Bariatric Surgery and Brain Health—A Longitudinal Observational Study Investigating the Effect of Surgery on Cognitive Function and Gray Matter Volume

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
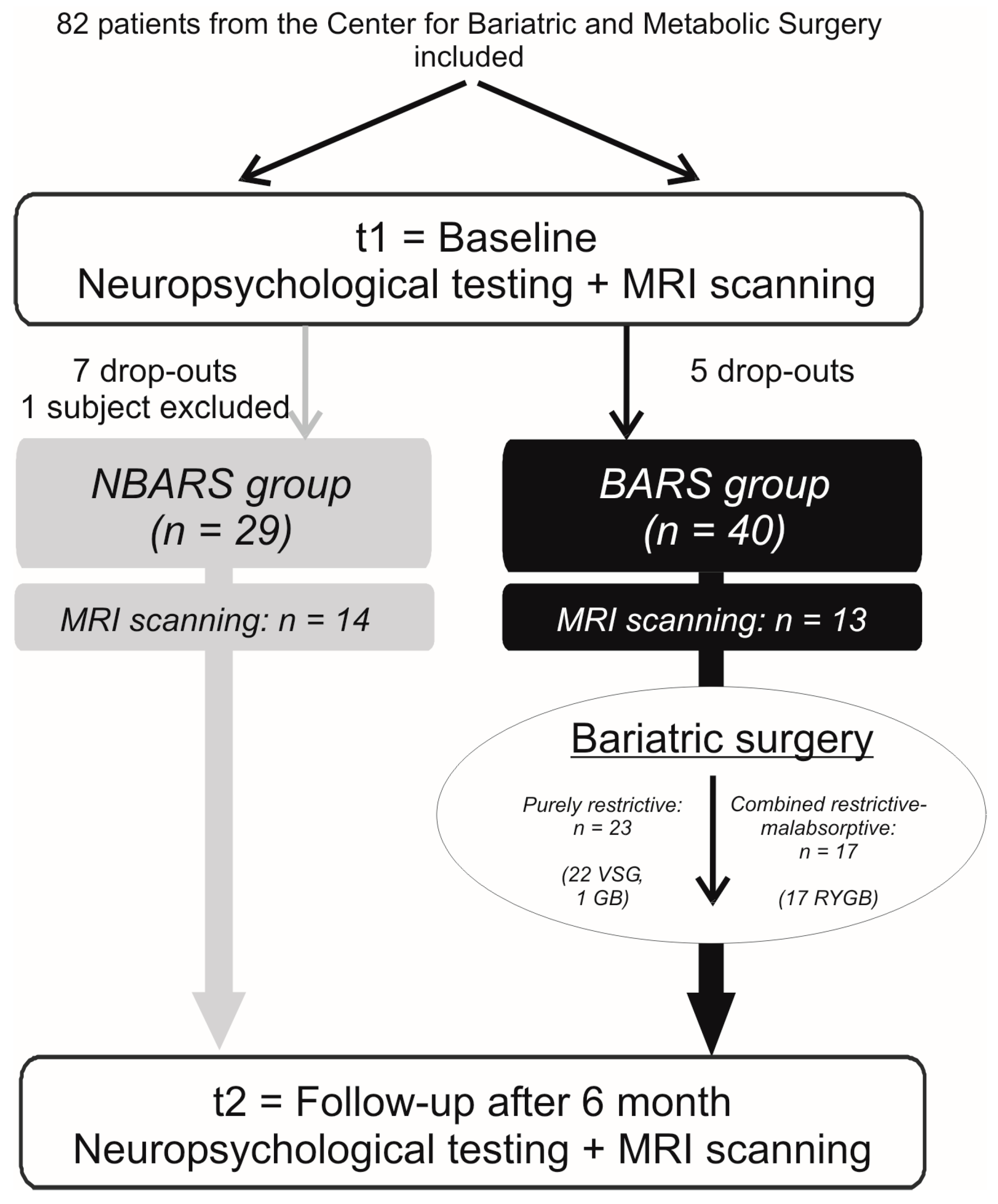
2.1. Study Overview
2.2. Participants
2.3. Assessment of Neuropsychological and Physical Data
- Executive functions = [zphonematic fluency + zsemantic fluency − zTMT (part B − part A)/part A − zStroop (part 3 − (part 1 + part 2))/2]/4;
- Memory = (zVLMT learning score + zVLMT delayed recall score + zVLMT recognition score + zdigit span backwards)/4;
- Sensomotor speed = (−zTMT part A − zStroop part A − zStroop part B)/3;
- Attention = zdigit span forwards.
