Garlic Consumption and All-Cause Mortality among Chinese Oldest-Old Individuals: A Population-Based Cohort Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment of Garlic Consumption
2.3. Death Ascertainment
2.4. Statistical Analysis
3. Results
3.1. Garlic Consumption and Baseline Characteristics
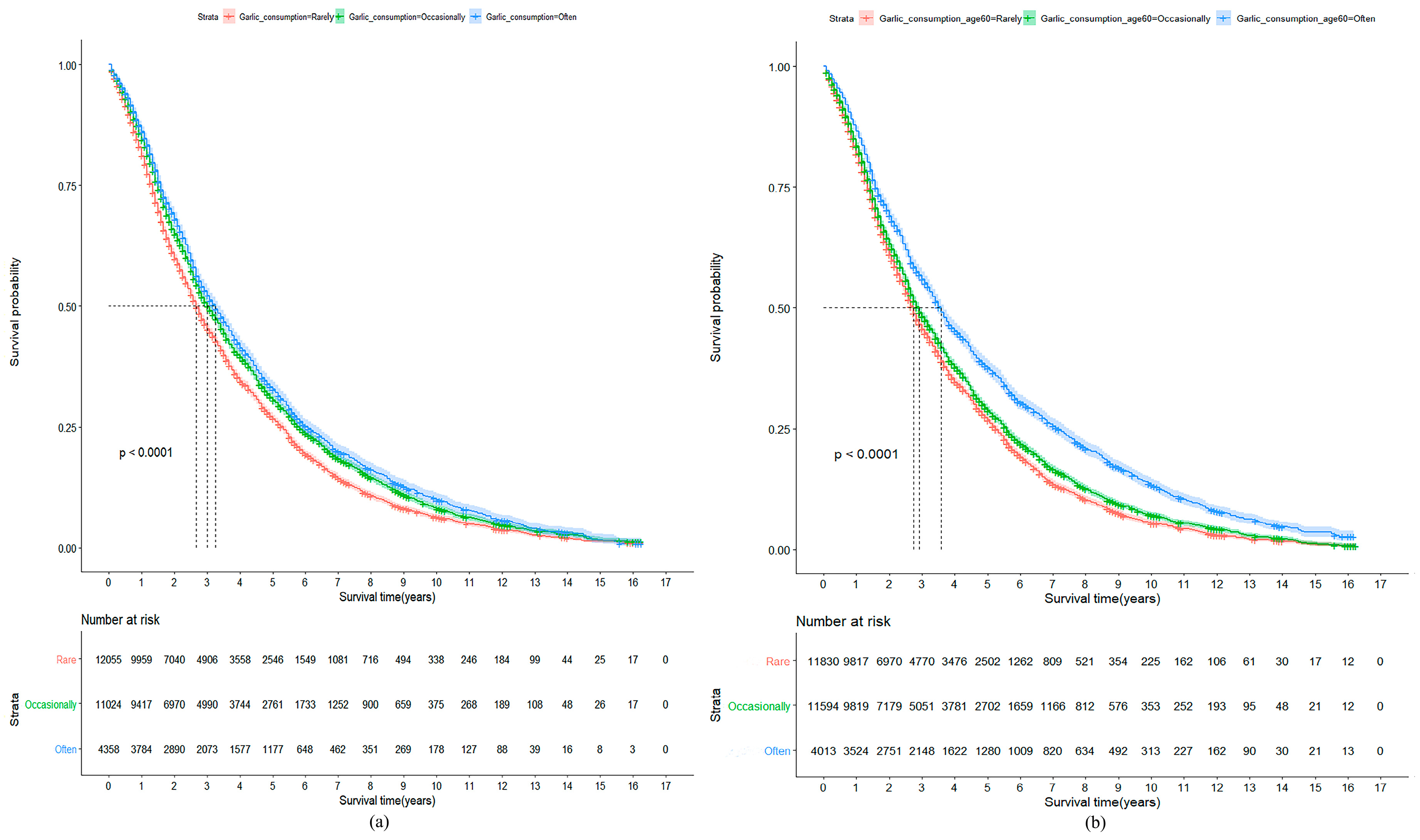
3.2. Garlic Consumption at Baseline or at 60 Years of Age and All-Cause Mortality
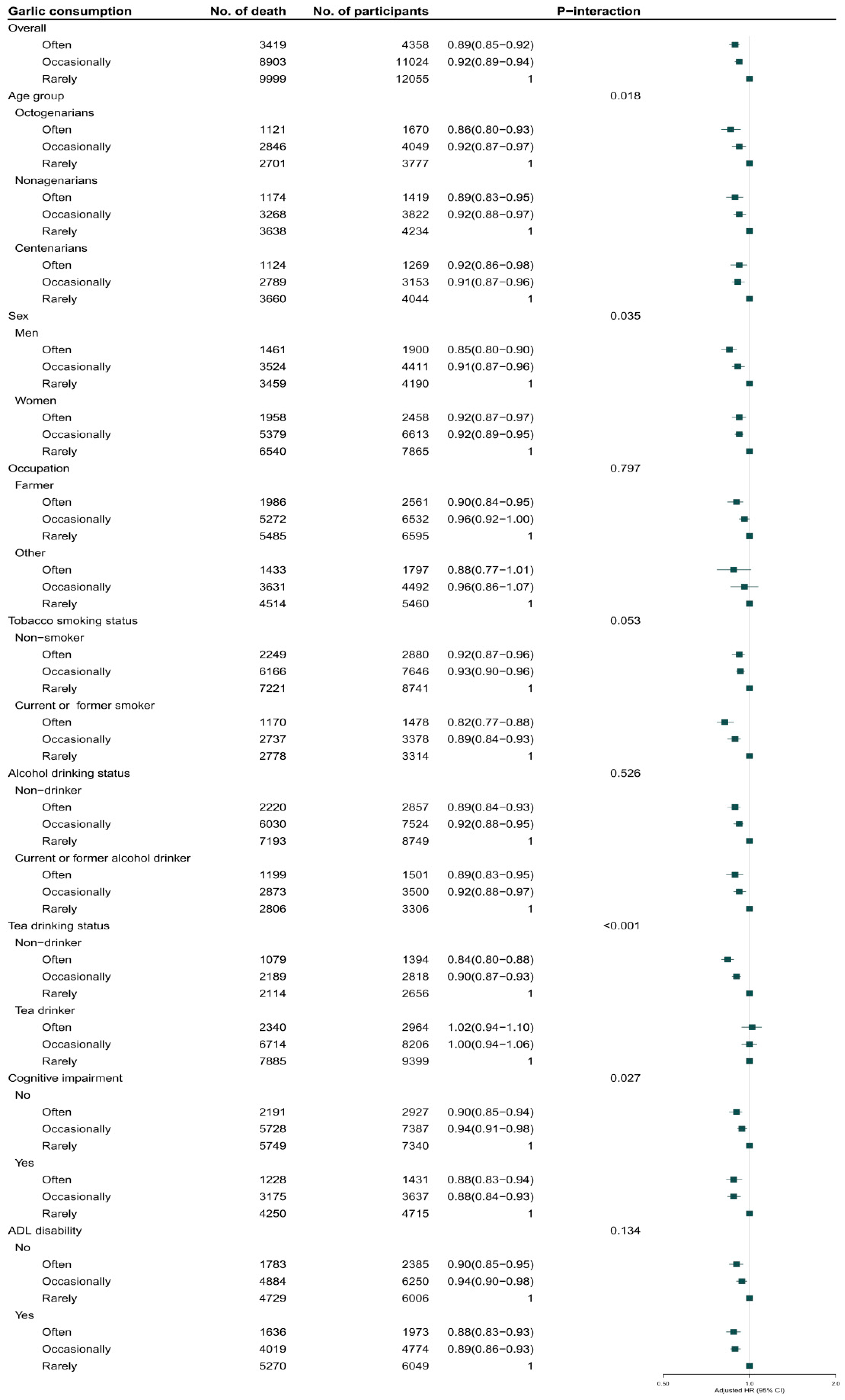
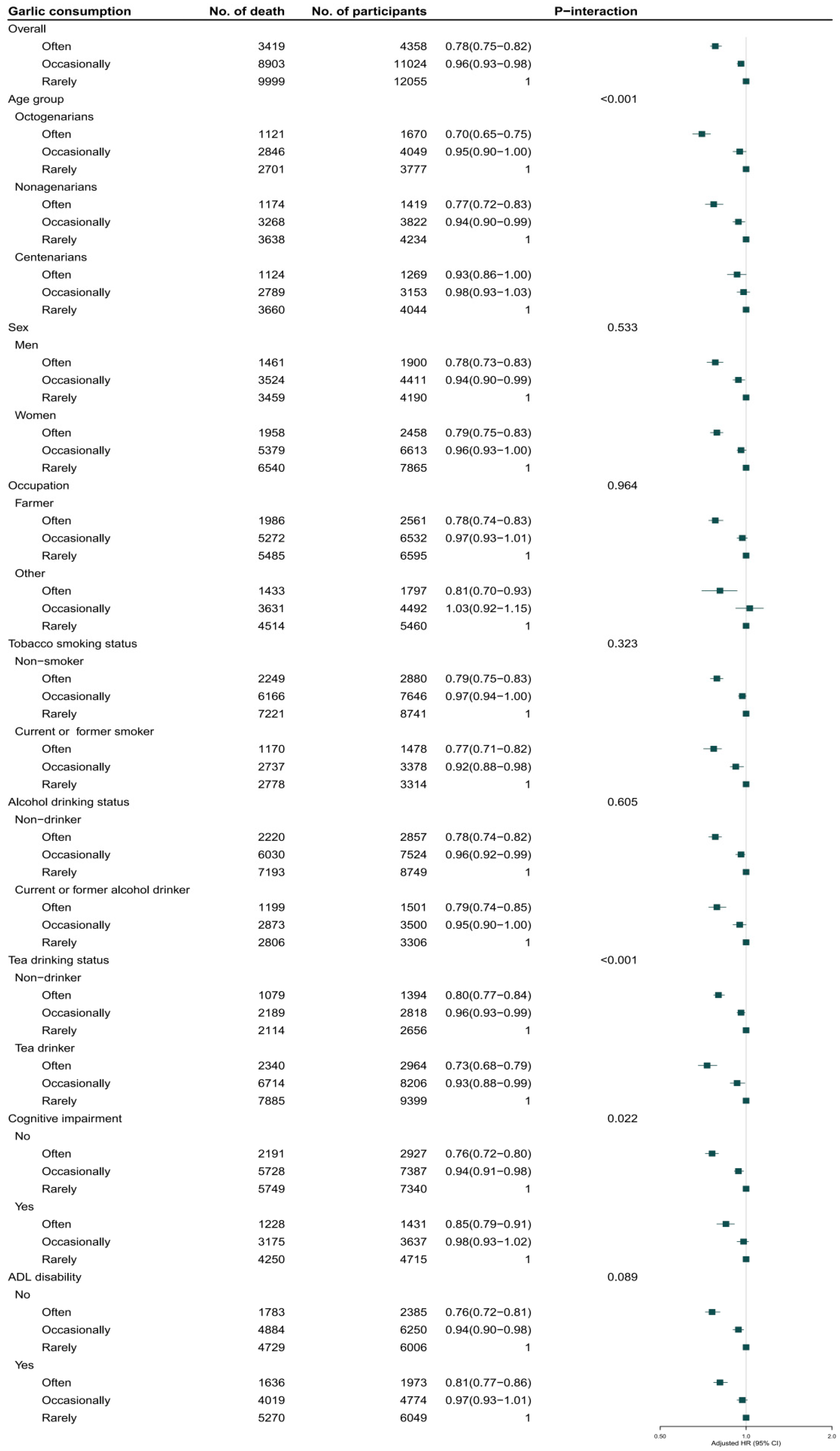
3.3. Sensitivity Analyses and Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Value of Agricultural Production (FAO). Available online: http://www.fao.org/home/en/ (accessed on 17 May 2019).
- Martins, N.; Petropoulos, S.; Ferreira, I.C. Chemical composition and bioactive compounds of garlic (Allium sativum L.) as affected by pre- and post-harvest conditions: A review. Food Chem. 2016, 211, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Rahman, K. Garlic and aging: New insights into an old remedy. Ageing Res. Rev. 2003, 2, 39–56. [Google Scholar] [CrossRef]
- Myneni, A.A.; Chang, S.C.; Niu, R.; Liu, L.; Swanson, M.K.; Li, J.; Su, J.; Giovino, G.A.; Yu, S.; Zhang, Z.F.; et al. Raw garlic consumption and lung cancer in a Chinese population. Cancer