Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression


Abstract
1. Introduction
2. Materials and Methods
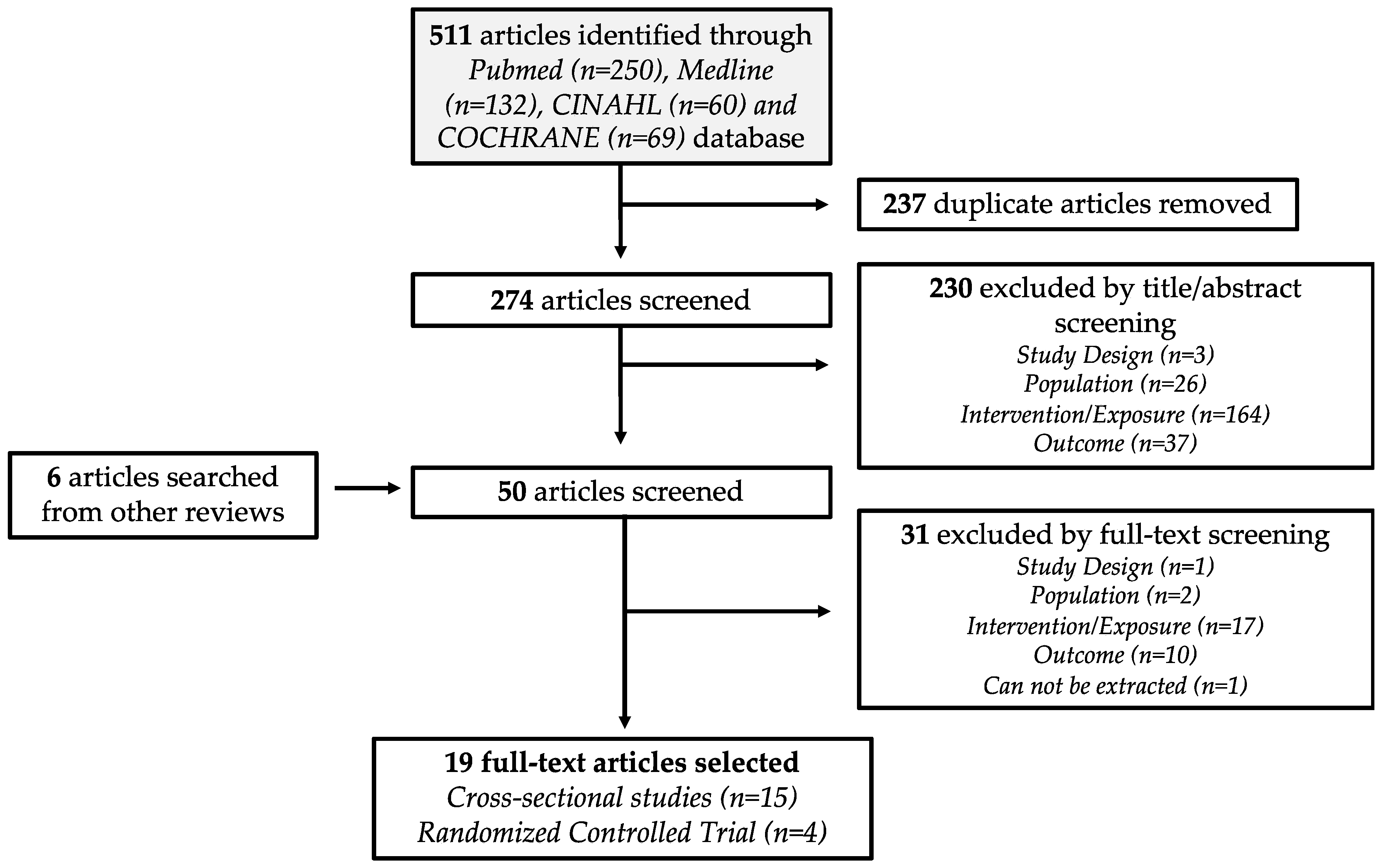
2.1. Search Strategy
2.2. Study Delection
2.3. Data Extraction
2.4. Sleep Quality Analysis
2.5. Dietary Analysis
2.6. Quality Assessment
2.7. Meta-Regression
3. Results
3.1. Study Characteristics
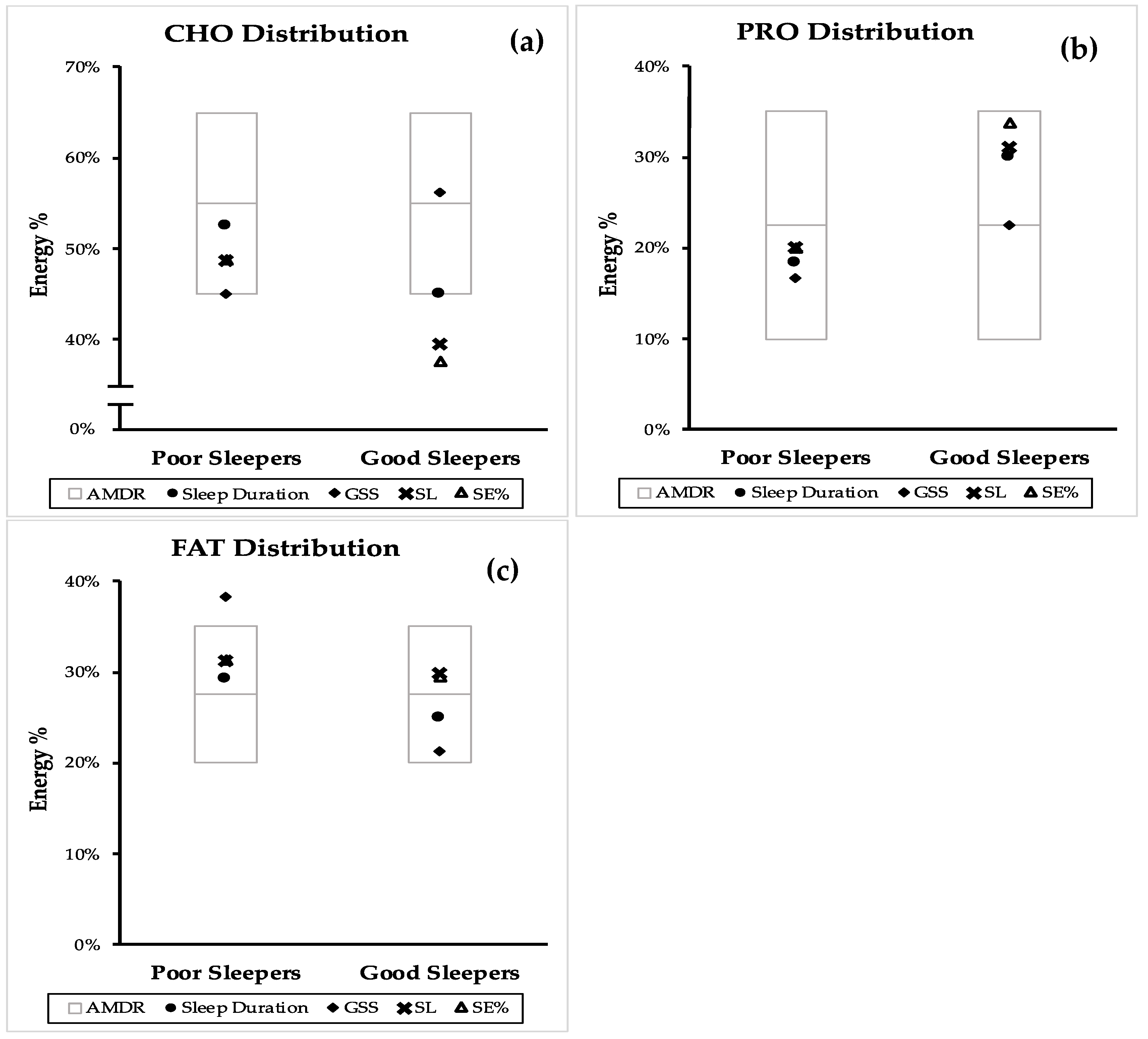
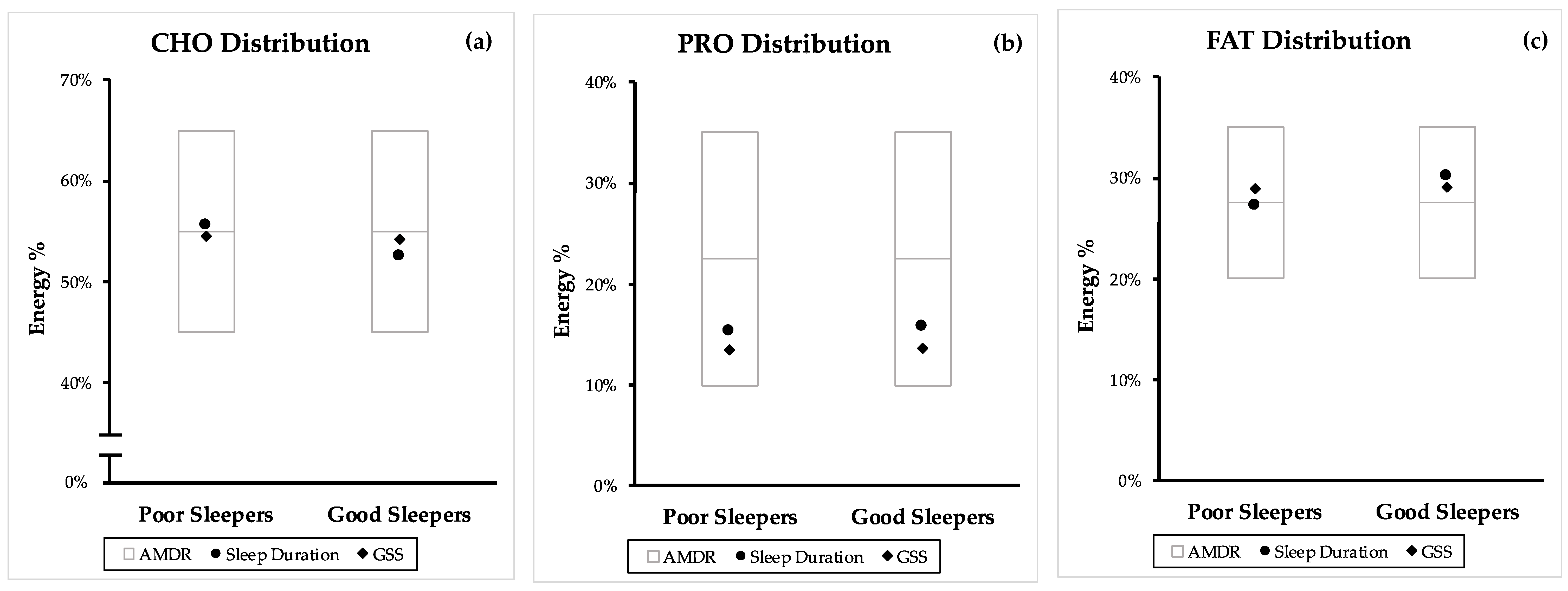
3.2. Macronutrient Distribution and Sleep Quality
3.3. Acceptable Macronutrient Distribution Range and Sleep Quality
3.4. Quality Assessment
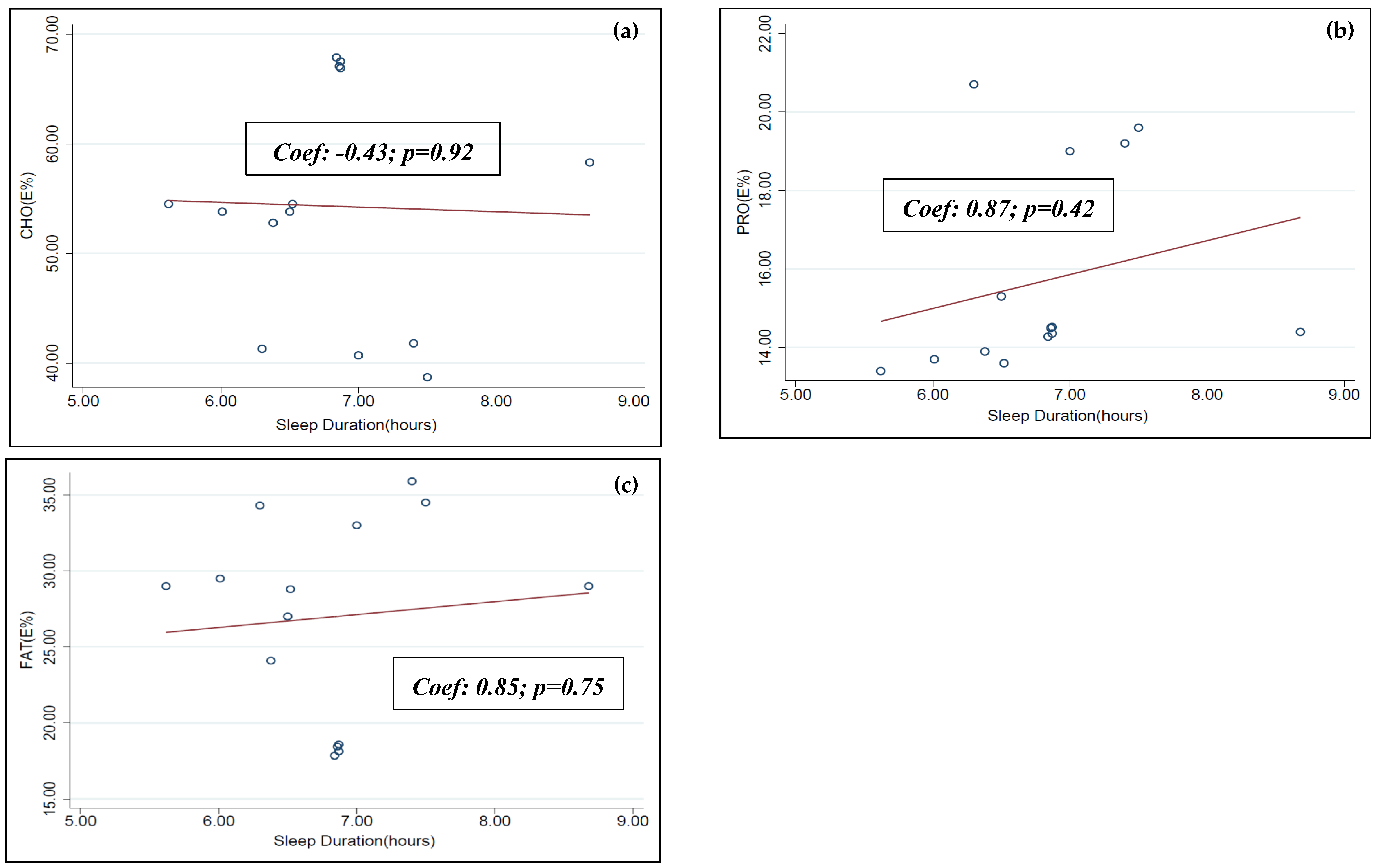
3.5. Meta-Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AANAT | Serotonin N-acetyltransferase |
| AMDR | Acceptable macronutrient distribution range |
| BBB | Blood brain barrier |
| BDHQ | Brief diet history questionnaire |
| CD | Cannot be determined |
| CHO | Dietary carbohydrate |
| CS | Cross-sectional studies |
| DHQ | Dietary History Questionnaires |
| E% | Percentage of energy intake |
| ER | Energy restricted |
| FAA | Food anticipatory activity |
| FAO | Food and Agriculture Organization of the United Nations |
| FAT | Dietary fat |
| FFQ | Food frequency questionnaire |
| GSS | Global sleep score |
| LNAA | Large neutral amino acids |
| NA | Not applicable |
| NCD | Non-communicable diseases |
| NHLBI | National Heart, Lung and Blood Institute |
| NR | Not reported |
| NREM | Non-rapid eye movement |
| NSF | National Sleep Foundation |
| PRO | Dietary protein |
| PRO:CHO ratio | Protein: carbohydrate ratio |
| PSQI | Pittsburgh Sleep Quality Index |
| REM | Rapid eye movement |
| RCT | Randomized controlled trial |
| SCN | Suprachiasmatic nucleus |
| SL | Sleep latency |
| SE% | Sleep efficiency |
| QACIS | Quality Assessment of Controlled Intervention Studies |
| QATOCC | Quality Assessment Tool for Observational Cohort and Cross-sectional Studies |
| WHO | World Health Organization |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Filter | Results Yielded |
|---|---|---|---|
| PubMed | (sleep [MeSH] OR “sleep”) AND (dietary proteins [MeSH] OR dietary fats [MeSH] OR dietary carbohydrates [MeSH] OR “macronutrients” OR “macronutrient”) | Human English Adult (19+) | 250 |
| Medline (Ovid) | (sleep [MeSH] OR “sleep”) AND (dietary proteins [MeSH] OR dietary fats [MeSH] OR dietary carbohydrates [MeSH] OR “macronutrients” OR “macronutrient”) | Human Adult (19+) | 132 |
| CINAHL | ((MH "Dietary Fats+") OR (MH "Dietary Proteins+") OR (MH "Dietary Carbohydrates+") OR "Macronutrients" OR "Macronutrient") AND sleep | Human English Adult (19+) | 60 |
| Cochrane | (sleep [MeSH]) AND (dietary proteins [MeSH] OR dietary fats [MeSH] OR dietary carbohydrates [MeSH] OR “macronutrients” OR “macronutrient”) | - | 69 |
| Total | 511 | ||
| Parameter | Description |
|---|---|
| Population | Adult 19+ y/o (mean age) |
| Intervention/Exposure | Groups which consume high carbs, proteins OR fats |
| Comparison | Groups which consume low carbs, proteins OR fats respectively |
