Molecular Approaches for Diagnosis, Therapy and Prevention of Cow’s Milk Allergy

 and
and
Abstract
1. Introduction
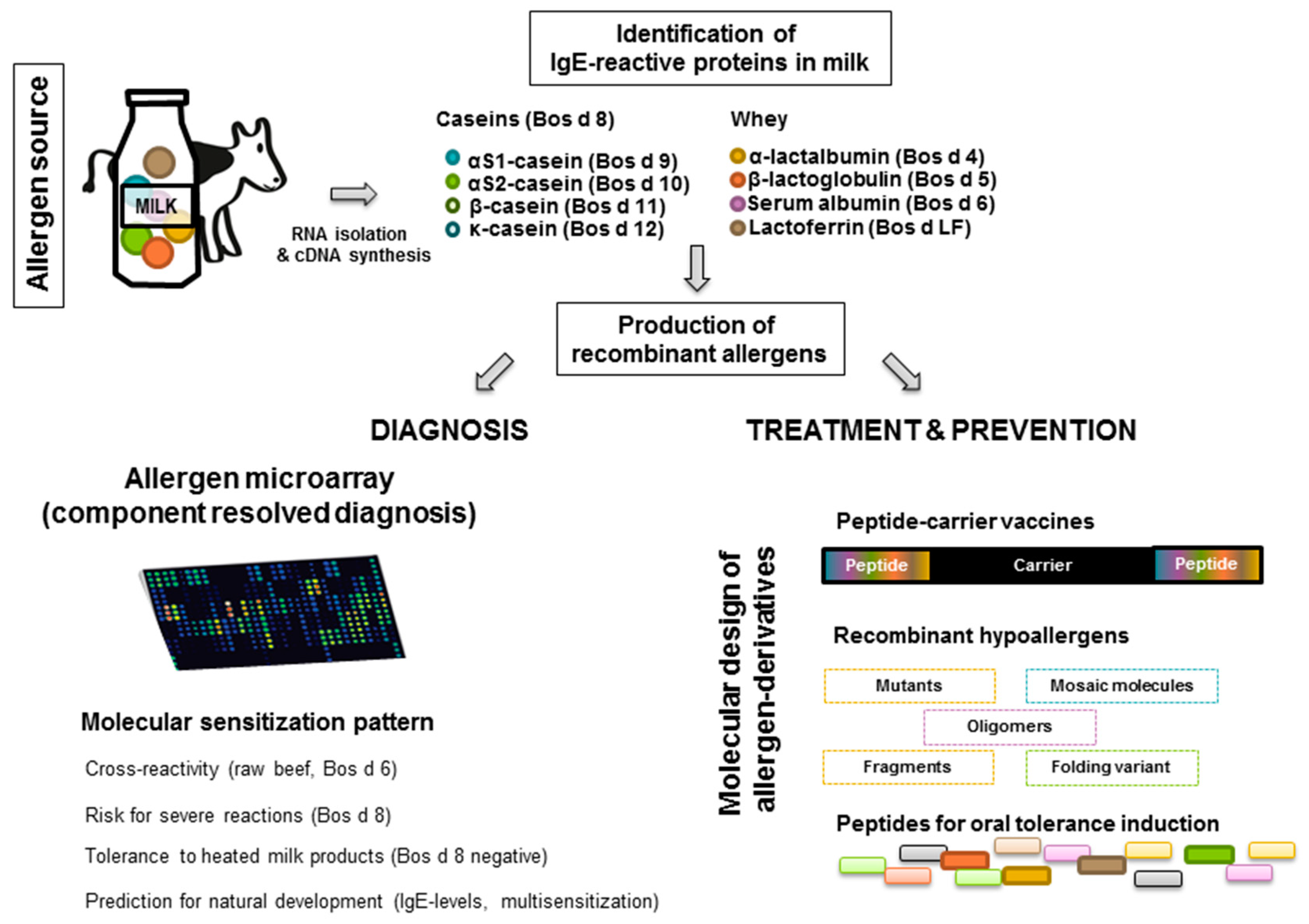
2. Cow’s Milk Allergen Molecules
2.1. Whey Proteins
2.1.1. Alpha-Lactalbumin (Bos d 4)
2.1.2. Beta-Lactoglobulin (Bos d 5)
2.1.3. Serum Albumin (Bos d 6)

{kind=link}
{kind=link}
| Whey | Caseins | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Allergen (UNIPROT) | Bos d 4 (B6V3I5) | Bos d 5 (G5E5H7) | Bos d 6 (B0JYQ0) | Bos d 7 | Bos d LF (B9VPZ5) | Bos d 8 | Bos d 9 (B5B3R8) | Bos d 10 (P02663) | Bos d 11 (P02666) | Bos d 12 (P02668) |
| Isoallergen (Accession number) | Bos d 4.0101 (P00711) | Bos d 5.0101 (P02754), Bos d 5.0102 (B5B0D4) | Bos d 6 (P02769) | Bos d 7.0101 | Bos d LF (P24627) | Bos d 9.0101 (P02662) | Bos d 10.0101 (P02663) | Bos d 11.0101 (P02666) | Bos d 12.0101 (P02668) | |
| Protein family | Albumins | Globulins, Lipocalins | Albumins | Immuno-globulins | Transferrins | Caseins | Caseins | Caseins | Caseins | Caseins |
| Protein name | Alpha-lactalbumin | Beta-lactoglobulin | Serum albumin | IgG | Lactoferrin | AlphaS1-casein, alphaS2-casein, beta-casein, kappa-casein | AlphaS1-casein | AlphaS2-casein | Beta-casein | Kappa-casein |
| Molecular weight [kiloDalton] | 14.19 | 18.31 | 67.20 | 160 | 76.14 | 22.89 | 24.35 | 23.58 | 18.97 | |
| Isoelectric point | 4.80 | 4.83 | 5.60 | n.a. | 8.67 | 4.95 | 8.34 | 5.13 | 5.93 | |
| Number of amino acids (AA) | 123 (AA 1-19 signal; AA 20-142 chain) | 162 (AA 1-16 signal; AA 17-162 chain) | 589 (AA 1-18 signal; AA 19-607) | n.a. | 689 (AA v1-19 signal; AA 20-708 chain) | 199 (AA 1-15 signal; AA 16-214 chain) | 207 (AA 1-15 signal; AA 16-222 chain) | 209 (AA 1-15 signal; AA 16-224 chain) | 169 (AA 1-21 signal; AA 22-190 chain) | |
| Number of patients (n), %IgE-positive | n = 58, 27.6% [18]; n = 140, 25% [19]; n = 78, 62.8% [20]; n = 51, 19.6% [21]; n = 45, 19% [22] | n = 58, 38.7% [18]; 10% [19]; n = 78, 43.6% [20]; n = 140, n = 51, 19.6% [21]; n = 45, 23% [22] | n = 58, 12.9% [18]; 25% [19]; n = 78, 3.8% [20]; n = 140; n = 51, 21.56% [21]; n = 45, 23% [22] | n = 58, 10.3% [18]; n = 140, 40% [19] | n = 58, 10.3% [18]; n = 140, 10% [19]; n = 78, 5.1% [20]; n = 51, 66.67% [21] | n = 58, 46.5% [18]; n = 140, 40% [19]; n = 51, 49.02% [21]; n = 45, 40% [22] | n = 58, 58% [18]; n = 140, 25% [19] | n = 58, 71.0% [18]; n = 140, 20% [19] | n = 58, 58.1% [18]; n = 140, 10% [19]; n = 78, 29.5% [20] | |
| Cross reactivity | n = 6,beta-lactoglobulin from buffalo’s, ewe’s milk, goat’s milk [23] | raw meat (beef, lamb, deer, pork) [24]; Cap h 6 (goat), Ovi a 6 (Sheep), Equ c 3 (horse), Equ as 6 (Donkey), Sus s 1 (Pig) [6] | Casein from buffalo’s, ewe’s milk, goat’s milk [23]; 30S component from soy (IgE-reactivity) [25] | |||||||
| Heat stability | Aggregation [26] | Aggregation [26] | Heat-sensitive | ? | ? | Heat-stabile | ||||
| Associated symptoms | Bos d 6-sensitized beef allergic children react to CM [27]; patients tolerated heated meat products [14,24] | Bos d 8-sensitized CM allergic patients react to heated products, Bos d 8-sIgE correlates with symptom severity [28] | ||||||||
2.1.4. Bos d 7 (Immunoglobulin)
2.1.5. Lactoferrin (Bos d LF)
2.2. Caseins (Bos d 8)
AlphaS1-Casein, AlphaS2-Casein, Beta-Casein, Kappa-Casein (Bos d 9–12)
3. Diagnosis of Cow’s Milk Allergy: From Classical Procedures Towards Molecular Diagnosis
3.1. Cow’s Milk-Specific IgE Measurement
3.2. Skin Testing
3.2.1. Skin Prick Test (SPT)
3.2.2. Atopy Patch Test (APT)
3.3. Food Challenges
3.4. Molecular Diagnosis
4. Current Treatment Strategies for Cow’s Milk Allergy
4.1. Avoidance and Hypoallergenic Milk Formulas
4.2. Substitution of CM by Non-Bovine Milk Sources
4.3. Pre- and Probiotics
4.4. Current Strategies for Allergen-Specific Immunotherapy of Cow’s Milk Allergy
4.4.1. Oral Immunotherapy (OIT)
4.4.2. Sublingual Immunotherapy (SLIT)
| Intervention | Administration Route | Procedure | Aim of Intervention | Ref. |
|---|---|---|---|---|
| Avoidance of CM proteins | Oral | Introduction of ehMF or aaMF into diet; Substitution of CM by non-bovine milk | Reduction of allergic symptoms due to the lack of CM-specific epitopes | [23,86,87,88,89,90,91,92,93,94,95] |
| OIT | Oral | Application of increasing amounts of CM | Desensitization; Clinical tolerance to CM allergens | [108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130] |
| SLIT | Sublingual | Application of increasing amounts of CM | Desensitization; Clinical tolerance to CM allergens | [131,132] |
| EPIT | Epicutaneous | Delivery of CM proteins via patch application | Desensitization; Clinical tolerance to CM allergens | [133,134,135,136,137,138] |
| Pre/ Probiotics | Oral | Given alone or in combination with hydrolyzed milk formulas | Immunomodulation | [100,101,102,103,104,105,106] |
4.4.3. Epicutaneous Immunotherapy (EPIT)
5. Emerging Strategies for the Treatment and Prevention of Cow’s Milk Allergy
5.1. IgE-Targeting Therapies
5.2. Subcutaneous Immunotherapy with Recombinant Hypoallergens
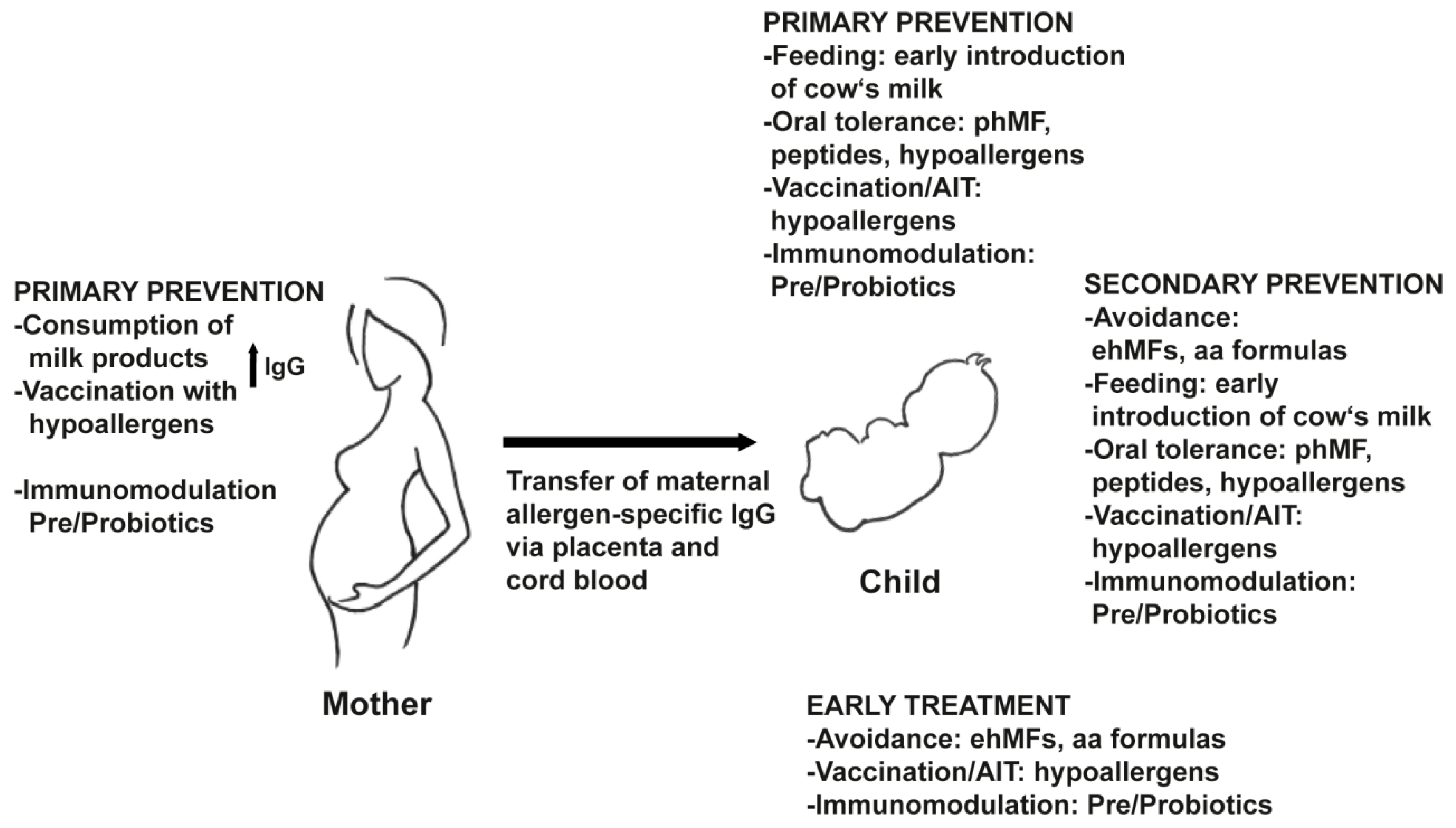
5.3. Strategies for the Prevention of Milk Allergy
6. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Valenta, R.; Hochwallner, H.; Linhart, B.; Pahr, S. Food allergies: The basics. Gastroenterology 2015, 148, 1120–1131. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Brozek, J.; Schünemann, H.; Bahna, S.L.; von Berg, A.; Beyer, K.; Bozzola, M.; Bradsher, J.; Compalati, E.; Ebisawa, M.; et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guidelines. World Allergy Organ. J. 2010, 3, 57–161. [Google Scholar] [CrossRef] [PubMed]
- Schoemaker, A.A.; Sprikkelman, A.B.; Grimshaw, K.E.; Roberts, G.; Grabenhenrich, L.; Rosenfeld, L.; Siegert, S.; Dubakiene, R.; Rudzeviciene, O.; Reche, M.; et al. Incidence and natural history of challenge-proven cow’s milk allergy in European children-EuroPrevall birth cohort. Allergy 2015, 70, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Lupinek, C.; Wollmann, E.; Baar, A.; Banerjee, S.; Breiteneder, H.; Broecker, B.M.; Bublin, M.; Curin, M.; Flicker, S.; Garmatiuk, T.; et al. Advances in allergen-microarray technology for diagnosis and monitoring of allergy: The MeDALL allergen-chip. Methods 2014, 66, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Anto, J.M.; Bousquet, J.; Akdis, M.; Auffray, C.; Keil, T.; Momas, I.; Postma, D.S.; Valenta, R.; Wickman, M.; Cambon-Thomsen, A.; et al. Mechanisms of the Development of Allergy (MeDALL): Introducing novel concepts in allergy phenotypes. J. Allergy Clin. Immunol. 2017, 139, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Villa, C.; Costa, J.; Oliveira, M.B.P.; Mafra, I. Bovine Milk Allergens: A Comprehensive Review. Compr. Rev. Food Sci. Food Saf. 2018, 17, 137–164. [Google Scholar] [CrossRef]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Spitzauer, S.; Valenta, R. Cow’s milk allergy: From allergens to new forms of diagnosis, therapy and prevention. Methods 2014, 66, 22–23. [Google Scholar] [CrossRef]