2.4. Statistical Analysis of Neuropsychological and Physical Data
2.5. MRI Data Acquisition and Voxel-Based Morphometry
3. Results
3.1. Baseline Characteristics
3.2. Changes in Physical and Neuropsychological Parameters
3.3. Changes in GM Volume
3.4. Differences between Surgical Procedures
4. Discussion
4.1. Effects of BARS on Cognitive Functions
4.2. Effects of BARS on Brain Structure
4.3. Influence of Surgical Procedure on Cognitive Performance
4.4. Limitations
4.5. Conclusion and Outlook
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
References
- Finucane, M.M.; Stevens, G.A.; Cowan, M.J.; Danaei, G.; Lin, J.K.; Paciorek, C.J.; Singh, G.M.; Gutierrez, H.R.; Lu, Y.; Bahalim, A.N.; et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet 2011, 377, 557–567. [Google Scholar] [CrossRef]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Cournot, M.; Marquie, J.C.; Ansiau, D.; Martinaud, C.; Fonds, H.; Ferrieres, J.; Ruidavets, J.B. Relation between body mass index and cognitive function in healthy middle-aged men and women. Neurology 2006, 67, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Elias, M.F.; Elias, P.K.; Sullivan, L.M.; Wolf, P.A.; D’Agostino, R.B. Obesity, diabetes and cognitive deficit: The Framingham Heart Study. Neurobiol. Aging 2005, 26 (Suppl. 1), 11–16. [Google Scholar] [CrossRef]
- Fitzpatrick, A.L.; Kuller, L.H.; Lopez, O.L.; Diehr, P.; O’Meara, E.S.; Longstreth, W.T., Jr.; Luchsinger, J.A. Midlife and late-life obesity and the risk of dementia: Cardiovascular health study. Arch. Neurol. 2009, 66, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.; Mattson, M.P.; Maudsley, S. Caloric restriction and intermittent fasting: Two potential diets for successful brain aging. Ageing Res. Rev. 2006, 5, 332–353. [Google Scholar] [CrossRef]
- Mattson, M.P. The impact of dietary energy intake on cognitive aging. Front. Aging Neurosci. 2010, 2, 5. [Google Scholar] [CrossRef]
- Siervo, M.; Arnold, R.; Wells, J.C.; Tagliabue, A.; Colantuoni, A.; Albanese, E.; Brayne, C.; Stephan, B.C. Intentional weight loss in overweight and obese individuals and cognitive function: A systematic review and meta-analysis. Obes. Rev. 2011, 12, 968–983. [Google Scholar] [CrossRef]
- Prehn, K.; Jumpertz von Schwartzenberg, R.; Mai, K.; Zeitz, U.; Witte, A.V.; Hampel, D.; Szela, A.M.; Fabian, S.; Grittner, U.; Spranger, J.; et al. Caloric Restriction in Older Adults-Differential Effects of Weight Loss and Reduced Weight on Brain Structure and Function. Cereb. Cortex 2017, 27, 1765–1778. [Google Scholar] [CrossRef]
- Yu, J.; Zhou, X.; Li, L.; Li, S.; Tan, J.; Li, Y.; Sun, X. The long-term effects of bariatric surgery for type 2 diabetes: Systematic review and meta-analysis of randomized and non-randomized evidence. Obes. Surg. 2015, 25, 143–158. [Google Scholar] [CrossRef]
- Peirson, L.; Douketis, J.; Ciliska, D.; Fitzpatrick-Lewis, D.; Ali, M.U.; Raina, P. Prevention of overweight and obesity in adult populations: A systematic review. CMAJ Open 2014, 2, E268–E272. [Google Scholar] [CrossRef] [PubMed]
- Wittgrove, A.C.; Clark, G.W.; Tremblay, L.J. Laparoscopic Gastric Bypass, Roux-en-Y: Preliminary Report of Five Cases. Obes. Surg. 1994, 4, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Galioto, R.; Spitznagel, M.B.; Strain, G.; Devlin, M.; Cohen, R.; Crosby, R.D.; Mitchell, J.E.; Gunstad, J. Cognitive function after bariatric surgery: Evidence for improvement 3 years after surgery. Am. J. Surg. 2014, 207, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Gunstad, J.; Strain, G.; Devlin, M.J.; Wing, R.; Cohen, R.A.; Paul, R.H.; Crosby, R.D.; Mitchell, J.E. Improved memory function 12 weeks after bariatric surgery. Surg. Obes. Relat. Dis. 2011, 7, 465–472. [Google Scholar] [CrossRef]
- Marques, E.L.; Halpern, A.; Correa Mancini, M.; de Melo, M.E.; Horie, N.C.; Buchpiguel, C.A.; Martins Novaes Coutinho, A.; Ono, C.R.; Prando, S.; Santo, M.A.; et al. Changes in neuropsychological tests and brain metabolism after bariatric surgery. J. Clin. Endocrinol. Metab. 2014, 99, E2347–E2352. [Google Scholar] [CrossRef]