| Outcome | Sleep duration, PSQI Score, REM/NREM duration, Polysomnography sleep measurements |
| Setting | Observational study & RCT |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shi et al., 2008 [27] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 0 | 6 |
| Haghighatdoost et al., 2012 [28] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 0 | 5 |
| Santana et al., 2012 [29] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | CD* | 0 | 0 (NR) | NA | 0 | 5 |
| Grandner et al., 2013 [30] | 1 | 1 | 1 | 1 | 0 | 0 | NA | 1 | 1 | 0 | 1 | 0 (NR) | NA | 1 | 8 |
| Kant & Graubard, 2014 [31] | 1 | 1 | 1 | 0 | 0 | 0 | NA | 1 | 1 | 0 | 0 | 0 (NR) | NA | 1 | 6 |
| Katagiri et al., 2014 [32] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | 1 | 1 | 0 (NR) | NA | 1 | 8 |
| Poggiogalle et al., 2016 [33] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | 1 | 1 | 0 (NR) | NA | 1 | 8 |
| Doo & Kim, 2016 [34] | 1 | 1 | 1 | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 1 | 8 |
| Doo et al., 2016 [35] | 1 | 1 | 1 | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 1 | 8 |
| Heath et al., 2016 [36] | 1 | 1 | 0 (NR) | 1 | 0 | 0 | NA | 1 | 1 | 1 | 1 | 0 (NR) | NA | 1 | 8 |
| Doo & Kim, 2016 [37] | 1 | 1 | 1 | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 1 | 8 |
| Bennett et al., 2017 [38] | 1 | 1 | 1 | 1 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 1 | 8 |
| Spaeth et al., 2017 [39] | 1 | 1 | 0 (NR) | 0 (NR) | 0 | 0 | NA | 1 | 1 | 1 | 1 | 0 (NR) | NA | CD* | 6 |
| Komada et al., 2017 [40] | 1 | 1 | 0 (NR) | 0 (NR) | 0 | 0 | NA | 1 | 1 | 1 | 1 | 0 (NR) | NA | 1 | 7 |
| Liu et al., 2018 [41] | 1 | 1 | 0 (NR) | 0 | 0 | 0 | NA | 1 | 1 | 1 | 0 | 0 (NR) | NA | 1 | 6 |
| Total Score of each question | 15 | 15 | 7 | 11 | 0 | 0 | NA | 15 | 15 | 12 | 6 | 0 | NA | 12 |
| Citation | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lindseth et al., 2013 [41] | 1 | 1 | 1 | 1 | 1 | 1 | 0 (NR) | 1 | 0 (NR) | 1 | 1 | 1 | 1 | 1 | 12 |
| Karl et al., 2015 [42] | 1 | 0 | 0 | 0 | 0 | 1 | 0 (NR) | 1 | 0 (NR) | 1 | 1 | 0 | 1 | 1 | 7 |
| Lindseth & Murray, 2016 [18] | 1 | 1 | 1 | 1 | 0 | 1 | 0 (NR) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Zhou et al., 2016 [17] | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Total Score of each question | 4 | 3 | 2 | 2 | 1 | 4 | 0 | 4 | 2 | 4 | 4 | 3 | 4 | 4 |



References
- Laposky, A.D.; Bass, J.; Kohsaka, A.; Turek, F.W. Sleep and circadian rhythms: Key components in the regulation of energy metabolism. FEBS Lett. 2008, 582, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Poggiogalle, E.; Jamshed, H.; Peterson, C.M. Circadian regulation of glucose, lipid, and energy metabolism in humans. Metabolism 2018, 84, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Froy, O. The relationship between nutrition and circadian rhythms in mammals. Front. Neuroendocrinol. 2007, 28, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- Stephan, F.K. Broken circadian clocks: A clock gene mutation and entrainment by feeding. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 285, R32–R33. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chattu, V.K.; Chattu, S.K.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The Interlinked Rising Epidemic of Insufficient Sleep and Diabetes Mellitus. Healthcare 2019, 7, 37. [Google Scholar] [CrossRef]