- Wal, J.M. Cow’s milk allergens. Allergy 1998, 53, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Focke-Tejkl, M.; Civaj, V.; Balic, N.; Nystrand, M.; Härlin, A.; Thalhamer, J.; Scheiblhofer, S.; et al. Visualization of clustered IgE epitopes on alpha-lactalbumin. J. Allergy Clin. Immunol. 2010, 125, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Wal, J.M. Bovine milk allergenicity. Ann. Allergy Asthma Immunol. 2004, 93 (Suppl. 5), S2–S11. [Google Scholar] [CrossRef]
- Monaci, L.; Tregoat, V.; van Hengel, A.J.; Anklam, E. Milk allergens, their characteristics and their detection in food: A review. Eur. Food Res. Technol. 2006, 223, 149–179. [Google Scholar] [CrossRef]
- Järvinen, K.M.; Chatchatee, P.; Bardina, L.; Beyer, K.; Sampson, H.A. IgE and IgG binding epitopes on alpha-lactalbumin and beta-lactoglobulin in cow’s milk allergy. Int. Arch. Allergy Immunol. 2001, 126, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Sélo, I.; Clément, G.; Bernard, H.; Chatel, J.; Créminon, C.; Peltre, G.; Wal, J. Allergy to bovine beta-lactoglobulin: Specificity of human IgE to tryptic peptides. Clin. Exp. Allergy 1999, 29, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Serrano, J.; Caballero, M.L.; Rodríguez-Pérez, R.; Carretero, P.; Pérez, R.; Blanco, J.G.; Juste, S.; Moneo, I. Sensitization to serum albumins in children allergic to cow’s milk and epithelia. Pediatr. Allergy Immunol. 2007, 18, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Spitzauer, S.; Pandjaitan, B.; Söregi, G.; Mühl, S.; Ebner, C.; Kraft, D.; Valenta, R.; Rumpold, H. IgE cross-reactivities against albumins in patients allergic to animals. J. Allergy Clin. Immunol. 1995, 96, 951–959. [Google Scholar] [CrossRef]
- Pandjaitan, B.; Swoboda, I.; Brandejsky-Pichler, F.; Rumpold, H.; Valenta, R.; Spitzauer, S. Escherichia coli expression and purification of recombinant dog albumin, a cross-reactive animal allergen. J. Allergy Clin. Immunol. 2000, 105, 279–285. [Google Scholar] [CrossRef]
- Reininger, R.; Swoboda, I.; Bohle, B.; Hauswirth, A.W.; Valent, P.; Rumpold, H.; Valenta, R.; Spitzauer, S. Characterization of recombinant cat albumin. Clin. Exp. Allergy 2003, 33, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- D’Urbano, L.E.; Pellegrino, K.; Artesani, M.C.; Donnanno, S.; Luciano, R.; Riccardi, C.; Tozzi, A.E.; Ravà, L.; De Benedetti, F.; Cavagni, G. Performance of a component-based allergen-microarray in the diagnosis of cow’s milk and hen’s egg allergy. Clin. Exp. Allergy 2010, 40, 1561–1570. [Google Scholar] [CrossRef]
- Ott, H.; Baron, J.M.; Heise, R.; Ocklenburg, C.; Stanzel, S.; Merk, H.F.; Niggemann, B.; Beyer, K. Clinical usefulness of microarray-based IgE detection in children with suspected food allergy. Allergy 2008, 63, 1521–1528. [Google Scholar] [CrossRef]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Balic, N.; Geller, B.; Nystrand, M.; Härlin, A.; Thalhamer, J.; Scheiblhofer, S.; Niggemann, B.; et al. Microarray and allergenic activity assessment of milk allergens. Clin. Exp. Allergy 2010, 40, 1809–1818. [Google Scholar] [CrossRef]
- Röckmann, H.; van Geel, M.J.; Knulst, A.C.; Huiskes, J.; Bruijnzeel-Koomen, C.A.; de Bruin-Weller, MS. Food allergen sensitization pattern in adults in relation to severity of atopic dermatitis. Clin. Transl. Allergy 2014, 4, 9. [Google Scholar] [CrossRef]
- Erwin, E.A.; Tripathi, A.; Ogbogu, P.U.; Commins, S.P.; Slack, M.A.; Cho, C.B.; Hamilton, R.G.; Workman, L.J.; Platts-Mills, T.A. IgE Antibody Detection and Component Analysis in Patients with Eosinophilic Esophagitis. J. Allergy Clin. Immunol. Pract. 2015, 3, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Restani, P.; Gaiaschi, A.; Plebani, A.; Beretta, B.; Cavagni, G.; Fiocchi, A.; Poiesi, C.; Velonà, T.; Ugazio, A.G.; Galli, C.L. Cross-reactivity between milk proteins from different animal species. Clin. Exp. Allergy 1999, 29, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Kattan, J.D.; Cocco, R.R.; Järvinen, K.M. Milk and soy allergy. Pediatr. Clin. North Am. 2011, 58, 407–426. [Google Scholar] [CrossRef]
- Rozenfeld, P.; Docena, G.H.; Añón, M.C.; Fossati, C.A. Detection and identification of a soy protein component that cross-reacts with caseins from cow’s milk. Clin. Exp. Immunol. 2002, 130, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Bloom, K.A.; Huang, F.R.; Bencharitiwong, R.; Bardina, L.; Ross, A.; Sampson, H.A.; Nowak-Węgrzyn, A. Effect of heat treatment on milk and egg proteins allergenicity. Pediatr. Allergy Immunol. 2014, 25, 740–746. [Google Scholar] [CrossRef]
- Martelli, A.; De Chiara, A.; Corvo, M.; Restani, P.; Fiocchi, A. Beef allergy in children with cow’s milk allergy; cow’s milk allergy in children with beef allergy. Ann. Allergy Asthma Immunol. 2002, 89 (Suppl. 6), 38–43. [Google Scholar] [CrossRef]
- Yanagida, N.; Sato, S.; Takahashi, K.; Nagakura, K.I.; Asaumi, T.; Ogura, K.; Ebisawa, M. Increasing specific immunoglobulin E levels correlate with the risk of anaphylaxis during an oral food challenge. Pediatr. Allergy Immunol. 2018, 29, 417–424. [Google Scholar] [CrossRef]
- Adédoyin, J.; Johansson, S.G.; Grönlund, H.; van Hage, M. Interference in immunoassays by human IgM with specificity for the carbohydrate moiety of animal proteins. J. Immunol. Methods 2006, 310, 117–125. [Google Scholar] [CrossRef]
- Adédoyin, J.; Grönlund, H.; Oman, H.; Johansson, S.G.; van Hage, M. Cat IgA, representative of new carbohydrate cross-reactive allergens. J. Allergy Clin. Immunol. 2007, 119, 640–645. [Google Scholar] [CrossRef]
- Grönlund, H.; Adédoyin, J.; Commins, S.P.; Platts-Mills, T.A.; van Hage, M. The carbohydrate galactose-alpha-1,3-galactose is a major IgE-binding epitope on cat IgA. J. Allergy Clin. Immunol. 2009, 123, 1189–1191. [Google Scholar] [CrossRef] [PubMed]
- Brock, J.H. Lactoferrin-50 years on. Biochem. Cell Biol. 2012, 90, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Schulmeister, U.; Hochwallner, H.; Swoboda, I.; Focke-Tejkl, M.; Geller, B.; Nystrand, M.; Härlin, A.; Thalhamer, J.; Scheiblhofer, S.; Keller, W.; et al. Cloning, expression, and mapping of allergenic determinants of alphaS1-casein, a major cow’s milk allergen. J. Immunol. 2009, 182, 7019–7029. [Google Scholar] [CrossRef] [PubMed]