- Miller, L.A.; Crosby, R.D.; Galioto, R.; Strain, G.; Devlin, M.J.; Wing, R.; Cohen, R.A.; Paul, R.H.; Mitchell, J.E.; Gunstad, J. Bariatric surgery patients exhibit improved memory function 12 months postoperatively. Obes. Surg. 2013, 23, 1527–1535. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Helmstaedter, C.; Lendt, M.; Lux, S. Verbaler Lern-und Merkfähigkeitstest (VLMT); Beltz: Göttingen, Germany, 2001. [Google Scholar]
- Handley, J.D.; Williams, D.M.; Caplin, S.; Stephens, J.W.; Barry, J. Changes in Cognitive Function Following Bariatric Surgery: A Systematic Review. Obes. Surg. 2016, 26, 2530–2537. [Google Scholar] [CrossRef]
- Thiara, G.; Cigliobianco, M.; Muravsky, A.; Paoli, R.A.; Mansur, R.; Hawa, R.; McIntyre, R.S.; Sockalingam, S. Evidence for Neurocognitive Improvement After Bariatric Surgery: A Systematic Review. Psychosomatics 2017, 58, 217–227. [Google Scholar] [CrossRef]
- Georgiadou, E.; Gruner-Labitzke, K.; Kohler, H.; de Zwaan, M.; Muller, A. Cognitive function and nonfood-related impulsivity in post-bariatric surgery patients. Front. Psychol. 2014, 5, 1502. [Google Scholar] [CrossRef]
- Buchwald, H.; Avidor, Y.; Braunwald, E.; Jensen, M.D.; Pories, W.; Fahrbach, K.; Schoelles, K. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef]
- Alosco, M.L.; Spitznagel, M.B.; Strain, G.; Devlin, M.; Cohen, R.; Crosby, R.D.; Mitchell, J.E.; Gunstad, J. Improved serum leptin and ghrelin following bariatric surgery predict better postoperative cognitive function. J. Clin. Neurol. 2015, 11, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ashrafian, H.; le Roux, C.W. Metabolic surgery and gut hormones—A review of bariatric entero-humoral modulation. Physiol. Behav. 2009, 97, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; Moran, T.H.; Papantoni, A.; Speck, C.; Bakker, A.; Kamath, V.; Carnell, S.; Steele, K.E. Short-term improvements in cognitive function following vertical sleeve gastrectomy and Roux-en Y gastric bypass: A direct comparison study. Surg. Endosc. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R., Jr.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S., Jr. Compendium of physical activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Kobe, T.; Witte, A.V.; Schnelle, A.; Lesemann, A.; Fabian, S.; Tesky, V.A.; Pantel, J.; Floel, A. Combined omega-3 fatty acids, aerobic exercise and cognitive stimulation prevents decline in gray matter volume of the frontal, parietal and cingulate cortex in patients with mild cognitive impairment. Neuroimage 2016, 131, 226–238. [Google Scholar] [CrossRef]
- Prehn, K.; Lesemann, A.; Krey, G.; Witte, A.V.; Kobe, T.; Grittner, U.; Floel, A. Using resting-state fMRI to assess the effect of aerobic exercise on functional connectivity of the DLPFC in older overweight adults. Brain Cogn. 2019, 131, 34–44. [Google Scholar] [CrossRef]
- Nho, K.; Risacher, S.L.; Crane, P.K.; DeCarli, C.; Glymour, M.M.; Habeck, C.; Kim, S.; Lee, G.J.; Mormino, E.; Mukherjee, S.; et al. Voxel and surface-based topography of memory and executive deficits in mild cognitive impairment and Alzheimer’s disease. Brain Imaging Behav. 2012, 6, 551–567. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state” A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, CD011145. [Google Scholar] [CrossRef]
- Lezak, M.D. Neuropsychological Assessment, 4th ed.; Oxford University Press: Oxford, NY, USA, 2004. [Google Scholar]
- Reitan, R.M.; Wolfson, D. The Halstead–Reitan Neuropsychological Test Battery: Theory and Clinical Interpretation; Neuropsychology Press: Tuscon, AZ, USA, 1993. [Google Scholar]