- Lo, J.C.; Groeger, J.A.; Cheng, G.H.; Dijk, D.J.; Chee, M.W. Self-reported sleep duration and cognitive performance in older adults: A systematic review and meta-analysis. Sleep Med. 2016, 17, 87–98. [Google Scholar] [CrossRef]
- Lim, J.; Dinges, D.F. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol. Bull. 2010, 136, 375–389. [Google Scholar] [CrossRef]
- DuBose, J.R.; Hadi, K. Improving inpatient environments to support patient sleep. Int. J. Qual. Health Care 2016, 28, 540–553. [Google Scholar] [CrossRef]
- Meolie, A.L.; Rosen, C.; Kristo, D.; Kohrman, M.; Gooneratne, N.; Aguillard, R.N.; Fayle, R.; Troell, R.; Townsend, D.; Claman, D.; et al. Oral nonprescription treatment for insomnia: An evaluation of products with limited evidence. J. Clin. Sleep Med. 2005, 1, 173–187. [Google Scholar]
- Peuhkuri, K.; Sihvola, N.; Korpela, R. Diet promotes sleep duration and quality. Nutr. Res. 2012, 32, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Southwell, P.R.; Evans, C.R.; Hunt, J.N. Effect of a hot milk drink on movements during sleep. Br. Med. J. 1972, 2, 429–431. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Ortuno, M.M.; Belanger, L.; Ivers, H.; LeBlanc, M.; Morin, C.M. The use of natural products for sleep: A common practice? Sleep Med. 2009, 10, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Pigeon, W.R.; Carr, M.; Gorman, C.; Perlis, M.L. Effects of a tart cherry juice beverage on the sleep of older adults with insomnia: A pilot study. J. Med. Food 2010, 13, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Phillips, F.; Chen, C.; Crisp, A.; McGuinness, B.; Kalucy, E.C.; Koval, J.; Kalucy, R.S.; Lacey, J.H. Isocaloric diet changes and electroencephalographic sleep. Lancet 1975, 2, 723–725. Available online: http://cochranelibrary-wiley.com/o/cochrane/clcentral/articles/908/CN-00012908/frame.html (accessed on 12 July 2019). [CrossRef]
- Keijzer, H.; Snitselaar, M.A.; Smits, M.G.; Spruyt, K.; Zee, P.C.; Ehrhart, F.; Curfs, L.M. Precision medicine in circadian rhythm sleep-wake disorders: Current state and future perspectives. Per. Med. 2017, 14, 171–182. [Google Scholar] [CrossRef]
- Zhou, J.; Kim, J.E.; Armstrong, C.L.; Chen, N.; Campbell, W.W. Higher-protein diets improve indexes of sleep in energy-restricted overweight and obese adults: Results from 2 randomized controlled trials. Am. J. Clin. Nutr. 2016, 103, 766–774. [Google Scholar] [CrossRef]
- Lindseth, G.; Murray, A. Dietary Macronutrients and Sleep. West. J. Nurs. Res. 2016, 38, 938–958. [Google Scholar] [CrossRef]