- Egan, M.; Lee, T.; Andrade, J.; Grishina, G.; Mishoe, M.; Gimenez, G.; Sampson, H.A.; Bunyavanich, S. Partially hydrolyzed whey formula intolerance in cow’s milk allergic patients. Pediatr. Allergy Immunol. 2017, 28, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.; O’Flynn, N. Diagnosis and assessment of food allergy in children and young people in primary care and community settings: NICE clinical guideline. Br. J. Gen. Pract. 2011, 61, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. European Society of Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef]
- Walsh, J.; Meyer, R.; Shah, N.; Quekett, J.; Fox, A.T. Differentiating milk allergy (IgE and non-IgE mediated) from lactose intolerance: Understanding the underlying mechanisms and presentations. Br. J. Gen. Pract. 2016, 66, e609–e611. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, F.L.; van Neerven, R.J.; van Katwijk, M.; Bos, J.D.; Kapsenberg, M.L. Serum-IgE-facilitated allergen presentation in atopic disease. J. Immunol. 1993, 150, 3643–3650. [Google Scholar]
- Campana, R.; Mothes, N.; Rauter, I.; Vrtala, S.; Reininger, R.; Focke-Tejkl, M.; Lupinek, C.; Balic, N.; Spitzauer, S.; Valenta, R. Non-IgE-mediated chronic allergic skin inflammation revealed with rBet v 1 fragments. J. Allergy Clin. Immunol. 2008, 121, 528–530. [Google Scholar] [CrossRef]
- Campana, R.; Moritz, K.; Marth, K.; Neubauer, A.; Huber, H.; Henning, R.; Blatt, K.; Hoermann, G.; Brodie, T.M.; Kaider, A.; et al. Frequent occurrence of T cell-mediated late reactions revealed by atopy patch testing with hypoallergenic rBet v 1 fragments. J. Allergy Clin. Immunol. 2016, 137, 601–609. [Google Scholar] [CrossRef][Green Version]
- Kounis, N.G.; Zavras, G.M. Histamine-induced coronary artery spasm: The concept of allergic angina. Br. J. Clin. Pract. 1991, 45, 121–128. [Google Scholar] [PubMed]
- Tzanis, G.; Bonou, M.; Mikos, N.; Biliou, S.; Koniara, I.; Kounis, N.G.; Barbetseas, J. Early stent thrombosis secondary to food allergic reaction: Kounis syndrome following rice pudding ingestion. World J. Cardiol. 2017, 9, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, M.; Subedi, R.; Shah, S.; Kozman, H. Kounis syndrome: A review article on epidemiology, diagnostic findings, mamagement and complications of allergic acute coronary syndrome. Int. J. Cardiol. 2017, 232, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lee, H.; Choi, A.R.; Park, K.H.; Ryu, J.H.; Oh, E.J. Comparison of allergen-specific IgE levels between Immulite 2000 and ImmunoCAP systems against six inhalant allergens and ten food allergens. Scand. J. Clin. Lab. Investig. 2018, 78, 606–612. [Google Scholar] [CrossRef] [PubMed]
- van Hage, M.; Hamsten, C.; Valenta, R. ImmunoCAP assays: Pros and cons in allergology. J. Allergy Clin. Immunol. 2017, 140, 974–977. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.P.O.; van Tilburg, M.F.; Tramontina Florean, E.O.P.; Guedes, M.I.F. Detection of serum and salivary IgE and IgG1 immunoglobulins specific for diagnosis of food allergy. PLoS ONE 2019, 14, e0214745. [Google Scholar] [CrossRef] [PubMed]
- Garib, V.; Rigler, E.; Gastager, F.; Campana, R.; Dorofeeva, Y.; Gattinger, P.; Zhernov, Y.; Khaitov, M.; Valenta, R. Determination of IgE and IgG reactivity to more than 170 allergen molecules in paper-dried blood spots. J. Allergy Clin. Immunol. 2019, 143, 437–440. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, B.; Indirli, G.C.; Bianchi, A.; Arasi, S.; Caimmi, D.; Dondi, A.; La Grutta, S.; Panetta, V.; Verga, M.C.; Calvani, M. Specific IgE and skin prick tests to diagnose allergy to fresh and baked cow’s milk according to age: A systematic review. Ital. J. Pediatr. 2017, 43, 93. [Google Scholar] [CrossRef]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Twaroch, T.E.; Vogelsang, H.; Kazemi-Shirazi, L.; Kundi, M.; Balic, N.; Quirce, S.; Rumpold, H.; et al. Patients suffering from non-IgE-mediated cow’s milk protein intolerance cannot be diagnosed based on IgG subclass or IgA responses to milk allergens. Allergy 2011, 66, 1201–1207. [Google Scholar] [CrossRef]
- Stapel, S.O.; Asero, R.; Ballmer-Weber, B.K.; Knol, E.F.; Strobel, S.; Vieths, S.; Kleine-Tebbe, J. Testing for IgG4 against foods is not recommended as a diagnostic. Allergy 2008, 63, 793–796. [Google Scholar] [CrossRef]
- Bock, S.A. AAAAI support of the EAACI Position Paper on IgG4. J. Allergy Clin. Immunol. 2010, 125, 1410. [Google Scholar] [CrossRef] [PubMed]
- Sporik, R.; Hill, D.J.; Hosking, C.S. Specificity of allergen skin testing in predicting positive open food challenges to milk, egg and peanut in children. Clin. Exp. Allergy 2000, 30, 1540–1546. [Google Scholar] [CrossRef] [PubMed]
- Saarinen, K.M.; Suomalainen, H.; Savilahti, E. Diagnostic value of skin-prick and patch tests and serum eosinophil cationic protein and cow’s milk-specific IgE in infants with cow’s milk allergy. Clin. Exp. Allergy 2001, 31, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Verstege, A.; Mehl, A.; Rolinck-Werninghaus, C.; Staden, U.; Nocon, M.; Beyer, K.; Niggemann, B. The predictive value of the skin prick test weal size for the outcome of oral food challenges. Clin. Exp. Allergy 2005, 35, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Calvani, M.; Alessandri, C.; Frediani, T.; Lucarelli, S.; Miceli Sopo, S.; Panetta, V.; Zappalã, D.; Zicari, A.M. Correlation between skin prick test using commercial extract of cow’s milk protein and fresh milk and food challenges. Pediatr. Allergy Immunol. 2007, 18, 583–588. [Google Scholar]
- Calvani, M.; Berti, I.; Fiocchi, A.; Galli, E.; Giorgio, V.; Martelli, A.; Miceli Sopo, S.; Panetta, V. Oral food challenge: Safety, adherence to guidelines and predictive value of skin prick testing. Pediatr. Allergy Immunol. 2012, 23, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Onesimo, R.; Monaco, S.; Greco, M.; Caffarelli, C.; Calvani, M.; Tripodi, S.; Sopo, S.M. Predictive value of MP4 (Milk Prick Four), a panel of skin prick test for the diagnosis of pediatric immediate cow’s milk allergy. Eur. Ann. Allergy Clin. Immunol. 2013, 45, 201–208. [Google Scholar] [PubMed]
- Niederberger, V.; Eckl-Dorna, J.; Pauli, G. Recombinant allergen-based provocation testing. Methods 2014, 66, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Valenta, R.; Karaulov, A.; Niederberger, V.; Zhernov, Y.; Elisyutina, O.; Campana, R.; Focke-Tejkl, M.; Curin, M.; Namazova-Baranova, L.; Wang, J.Y.; et al. Allergen Extracts for In Vivo Diagnosis and Treatment of Allergy: Is There a Future? J. Allergy Clin. Immunol. Pract. 2018, 6, 1845–1855. [Google Scholar] [CrossRef]