- van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Dullemeijer, C.; Olderikkert, M.G.; Beekman, A.T.; de Groot, C.P. Effect of fish oil on cognitive performance in older subjects: A randomized, controlled trial. Neurology 2008, 71, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Mueller, K.; Moller, H.E.; Horstmann, A.; Busse, F.; Lepsien, J.; Bluher, M.; Stumvoll, M.; Villringer, A.; Pleger, B. Physical exercise in overweight to obese individuals induces metabolic- and neurotrophic-related structural brain plasticity. Front. Hum. Neurosci. 2015, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- Frey, I.; Berg, A.; Grathwohl, D.; Keul, J. [Freiburg Questionnaire of physical activity--development, evaluation and application]. Soz. Praventivmed. 1999, 44, 55–64. [Google Scholar] [CrossRef]
- Kuhner, C.; Burger, C.; Keller, F.; Hautzinger, M. Reliability and validity of the Revised Beck Depression Inventory (BDI-II). Results from German samples. Nervenarzt 2007, 78, 651–656. [Google Scholar] [CrossRef]
- Lehrl, S. Mehrfachwahl-Wortschatz-Intelligenztest MWT-B, 5th ed.; Spitta Verlag: Balingen, Germany, 2005. [Google Scholar]
- Tohka, J.; Zijdenbos, A.; Evans, A. Fast and robust parameter estimation for statistical partial volume models in brain MRI. Neuroimage 2004, 23, 84–97. [Google Scholar] [CrossRef]
- Rajapakse, J.C.; Giedd, J.N.; Rapoport, J.L. Statistical approach to segmentation of single-channel cerebral MR images. IEEE Trans. Med. Imaging 1997, 16, 176–186. [Google Scholar] [CrossRef]
- Cuadra, M.B.; Cammoun, L.; Butz, T.; Cuisenaire, O.; Thiran, J.-P. Comparison and validation of tissue modelization and statistical classification methods in T1-weighted MR brain images. IEEE Trans. Med. Imaging 2005, 24, 1548–1565. [Google Scholar] [CrossRef]
- Ashburner, J. A fast diffeomorphic image registration algorithm. Neuroimage 2007, 38, 95–113. [Google Scholar] [CrossRef]
- Freund, W.; Faust, S.; Gaser, C.; Gron, G.; Birklein, F.; Wunderlich, A.P.; Muller, M.; Billich, C.; Schutz, U.H. Regionally accentuated reversible brain grey matter reduction in ultra marathon runners detected by voxel-based morphometry. BMC Sports. Sci. Med. Rehabil. 2014, 6, 4. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Silver, M.; Montana, G.; Nichols, T.E. False positives in neuroimaging genetics using voxel-based morphometry data. Neuroimage 2011, 54, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Sterr, A. Is DARTEL-based voxel-based morphometry affected by width of smoothing kernel and group size? A study using simulated atrophy. J. Magn. Reson. Imaging 2013, 37, 1468–1475. [Google Scholar] [CrossRef]
- Hodgson, K.; Poldrack, R.A.; Curran, J.E.; Knowles, E.E.; Mathias, S.; Goring, H.H.H.; Yao, N.; Olvera, R.L.; Fox, P.T.; Almasy, L.; et al. Shared Genetic Factors Influence Head Motion During MRI and Body Mass Index. Cereb. Cortex 2017, 27, 5539–5546. [Google Scholar] [CrossRef] [PubMed]
- Makowski, C.; Lepage, M.; Evans, A.C. Head motion: The dirty little secret of neuroimaging in psychiatry. J. Psychiatry Neurosci. 2019, 44, 62–68. [Google Scholar] [CrossRef]
- Zeng, L.L.; Wang, D.; Fox, M.D.; Sabuncu, M.; Hu, D.; Ge, M.; Buckner, R.L.; Liu, H. Neurobiological basis of head motion in brain imaging. Proc. Natl. Acad. Sci. USA 2014, 111, 6058–6062. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Witte, A.V.; Fobker, M.; Gellner, R.; Knecht, S.; Floel, A. Caloric restriction improves memory in elderly humans. Proc. Natl. Acad. Sci. USA 2009, 106, 1255–1260. [Google Scholar] [CrossRef]
- Herpertz, S.; Muller, A.; Burgmer, R.; Crosby, R.D.; de Zwaan, M.; Legenbauer, T. Health-related quality of life and psychological functioning 9 years after restrictive surgical treatment for obesity. Surg. Obes. Relat. Dis. 2015, 11, 1361–1370. [Google Scholar] [CrossRef]
- Hawkins, M.A.; Alosco, M.L.; Spitznagel, M.B.; Strain, G.; Devlin, M.; Cohen, R.; Crosby, R.D.; Mitchell, J.E.; Gunstad, J. The Association Between Reduced Inflammation and Cognitive Gains After Bariatric Surgery. Psychosom. Med. 2015, 77, 688–696. [Google Scholar] [CrossRef][Green Version]