- Cho, K.H.; Cho, E.H.; Hur, J.; Shin, D. Association of Sleep Duration and Obesity According to Gender and Age in Korean Adults: Results from the Korea National Health and Nutrition Examination Survey 2007–2015. J. Korean Med. Sci. 2018, 33, e345. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Hillard, P.J.A.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.M.; Song, Y.; Fung, C.H.; Dzierzewski, J.M.; Mitchell, M.N.; Jouldjian, S.; Josephson, K.R.; Alessi, C.A.; Martin, J.L. Measuring Sleep in Vulnerable Older Adults: A Comparison of Subjective and Objective Sleep Measures. Clin. Gerontol. 2018, 41, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Praharaj, S.K.; Gupta, R.; Gaur, N. Clinical Practice Guideline on Management of Sleep Disorders in the Elderly. Indian J. Psychiatry 2018, 60 (Suppl. S3), S383–S396. [Google Scholar] [PubMed]
- Heslehurst, N.; Sattar, N.; Rajasingam, D.; Wilkinson, J.; Summerbell, C.D.; Rankin, J. Existing maternal obesity guidelines may increase inequalities between ethnic groups: A national epidemiological study of 502,474 births in England. BMC Pregnancy Childbirth 2012, 12, 156. [Google Scholar] [CrossRef] [PubMed]
- Board, F.A.N. (Ed.) Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Study Quality Assessment Tools. 2019. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 13 May 2019).
- Shi, Z.; McEvoy, M.; Luu, J.; Attia, J. Dietary fat and sleep duration in Chinese men and women. Int. J. Obes. 2008, 32, 1835–1840. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Karimi, G.; Esmaillzadeh, A.; Azadbakht, L. Sleep deprivation is associated with lower diet quality indices and higher rate of general and central obesity among young female students in Iran. Nutrition 2012, 28, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Santana, A.A.; Pimentel, G.D.; Romualdo, M.; Oyama, L.M.; Santos, R.V.T.; Pinho, R.A.; de Souza, C.T.; Rodrigues, B.; Caperuto, E.C.; Lira, F.S. Sleep duration in elderly obese patients correlated negatively with intake fatty. Lipids Health Dis. 2012, 11, 99. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Dietary nutrients associated with short and long sleep duration. Data from a nationally representative sample. Appetite 2013, 64, 71–80. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005-2010. Am. J. Clin. Nutr. 2014, 100, 938–947. [Google Scholar] [CrossRef]
- Katagiri, R.; Asakura, K.; Kobayashi, S.; Suga, H.; Sasaki, S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. J. Occup. Health 2014, 56, 359–368. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Lubrano, C.; Gnessi, L.; Marocco, C.; Di Lazzaro, L.; Polidoro, G.; Luisi, F.; Merola, G.; Mariani, S.; Migliaccio, S.; et al. Reduced sleep duration affects body composition, dietary intake and quality of life in obese subjects. Eat. Weight Disord. 2016, 21, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Doo, M.; Kim, Y. Association between sleep duration and obesity is modified by dietary macronutrients intake in Korean. Obes. Res. Clin. Pract. 2016, 10, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Doo, H.; Chun, H.; Doo, M. Associations of daily sleep duration and dietary macronutrient consumption with obesity and dyslipidemia in Koreans: A cross-sectional study. Medicine 2016, 95, e5360. [Google Scholar] [CrossRef] [PubMed]