- Furuta, G.T.; Liacouras, C.A.; Collins, M.H.; Gupta, S.K.; Justinich, C.; Putnam, P.E.; Bonis, P.; Hassall, E.; Straumann, A.; Rothenberg, M.E. First International Gastrointestinal Eosinophil Research Symposium (FIGERS) Subcommittees. Eosinophilic esophagitis in children and adults: A systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 2007, 133, 1342–1363. [Google Scholar] [CrossRef]
- Canani, R.B.; Buongiovanni, A.; Nocerino, R.; Cosenza, L.; Troncone, R. Toward a standardized reading of the atopy patch test in children with suspected cow’s milk allergy-related gastrointestinal symptoms. Allergy 2011, 66, 1499–1500. [Google Scholar] [CrossRef] [PubMed]
- Mowszet, K.; Matusiewicz, K.; Iwańczak, B. Value of the atopy patch test in the diagnosis of food allergy in children with gastrointestinal symptoms. Adv. Clin. Exp. Med. 2014, 23, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Caglayan Sozmen, S.; Povesi Dascola, C.; Gioia, E.; Mastrorilli, C.; Rizzuti, L.; Caffarelli, C. Diagnostic accuracy of patch test in children with food allergy. Pediatr. Allergy Immunol. 2015, 26, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, M.; Rafiee, E.; Darougar, S.; Mesdaghi, M.; Chavoshzadeh, Z. Is the Atopy Patch Test Reliable in the Evaluation of Food Allergy-Related Atopic Dermatitis? Int. Arch. Allergy Immunol. 2018, 175, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Nocerino, R.; Granata, V.; Di Costanzo, M.; Pezzella, V.; Leone, L.; Passariello, A.; Terrin, G.; Troncone, R.; Berni Canani, R. Atopy patch tests are useful to predict oral tolerance in children with gastrointestinal symptoms related to non-IgE-mediated cow’s milk allergy. Allergy 2013, 68, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; Dutoit, G.; Eigenmann, P.; et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy 2014, 69, 1008–1025. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.T.; Matsui, E.C.; Conover-Walker, M.K.; Wood, R.A. Risk of oral food challenges. J. Allergy Clin. Immunol. 2004, 114, 1164–1168. [Google Scholar] [CrossRef]
- Yanagida, N.; Sato, S.; Asaumi, T.; Ogura, K.; Ebisawa, M. Risk Factors for Severe Reactions during Double-Blind Placebo-Controlled Food Challenges. Int. Arch. Allergy Immunol. 2017, 172, 173–182. [Google Scholar] [CrossRef]
- Matricardi, P.M.; Kleine-Tebbe, J.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalbrse, R.C.; Agache, I.; Asero, R.; Ballmer-Weber, B. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27 (Suppl. 23), 1–250. [Google Scholar] [CrossRef]
- Sievers, S.; Cretich, M.; Gagni, P.; Ahrens, B.; Grishina, G.; Sampson, H.A.; Niggemann, B.; Chiari, M.; Beyer, K. Performance of a polymer coated silicon microarray for simultaneous detection of food allergen-specific IgE and IgG4. Clin. Exp. Allergy 2017, 47, 1057–1068. [Google Scholar] [CrossRef]
- Ahrens, B.; Lopes de Oliveira, L.C.; Grabenhenrich, L.; Schulz, G.; Niggemann, B.; Wahn, U.; Beyer, K. Individual cow’s milk allergens as prognostic markers for tolerance development? Clin. Exp. Allergy 2012, 42, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Petersen, T.H.; Mortz, C.G.; Bindslev-Jensen, C.; Eller, E. Cow’s milk allergic children-Can component-resolved diagnostics predict duration and severity? Pediatr. Allergy Immunol. 2018, 29, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Savilahti, E.M.; Rantanen, V.; Lin, J.S.; Karinen, S.; Saarinen, K.M.; Goldis, M.; Mäkelä, M.J.; Hautaniemi, S.; Savilahti, E.; Sampson, H.A. Early recovery from cow’s milk allergy is associated with decreasing IgE and increasing IgG4 binding to cow’s milk epitopes. J. Allergy Clin. Immunol. 2010, 125, 1315–1321. [Google Scholar] [CrossRef] [PubMed]
- Cerecedo, I.; Zamora, J.; Shreffler, W.G.; Lin, J.; Bardina, L.; Dieguez, M.C.; Wang, J.; Muriel, A.; de la Hoz, B.; Sampson, H.A. Mapping of the IgE and IgG4 sequential epitopes of milk allergens with a peptide microarray-based immunoassay. J. Allergy Clin. Immunol. 2008, 122, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lin, J.; Bardina, L.; Goldis, M.; Nowak-Wegrzyn, A.; Shreffler, W.G.; Sampson, H.A. Correlation of IgE/IgG4 milk epitopes and affinity of milk-specific IgE antibodies with different phenotypes of clinical milk allergy. J. Allergy Clin. Immunol. 2010, 125, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Fedenko, E.; Elisyutina, O.; Shtyrbul, O.; Pampura, A.; Valenta, R.; Lupinek, C.; Khaitov, M. Microarray-based IgE serology improves management of severe atopic dermatitis in two children. Pediatr. Allergy Immunol. 2016, 27, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, K.M.; Westfall, J.E.; Seppo, M.S.; James, A.K.; Tsuang, A.J.; Feustel, P.J.; Sampson, H.A.; Berin, C. Role of maternal elimination diets and human milk IgA in the development of cow’s milk allergy in the infants. Clin. Exp. Allergy 2014, 44, 69–78. [Google Scholar] [CrossRef]
- Tuokkola, J.; Luukkainen, P.; Tapanainen, H.; Kaila, M.; Vaarala, O.; Kenward, M.G.; Virta, L.; Veijola, R.; Simell, O.; Ilonen, J.; et al. Maternal diet during pregnancy and lactation and cow’s milk allergy in offspring. Eur. J. Clin. Nutr. 2016, 70, 554–559. [Google Scholar] [CrossRef]
- Lupinek, C.; Hochwallner, H.; Johansson, C.; Mie, A.; Rigler, E.; Scheynius, A.; Alm, J.; Valenta, R. Maternal allergen-specific IgG might protect the child against allergic sensitization. J. Allergy Clin. Immunol, 2019; in press. [Google Scholar]
- Picariello, G.; De Cicco, M.; Nocerino, R.; Paparo, L.; Mamone, G.; Addeo, F.; Berni Canani, R. Excretion of Dietary Cow’s Milk Derived Peptides into Breast Milk. Front. Nutr. 2019, 12, 6–25. [Google Scholar] [CrossRef]
- Schulmeister, U.; Swoboda, I.; Quirce, S.; de la Hoz, B.; Ollert, M.; Pauli, G.; Valenta, R.; Spitzauer, S. Sensitization to human milk. Clin. Exp. Allergy 2008, 38, 60–68. [Google Scholar] [CrossRef]
- Schocker, F.; Recke, A.; Kull, S.; Worm, M.; Jappe, U. Persistent cow’s milk anaphylaxis from early childhood monitored by IgE and BAT to cow’s and human milk under therapy. Pediatr. Allergy Immunol. 2018, 29, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R.; Groetch, M.; Venter, C. When Should Infants with Cow’s Milk Protein Allergy Use an Amino Acid Formula? A Practical Guide. J. Allergy Clin. Immunol. Pract. 2018, 6, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Dipasquale, V.; Serra, G.; Corsello, G.; Romano, C. Standard and Specialized Infant Formulas in Europe: Making, Marketing, and Health Outcomes. Nutr. Clin. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kiewiet, M.B.G.; Gros, M.; van Neerven, R.J.J.; Faas, M.M.; de Vos, P. Immunomodulating properties of protein hydrolysates for application in cow’s milk allergy. Pediatr. Allergy Immunol. 2015, 26, 206–217. [Google Scholar] [CrossRef] [PubMed]