Epidemiol. Biomark. Prev. 2016, 25, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Missbach, B.; Hoffmann, G. An umbrella review of garlic intake and risk of cardiovascular disease. Phytomedicine 2016, 23, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Pelucchi, C.; Guercio, V.; La, V.C.; Galeone, C. Allium vegetable intake and gastric cancer: A case–control study and meta-analysis. Mol. Nutr. Food Res. 2015, 59, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Kodali, R.T.; Eslick, G.D. Meta-analysis: Does garlic intake reduce risk of gastric cancer? Nutr. Cancer 2015, 67, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.Y.; Wu, M.; Han, R.Q.; Zhang, X.F.; Wang, X.S.; Liu, A.M.; Zhou, J.Y.; Lu, Q.Y.; Zhang, Z.F.; Zhao, J.K. Raw garlic consumption as a protective factor for lung cancer, a population-based case–control study in a Chinese population. Cancer Prev. Res. 2013, 6, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Frank, O.R.; Stocks, N.P.; Fakler, P.; Sullivan, T. Effect of garlic on blood pressure: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2013, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Dorant, E.; van den Brandt, P.A.; Goldbohm, R.A. A prospective cohort study on Allium vegetable consumption, garlic supplement use, and the risk of lung carcinoma in The Netherlands. Cancer Res. 1994, 54, 6148–6153. [Google Scholar]