- Trachtenberg, J.T.; Chen, B.E.; Knott, G.W.; Feng, G.; Sanes, J.R.; Welker, E.; Svoboda, K. Long-term in vivo imaging of experience-dependent synaptic plasticity in adult cortex. Nature 2002, 420, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Zatorre, R.J.; Fields, R.D.; Johansen-Berg, H. Plasticity in gray and white: Neuroimaging changes in brain structure during learning. Nat. Neurosci. 2012, 15, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Tuulari, J.J.; Karlsson, H.K.; Antikainen, O.; Hirvonen, J.; Pham, T.; Salminen, P.; Helmio, M.; Parkkola, R.; Nuutila, P.; Nummenmaa, L. Bariatric Surgery Induces White and Grey Matter Density Recovery in the Morbidly Obese: A Voxel-Based Morphometric Study. Hum. Brain Mapp. 2016, 37, 3745–3756. [Google Scholar] [CrossRef] [PubMed]
- Rullmann, M.; Preusser, S.; Poppitz, S.; Heba, S.; Hoyer, J.; Schutz, T.; Dietrich, A.; Muller, K.; Pleger, B. Gastric-bypass surgery induced widespread neural plasticity of the obese human brain. Neuroimage 2018, 172, 853–863. [Google Scholar] [CrossRef]
- Liu, L.; Ji, G.; Li, G.; Hu, Y.; Jin, Q.; Hu, C.; Zhao, J.; Meng, Q.; von Deneen, K.M.; Chen, A.; et al. Structural changes in brain regions involved in executive-control and self-referential processing after sleeve gastrectomy in obese patients. Brain Imaging Behav. 2019, 13, 830–840. [Google Scholar] [CrossRef]
- Horstmann, A.; Busse, F.P.; Mathar, D.; Muller, K.; Lepsien, J.; Schlogl, H.; Kabisch, S.; Kratzsch, J.; Neumann, J.; Stumvoll, M.; et al. Obesity-Related Differences between Women and Men in Brain Structure and Goal-Directed Behavior. Front. Hum. Neurosci. 2011, 5, 58. [Google Scholar] [CrossRef]
- Kenny, P.J. Reward mechanisms in obesity: New insights and future directions. Neuron 2011, 69, 664–679. [Google Scholar] [CrossRef]
- Coveleskie, K.; Gupta, A.; Kilpatrick, L.A.; Mayer, E.D.; Ashe-McNalley, C.; Stains, J.; Labus, J.S.; Mayer, E.A. Altered functional connectivity within the central reward network in overweight and obese women. Nutr. Diabetes 2015, 5, e148. [Google Scholar] [CrossRef]
- Rothemund, Y.; Preuschhof, C.; Bohner, G.; Bauknecht, H.C.; Klingebiel, R.; Flor, H.; Klapp, B.F. Differential activation of the dorsal striatum by high-calorie visual food stimuli in obese individuals. Neuroimage 2007, 37, 410–421. [Google Scholar] [CrossRef]
- Backman, O.; Stockeld, D.; Rasmussen, F.; Naslund, E.; Marsk, R. Alcohol and substance abuse, depression and suicide attempts after Roux-en-Y gastric bypass surgery. Br. J. Surg. 2016, 103, 1336–1342. [Google Scholar] [CrossRef]
- Musselman, D.; Shenvi, N.; Manatunga, A.; Miller, A.H.; Lin, E.; Gletsu-Miller, N. The effects of roux en y gastric bypass surgery on neurobehavioral symptom domains associated with severe obesity. Physiol. Behav. 2019, 204, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Ochner, C.N.; Kwok, Y.; Conceicao, E.; Pantazatos, S.P.; Puma, L.M.; Carnell, S.; Teixeira, J.; Hirsch, J.; Geliebter, A. Selective reduction in neural responses to high calorie foods following gastric bypass surgery. Ann. Surg. 2011, 253, 502–507. [Google Scholar] [CrossRef]
- van de Sande-Lee, S.; Pereira, F.R.; Cintra, D.E.; Fernandes, P.T.; Cardoso, A.R.; Garlipp, C.R.; Chaim, E.A.; Pareja, J.C.; Geloneze, B.; Li, L.M.; et al. Partial reversibility of hypothalamic dysfunction and changes in brain activity after body mass reduction in obese subjects. Diabetes 2011, 60, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ji, G.; Xu, M.; Cai, W.; Zhu, Q.; Qian, L.; Zhang, Y.E.; Yuan, K.; Liu, J.; Li, Q.; et al. Recovery of brain structural abnormalities in morbidly obese patients after bariatric surgery. Int. J. Obes. 2016, 40, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Sherf Dagan, S.; Goldenshluger, A.; Globus, I.; Schweiger, C.; Kessler, Y.; Kowen Sandbank, G.; Ben-Porat, T.; Sinai, T. Nutritional Recommendations for Adult Bariatric Surgery Patients: Clinical Practice. Adv. Nutr. 2017, 8, 382–394. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| (a) Whole Sample | |||
| NBARS Group | BARS Group | p | |
| n | 29 | 40 | |
| Age (years) | 45 (12) | 46 (11) | 0.61 |
| Gender (% women) | 55.2 | 70.0 | 0.21 a |
| Weight (kg) | 133.2 (22.6) | 140.9 (29.3) | 0.24 |
| BMI (kg/m2) | 44.6 (5.7) | 49.2 (7.7) | 0.01 |