- von Berg, A.; Filipiak-Pittroff, B.; Krämer, U.; Link, E.; Bollrath, C.; Brockow, I.; Koletzko, S.; Grübl, A.; Heinrich, J.; Wichmann, HE.; et al. GINIplus study group. Preventive effect of hydrolyzed infant formulas persists until age 6 years: Long-term results from the German Infant Nutritional Intervention Study (GINI). J. Allergy Clin. Immunol. 2008, 121, 1442–1447. [Google Scholar] [CrossRef]
- von Berg, A.; Filipiak-Pittroff, B.; Krämer, U.; Hoffmann, B.; Link, E.; Beckmann, C.; Hoffmann, U.; Reinhardt, D.; Grübl, A.; Heinrich, J.; et al. GINIplus study group. Allergies in high-risk schoolchildren after early intervention with cow’s milk protein hydrolysates: 10-year results from the German Infant Nutritional Intervention (GINI) study. J. Allergy Clin. Immunol. 2013, 131, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Cabana, M.D. The Role of Hydrolyzed Formula in Allergy Prevention. Ann. Nutr. Metab. 2017, 70 (Suppl. 2), 38–45. [Google Scholar] [CrossRef]
- Hochwallner, H.; Schulmeister, U.; Swoboda, I.; Focke-Tejkl, M.; Reininger, R.; Civaj, V.; Campana, R.; Thalhamer, J.; Scheiblhofer, S.; Balic, N.; et al. Infant milk formulas differ regarding their allergenic activity and induction of T-cell and cytokine responses. Allergy 2017, 72, 416–424. [Google Scholar] [CrossRef]
- Dupont, C.; Chouraqui, J.P.; Linglart, A.; Bocquet, A.; Darmaun, D.; Feillet, F.; Frelut, M.L.; Girardet, J.P.; Hankard, R.; Rozé, J.C.; et al. Committee on Nutrition of the French Society of Pediatrics. Nutritional management of cow’s milk allergy in children: An update. Arch. Pediatr. 2018, 25, 236–243. [Google Scholar] [CrossRef]
- Doulgeraki, A.E.; Manousakis, E.M.; Papadopoulos, N.G. Bone health assessment of food allergic children on restrictive diets: A practical guide. J. Pediatr. Endocrinol. Metab. 2017, 30, 133–139. [Google Scholar] [CrossRef]
- Souroullas, K.; Aspri, M.; Papademas, P. Donkey milk as a supplement in infant formula: Benefits and technological challenges. Food Res. Int. 2018, 109, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Barni, S.; Sarti, L.; Mori, F.; Muscas, G.; Belli, F.; Pucci, N.; Novembre, E. Tolerability and palatability of donkey’s milk in children with cow’s milk allergy. Pediatr. Allergy Immunol. 2018, 29, 329–331. [Google Scholar] [CrossRef] [PubMed]
- Umpiérrez, A.; Quirce, S.; Marañón, F.; Cuesta, J.; García-Villamuza, Y.; Lahoz, C.; Sastre, J. Allergy to goat and sheep cheese with good tolerance to cow cheese. Clin. Exp. Allergy 1999, 29, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Cases, B.; García-Ara, C.; Boyano, M.T.; Pérez-Gordo, M.; Pedrosa, M.; Vivanco, F.; Quirce, S.; Pastor-Vargas, C. Phosphorylation reduces the allergenicity of cow casein in children with selective allergy to goat and sheep milk. J. Investig. Allergol. Clin. Immunol. 2011, 21, 398–400. [Google Scholar] [PubMed]
- Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [PubMed]
- Candreva, Á.M.; Ferrer-Navarro, M.; Bronsoms, S.; Quiroga, A.; Curciarello, R.; Cauerhff, A.; Petruccelli, S.; Docena, G.H.; Trejo, S.A. Identification of cross-reactive B-cell epitopes between Bos d 9.0101(Bos Taurus) and Gly m 5.0101 (Glycine max) by epitope mapping MALDI-TOF MS. Proteomics 2017, 17, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Bocquet, A.; Dupont, C.; Chouraqui, J.-P.; Darmaun, D.; Feillet, F.; Frelut, M.-L.; Girardet, J.-P.; Hankard, R.; Lapillonne, A.; Rozé, J.-C.; et al. Efficacy and safety of hydrolyzed rice-protein formulas for the treatment of cow’s milk protein allergy. Archives de Pédiatrie 2019, 26, 238–246. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, M.; Han, S.; Ma, S.; Zou, Z.; Ding, F.; Li, X.; Li, L.; Tang, B.; Wang, H.; et al. Production of hypoallergenic milk from DNA-free beta-lactoglobulin (BLG) gene knockout cow using zinc-finger nucleases mRNA. Sci. Rep. 2018, 8, 15430. [Google Scholar] [CrossRef]
- Tan-Lim, C.S.C.; Esteban-Ipac, N.A.R. Probiotics as treatment for food allergies among pediatric patients: A meta-analysis. World Allergy Organ. J. 2018, 11, 25. [Google Scholar] [CrossRef]
- Berni Canani, R.; Di Costanzo, M.; Bedogni, G.; Amoroso, A.; Cosenza, L.; Di Scala, C.; Granata, V.; Nocerino, R. Extensively hydrolyzed casein formula containing Lactobacillus rhamnosus GG reduces the occurrence of other allergic manifestations in children with cow’s milk allergy: 3-year randomized controlled trial. J. Allergy Clin. Immunol. 2017, 139, 1906–1913. [Google Scholar] [CrossRef]
- Schmidt, R.M.; Pilmann Laursen, R.; Bruun, S.; Larnkjaer, A.; Mølgaard, C.; Michaelsen, K.F.; Høst, A. Probiotics in late infancy reduce the incidence of eczema: A randomized controlled trial. Pediatr. Allergy Immunol. 2019, 30, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Lundelin, K.; Poussa, T.; Salminen, S.; Isolauri, E. Long-term safety and efficacy of perinatal probiotic intervention: Evidence from a follow-up study of four randomized, double-blind, placebo-controlled trials. Pediatr. Allergy Immunol. 2017, 28, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.; Barthow, C.; Mitchell, E.A.; Kang, J.; van Zyl, N.; Purdie, G.; Stanley, T.; Fitzharris, P.; Murphy, R.; Crane, J. Effects of Lactobacillus rhamnosus HN001 in early life on the cumulative prevalence of allergic disease to 11 years. Pediatr. Allergy Immunol. 2018, 29, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Boyle, R.J.; Tang, M.L.; Chiang, W.C.; Chua, M.C.; Ismail, I.; Nauta, A.; Hourihane, J.O.B.; Smith, P.; Gold, M.; Ziegler, J.; et al. Prebiotic-supplemented partially hydrolysed cow’s milk formula for the prevention of eczema in high-risk infants: A randomized controlled trial. Allergy 2016, 71, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Wopereis, H.; Sim, K.; Shaw, A.; Warner, J.O.; Knol, J.; Kroll, J.S. Intestinal microbiota in infants at high risk for allergy: Effects of prebiotics and role in eczema development. J. Allergy Clin. Immunol. 2018, 141, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Pajno, G.B.; Fernandez-Rivas, M.; Arasi, S.; Roberts, G.; Akdis, C.A.; Alvaro-Lozano, M.; Beyer, K.; Bindslev-Jensen, C.; Burks, W.; Ebisawa, M.; et al. EAACI Allergen Immunotherapy Guidelines Group. EAACI Guidelines on allergen immunotherapy: IgE-mediated food allergy. Allergy 2018, 73, 799–815. [Google Scholar] [CrossRef] [PubMed]