- Zeng, T.; Zhang, C.L.; Zhao, X.L.; Xie, K.Q. The roles of garlic on the lipid parameters: A systematic review of the literature. Crit. Rev. Food Sci. Nutr. 2013, 53, 215–230. [Google Scholar] [CrossRef]
- Stabler, S.N.; Tejani, A.M.; Huynh, F.; Fowkes, C. Garlic for the prevention of cardiovascular morbidity and mortality in hypertensive patients. J. Evid. Based Med. 2012, 5, 243. [Google Scholar] [CrossRef] [PubMed]
- De Souza Silva, J.E.; Santos Souza, C.A.; da Silva, T.B.; Gomes, I.A.; Brito Gde, C.; de Souza Araújo, A.A.; de Lyra-Júnior, D.P.; da Silva, W.B.; da Silva, F.A. Use of herbal medicines by elderly patients: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.P.; Lawson, L.D. Garlic: The Science and Therapeutic Application of Allium sativum L. and Related Species, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1996; p. 329. [Google Scholar]
- Capasso, A. Antioxidant action and therapeutic efficacy of Allium sativum L. Molecules 2013, 18, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Production of Garlic: Top 10 Producers, Average 1994–2017. Available online: http://www.fao.org/faostat/en/#data/QC/visualize (accessed on 17 May 2019).