- Heath, G.; Coates, A.; Sargent, C.; Dorrian, J. Sleep Duration and Chronic Fatigue Are Differently Associated with the Dietary Profile of Shift Workers. Nutrients 2016, 8, 771. [Google Scholar] [CrossRef] [PubMed]
- Doo, M.; Kim, Y. Sleep duration and dietary macronutrient consumption can modify the cardiovascular disease for Korean women but not for men. Lipids Health Dis. 2016, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.J.; Truby, H.; Zia, Z.; Cain, S.W.; Blumfield, M.L. Investigating the relationship between sleep and macronutrient intake in women of childbearing age. Eur. J. Clin. Nutr. 2017, 71, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, A.M.; Dinges, D.F.; Goel, N. Objective Measurements of Energy Balance Are Associated with Sleep Architecture in Healthy Adults. Sleep 2017, 40, 1–8. [Google Scholar] [CrossRef]
- Komada, Y.; Narisawa, H.; Ueda, F.; Saito, H.; Sakaguchi, H.; Mitarai, M.; Suzuki, R.; Tamura, N.; Inoue, S.; Inoue, Y. Relationship between Self-Reported Dietary Nutrient Intake and Self-Reported Sleep Duration among Japanese Adults. Nutrients 2017, 9, 134. [Google Scholar] [CrossRef]
- Liu, X.; Wu, D.; Qi, X.; Niu, Y.; Li, W.; Lu, Y.; Chang, J. The associations between carbohydrate and protein intakes with habitual sleep duration among adults living in urban and rural areas. Clin. Nutr. 2018, 37, 1631–1637. [Google Scholar] [CrossRef]
- Karl, J.; Thompson, L.; Niro, P.; Margolis, L.M.; McClung, J.P.; Cao, J.J.; Whigham, L.D.; Combs, G.F., Jr.; Young, A.J.; Lieberman, H.R.; et al. Transient decrements in mood during energy deficit are independent of dietary protein-to-carbohydrate ratio. Physiol. Behav. 2015, 139, 524–531. [Google Scholar] [CrossRef]
- Zadeh, S.S.; Begum, K. Comparison of nutrient intake by sleep status in selected adults in Mysore, India. Nutr. Res. Pract. 2011, 5, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; O’Connor, L.E.; Sands, L.P.; Slebodnik, M.B.; Campbell, W.W. Effects of dietary protein intake on body composition changes after weight loss in older adults: A systematic review and meta-analysis. Nutr. Rev. 2016, 74, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Fernstrom, J.D. Large neutral amino acids: Dietary effects on brain neurochemistry and function. Amino Acids 2013, 45, 419–430. [Google Scholar] [CrossRef]
- Carneiro, B.T.; Araujo, J.F. The food-entrainable oscillator: A network of interconnected brain structures entrained by humoral signals? Chronobiol. Int. 2009, 26, 1273–1289. [Google Scholar] [CrossRef] [PubMed]
- Lomenick, J.P.; Melguizo, M.S.; Mitchell, S.L.; Summar, M.L.; Anderson, J.W. Effects of meals high in carbohydrate, protein, and fat on ghrelin and peptide YY secretion in prepubertal children. J. Clin. Endocrinol. Metab. 2009, 94, 4463–4471. [Google Scholar] [CrossRef] [PubMed]