- Berti, I.; Badina, L.; Cozzi, G.; Giangreco, M.; Bibalo, C.; Ronfani, L.; Barbi, E.; Ventura, A.; Longo, G. Early oral immunotherapy in infants with cow’s milk protein allergy. Pediatr. Allergy Immunol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Yanagida, N.; Sato, S.; Ebisawa, M. Clinical aspects of oral immunotherapy for the treatment of allergies. Semin. Immunol. 2017, 30, 45–51. [Google Scholar] [CrossRef]
- Taniuchi, S.; Takahashi, M.; Soejima, K.; Hatano, Y.; Minami, H. Immunotherapy for cow’s milk allergy. Hum. Vaccin. Immunother. 2017, 13, 2443–2451. [Google Scholar] [CrossRef]
- Longo, G.; Barbi, E.; Berti, I.; Meneghetti, R.; Pittalis, A.; Ronfani, L.; Ventura, A. Specific oral tolerance induction in children with very severe cow’s milk-induced reactions. J. Allergy Clin. Immunol. 2008, 121, 343–347. [Google Scholar] [CrossRef]
- Skripak, J.M.; Nash, S.D.; Rowley, H.; Brereton, N.H.; Oh, S.; Hamilton, R.G.; Matsui, E.C.; Burks, A.W.; Wood, R.A. A randomized, double-blind, placebo-controlled study of milk oral immunotherapy for cow’s milk allergy. J. Allergy Clin. Immunol. 2008, 122, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Pajno, G.B.; Caminiti, L.; Ruggeri, P.; De Luca, R.; Vita, D.; La Rosa, M.; Passalacqua, G. Oral immunotherapy for cow’s milk allergy with a weekly up-dosing regimen: A randomized single-blind controlled study. Ann. Allergy Asthma Immunol. 2010, 105, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Martorell, A.; De La Hoz, B.; Ibáñez, M.D.; Boné, J.; Terrados, M.S.; Michavila, A.; Plaza, A.M.; Alonso, E.; Garde, J.; Nevot, S.; et al. Oral desensitization as a useful treatment in 2-year-old children with cow’s milk allergy. Clin. Exp. Allergy 2011, 41, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Salmivesi, S.; Korppi, M.; Mäkelä, M.J.; Paassilta, M. Milk oral immunotherapy is effective in school-aged children. Acta Paediatr. 2013, 102, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Fariñas, M.; Suprun, M.; Chang, H.L.; Gimenez, G.; Grishina, G.; Getts, R.; Nadeau, K.; Wood, R.A.; Sampson, H.A. Predicting development of sustained unresponsiveness to milk oral immunotherapy using epitope-specific antibody binding profiles. J. Allergy Clin. Immunol. 2019, 143, 1038–1046. [Google Scholar] [CrossRef]
- Kauppila, T.K.; Paassilta, M.; Kukkonen, A.K.; Kuitunen, M.; Pelkonen, A.S.; Makela, M.J. Outcome of oral immunotherapy for persistent cow’s milk allergy from 11 years of experience in Finland. Pediatr. Allergy Immunol. 2019, 30, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Keet, C.A.; Seopaul, S.; Knorr, S.; Narisety, S.; Skripak, J.; Wood, R.A. Long-term follow-up of oral immunotherapy for cow’s milk allergy. J. Allergy Clin. Immunol. 2013, 132, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Manabe, T.; Sato, S.; Yanagida, N.; Hayashi, N.; Nishino, M.; Takahashi, K.; Nagakura, K.I.; Asaumi, T.; Ogura, K.; Ebisawa, M. Long-term outcomes after sustained unresponsiveness in patients who underwent oral immunotherapy for egg, cow’s milk, or wheat allergy. Allergol. Int. 2019. [Google Scholar] [CrossRef] [PubMed]
- De Schryver, S.; Mazer, B.; Clarke, A.E.; St Pierre, Y.; Lejtenyi, D.; Langlois, A.; Torabi, B.; Zhao, W.w.; Chan, E.S.; Ingrid Baerg, R.N. Adverse Events in Oral Immunotherapy for the Desensitization of Cow’s Milk Allergy in Children: A Randomized Controlled Trial. J. Allergy Clin. Immunol. Pract 2019. [Google Scholar] [CrossRef] [PubMed]
- Nadeau, K.C.; Schneider, L.C.; Hoyte, L.; Borras, I.; Umetsu, D.T. Rapid oral desensitization in combination with omalizumab therapy in patients with cow’s milk allergy. J. Allergy Clin. Immunol. 2011, 127, 1622–1624. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Taniuchi, S.; Soejima, K.; Hatano, Y.; Yamanouchi, S.; Kaneko, K. Successful desensitization in a boy with severe cow’s milk allergy by a combination therapy using omalizumab and rush oral immunotherapy. Allergy Asthma Clin. Immunol. 2015, 11, 18. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.A.; Kim, J.S.; Lindblad, R.; Nadeau, K.; Henning, A.K.; Dawson, P.; Plaut, M.; Sampson, H.A. A randomized, double-blind, placebo-controlled study of omalizumab combined with oral immunotherapy for the treatment of cow’s milk allergy. J. Allergy Clin. Immunol. 2016, 137, 1103–1110. [Google Scholar] [CrossRef]
- Martorell-Calatayud, C.; Michavila-Gómez, A.; Martorell-Aragonés, A.; Molini-Menchón, N.; Cerdá-Mir, J.C.; Félix-Toledo, R.; De Las Marinas-Álvarez, M.D. Anti-IgE-assisted desensitization to egg and cow’s milk in patients refractory to conventional oral immunotherapy. Pediatr. Allergy Immunol. 2016, 27, 544–546. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Soejima, K.; Taniuchi, S.; Hatano, Y.; Yamanouchi, S.; Ishikawa, H.; Irahara, M.; Sasaki, Y.; Kido, H.; Kaneko, K. Oral immunotherapy combined with omalizumab for high–risk cow’s milk allergy: A randomized controlled trial. Sci. Rep. 2017, 7, 17453. [Google Scholar] [CrossRef] [PubMed]
- Freeland, D.M.H.; Manohar, M.; Andorf, S.; Hobson, B.D.; Zhang, W.; Nadeau, K.C. Oral immunotherapy for food allergy. Semin. Immunol. 2017, 30, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, H.; Alyasin, S.; Haghighat, M.; Nabavizadeh, H.; Esmaeilzadeh, E.; Mosavat, F. The effect of baked milk on accelerating unheated cow’s milk tolerance: A control randomized clinical trial. Pediatr. Allergy Immunol. 2018, 29, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.R.; Nachshon, L.; Appel, M.Y.; Elizur, A.; Levy, M.B.; Eisenberg, E.; Sampson, H.A.; Katz, Y. Efficacy of baked milk oral immunotherapy in baked milk-reactive allergic patients. J. Allergy Clin. Immunol. 2015, 136, 1601–1606. [Google Scholar] [CrossRef]
- Amat, F.; Kouche, C.; Gaspard, W.; Lemoine, A.; Guiddir, T.; Lambert, N.; Zakariya, M.; Ridray, C.; Nemni, A.; Saint-Pierre, P.; et al. Is a slow-progression baked milk protocol of oral immunotherapy always a safe option for children with cow’s milk allergy? A randomized controlled trial. Clin. Exp. Allergy 2017, 47, 1491–1496. [Google Scholar] [CrossRef]
- Inuo, C.; Tanaka, K.; Suzuki, S.; Nakajima, Y.; Yamawaki, K.; Tsuge, I.; Urisu, A.; Kondo, Y. Oral Immunotherapy Using Partially Hydrolyzed Formula for Cow’s Milk Protein Allergy: A Randomized, Controlled Trial. Int. Arch. Allergy Immunol. 2018, 177, 259–268. [Google Scholar] [CrossRef]
- de Boissieu, D.; Dupont, C. Sublingual immunotherapy for cow’s milk protein allergy: A preliminary report. Allergy 2006, 61, 1238–1239. [Google Scholar] [CrossRef]