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Qiu, L.; Sautter, J.; Gu, D. Associations between frequency of tea consumption and health and mortality: Evidence from old Chinese. Br. J. Nutr. 2012, 108, 1686–1697. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Dupre, M.E. Assessment of reliability of mortality and morbidity in the 1998–2002 CLHLS waves. In Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions; Zeng, Y., Dudley, L., Poston, J.R., Denese, A.V., Gu, D., Eds.; Springer: Dordrecht, The Netherlands, 2008; pp. 99–115. [Google Scholar]
- An, R.; Liu, G.; Khan, N.; Yan, H.; Wang, Y. Dietary habits and cognitive impairment risk among oldest-old Chinese. J. Gerontol. B Psychol. Sci. Soc. Sci. 2019, 74, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Zhang, T.; Byles, J.; Martin, S.; Avery, J.C.; Taylor, A.W. Food habits, lifestyle factors and mortality among oldest old Chinese: The Chinese Longitudinal Healthy Longevity Survey (CLHLS). Nutrients 2015, 7, 7562–7579. [Google Scholar] [CrossRef]
- Patrician, P.A. Multiple imputation for missing data. Res. Nurs. Health. 2002, 25, 76–84. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folsein, S.E.; McHugh, R.R. “MiniMental state”: A practical method for grading the cognitive state of pattern for clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Zhang, Z. Gender differentials in cognitive impairment and decline of the oldest old in China. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, S107–S115. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Hsu-Hage, B.H.; Wahlqvist, M.L. The use of knee height to estimate maximum stature in elderly Chinese. J. Nutr. Health Aging. 1998, 2, 84–87. [Google Scholar] [PubMed]
- Lv, Y.B.; Yuan, J.Q.; Mao, C.; Gao, X.; Yin, Z.X.; Kraus, V.B.; Luo, J.S.; Chen, H.S.; Zeng, Y.; Wang, W.T.; et al. Association of body mass index with disability in activities of daily living among Chinese adults 80 years of age or older. JAMA Netw. Open 2018, 1, e181915. [Google Scholar] [CrossRef] [PubMed]
- Rana, S.V.; Pal, R.; Vaiphei, K.; Sharma, S.K.; Ola, R.P. Garlic in health and disease. Nutr. Res. Rev. 2011, 24, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.C.; Cottrell, S.L.; Plummer, S.; Lloyd, D. Antimicrobial properties of Allium sativum (garlic). Appl. Microbiol. Biotechnol. 2001, 57, 282–286. [Google Scholar] [CrossRef]
- Hanum, F.; Anilakumar, K.R.; Viswanathan, K.R. Anticarcinogenic properties of garlic: A review. Crit. Rev. Food Sci. Nutr. 2004, 44, 479–488. [Google Scholar]
- Talib, W.H. Consumption of garlic and lemon aqueous extracts combination reduces tumor burden by angiogenesis inhibition, apoptosis induction, and immune system modulation. Nutrition 2017, 43, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Harman, D. Ageing: A theory based on free radical and radiation chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Luca, M.; Luca, A.; Calandra, C. The role of oxidative damage in the pathogenesis and progression of Alzheimer’s disease and vascular dementia. Oxid. Med. Cell. Longev. 2015, 2015, 504678. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, P.D.; Barrera, D.; Rivero, I.; Mata, R.; Medina-Campos, O.N.; Hernandez-Pando, R.; Pedraza-Chaverrí, J. Antioxidant S-allylcysteine prevents gentamicin-induced oxidative stress and renal damage. Free Radic. Biol. Med. 2003, 35, 317–324. [Google Scholar] [CrossRef]