| Education (years) | 16 (3) | 15 (4) | 0.66 |
| Verbal intelligence (vocabulary test score) | 29.8 (3.4) | 29.7 (3.11) | 0.66 |
| BDI (Beck’s depression inventory score) | 14.6 (7.3) c | 13.1 (9.3) b | 0.51 |
| Fasting glucose (mg/dL) | 117.8 (33.2) d | 127.4 (62.5) | 0.46 |
| HbA1c (%) | 6.1 (1.0) d | 6.3 (1.1) | 0.44 |
| (b) MRI Sample | |||
| NBARS Group | BARS Group | p | |
| n | 14 | 13 | |
| Age (years) | 47 (12) | 41 (11) | 0.15 |
| Gender (% women) | 57.1 | 84.6 | 0.12 a |
| Weight (kg) | 123.7 (14.9) | 123.8 (16.4) | 0.98 |
| BMI (kg/m2) | 42.5 (4.7) | 44.5 (5.6) | 0.30 |
| Education (years) | 15.5 (2.3) | 15.3 (3.0) | 0.88 |
| Verbal intelligence (vocabulary test score) | 30.2 (3.3) | 29.5 (2.5) | 0.56 |
| BDI (Beck’s depression inventory score) | 16.2 (6.6) d | 17.3 (13.2) | 0.78 |
| Fasting glucose (mg/dL) | 113.8 (26.6) d | 130.8 (93.6) | 0.54 |
| HbA1c (%) | 6.0 (1.1) d | 6.2 (1.1) | 0.70 |
| (c) Comparison of Surgical Procedures | |||
| VSG/GB Group | RYGB Group | p | |
| n | 23 | 17 | |
| Age (years) | 47 (11) | 45 (10) | 0.71 |
| Gender (% women) | 57 | 88 | 0.03 a |
| Weight (kg) | 147.8 (29.3) | 131.6 (27.5) | 0.08 |
| BMI (kg/m2) | 50.2 (8.5) | 47.7 (6.5) | 0.31 |
| Education (years) | 15 (4) | 16 (4) | 0.29 |
| Verbal intelligence (vocabulary test score) | 30.2 (2.5) | 29.1 (3.8) | 0.25 |
| BDI (Beck’s depression inventory score) | 14.0 (9.1) d | 11.9 (9.7) d | 0.51 |
| Fasting glucose (mg/dL) | 133.8 (79.2) | 118.7 (27.7) | 0.46 |
| HbA1c (%) | 6.3 (1.1) | 6.2 (1.0) | 0.66 |
| Within Groups | Between Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NBARS Group (n = 29) | BARS Group (n = 40) | Results of the Multiple Linear Regression | ||||||||
| t1 | t2 | p | t1 | t2 | p | ß | 95% CI | ηp2 | p | |
| Anthropometric Parameters | ||||||||||
| Weight (kg) | 133.2 (22.6) | 133.5 (21.6) | 0.81 | 141.0 (29.7) | 111.0 (25.6) | <0.001 a | −28.5 | (−33.0, −23.9) | 0.72 | <0.001 |
| BMI (kg/m2) | 44.6 (5.7) | 44.7 (5.3) | 0.84 | 49.3 (7.8) | 38.8 (7.4) | <0.001 a | −9.9 | (−11.3, −8.4) | 0.74 | <0.001 |
| Body fat percentage (%) | 44.6 (8.1) | 43.9 (7.9) | 0.37 a | 46.6 (9.5) | 40.3 (7.8) | <0.001 a | −6.1 | (−8.3, −3.9) | 0.34 | <0.001 |
| Systolic blood pressure (mm Hg) | 133.3 (15.1) | 130.9 (12.5) | 0.27 b | 136.3 (15.0) | 126.2 (11.8) | <0.001 c | −7.1 | (−12.2, −2.0) | 0.12 | 0.01 |
| Diastolic blood pressure (mm Hg) | 90.4 (13.1) | 88.2 (9.9) | 0.23 b | 89.0 (10.0) | 83.3 (10.0) | <0.001 d | −4.3 | (−8.6, 0.0) | 0.07 | 0.05 |
| Serum levels | ||||||||||
| Fasting glucose (mg/dL) | 119.2 (34.0) | 114.9 (19.3) | 0.40 c | 127.4 (62.5) | 110.8 (41.0) | 0.01 | −10.3 | (−17.4, −3.1) | 0.12 | 0.01 |
| HbA1c (%) | 6.1 (1.0) | 5.8 (0.6) | 0.08 b | 6.3 (1.1) | 5.9 (1.1) | <0.001 | −6.1 | (−14.7, 2.6) | 0.03 | 0.17 |
| Fasting insulin (µU/mL) | 25.5 (17.4) | 27.0 (13.2) | 0.49 b | 29.2 (19.6) | 12.4 (7.8) | <0.001 a | −16.4 | (−21.1, −11.8) | 0.45 | <0.001 |
| HOMA-index | 7.9 (6.5) | 8.1 (4.5) | 0.84 c | 9.1 (7.1) | 3.3 (2.3) | <0.001 b | −5.2 | (−7.2, −3.3) | 0.34 | <0.001 |
| Triacylglycerides (mg/dL) | 150.0 (59.0) | 155.7 (71.5) | 0.53 b | 176.8 (82.1) | 129.5 (42.5) | <0.001 | −13.0 | (−21.7, −4.3) | 0.13 | 0.004 |
| Total cholesterol (mg/dL) | 191.9 (35.1) | 185.6 (32.3) | 0.22 b | 194.1 (36.3) | 182.5 (36.3) | 0.02 | −6.4 | (−20.5, 7.8) | 0.01 | 0.37 |
| LDL-to-HDL ratio | 2.8 (1.2) | 2.6 (1.0) | 0.12 b | 2.6 (0.8) | 2.4 (0.7) | 0.01 | −0.1 | (−0.5, 0.2) | 0.01 | 0.39 |
| TNF-α (pg/mL) | 7.5 (2.1) | 8.0 (2.7) | 0.22 b | 10.1 (4.0) | 8.4 (3.7) | 0.01 a | −1.0 | (−2.6, 0.6) | 0.03 | 0.21 |
| IL-6 (pg/mL | 3.2 (1.5) | 3.7 (2.0) | 0.11 b | 3.6 (1.8) | 2.8 (1.0) | <0.001 a | −1.2 | (−2.0, −0.4) | 0.13 | 0.004 |
| hsCRP (mg/L) | 8.5 (6.9) | 9.5 (8.1) | 0.28 b | 12.9 (11.6) | 7.0 (7.8) | <0.001 | −19.7 | (−27.8, −11.7) | 0.28 | <0.001 |
| Leptin (ng/mL) | 12.7 (7.6) | 17.0 (11.5) | 0.02 c | 22.7 (11.8) | 12.7 (12.0) | <0.001 a | −11.9 | (−17.7, −6.2) | 0.22 | <0.001 |
| Test Scores | ||||||||||
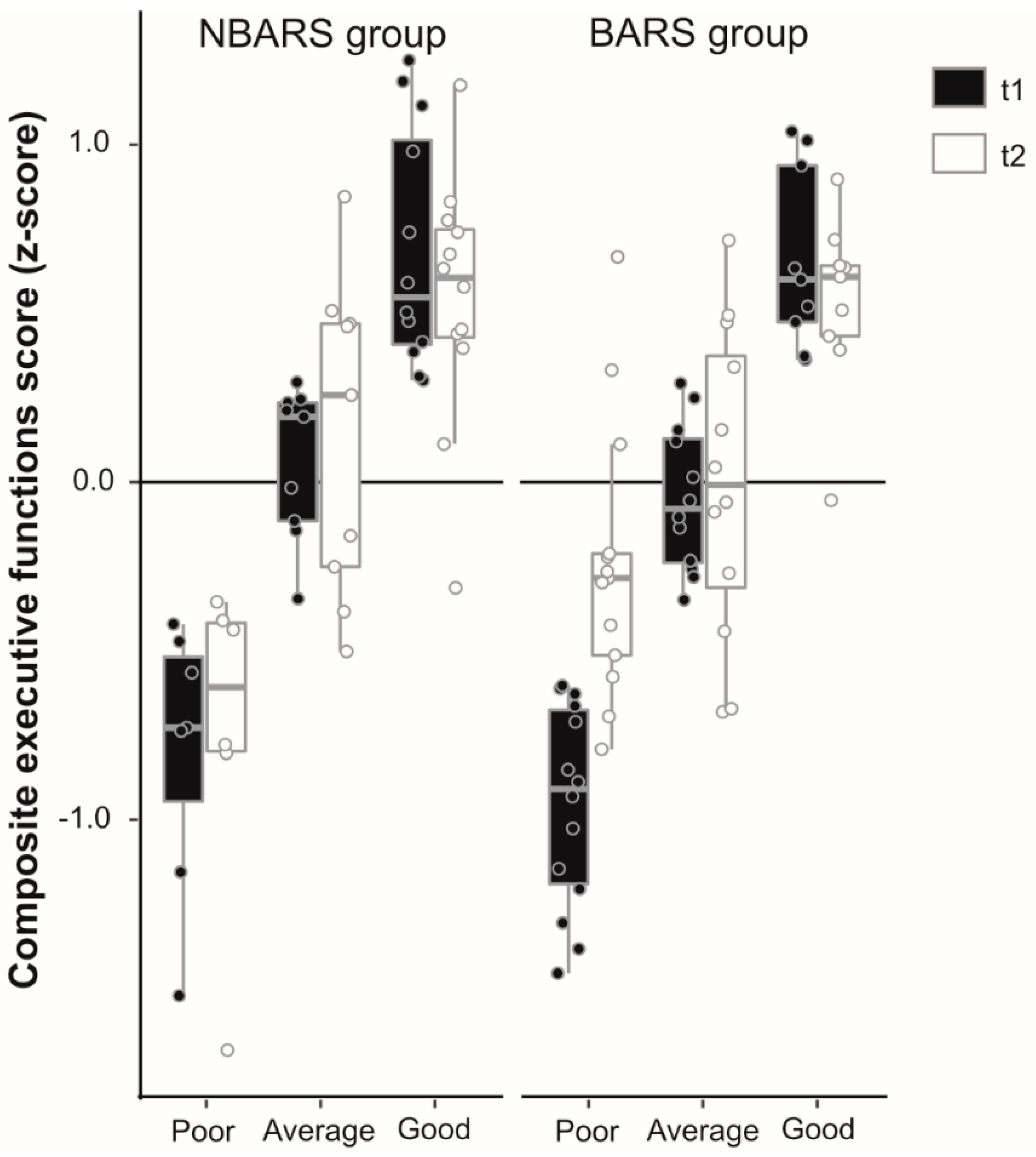
