do-Brasil (Bertholletia Excelsa H.B.K.). Ph.D. Thesis, Programa de Pós-Graduação em Ciência e Tecnologia de Alimentos, Faculdade de Agronomia, Universidade Federal de Pelotas, Pelotas Rio Grande do Sul, Brazil, 2015; p. 146. [Google Scholar]
- Funasaki, M.; Menezes, I.S.; Barroso, H.S.; Zanotto, S.P.; Carioca, C.R.F. Tocopherol profile of Brazil nut oil from different geographic areas of the Amazon region. Acta Amaz. 2013, 43, 505–510. [Google Scholar] [CrossRef][Green Version]
- Yang, J.; Liu, R.H.; Halim, L. Antioxidant and antiproliferative activities of common edible nut seeds. LWT Food Sci. Technol. 2009, 42, 1–8. [Google Scholar] [CrossRef]
- Abe, L.T.; Lajolo, F.M.; Genovese, M.I. Comparison of phenol content and antioxidant capacity of nuts. Ciênc. Tecnol. Aliment. 2010, 30, 254–259. [Google Scholar] [CrossRef]
- Brand-Williams, W.; Cuvelier, M.E.; Berset, C. Use of a free radical method to evaluate antioxidant activity. LWT Food Sci. Technol. 1995, 28, 25–30. [Google Scholar] [CrossRef]
- Singh, B.; Singh, J.P.; Kaur, A.; Singh, N. Phenolic compounds as beneficial phytochemicals in pomegranate (Punica granatum L.) peel: A review. Food Chem. 2018, 261, 75–86. [Google Scholar] [CrossRef]
- Maranhão, P.A.; Kraemer-Aguiar, L.G.; De Oliveira, C.L.; Kuschnir, M.C.C.; Vieira, Y.R.; Souza, M.G.C.; Koury, J.C.; Bouskela, E. Brazil nuts intake improves lipid profile, oxidative stress and microvascular function in obese adolescents: A randomized controlled trial. Nutr. Metab. (Lond.) 2011, 8, 32. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Fatty Acid | Usual Name | Brazil Nut Oil (%) | Soybean Oil * (%) |
|---|---|---|---|
| C8:0 | Caprylic Acid | 0.03 | - |
| C10:0 | Capric Acid | 0.04 | - |
| C12:0 | Lauric Acid | 1.19 | - |
| C14:0 | Myristic Acid | 0.72 | - |
| C16:0 | Palmitic Acid | 14.89 | 11.50 |
| C16:1 | Palmitoleic Acid | 0.32 | - |
| C17:0 | Margaric Acid | 0.07 | - |
| C18:0 | Stearic Acid | 10.04 | 3.62 |
| C18:1 | Oleic Acid | 37.58 | 24.0 |
| C18:2 | Linoleic Acid | 34.71 | 54.6 |
| C18:3 | α-Linolenic Acid | 0.28 | 5.87 |
| C20:0 | Arachidic Acid | 0.08 | 0.46 |
| C22:0 | Behenic Acid | 0.05 | - |
| ∑ Saturated | 27.11 | 15.58 | |
| ∑ Monounsaturated | 37.90 | 24.0 | |
| ∑ Polyunsaturated | 34.99 | 60.47 |
| BNO | SO | |||||
|---|---|---|---|---|---|---|
| Before | After | Δ | Before | After | Δ | |
| Sample size | 15 | 15 | 15 | 16 | 16 | 16 |
| BMI | 32.2 | 31.5 | −0.7 | 30.8 | 30.8 | −0.1 |
| ±4.4 | ±4.4 | 1.2 | ±4.4 | ±4.5 | 0.3 | |
| p-value (intragroup) | 0.0566 | 0.4539 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.4125 | 0.6601 | 0.1280 | |||
| %BF | 39.9 | 40.3 | 0.4 | 43.7 | 44.3 | 0.6 |
| ±8.1 | ±8.7 | 1.4 | ±6.6 | ±6.4 | 1.4 | |
| p-value (intragroup) | 0.9089 | 0.8045 | ||||
| T0 | T0 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.0782 | 0.0904 | 0.8712 | |||
| WC | 109.1 | 108.2 | −1.3 | 102.3 | 101.3 | −1.0 |
| ±10.3 | ±8.8 | 2.7 | ±10.7 | ±9.8 | 3.6 | |
| p-value (intragroup) | 0.3224 | 0.2859 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.1303 | 0.0939 | 0.9569 | |||
| SBP | 132.0 | 130.6 | −1.4 | 133.9 | 125.8 | −8.2 |
| ±19.8 | ±16.7 | 12.7 | ±17.3 | ±14.4 | 16.6 | |
| p-value (intragroup) | 0.5434 | 0.4456 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.7824 | 0.4073 | 0.3705 | |||
| DBP | 78.5 | 78.2 | −0.3 | 78.8 | 76.3 | −2.5 |
| ±11.8 | ±10.4 | 4.1 | ±6.8 | ±11.0 | 10.2 | |
| p-value (intragroup) | 0.8062 | 0.3051 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.5532 | 0.4768 | 0.5673 | |||
| BNO | SO | |||||
|---|---|---|---|---|---|---|