- Budoff, M.J.; Ahmadi, N.; Gul, K.M.; Liu, S.T.; Flores, F.R.; Tiano, J.; Takasu, J.; Miller, E.; Tsimikas, S. Aged garlic extract supplemented with B vitamins, folic acid and L-arginine retards the progression of subclinical atherosclerosis: A randomized clinical trial. Prev. Med. 2009, 49, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Ide, N.; Lau, B.H. Garlic compounds minimize intracellular oxidative stress and inhibit nuclear factor-κB activation. J. Nutr. 2001, 131, 1020S–1026S. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kwon, O. Garlic intake and cancer risk: An analysis using the Food and Drug Administration’s evidence-based review system for the scientific evaluation of health claims. Am. J. Clin. Nutr. 2009, 89, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, H.Q.; Wang, Y.; Xu, H.X.; Fan, W.T.; Wang, M.L.; Sun, PH.; Xie, X.Y. An intervention study to prevent gastric cancer by microselenium and large dose of allitridum. Chin. Med. J. 2004, 117, 1155–1160. [Google Scholar] [PubMed]
- Petrovic, V.; Nepal, A.; Olaisen, C.; Bachke, S.; Hira, J.; Søgaard, C.; Røst, L.; Misund, K.; Andreassen, T.; Melø, T.; et al. Anti-cancer potential of homemade fresh garlic extract is related to increased endoplasmic reticulum stress. Nutrients 2018, 10, 450. [Google Scholar] [CrossRef]
- Borzì, A.; Biondi, A.; Basile, F.; Luca, S.; Vicari, E.; Vacante, M. Olive oil effects on colorectal cancer. Nutrients 2019, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.W.; Chen, H.W.; Sheen, L.Y.; Lii, C.K. Garlic: Health benefits and actions. Biomedicine 2012, 2, 17–29. [Google Scholar] [CrossRef]
- Reem, S.; Aya, A.; Kalidas, S.; Sarkar, D.; Eid, A.H. Mechanisms underlying the antihypertensive effects of garlic bioactives. Nutr. Res. 2014, 34, 106–115. [Google Scholar]
- Rodrigues, C.; Percival, S.S. Immunomodulatory effects of glutathione, garlic derivatives, and hydrogen sulfide. Nutrients 2019, 11, 295. [Google Scholar] [CrossRef]
- Percival, S.S. Aged garlic extract modifies human immunity. J. Nutr. 2016, 146, 433S–436S. [Google Scholar] [CrossRef]
- Loera, J.A.; Black, S.A.; Markides, K.S.; Espino, D.V.; Goodwin, J.S. The use of herbal medicine by older Mexican Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M714–M718. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Fei, Z.; Qiu, C.; Brasher, M.S.; Kraus, V.B.; Zhao, W.; Shi, X.; Zeng, Y. Dietary diversity and cognitive function among elderly people: A population-based study. J. Nutr. Health Aging. 2017, 21, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Wahlqvist, M.L.; Lee, M.S. Appetite predicts mortality in free-living older adults in association with dietary diversity. A NAHSIT cohort study. Appetite 2014, 83, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, F.; Capasso, R.; Izzo, A.A. Garlic (Allium sativum L.): Adverse effects and drug interactions in humans. Mol. Nutr. Food Res. 2007, 51, 1386–1397. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Milner, J.A. The influence of heating on the anticancer properties of garlic. J. Nutr. 2001, 131, 1054S–1057S. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| TbVariable | Octogenarians | Nonagenarians | Centenarians | All | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Often | Occasionally | Rare | p Value | Often | Occasionally | Rare | p Value | Often | Occasionally | Rare | p Value | Often | Occasionally | Rare | p Value | |
| Number of participants | 1670 (17.6) | 4049 (42.6) | 3777 (39.8) | 1419 (15.0) | 3822 (40.3) | 4234 (44.7) | 1269 (15.0) | 3153 (37.2) | 4044 (47.8) | 4358 (15.9) | 11024 (40.2) | 12055 (43.9) | ||||
| Age (year) | 84.3 ± 3.0 | 84.2 ± 3.0 | 84.3 ± 3.0 | 0.746 | 93.5 ± 2.8 | 93.7 ± 2.9 | 93.8 ± 2.9 | 0.001 | 101.6 ± 2.0 | 101.6 ± 2.0 | 101.5 ± 1.9 | 0.003 | 92.3 ± 7.6 | 92.5 ± 7.5 | 93.4 ± 7.4 | <0.001 |