| Executive functions (z-scores) | 0.18 (0.6) | 0.12 (0.7) | 0.51 b | −0.21 (0.7) | 0.05 (0.5) | 0.01 e | 0.2 | (−0.1, 0.4) | 0.04 | 0.13 |
| Memory (z-scores) | 0.09 (0.8) | 0.15 (0.6) | 0.67 | −0.08 (0.9) | −0.08 (0.8) | 0.95 | −0.1 | (−0.4, 0.2) | 0.01 | 0.5 |
| Sensomotoric speed (z-scores) | −0.18 (0.7) | −0.02 (0.8) | 0.26 a | 0.02 (0.9) | 0.12 (0.8) | 0.3 | 0.1 | (0.3, 0.4) | 0 | 0.74 |
| Attention (z-scores) | 0.19 (1.2) | 0.12 (1.1) | 0.73 | −0.15 (0.9) | −0.07 (0.9) | 0.6 | −0.05 | (−0.5, 0.4) | 0 | 0.84 |
| PANAS + | 29.14 (6.9) | 29.55 (5.8) | 0.63 | 32.26 (7.5) | 32.54 (7.6) | 0.77 a | 0.1 | (−2.4, 2.6) | 0 | 0.94 |
| PANAS − | 14.07 (4.9) | 13.90 (4.2) | 0.81 | 11.90 (1.6) | 11.73 (0.7) | 0.7 | 0.1 | (−1.5, 1.6) | 0 | 0.91 |
| STAI state anxiety | 36.93 (88.5) | 38.83 (8.8) | 0.22 | 36.53 (9.1) | 33.00 (7.5) | 0.02 | −4.7 | (−8.3, −1.1) | 0.1 | 0.01 |
| STAI trait anxiety | 44.18 (11.9) | 43.09 (13.2) | 0.53 f | 43.33 (11.0) | 38.13 (10.6) | 0.02 g | −3.4 | (−8.5, 1.7) | 0.04 | 0.18 |
| BDI | 14.57 (7.5) | 13.87 (10.4) | 0.63 e | 13.24 (9.9) | 6.39 (8.1) | <0.001 f | −6.5 | (−10.4, −2.5) | 0.18 | 0.002 |
| SF-12 physiologic | 39.44 (11.2) | 40.23 (11.4) | 0.67 g | 34.31 (10.8) | 45.21 (10.3) | <0.001 g | 9.2 | (4.0, 14.3) | 0.23 | 0.001 |
| SF-12 psychologic | 45.65 (11.8) | 45.81 (12.8) | 0.96 g | 47.27 (12.4) | 51.18 (11.6) | 0.18 g | 1.3 | (−5.4, 8.0) | 0 | 0.7 |
| FKA | 2.70 (1.6) | 2.05 (1.1) | 0.03 h | 2.58 (1.5) | 2.84 (1.2) | 0.26 h | 0.9 | (0.2, 1.5) | 0.15 | 0.01 |
| Anatomical Region | L/R | Number of Voxels in Cluster | Z score of Local Maximum | MNI Peak Voxel Coordinates | ||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| (a) Group x Time interactions | ||||||
| BARS group > NBARS groupt2>t1 (indicating an increase of volume in the surgery compared to the control group) | ||||||
| Superior temporal gyrus, insula, inferior frontal gyrus | L | 3566 | 3.97 | −44 | −13 | −3 |
| BARS group > NBARS groupt1>t2 (indicating a decrease of volume in the surgery compared to the control group) | ||||||
| Nucleus accumbens * | L | 78 | 3.32 | −8 | 6 | −6 |
| (b) Within surgery group comparisons | ||||||
| BARS groupt2>t1 (indicating an increase) | ||||||
| Middle occipital gyrus, supramarginal gyrus | L | 3175 | 3.74 | −30 | −70 | 25 |
| BARS groupt1>t2 (indicating a decrease) | ||||||
| No ROI, nucleus putamen | L | 8877 | 4.84 | −9 | 4 | −15 |
| Supramarginal gyrus, cerebellum | R | 2586 | 4.43 | 62 | −42 | 30 |
| No ROI, medial inferior occipital cortex | L | 3004 | 3.85 | −26 | −102 | −9 |
| (c) Within control group comparisons | ||||||
| NBARS groupt2>t1 (indicating an increase) | No suprathreshold clusters | |||||
| NBARS groupt1>t2 (indicating a decrease) | No suprathreshold clusters | |||||
| Within Groups | Between Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| VSG/GB Group (n = 23) | RYGB Group (n = 17) | Results of the Multiple Linear Regression | ||||||||
| t1 | t2 | p | t1 | t2 | p | ß | 95% CI | ηp2 | p | |
| Anthropometric Parameters | ||||||||||
| Weight (kg) | 148.3 (29.8) | 120.0 (24.6) | <0.001 a | 131.6 (27.5) | 99.44 (22.4) | <0.001 | −6.7 | (−12.8, −0.6) | 0.13 | 0.03 |
| BMI (kg/m2) | 50.5 (8.6) | 41.0 (7.9) | <0.001 a | 47.7 (6.5) | 36.0 (5.6) | <0.001 | −2.3 | (−4.2, −0.4) | 0.15 | 0.02 |
| Body fat percentage (%) | 44.3 (11.3) | 39.4 (9.2) | 0.001 a | 49.5 (5.2) | 41.4 (5.6) | <0.001 | −0.8 | (−3.7, 2.1) | 0.01 | 0.59 |
| Systolic blood pressure (mm Hg) | 135.3 (13.8) | 128.1 (10.5) | 0.02 a | 137.7 (17.1) | 123.6 (13.4) | <0.001 b | −5.4 | (−12.0, 1.2) | 0.08 | 0.11 |
| Diastolic blood pressure (mm Hg) | 87.6 (9.8) | 84.2 (9.7) | 0.06 a | 90.0 (10.7) | 81.5 (10.3) | 0.002 b | −4.2 | (−9.9, 1.5) | 0.07 | 0.14 |
| Serum Levels | ||||||||||
| Fasting glucose (mg/dL) | 133.8 (79.2) | 113.8 (49.3) | 0.02 | 118.7 (27.7) | 106.7 (27.0) | 0.18 | 1.1 | (−3.7, 5.9) | 0.01 | 0.65 |
| HbA1c (%) | 6.3 (1.1) | 6.0 (1.2) | 0.001 | 6.2 (1.0) | 5.8 (0.8) | 0.003 | −0.1 | (−0.4, 0.2) | 0.01 | 0.56 |