- Rontoyanni, V.G.; Baic, S.; Cooper, A.R. Association between nocturnal sleep duration, body fatness, and dietary intake in Greek women. Nutrition 2007, 23, 773–777. [Google Scholar] [CrossRef]
- Catala, A. The function of very long chain polyunsaturated fatty acids in the pineal gland. Biochim. Biophys. Acta 2010, 1801, 95–99. [Google Scholar] [CrossRef]
- Diethelm, K.; Remer, T.; Jilani, H.; Kunz, C.; Buyken, A.E. Associations between the macronutrient composition of the evening meal and average daily sleep duration in early childhood. Clin. Nutr. 2011, 30, 640–646. [Google Scholar] [CrossRef]
- Afaghi, A.; O’Connor, H.; Chow, C.M. High-glycemic-index carbohydrate meals shorten sleep onset. Am. J. Clin. Nutr. 2007, 85, 426–430. [Google Scholar] [CrossRef]
- Kang, B.; Doo, M.; Kim, Y. Associations between self-reported sleep quality and duration and dietary consumptions, psychological symptomsm and obesity in Korean adults. Prev. Nutr. Food Sci. 2017, 22, 271–276. [Google Scholar] [CrossRef][Green Version]
- Spiegel, K.; Leproult, R.; L’Hermite-Baleriaux, M.; Copinschi, G.; Penev, P.D.; Van Cauter, E. Leptin levels are dependent on sleep duration. Relationships with sympathovagal balance, carbohydrate regulation, cortisol, and thyrotropin. J. Clin. Endocrinol. Metab. 2004, 89, 5762–5771. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief communication. Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Annunziata, G.; Di Somma, C.; Laudisio, D.; Colao, A.; Savastano, S. Obesity and sleep disturbance: The chicken or the egg? Crit. Rev. Food Sci. Nutr. 2019, 59, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Singareddy, R.; Vgontzas, A.N.; Fernandez-Mendoza, J.; Liao, D.; Calhoun, S.; Shaffer, M.L.; Bixler, E.O. Risk factors for incident chronic insomnia: A general population prospective study. Sleep Med. 2012, 13, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Demisch, K.; Bauer, J.; Georgi, K. Treatment of severe chronic insomnia with L-tryptophan and varying sleeping times. Pharmacopsychiatry 1987, 20, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Choi, J.; Ahn, A.; Oh, E.; Kweon, H.; Cho, D. Acceptable macronutrient distribution ranges and hypertension. Clin. Exp. Hypertens. 2015, 37, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Pilcher, J.J.; Ginter, D.R.; Sadowsky, B. Sleep quality versus sleep quantity: Relationships between sleep and measures of health, well-being and sleepiness in college students. J. Psychosom. Res. 1997, 42, 583–596. [Google Scholar] [CrossRef]
- Grech, A.; Rangan, A.; Allman-Farinelli, M. Macronutrient Composition of the Australian Population’s Diet; Trends from Three National Nutrition Surveys 1983, 1995 and 2012. Nutrients 2018, 10, 1045. [Google Scholar] [CrossRef]
- Dietary Reference Intakes for Japanese; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2015.