| BMI (kg/m2) | 20.1 ± 3.8 | 19.8 ± 3.6 | 19.7 ± 3.9 | 0.001 | 19.4 ± 3.7 | 18.9 ± 3.3 | 18.9 ± 3.3 | <0.001 | 18.7 ± 3.4 | 18.5 ± 3.3 | 18.4 ± 3.3 | 0.001 | 19.5 ± 3.7 | 19.1 ± 3.5 | 19.0 ± 3.5 | <0.001 |
| Sex | <0.001 | <0.001 | 0.089 | <0.001 | ||||||||||||
| Men | 932 (55.8) | 2127 (52.5) | 1770 (46.9) | 693 (48.8) | 1664 (43.5) | 1657 (39.1) | 275 (21.7) | 620 (19.7) | 763 (18.9) | 1900 (43.6) | 4411 (40.0) | 4190 (34.8) | ||||
| Women | 738 (44.2) | 1922 (47.5) | 2007 (53.1) | 726 (51.2) | 2158 (56.5) | 2577 (60.9) | 994 (78.3) | 2533 (80.3) | 3281 (81.1) | 2458 (56.4) | 6613 (60.0) | 7865 (65.2) | ||||
| Occupation | 0.019 | 0.006 | <0.001 | <0.001 | ||||||||||||
| Farmer | 923 (55.3) | 2228 (55.0) | 1970 (52.2) | 811 (57.2) | 2253 (58.9) | 2347 (55.4) | 827 (65.2) | 2051 (65.0) | 2278 (56.3) | 2561 (58.8) | 6532 (59.3) | 6595 (54.7) | ||||
| Other | 747 (44.7) | 1821 (45.0) | 1807 (47.8) | 608 (42.8) | 1569 (41.1) | 1887 (44.6) | 442 (34.8) | 1102 (35.0) | 1766 (43.7) | 1797 (41.2) | 4492 (40.7) | 5460 (45.3) | ||||
| Residence | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Urban | 457 (27.4) | 1007 (24.9) | 1129 (29.9) | 340 (24.0) | 782 (20.5) | 1146 (27.1) | 270 (21.3) | 628 (19.9) | 1099 (27.2) | 1067 (24.5) | 2417 (21.9) | 3374 (28.0) | ||||
| Rural | 1213 (72.6) | 3042 (75.1) | 2648 (70.1) | 1079 (76.0) | 3040 (79.5) | 3088 (72.9) | 999 (78.7) | 2525 (80.1) | 2945 (72.8) | 3291 (75.5) | 8607 (78.1) | 8681 (72.0) | ||||
| Marital status | <0.001 | 0.274 | 0.865 | <0.001 | ||||||||||||
| In marriage | 630 (37.7) | 1327 (32.8) | 1195 (31.6) | 207 (14.6) | 535 (14.0) | 554 (13.1) | 46 (3.6) | 106 (3.4) | 134 (3.3) | 883 (20.3) | 1968 (17.9) | 1883 (15.6) | ||||
| Not in marriage | 1040 (62.3) | 2722 (67.2) | 2582 (68.4) | 1212 (85.4) | 3287 (86.0) | 3680 (86.9) | 1223 (96.4) | 3047 (96.6) | 3910 (96.7) | 3475 (79.7) | 9056 (82.1) | 10172 (84.4) | ||||
| Educational background | 0.035 | 0.004 | 0.513 | <0.001 | ||||||||||||
| Illiteracy | 960 (57.5) | 2447 (60.4) | 2310 (61.2) | 950 (66.9) | 2729 (71.4) | 3015 (71.2) | 1080 (85.1) | 2693 (85.4) | 3415 (84.4) | 2990 (68.6) | 7869 (71.4) | 8740 (72.5) | ||||
| Literacy | 710 (42.5) | 1602 (39.6) | 1467 (38.8) | 469 (33.1) | 1093 (28.6) | 1219 (28.8) | 189 (14.9) | 460 (14.6) | 629 (15.6) | 1368 (31.4) | 3155 (28.6) | 3315 (27.5) | ||||
| Living pattern | <0.001 | 0.012 | <0.001 | <0.001 | ||||||||||||
| With family members | 1397 (83.7) | 3238 (80.0) | 2959 (78.3) | 1210 (85.3) | 3142 (82.2) | 3468 (81.9) | 1151 (90.7) | 2809 (89.1) | 3516 (86.9) | 3758 (86.2) | 9189 (83.4) | 9943 (82.5) | ||||
| Alone or at nursing home | 273 (16.3) | 811 (20.0) | 818 (21.7) | 209 (14.7) | 680 (17.8) | 766 (18.1) | 118 (9.3) | 344 (10.9) | 528 (13.1) | 600 (13.8) | 1835 (16.6) | 2112 (17.5) | ||||
| Tobacco smoking status | <0.001 | 0.002 | <0.001 | <0.001 | ||||||||||||
| Non-smoker | 970 (58.1) | 2422 (59.8) | 2397 (63.5) | 937 (66.0) | 2687 (70.3) | 3026 (71.5) | 973 (76.7) | 2537 (80.5) | 3318 (82.0) | 2880 (66.1) | 7646 (69.4) | 8741 (72.5) | ||||
| Current smoker | 400 (24.0) | 962 (23.8) | 739 (19.6) | 254 (17.9) | 611 (16.0) | 618 (14.6) | 139 (11.0) | 301 (9.5) | 280 (6.9) | 793 (18.2) | 1874 (17.0) | 1637 (13.6) | ||||
| Former smoker | 300 (18.0) | 665 (16.4) | 641 (17.0) | 228 (16.1) | 524 (13.7) | 590 (13.9) | 157 (12.4) | 315 (10.0) | 446 (11.0) | 685 (15.7) | 1504 (13.6) | 1677 (13.9) | ||||
| Alcohol drinking status | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Non-drinker | 1035 (62.0) | 2579 (63.7) | 2667 (70.6) | 923 (65.0) | 2635 (68.9) | 3030 (71.6) | 899 (70.8) | 2310 (73.3) | 3052 (75.5) | 2857 (65.6) | 7524 (68.3) | 8749 (72.6) | ||||
