Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status—The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
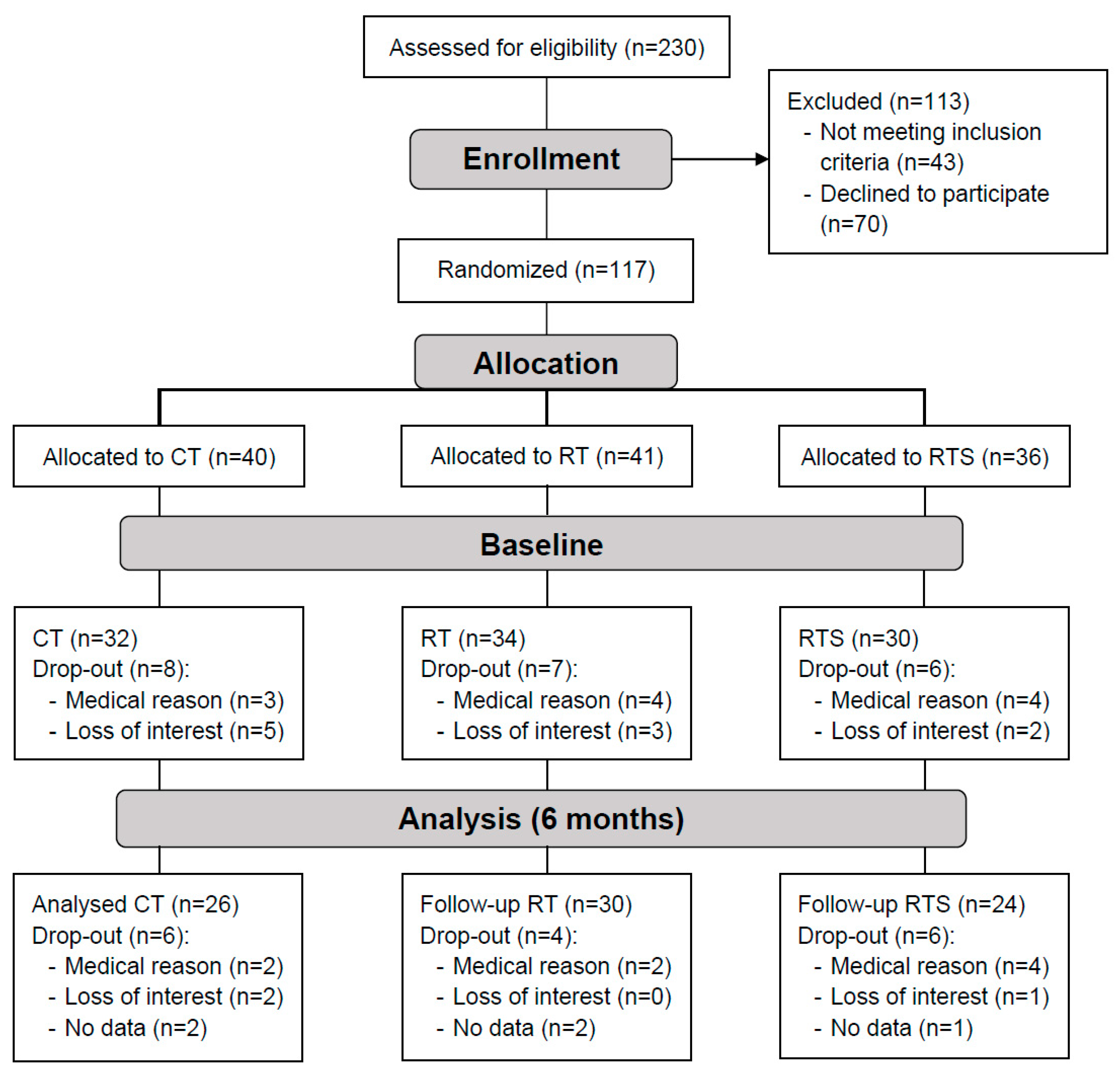
2.2. Study Design
2.3. Resistance Training
2.4. Resistance Training and Supplementation
2.5. Cognitive Training
2.6. Measurements of Plasma Micronutrients
2.7. Dietary Assessment
2.8. Chair Rise Test
2.9. Handgrip Strength
2.10. Six-Minutes-Walking Test
2.11. Isokinetic Dynamometry
2.12. Statistics
3. Results
3.1. Baseline Characteristics of Fat Soluble Micronutrients
3.2. Plasma Status of Fat Soluble Micronutrients of Institutionalized Elderly
3.3. Intervention
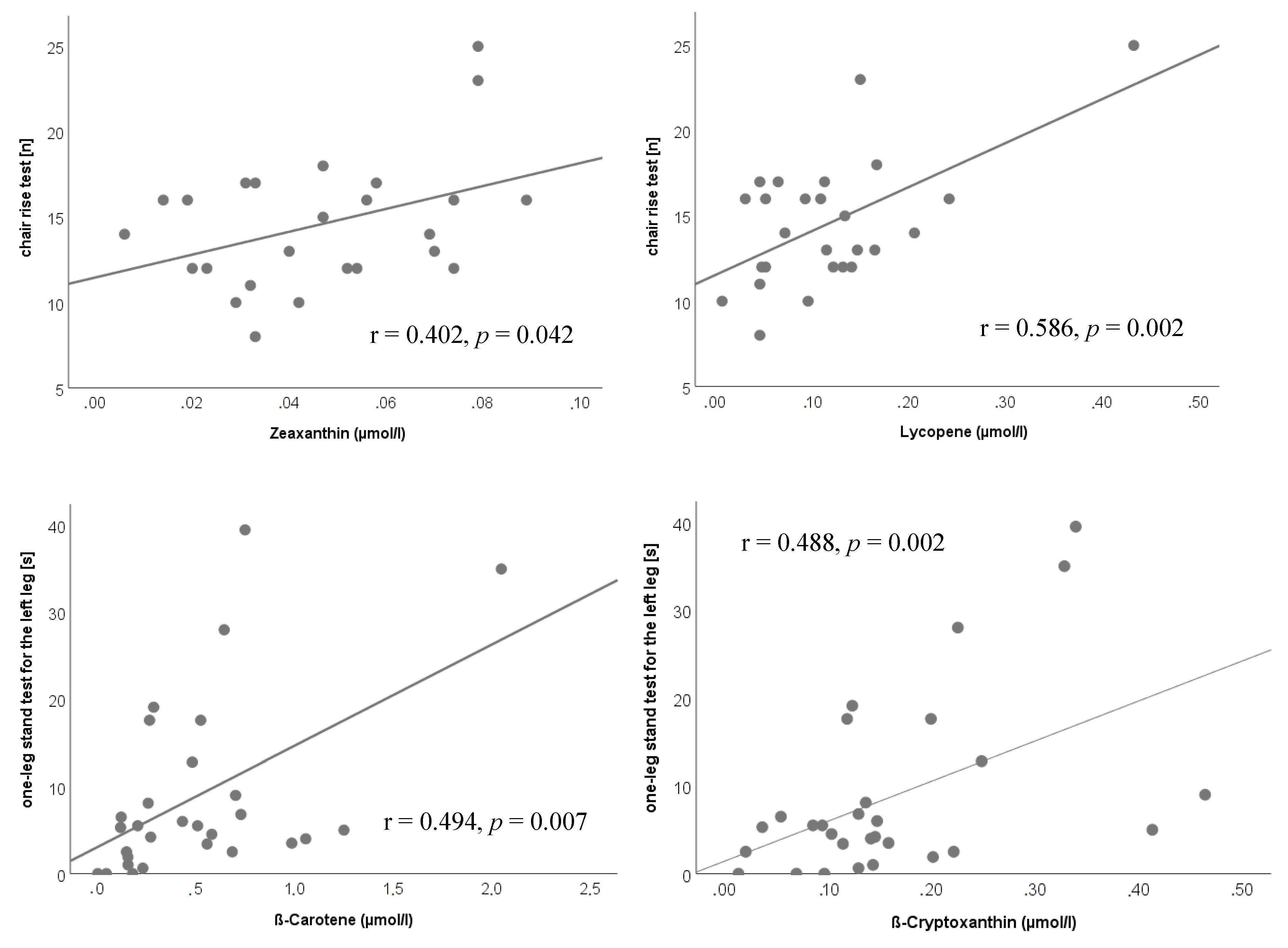
3.4. Correlations after Six Months of Intervention
4. Discussion
4.1. Plasma Status of Fat Soluble Micronutrients of Institutionalized Elderly
4.2. Effect of the Intervention on Plasma Status of Fat Soluble Micronutrients of Institutionalized Elderly
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Franzke, B.; Neubauer, O.; Wagner, K.H. Super DNAging-New insights into DNA integrity, genome stability and telomeres in the oldest old. Mutat. Res. Rev. Mutat. Res. 2015, 766, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Pirlich, M.; Schütz, T.; Norman, K.; Gastell, S.; Lübke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Güldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Shultz, J.M. Impact of aging on eating behaviors, food choices, nutrition, and health status. J. Nutr. Health Aging 2001, 5, 75–79. [Google Scholar] [PubMed]
- Chandra, R.K. Impact of nutritional status and nutrient supplements on immune responses and incidence of infection in older individuals. Ageing Res. Rev. 2004, 3, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Fairfield, K.M.; Fletcher, R.H. Vitamins for chronic disease prevention in adults: Scientific review. JAMA 2002, 287, 3116–3126. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.M. Factors in aging that effect the bioavailability of nutrients. J. Nutr. 2001, 131, 1359S–1361S. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; Ponce, G.; Sánchez Lara, I.; Barrios, R.; Llodra, J.C.; Bravo, M. Association of the oral health impact profile with malnutrition risk in Spanish elders. Arch. Gerontol. Geriatr. 2013, 57, 398–402. [Google Scholar] [CrossRef]
- Nieuwenhuizen, W.F.; Weenen, H.; Rigby, P.; Hetherington, M.M. Older adults and patients in need of nutritional support: Review of current treatment options and factors influencing nutritional intake. Clin. Nutr. 2010, 29, 160–169. [Google Scholar] [CrossRef]