- Su, C.; Zhao, J.; Wu, Y.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B. Temporal Trends in Dietary Macronutrient Intakes among Adults in Rural China from 1991 to 2011: Findings from the CHNS. Nutrients 2017, 9, 227. [Google Scholar] [CrossRef]
- Paik, H.Y. Dietary Reference Intakes for Koreans (KDRIs). Asia Pac. J. Clin. Nutr. 2008, 17, 416–419. [Google Scholar]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Trakada, G.; Steiropoulos, P.; Zarogoulidis, P.; Nena, E.; Papanas, N.; Maltezos, E.; Bouros, D. A fatty meal aggravates apnea and increases sleep in patients with obstructive sleep apnea. Sleep Breath. 2014, 18, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Yajima, K.; Seya, T.; Iwayama, K.; Hibi, M.; Hari, S.; Nakashima, Y.; Ogata, H.; Omi, N.; Satoh, M.; Tokuyama, K. Effects of nutrient composition of dinner on sleep architecture and energy metabolism during sleep. J. Nutr. Sci. Vitaminol. 2014, 60, 114–121. [Google Scholar] [CrossRef] [PubMed]


| Citation | Country | Population | n | Age [mean, SD](y) | BMI [mean, SD] | Dietary Collection Method | Measurement of Sleep Quality | Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|
| Shi et al., 2008 1 [27] | China | Healthy | 2828 | 47.1 (14.2) | 23.5 (3.5) | 3-Day food record | Sleep duration (24-h) | 8 |
| Haghighatdoost et al., 2012 [28] | Iran | Healthy | 223 | 20.7 (1.8) | 22.5 (2.8) | FFQ | Sleep duration (Nocturnal) | 6 |
| Santana et al., 2012 [29] | Brazil | Elderly and obese | 58 | 66.2 (4.0) | 33.8 (2.7) | 24-h Recall | Sleep duration (Nocturnal) | 5 |
| Grandner et al., 2013 2 [30] | USA | Healthy | 4548 | 46.3 (16.5) | 28.7 (6.8) | 24-h Recall | Sleep duration (Nocturnal) | 8 |
| Kant & Graubard, 2014 2 [31] | USA | Healthy | 15,199 | - | - | 24-h Recall | Sleep duration (Nocturnal) | 6 |
| Katagiri et al., 2014 [32] | Japan | Healthy | 3129 | 47.6 (4.0) | 21.9 (3.0) | DHQ | Sleep duration (Nocturnal), PSQI | 8 |
| Poggiogalle et al., 2016 [33] | Italy | Healthy (Caucasian) | 42 | 52.5 (11.2) | 40.1 (6.7) | 3-Day food record | Sleep duration (24-h) | 8 |
| Doo & Kim, 2016 3 [34] | Korea | Healthy | 14,111 | 44.8 (0.3) | 23.7 (0.1) | FFQ | Sleep duration (24-h) | 8 |
| Doo et al., 2016 3 [35] | Korea | Healthy | 14,680 | 45.2 (0.3) | 23.6 (0.1) | FFQ | Sleep duration (24-h) | 8 |
| Heath et al., 2016 [36] | Australia | Healthy (Shift-workers) | 118 | 43.4 (9.9) | 27.1 (4.3) | FFQ | Sleep duration (24-h) | 8 |
| Doo & Kim, 2016 3 [37] | Korea | Healthy | 14,111 | 44.9 (0.2) | 23.7 (0.1) | FFQ | Sleep duration (24-h) | 8 |
| Bennett et al., 2017 [38] | Australia | Healthy | 6594 | 33.7 | 26.0 | FFQ | Sleep duration (24-h) | 8 |
| Spaeth et al., 2017 [39] | USA | Healthy | 46 | 33.9 (9.1) | 24.5 (3.6) | Weight | Sleep duration (Nocturnal), SL, SE% | 6 |
| Komada et al., 2017 [40] | Japan | Healthy | 1902 | 48.0 (10.3) | 22.4 (3.3) | BDHQ | Sleep duration (Nocturnal), SL | 7 |
| Liu et al., 2018 1 [41] | China | Healthy | 9239 | 50.5 (15.0) | 23.35 (3.5) | 24-h Recall | Sleep duration (24-h) | 6 |
| Average Score | 7.2 | |||||||
| Citation | Study Design | Country | Population | n | Age [mean, SD] (y) | BMI [mean, SD] | Control | Intervention | Intervention Duration | Sleep Evaluation | Quality Assessment Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lindseth et al., 2013 [41] | Double-blind Crossover | USA | Healthy | 44 | 20.6 (2.0) | 24.8 (3.5) | 35% FAT 50% CHO 15% PRO | High-FAT (56% FAT, 22% CHO, 22% PRO) High-CHO (22% FAT, 56% CHO, 22% PRO) High-PRO (22% FAT, 22% CHO, 56% PRO) | 4 days (2-wk washout) | SL, SE% | 12 |