| Current drinker | 439 (26.3) | 999 (24.7) | 683 (18.1) | 318 (22.4) | 780 (20.4) | 763 (18.0) | 248 (19.5) | 584 (18.5) | 629 (15.6) | 1005 (23.1) | 2363 (21.4) | 2075 (17.2) | ||||
| Former drinker | 196 (11.7) | 471 (11.6) | 427 (11.3) | 178 (12.5) | 407 (10.6) | 441 (10.4) | 122 (9.6) | 259 (8.2) | 363 (9.0) | 496 (11.4) | 1137 (10.3) | 1231 (10.2) | ||||
| Regular exercise | 0.554 | 0.613 | <0.001 | 0.002 | ||||||||||||
| Yes | 763 (45.7) | 1910 (47.2) | 1780 (47.1) | 553 (39.0) | 1516 (39.7) | 1634 (38.6) | 368 (29.0) | 1114 (35.3) | 1313 (32.5) | 1684 (38.6) | 4540 (41.2) | 4727 (39.2) | ||||
| No | 907 (54.3) | 2139 (52.8) | 1997 (52.9) | 866 (61.0) | 2306 (60.3) | 2600 (61.4) | 901 (71.0) | 2039 (64.7) | 2731 (67.5) | 2674 (61.4) | 6484 (58.8) | 7328 (60.8) | ||||
| Meat consumption | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Often | 702 (42.0) | 1294 (32.0) | 1131 (29.9) | 624 (44.0) | 1263 (33.0) | 1316 (31.1) | 599 (47.2) | 1090 (34.6) | 1311 (32.4) | 1925 (44.2) | 3647 (33.1) | 3758 (31.2) | ||||
| Occasionally | 685 (41.0) | 2157 (53.3) | 1828 (48.4) | 597 (42.1) | 2017 (52.8) | 1982 (46.8) | 496 (39.1) | 1600 (50.7) | 1748 (43.2) | 1778 (40.8) | 5774 (52.4) | 5558 (46.1) | ||||
| Rarely | 283 (16.9) | 598 (14.8) | 818 (21.7) | 198 (14.0) | 542 (14.2) | 936 (22.1) | 174 (13.7) | 463 (14.7) | 985 (24.4) | 655 (15.0) | 1603 (14.5) | 2739 (22.7) | ||||
| Fish consumption | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Often | 421 (25.2) | 594 (14.7) | 586 (15.5) | 437 (30.8) | 631 (16.5) | 753 (17.8) | 416 (32.8) | 507 (16.1) | 767 (19.0) | 1274 (29.2) | 1732 (15.7) | 2106 (17.5) | ||||
| Occasionally | 781 (46.8) | 2413 (59.6) | 1864 (49.4) | 622 (43.8) | 2176 (56.9) | 2023 (47.8) | 547 (43.1) | 1740 (55.2) | 1699 (42.0) | 1950 (44.7) | 6329 (57.4) | 5586 (46.3) | ||||
| Rarely | 468 (28.0) | 1042 (25.7) | 1327 (35.1) | 360 (25.4) | 1015 (26.6) | 1458 (34.4) | 306 (24.1) | 906 (28.7) | 1578 (39.0) | 1134 (26.0) | 2963 (26.9) | 4363 (36.2) | ||||
| Vegetable consumption | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Often | 1501 (89.9) | 3474 (85.8) | 3049 (80.7) | 1232 (86.8) | 3158 (82.6) | 3221 (76.1) | 1086 (85.6) | 2528 (80.2) | 2945 (72.8) | 3819 (87.6) | 9160 (83.1) | 9215 (76.4) | ||||
| Occasionally | 133 (8.0) | 502 (12.4) | 581 (15.4) | 149 (10.5) | 541 (14.2) | 723 (17.1) | 143 (11.3) | 502 (15.9) | 729 (18.0) | 425 (9.8) | 1545 (14.0) | 2033 (16.9) | ||||
| Rarely | 36 (2.2) | 73 (1.8) | 147 (3.9) | 38 (2.7) | 123 (3.2) | 290 (6.8) | 40 (3.2) | 123 (3.9) | 370 (9.1) | 114 (2.6) | 319 (2.9) | 807 (6.7) | ||||
| Fruits consumption | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Often | 556 (33.3) | 924 (22.8) | 789 (20.9) | 513 (36.2) | 881 (23.1) | 961 (22.7) | 494 (38.9) | 799 (25.3) | 1043 (25.8) | 1563 (35.9) | 2604 (23.6) | 2793 (23.2) | ||||
| Occasionally | 686 (41.1) | 2109 (52.1) | 1822 (48.2) | 543 (38.3) | 1920 (50.2) | 1880 (44.4) | 464 (36.6) | 1492 (47.3) | 1680 (41.5) | 1693 (38.8) | 5521 (50.1) | 5382 (44.6) | ||||
| Rarely | 428 (25.6) | 1016 (25.1) | 1166 (30.9) | 363 (25.6) | 1021 (26.7) | 1393 (32.9) | 311 (24.5) | 862 (27.3) | 1321 (32.7) | 1102 (25.3) | 2899 (26.3) | 3880 (32.2) | ||||
| Tea drinking | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Often | 553 (33.1) | 1233 (30.5) | 1022 (27.1) | 492 (34.7) | 993 (26.0) | 935 (22.1) | 349 (27.5) | 592 (18.8) | 699 (17.3) | 1394 (32.0) | 2818 (25.6) | 2656 (22.0) | ||||
| Occasionally | 258 (15.4) | 680 (16.8) | 536 (14.2) | 193 (13.6) | 700 (18.3) | 521 (12.3) | 153 (12.1) | 624 (19.8) | 445 (11.0) | 604 (13.9) | 2004 (18.2) | 1502 (12.5) | ||||