- Keet, C.A.; Frischmeyer-Guerrerio, P.A.; Thyagarajan, A.; Schroeder, J.T.; Hamilton, R.G.; Boden, S.; Steele, P.; Driggers, S.; Burks, A.W.; Wood, R.A. The safety and efficacy of sublingual and oral immunotherapy for milk allergy. J. Allergy Clin. Immunol. 2012, 129, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Lanser, B.J.; Leung, D.Y.M. The Current State of Epicutaneous Immunotherapy for Food Allergy: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2018, 55, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Sampson, H.A. Safety and efficacy of epicutaneous immunotherapy for food allergy. Pediatr. Allergy Immunol. 2018, 29, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Dupont, C.; Kalach, N.; Soulaines, P.; Legoué-Morillon, S.; Piloquet, H.; Benhamou, P.H. Cow’s milk epicutaneous immunotherapy in children: A pilot trial of safety, acceptability, and impact on allergic reactivity. J. Allergy Clin. Immunol. 2010, 125, 1165–1167. [Google Scholar] [CrossRef] [PubMed]
- Rutault, K.; Agbotounou, W.; Peillon, A.; Thébault, C.; Vincent, F.; Martin, L. Safety of Viaskin Milk Epicutaneous Immunotherapy (EPIT) in IgE-Mediated Cow’s Milk Allergy (CMA) in Children (MILES Study). J. Allergy Clin. Immunol. 2016, 137, AB132. [Google Scholar] [CrossRef]
- Senti, G.; von Moos, S.; Kündig, TM. Epicutaneous Immunotherapy for Aeroallergen and Food Allergy. Curr. Treat. Options Allergy 2013, 1, 68–78. [Google Scholar] [CrossRef][Green Version]
- Bird, J.A.; Sánchez-Borges, M.; Ansotegui, I.J.; Ebisawa, M.; Ortega Martell, J.A. Skin as an immune organ and clinical applications of skin-based immunotherapy. World Allergy Organ. J. 2018, 11, 38. [Google Scholar] [CrossRef]
- Campana, R.; Moritz, K.; Neubauer, A.; Huber, H.; Henning, R.; Brodie, T.M.; Kaider, A.; Sallusto, F.; Wöhrl, S.; Valenta, R. Epicutaneous allergen application preferentially boosts specific T cell responses in sensitized patients. Sci. Rep. 2017, 7, 11657. [Google Scholar] [CrossRef]
- Zhernov, Y.; Curin, M.; Khaitov, M.; Karaulov, A.; Valenta, R. Recombinant allergens for immunotherapy: State of the art. Curr. Opin. Allergy Clin. Immunol. 2019, in press. [Google Scholar] [CrossRef]
- Dahdah, L.; Ceccarelli, S.; Amendola, S.; Campagnano, P.; Cancrini, C.; Mazzina, O.; Fiocchi, A. IgE Immunoadsorption Knocks Down the Risk of Food-Related Anaphylaxis. Pediatrics 2015, 136, e1617–e1620. [Google Scholar] [CrossRef]
- Lupinek, C.; Derfler, K.; Lee, S.; Prikoszovich, T.; Movadat, O.; Wollmann, E.; Cornelius, C.; Weber, M.; Fröschl, R.; Selb, R.; et al. Extracorporeal IgE Immunoadsorption in Allergic Asthma: Safety and Efficacy. EBioMedicine 2017, 17, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Incorvaia, C.; Riario-Sforza, G.G.; Ridolo, E. IgE Depletion in Severe Asthma: What We Have and What Could Be Added in the Near Future. EBioMedicine 2017, 17, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Artesani, M.C.; Riccardi, C.; Mennini, M.; Pecora, V.; Fierro, V.; Calandrelli, V.; Dahdah, L.; Valluzzi, R.L. Impact of Omalizumab on Food Allergy in Patients Treated for Asthma: A Real-Life Study. J. Allergy Clin. Immunol. Pract. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Noon, L. Prophylactic inoculation against hayfever. Lancet 1911, 4, 1572. [Google Scholar] [CrossRef]
- Curin, M.; Khaitov, M.; Karaulov, A.; Namazova-Baranova, L.; Campana, R.; Garib, V.; Valenta, R. Next-Generation of Allergen-Specific Immunotherapies: Molecular Approaches. Curr. Allergy Asthma Rep. 2018, 18, 39. [Google Scholar] [CrossRef] [PubMed]
- Valenta, R.; Karaulov, A.; Niederberger, V.; Gattinger, P.; van Hage, M.; Flicker, S.; Linhart, B.; Campana, R.; Focke-Tejkl, M.; Curin, M.; et al. Molecular Aspects of Allergens and Allergy. Adv. Immunol. 2018, 138, 195–256. [Google Scholar] [PubMed]
- Valenta, R.; Campana, R.; Niederberger, V. Recombinant allergy vaccines based on allergen-derived B cell epitopes. Immunol. Lett. 2017, 189, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Focke-Tejkl, M.; Weber, M.; Niespodziana, K.; Neubauer, A.; Huber, H.; Henning, R.; Stegfellner, G.; Maderegger, B.; Hauer, M.; Stolz, F.; et al. Development and characterization of a recombinant, hypoallergenic, peptide-based vaccine for grass pollen allergy. J. Allergy Clin. Immunol. 2015, 135, 1207–1217. [Google Scholar] [CrossRef]
- Weber, M.; Niespodziana, K.; Linhart, B.; Neubauer, A.; Huber, H.; Henning, R.; Valenta, R.; Focke-Tejkl, M. Comparison of the immunogenicity of BM32, a recombinant hypoallergenic B cell epitope-based grass pollen allergy vaccine with allergen extract-based vaccines. J. Allergy Clin. Immunol. 2017, 140, 1433–1436. [Google Scholar] [CrossRef]
- Zieglmayer, P.; Focke-Tejkl, M.; Schmutz, R.; Lemell, P.; Zieglmayer, R.; Weber, M.; Kiss, R.; Blatt, K.; Valent, P.; Stolz, F.; et al. Mechanisms, safety and efficacy of a B cell epitope-based vaccine for immunotherapy of grass pollen allergy. EBioMedicine 2016, 11, 43–57. [Google Scholar] [CrossRef]
- Niederberger, V.; Neubauer, A.; Gevaert, P.; Zidarn, M.; Worm, M.; Aberer, W.; Malling, H.J.; Pfaar, O.; Klimek, L.; Pfützner, W.; et al. Safety and efficacy of immunotherapy with the recombinant B-cell epitope-based grass pollen vaccine BM32. J. Allergy Clin. Immunol. 2018, 142, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Orengo, J.M.; Radin, A.R.; Kamat, V.; Badithe, A.; Ben, L.H.; Bennett, B.L.; Zhong, S.; Birchard, D.; Limnander, A.; Rafique, A.; et al. Treating cat allergy with monoclonal IgG antibodies that bind allergen and prevent IgE engagement. Nat. Commun. 2018, 9, 1421. [Google Scholar] [CrossRef] [PubMed]
- Swoboda, I.; Bugajska-Schretter, A.; Linhart, B.; Verdino, P.; Keller, W.; Schulmeister, U.; Sperr, W.R.; Valent, P.; Peltre, G.; Quirce, S.; et al. A recombinant hypoallergenic parvalbumin mutant for immunotherapy of IgE-mediated fish allergy. J. Immunol. 2007, 178, 6290–6296. [Google Scholar] [CrossRef] [PubMed]
- Zuidmeer-Jongejan, L.; Huber, H.; Swoboda, I.; Rigby, N.; Versteeg, S.A.; Jensen, B.M.; Quaak, S.; Akkerdaas, J.H.; Blom, L.; Asturias, J.; et al. Development of a hypoallergenic recombinant parvalbumin for first-in-man subcutaneous immunotherapy of fish allergy. Int. Arch. Allergy Immunol. 2015, 166, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Clintrials.gov Identifier NCT02017626, NCT02382718. Available online: https://clinicaltrials.gov/ct2/results?cond=Allergy+to+Fish&term=mCyp+c+1&cntry=&state=&city=&dist= (accessed on 28 June 2019).