| Karl et al., 2015 [42] | Block | USA | Healthy | 39 | 21.0 (3.7) | 25.0 (3.7) | 31% FAT 55% CHO 14% PRO | Moderate-PRO [30% FAT, 43%CHO, 27%PRO] High-PRO [30%FAT, 28%CHO, 42%PRO] *40% energy deficit | 21 days | SL | 7 |
| Lindseth & Murray, 2016 [18] | Crossover | USA | Healthy | 36 | 20.9 (1.9) | 24.6 (4.1) | 35% FAT 50% CHO 15% PRO) | High-FAT (65% FAT, 25% CHO, 10% PRO) High-CHO (10% FAT, 80% CHO, 10% PRO) High-PRO (15% FAT, 40% CHO, 45% PRO) | 4 days (2-wk washout) | Sleep duration (Nocturnal), PSQI, SL, SE% | 12 |
| Zhou et al., 2016 [17] | Crossover | USA | Overweight/Obese | 14 | 56.0 (3.0) | 30.9 (0.6) | 25% FAT 65% CHO 10% PRO | Moderate-PRO (25% FAT, 55% CHO, 20% PRO) High-PRO (25% FAT, 45% CHO, 30% PRO) *750kcal energy deficit | 4 weeks | Sleep duration (Nocturnal), PSQI | 10 |
| Average Score | 10.3 | ||||||||||
| Data Groups | POOR SLEEPERS | GOOD SLEEPERS | |||||
|---|---|---|---|---|---|---|---|
| CHO | PRO | FAT | CHO | PRO | FAT | ||
| SLEEP DURATION | < 7 h duration | ≥ 7 h duration | |||||
| Combined | Mean (E%) | 55.0 | 15.9 | 27.6 | 52.1 | 16.4 | 30.0 |
| Range (E%) | 25.0–80.0 | 10.0–45.0 | 10.0–65.0 | 39.1–67.2 | 12.2–30.0 | 18.4–36.1 | |
| CS | Mean (E%) | 55.6 | 15.3 | 27.3 | 52.5 | 15.7 | 30.2 |
| Range (E%) | 38.7–69.9 | 12.8–21.5 | 16.3–36.8 | 39.1–67.2 | 12.2–20.7 | 18.4–36.1 | |
| RCT | Mean (E%) | 52.5 | 18.3 | 29.2 | 45.0 | 30.0 | 25.0 |
| Range (E%) | 25.0–80.0 | 10.0–45.0 | 10.0–65.0 | 45.0–45.0 | 30.0–30.0 | 25.0v25.0 | |
| PSQI | GSS > 5 | GSS ≤ 5 | |||||
| Combined | Mean (E%) | 47.4 | 15.9 | 36.0 | 55.4 | 18.7 | 24.6 |
| Range (E%) | 25.0–65.0 | 10.0–30.0 | 25.0–65.0 | 40.0–80.0 | 10.0–45.0 | 10.0–35.0 | |
| CS | Mean (E%) | 54.5 | 13.4 | 29.0 | 54.2 | 13.6 | 29.1 |
| Range (E%) | 54.4–54.5 | 13.4–13.4 | 29.0–29.0 | 53.8–54.5 | 13.6–13.7 | 28.8–29.5 | |
| RCT | Mean (E%) | 45.0 | 16.7 | 38.3 | 56.3 | 22.5 | 21.3 |
| Range (E%) | 25.0–65.0 | 10.0–30.0 | 25.0–65.0 | 40.0–80.0 | 10.0–45.0 | 10.0–35.0 | |
| SLEEP LATENCY (SL) * | SL > 30 min | SL ≤ 30 min | |||||
| RCT | Mean (E%) | 48.8 | 20.0 | 31.3 | 39.4 | 31.1 | 29.9 |
| Range (E%) | 25.0–80.0 | 10.0–45.0 | 10.0–65.0 | 22.0–56.0 | 14.0–56.0 | 18.0–56.0 | |
| SLEEP EFFICIENCY (SE%) * | SE% ≤ 85% | SE% > 85% | |||||
| RCT | Mean (E%) | 48.8 | 20.0 | 31.3 | 37.5 | 33.8 | 29.5 |
| Range (E%) | 25.0–80.0 | 10.0–45.0 | 10.0–65.0 | 22.0–56.0 | 22.0–56 | 18.0–56.0 | |
| Data Groups | POOR SLEEPERS | GOOD SLEEPERS | |||||
|---|---|---|---|---|---|---|---|
| CHO | PRO | FAT | CHO | PRO | FAT | ||
| SLEEP DURATION | <7 h duration | ≥ 7 h duration | |||||
| Non-obese * | Mean (E%) | 55.2 | 15.6 | 27.5 | 52.9 | 15.7 | 29.9 |
| Range (E%) | 25.0–80.0 | 10.0–45.0 | 10.0–65.0 | 39.1–67.2 | 12.2–20.7 | 18.4–36.1 | |
| Obese* * | Mean (E%) | 52.7 | 17.9 | 28.3 | 42.2 | 22.2 | 32.1 |
| Range (E%) | 38.7–65.0 | 10.0–21.5 | 24.9–34.5 | 40.7–45.0 | 19.0–30.0 | 25.0–35.9 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sutanto, C.N.; Wang, M.X.; Tan, D.; Kim, J.E. Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression. Nutrients 2020, 12, 126. https://doi.org/10.3390/nu12010126
Sutanto CN, Wang MX, Tan D, Kim JE. Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression. Nutrients. 2020; 12(1):126. https://doi.org/10.3390/nu12010126
Chicago/Turabian StyleSutanto, Clarinda Nataria, Min Xian Wang, Denise Tan, and Jung Eun Kim. 2020. "Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression" Nutrients 12, no. 1: 126. https://doi.org/10.3390/nu12010126
APA StyleSutanto, C. N., Wang, M. X., Tan, D., & Kim, J. E. (2020). Association of Sleep Quality and Macronutrient Distribution: A Systematic Review and Meta-Regression. Nutrients, 12(1), 126. https://doi.org/10.3390/nu12010126