| Rarely | 859 (51.4) | 2136 (52.8) | 2219 (58.8) | 734 (51.7) | 2129 (55.7) | 2778 (65.6) | 767 (60.4) | 1937 (61.4) | 2900 (71.7) | 2360 (54.2) | 6202 (56.3) | 7897 (65.5) | ||||
| Hypertension | 0.008 | 0.031 | 0.605 | 0.005 | ||||||||||||
| Yes | 956 (57.2) | 2302 (56.9) | 2272 (60.2) | 759 (53.5) | 2078 (54.4) | 2404 (56.8) | 649 (51.1) | 1647 (52.2) | 2133 (52.7) | 2364 (54.2) | 6027 (54.7) | 6809 (56.5) | ||||
| No | 714 (42.8) | 1747 (43.1) | 1505 (39.8) | 660 (46.5) | 1744 (45.6) | 1830 (43.2) | 620 (48.9) | 1506 (47.8) | 1911 (47.3) | 1994 (45.8) | 4997 (45.3) | 5246 (43.5) | ||||
| Heart disease | 0.015 | 0.007 | 0.040 | <0.001 | ||||||||||||
| Yes | 147 (8.8) | 282 (7.0) | 320 (8.5) | 95 (6.7) | 209 (5.5) | 304 (7.2) | 73 (5.8) | 147 (4.7) | 243 (6.0) | 315 (7.2) | 638 (5.8) | 867 (7.2) | ||||
| No | 1523 (91.2) | 3767 (93.0) | 3457 (91.5) | 1324 (93.3) | 3613 (94.5) | 3930 (92.8) | 1196 (94.2) | 3006 (95.3) | 3801 (94.0) | 4043 (92.8) | 10386 (94.2) | 11188 (92.8) | ||||
| Cerebrovascular disease | 0.103 | 0.613 | 0.775 | 0.287 | ||||||||||||
| Yes | 94 (5.6) | 175 (4.3) | 175 (4.6) | 57 (4.0) | 137 (3.6) | 168 (4.0) | 35 (2.8) | 99 (3.1) | 119 (2.9) | 186 (4.3) | 411 (3.7) | 462 (3.8) | ||||
| No | 1576 (94.4) | 3874 (95.7) | 3602 (95.4) | 1362 (96.0) | 3685 (96.4) | 4066 (96.0) | 1234 (97.2) | 3054 (96.9) | 3925 (97.1) | 4172 (95.7) | 10613 (96.3) | 11593 (96.2) | ||||
| Respiratory disease | 0.947 | 0.898 | 0.860 | 0.928 | ||||||||||||
| Yes | 217 (13.0) | 537 (13.3) | 493 (13.1) | 153 (10.8) | 397 (10.4) | 450 (10.6) | 114 (9.0) | 297 (9.4) | 384 (9.5) | 484 (11.1) | 1231 (11.2) | 1327 (11.0) | ||||
| No | 1453 (87.0) | 3512 (86.7) | 3284 (86.9) | 1266 (89.2) | 3425 (89.6) | 3784 (89.4) | 1155 (91.0) | 2856 (90.6) | 3660 (90.5) | 3874 (88.9) | 9793 (88.8) | 10728 (89.0) | ||||
| Cognitive impairment | 0.023 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Yes | 217 (13.0) | 529 (13.1) | 568 (15.0) | 471 (33.2) | 1272 (33.3) | 1599 (37.8) | 743 (58.6) | 1836 (58.2) | 2548 (63.0) | 1431 (32.8) | 3637 (33.0) | 4715 (39.1) | ||||
| No | 1453 (87.0) | 3520 (86.9) | 3209 (85.0) | 948 (66.8) | 2550 (66.7) | 2635 (62.2) | 526 (41.4) | 1317 (41.8) | 1496 (37.0) | 2927 (67.2) | 7387 (67.0) | 7340 (60.9) | ||||
| ADL disability | 0.140 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Yes | 526 (31.5) | 1243 (30.7) | 1238 (32.8) | 662 (46.7) | 1648 (43.1) | 2105 (49.7) | 785 (61.9) | 1883 (59.7) | 2706 (66.9) | 1973 (45.3) | 4774 (43.3) | 6049 (50.2) | ||||
| No | 1144 (68.5) | 2806 (69.3) | 2539 (67.2) | 757 (53.3) | 2174 (56.9) | 2129 (50.3) | 484 (38.1) | 1270 (40.3) | 1338 (33.1) | 2385 (54.7) | 6250 (56.7) | 6006 (49.8) | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, X.; Lv, Y.; Mao, C.; Yuan, J.; Yin, Z.; Gao, X.; Zhang, Z. Garlic Consumption and All-Cause Mortality among Chinese Oldest-Old Individuals: A Population-Based Cohort Study. Nutrients 2019, 11, 1504. https://doi.org/10.3390/nu11071504
Shi X, Lv Y, Mao C, Yuan J, Yin Z, Gao X, Zhang Z. Garlic Consumption and All-Cause Mortality among Chinese Oldest-Old Individuals: A Population-Based Cohort Study. Nutrients. 2019; 11(7):1504. https://doi.org/10.3390/nu11071504
Chicago/Turabian StyleShi, Xiaoming, Yuebin Lv, Chen Mao, Jinqiu Yuan, Zhaoxue Yin, Xiang Gao, and Zuofeng Zhang. 2019. "Garlic Consumption and All-Cause Mortality among Chinese Oldest-Old Individuals: A Population-Based Cohort Study" Nutrients 11, no. 7: 1504. https://doi.org/10.3390/nu11071504
APA StyleShi, X., Lv, Y., Mao, C., Yuan, J., Yin, Z., Gao, X., & Zhang, Z. (2019). Garlic Consumption and All-Cause Mortality among Chinese Oldest-Old Individuals: A Population-Based Cohort Study. Nutrients, 11(7), 1504. https://doi.org/10.3390/nu11071504