| Before | After | Δ | Before | After | Δ | |
| Sample size | 15 | 15 | 16 | 16 | 16 | 16 |
| Cholesterol | 243.1 | 240.0 | −3.1 | 216.6 | 240.5 | 23.9 |
| ±59.9 | ±53.4 | ±66.2 | ±35.2 | ±38.8 | ±38.6 | |
| p-value (intragroup) | 0.8604 | 0.0253 * | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.3738 | 0.9370 | 0.2684 | |||
| LDL | 161.3 | 151.3 | −9.9 | 132.6 | 155.3 | 22.7 |
| ±58.8 | ±59.0 | ±68.6 | ±37.5 | ±38.7 | ±43.6 | |
| p-value (intragroup) | 0.5823 | 0.0437 * | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.2599 | 0.9656 | 0.2434 | |||
| HDL | 36.5 | 29.7 | −6.8 | 40.2 | 42.6 | 2.2 |
| ±8.1 | ±8.2 | ±8.7 | ±12.2 | ±14.3 | ±9.9 | |
| p-value (intragroup) | 0.0087 * | 0.3499 | ||||
| T0 | T1 | Δ (T1 = T0) | ||||
| p-value (BNO × SO) | 0.2948 | 0.1665 | 0.0121 * | |||
| Triglycerides | 226.7 | 295.3 | 68.6 | 218.3 | 213.8 | −4.5 |
| ±32.1 | ±73.8 | ±83.6 | ±36.6 | ±46.0 | ±−4.5 | |
| p-value (intragroup) | 0.0045 *b | 0.8501 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.8451 | 0.0021 *a | 0.0066 *a | |||
| Glucose | 153.4 | 157.6 | 4.1 | 115,8 | 106.8 | −9.0 |
| ±78.1 | ±68.2 | ±43.1 | ±32 | ±26.9 | ±38.8 | |
| p-value (intragroup) | 0.7143 | 0.3678 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.5016 | 0.0282 *c | 0.0368 * | |||
| BNO | SO | |||||
|---|---|---|---|---|---|---|
| Before | After | Δ | Before | After | Δ | |
| Sample size | 14 | 14 | 14 | 15 | 15 | 15 |
| TEAC | 3.20 | 3.26 | 0.06 | 3.39 | 3.50 | 0.10 |
| ±0.80 | ±0.69 | ±1.12 | ±0.10 | ±0.10 | ±0.13 | |
| p-value (intragroup) | 0.8727 | 0.0110 * | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.3041 | 0.4767 | 0.6112 | |||
| MDA | 3.18 | 2.27 | −0.84 | 2.91 | 2.60 | −0.31 |
| ±0.93 | ±0.96 | ±1.92 | ±0.48 | ±1.42 | ±1.51 | |
| p-value (intragroup) | 0.0296 * | 0.4511 | ||||
| T0 | T1 | Δ (T1 − T0) | ||||
| p-value (BNO × SO) | 0.9658 | 0.8362 | 0.5053 | |||
| MDA/triglycerides (nmol/mg) | 1.40 | 0.77 | −0.63 | 1.33 | 1.22 | −0.12 |
| MDA/TEAC | 0.99 | 0.69 | −0.3 | 0.86 | 0.74 | −0.12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa e Silva, L.M.; Pereira de Melo, M.L.; Faro Reis, F.V.; Monteiro, M.C.; dos Santos, S.M.; Quadros Gomes, B.A.; Meller da Silva, L.H. Comparison of the Effects of Brazil Nut Oil and Soybean Oil on the Cardiometabolic Parameters of Patients with Metabolic Syndrome: A Randomized Trial. Nutrients 2020, 12, 46. https://doi.org/10.3390/nu12010046
Costa e Silva LM, Pereira de Melo ML, Faro Reis FV, Monteiro MC, dos Santos SM, Quadros Gomes BA, Meller da Silva LH. Comparison of the Effects of Brazil Nut Oil and Soybean Oil on the Cardiometabolic Parameters of Patients with Metabolic Syndrome: A Randomized Trial. Nutrients. 2020; 12(1):46. https://doi.org/10.3390/nu12010046
Chicago/Turabian StyleCosta e Silva, Lívia Martins, Maria Luisa Pereira de Melo, Fernando Vinicius Faro Reis, Marta Chagas Monteiro, Savio Monteiro dos Santos, Bruno Alexandre Quadros Gomes, and Luiza Helena Meller da Silva. 2020. "Comparison of the Effects of Brazil Nut Oil and Soybean Oil on the Cardiometabolic Parameters of Patients with Metabolic Syndrome: A Randomized Trial" Nutrients 12, no. 1: 46. https://doi.org/10.3390/nu12010046
APA StyleCosta e Silva, L. M., Pereira de Melo, M. L., Faro Reis, F. V., Monteiro, M. C., dos Santos, S. M., Quadros Gomes, B. A., & Meller da Silva, L. H. (2020). Comparison of the Effects of Brazil Nut Oil and Soybean Oil on the Cardiometabolic Parameters of Patients with Metabolic Syndrome: A Randomized Trial. Nutrients, 12(1), 46. https://doi.org/10.3390/nu12010046