| Fasting insulin (µU/mL) | 29.0 (20.1) | 13.7 (8.5) | <0.001 | 29.6 (19.6) | 10.27 (6.2) | <0.001 a | −3.8 | (−6.9, −0.7) | 0.16 | 0.02 |
| HOMA-index | 8.8 (6.7) | 3.7 (2.1) | <0.001 a | 9.4 (7.8) | 2.8 (2.5) | <0.001 a | −3.0 | (−4.8, −1.2) | 0.26 | 0.002 |
| Triacylglycerides (mg/dL) | 200.1 (91.6) | 141.7 (45.2) | 0.01 | 145.2 (55.3) | 112.9 (32.9) | <0.001 | −2.5 | (−7.8, 2.7) | 0.03 | 0.34 |
| Total cholesterol (mg/dL) | 197.9 (40.4) | 193.7 (35.9) | 0.49 | 189.0 (30.1) | 167.4 (32.0) | 0.01 | −20.6 | (−38.7, −2.5) | 0.13 | 0.03 |
| LDL-to-HDL ratio | 2.7 (0.8) | 2.5 (0.7) | 0.16 | 2.5 (0.9) | 2.2 (0.7) | 0.04 | −0.2 | (−0.6, 0.1) | 0.04 | 0.22 |
| TNF-α (pg/mL) | 10.3 (3.7) | 8.3 (3.0) | 0.03 | 9.7 (4.4) | 8.6 (4.6) | 0.07 a | 0.8 | (−1.3, 2.9) | 0.02 | 0.45 |
| IL-6 (pg/mL | 3.7 (2.1) | 2.8 (1.1) | 0.02 | 3.4 (1.3) | 2.7 (0.9) | 0.02 a | −1.1 | (−6.5, 4.4) | 0.01 | 0.69 |
| hsCRP (mg/L) | 12.6 (10.8) | 8.0 (8.6) | 0.003 | 13.3 (13.0) | 5.5 (6.4) | 0.003 | −2.9 | (−8.7, 3.0) | 0.03 | 0.32 |
| Leptin (ng/mL) | 23.7 (13.3) | 15.2 (13.6) | 0.002 a | 21.4 (9.7) | 9.4 (8.7) | <0.001 | −4.4 | (−11.0, 2.1) | 0.05 | 0.18 |
| Test Scores | ||||||||||
| Executive functions (z-scores) | −0.10 (0.7) | 0.20 (0.6) | 0.03 c | −0.15 (0.8) | 0.06 (0.5) | 0.17 a | −0.2 | (−0.4, 0.1) | 0.04 | 0.3 |
| Memory (z-scores) | −0.23 (0.8) | −0.23 (0.8) | 0.98 | 0.31 (0.9) | 0.32 (0.5) | 0.96 | 5.1 | (−1.6, 11.7) | 0.07 | 0.13 |
| Sensomotoric speed (z-scores) | −0.07 (1.0) | 0.03 (0.8) | 0.92 | −0.01 (0.7) | 0.07 (0.7) | 0.88 | −0.0 | (−0.4, 0.3) | 0 | 0.84 |
| Attention (z-scores) | −0.22 (1.0) | −0.20 (0.9) | 0.92 | 0.19 (0.9) | 0.37 (1.1) | 0.47 | 0.4 | (−0.2, 1.0) | 0.05 | 0.21 |
| PANAS + | 33.04 (8.2) | 33.96 (8.6) | 0.5 | 31.13 (6.5) | 30.50 (5.6) | 0.63 a | −2.2 | (−5.7, 1.3) | 0.05 | 0.22 |
| PANAS − | 12.09 (1.8) | 11.04 (1.5) | 0.01 | 11.65 (1.3) | 12.65 (4.0) | 0.27 | 5.4 | (−1.0, 11.7) | 0.08 | 0.1 |
| STAI state anxiety | 35.96 (9.3) | 30.78 (7.2) | 0.01 | 37.29 (9.1) | 36.00 (6.9) | 0.55 | 3.8 | (−0.5, 8.1) | 0.09 | 0.08 |
| STAI trait anxiety | 43.20 (12.5) | 35.93 (10.4) | 0.01 | 42.71 (9.6) | 41.43 (10.2) | 0.58 d | 5.8 | (−0.5, 12.0) | 0.13 | 0.07 |
| BDI | 14.50 (10.6) | 6.88 (8.8) | 0.001 | 11.94 (9.7) | 6.25 (7.7) | 0.01 a | −0.2 | (−4.6, 4.2) | 0 | 0.92 |
| SF-12 physiologic | 31.72 (8.1) | 45.61 (8.7) | <0.001 | 38.07 (13.1) | 43.93 (12.2) | 0.04 e | −5.4 | (−11.9, 1.0) | 0.11 | 0.1 |
| SF-12 psychologic | 47.55 (13.5) | 51.98 (11.4) | 0.23 | 48.00 (11.3) | 49.69 (12.5) | 0.57 e | −0.9 | (−8.3, 6.5) | 0 | 0.8 |
| FKA | 2.94 (1.6) | 3.19 (1.4) | 0.43 | 2.20 (1.4) | 2.47 (1.0) | 0.43 b | −0.3 | (−1.1, 0.5) | 0.02 | 0.47 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prehn, K.; Profitlich, T.; Rangus, I.; Heßler, S.; Witte, A.V.; Grittner, U.; Ordemann, J.; Flöel, A. Bariatric Surgery and Brain Health—A Longitudinal Observational Study Investigating the Effect of Surgery on Cognitive Function and Gray Matter Volume. Nutrients 2020, 12, 127. https://doi.org/10.3390/nu12010127
Prehn K, Profitlich T, Rangus I, Heßler S, Witte AV, Grittner U, Ordemann J, Flöel A. Bariatric Surgery and Brain Health—A Longitudinal Observational Study Investigating the Effect of Surgery on Cognitive Function and Gray Matter Volume. Nutrients. 2020; 12(1):127. https://doi.org/10.3390/nu12010127
Chicago/Turabian StylePrehn, Kristin, Thorge Profitlich, Ida Rangus, Sebastian Heßler, A. Veronica Witte, Ulrike Grittner, Jürgen Ordemann, and Agnes Flöel. 2020. "Bariatric Surgery and Brain Health—A Longitudinal Observational Study Investigating the Effect of Surgery on Cognitive Function and Gray Matter Volume" Nutrients 12, no. 1: 127. https://doi.org/10.3390/nu12010127
APA StylePrehn, K., Profitlich, T., Rangus, I., Heßler, S., Witte, A. V., Grittner, U., Ordemann, J., & Flöel, A. (2020). Bariatric Surgery and Brain Health—A Longitudinal Observational Study Investigating the Effect of Surgery on Cognitive Function and Gray Matter Volume. Nutrients, 12(1), 127. https://doi.org/10.3390/nu12010127