- Westman, M.; Lupinek, C.; Bousquet, J.; Andersson, N.; Pahr, S.; Baar, A.; Bergström, A.; Holmström, M.; Stjärne, P.; Lødrup Carlsen, K.C.; et al. Mechanisms for the Development of Allergies Consortium. Early childhood IgE reactivity to pathogenesis-related class 10 proteins predicts allergic rhinitis in adolescence. J. Allergy Clin. Immunol. 2015, 135, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Hatzler, L.; Panetta, V.; Lau, S.; Wagner, P.; Bergmann, R.L.; Illi, S.; Bergmann, K.E.; Keil, T.; Hofmaier, S.; Rohrbach, A.; et al. Molecular spreading and predictive value of preclinical IgE response to Phleum pratense in children with hay fever. J. Allergy Clin. Immunol. 2012, 130, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Asarnoj, A.; Hamsten, C.; Wadén, K.; Lupinek, C.; Andersson, N.; Kull, I.; Curin, M.; Anto, J.; Bousquet, J.; Valenta, R.; et al. Sensitization to cat and dog allergen molecules in childhood and prediction of symptoms of cat and dog allergy in adolescence: A BAMSE/MeDALL study. J. Allergy Clin. Immunol. 2016, 137, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Posa, D.; Perna, S.; Resch, Y.; Lupinek, C.; Panetta, V.; Hofmaier, S.; Rohrbach, A.; Hatzler, L.; Grabenhenrich, L.; Tsilochristou, O.; et al. Evolution and predictive value of IgE responses toward a comprehensive panel of house dust mite allergens during the first 2 decades of life. J. Allergy Clin. Immunol. 2017, 139, 541–549. [Google Scholar] [CrossRef]
- Wickman, M.; Lupinek, C.; Andersson, N.; Belgrave, D.; Asarnoj, A.; Benet, M.; Pinart, M.; Wieser, S.; Garcia-Aymerich, J.; Baar, A.; et al. Detection of IgE Reactivity to a Handful of Allergen Molecules in Early Childhood Predicts Respiratory Allergy in Adolescence. EBioMedicine 2017, 26, 91–99. [Google Scholar] [CrossRef]
- Lupinek, C.; Marth, K.; Niederberger, V.; Valenta, R. Analysis of serum IgE reactivity profiles with microarrayed allergens indicates absence of de novo IgE sensitizations in adults. J. Allergy Clin. Immunol. 2012, 130, 1418–1420. [Google Scholar] [CrossRef]
- Westman, M.; Asarnoj, A.; Hamsten, C.; Wickman, M.; van Hage, M. Windows of opportunity for tolerance induction for allergy by studying the evolution of allergic sensitization in birth cohorts. Semin. Immunol. 2017, 30, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Ohsaki, A.; Venturelli, N.; Buccigrosso, T.M.; Osganian, S.K.; Lee, J.; Blumberg, R.S.; Oyoshi, M.K. Maternal IgG immune complexes induce food allergen-specific tolerance in offspring. J. Exp. Med. 2018, 215, 91–113. [Google Scholar] [CrossRef] [PubMed]
- Campana, R.; Marth, K.; Zieglmayer, P.; Weber, M.; Lupinek, C.; Zhernov, Y.; Elisyutina, O.; Khaitov, M.; Rigler, E.; Westritschnig, K.; et al. Vaccination of nonallergic individuals with recombinant hypoallergenic fragments of birch pollen allergen Bet v 1: Safety, effects, and mechanisms. J. Allergy Clin. Immunol. 2019, 143, 1258–1261. [Google Scholar] [CrossRef] [PubMed]
- Glovsky, M.M.; Ghekiere, L.; Rejzek, E. Effect of maternal immunotherapy on immediate skin test reactivity, specific rye I IgG and IgE antibody, and total IgE of the children. Ann. Allergy 1991, 67, 21–24. [Google Scholar] [PubMed]
- Flicker, S.; Linhart, B.; Wild, C.; Wiedermann, U.; Valenta, R. Passive immunization with allergen-specific IgG antibodies for treatment and prevention of allergy. Immunobiology 2013, 218, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef]
- Perkin, M.R.; Logan, K.; Marrs, T.; Radulovic, S.; Craven, J.; Flohr, C.; Lack, G.; EAT Study Team. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J. Allergy Clin. Immunol. 2016, 137, 1477–1486. [Google Scholar] [CrossRef]
- Szajewska, H.; Horvath, A. Meta-analysis of the evidence for a partially hydrolyzed 100% whey formula for the prevention of allergic diseases. Curr. Med. Res. Opin. 2010, 26, 423–437. [Google Scholar] [CrossRef]
- Alexander, D.D.; Cabana, M.D. Partially hydrolyzed 100% whey protein infant formula and reduced risk of atopic dermatitis: A meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 356–358. [Google Scholar] [CrossRef]
- Gouw, J.W.; Jo, J.; Meulenbroek, L.A.P.M.; Heijjer, T.S.; Kremer, E.; Sandalova, E.; Knulst, A.C.; Jeurink, P.V.; Garssen, J.; Rijnierse, A.; et al. Identification of peptides with tolerogenic potential in a hydrolysed whey-based infant formula. Clin. Exp. Allergy 2018, 48, 1345–1353. [Google Scholar] [CrossRef]
- Ueno, H.M.; Kato, T.; Ohnishi, H.; Kawamoto, N.; Kato, Z.; Kaneko, H.; Kondo, N.; Nakano, T. T-cell epitope-containing hypoallergenic β-lactoglobulin for oral immunotherapy in milk allergy. Pediatr. Allergy Immunol. 2016, 27, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.M.; Kato, T.; Ohnishi, H.; Kawamoto, N.; Kato, Z.; Kaneko, H.; Kondo, N.; Nakano, T. Hypoallergenic casein hydrolysate for peptide-based oral immunotherapy in cow’s milk allergy. J. Allergy Clin. Immunol. 2018, 142, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Rezende, R.M.; Weiner, H.L. History and mechanisms of oral tolerance. Semin. Immunol. 2017, 30, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Campana, R.; Huang, H.J.; Freidl, R.; Linhart, B.; Vrtala, S.; Wekerle, T.; Karaulov, A.; Valenta, R. Recombinant allergen and peptide-based approaches for allergy prevention by oral tolerance. Semin. Immunol. 2017, 30, 67–80. [Google Scholar] [CrossRef] [PubMed]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linhart, B.; Freidl, R.; Elisyutina, O.; Khaitov, M.; Karaulov, A.; Valenta, R. Molecular Approaches for Diagnosis, Therapy and Prevention of Cow’s Milk Allergy. Nutrients 2019, 11, 1492. https://doi.org/10.3390/nu11071492
Linhart B, Freidl R, Elisyutina O, Khaitov M, Karaulov A, Valenta R. Molecular Approaches for Diagnosis, Therapy and Prevention of Cow’s Milk Allergy. Nutrients. 2019; 11(7):1492. https://doi.org/10.3390/nu11071492
Chicago/Turabian StyleLinhart, Birgit, Raphaela Freidl, Olga Elisyutina, Musa Khaitov, Alexander Karaulov, and Rudolf Valenta. 2019. "Molecular Approaches for Diagnosis, Therapy and Prevention of Cow’s Milk Allergy" Nutrients 11, no. 7: 1492. https://doi.org/10.3390/nu11071492
APA StyleLinhart, B., Freidl, R., Elisyutina, O., Khaitov, M., Karaulov, A., & Valenta, R. (2019). Molecular Approaches for Diagnosis, Therapy and Prevention of Cow’s Milk Allergy. Nutrients, 11(7), 1492. https://doi.org/10.3390/nu11071492