- Smoliner, C.; Norman, K.; Wagner, K.H.; Hartig, W.; Lochs, H.; Pirlich, M. Malnutrition and depression in the institutionalised elderly. Br. J. Nutr. 2009, 102, 1663–1667. [Google Scholar] [CrossRef]
- Muzembo, B.A.; Nagano, Y.; Eitoku, M.; Ngatu, N.R.; Matsui, T.; Bhatti, S.A.; Hirota, R.; Ishida, K.; Suganuma, N. A cross-sectional assessment of oxidative DNA damage and muscle strength among elderly people living in the community. Environ. Health Prev. Med. 2014, 19, 21–29. [Google Scholar] [CrossRef]
- Wakimoto, P.; Block, G. Dietary intake, dietary patterns, and changes with age: An epidemiological perspective. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; Van Loon, L.J.; de Groot, L.C. Dietary Protein Intake in Dutch Elderly People: A Focus on Protein Sources. Nutrients 2015, 7, 9697–9706. [Google Scholar] [CrossRef] [PubMed]
- Roman Viñas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Serra Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.R. Vitamins in aging, health, and longevity. Clin. Interv. Aging 2006, 1, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Lesourd, B. Nutrition: A major factor influencing immunity in the elderly. J. Nutr. Health Aging 2004, 8, 28–37. [Google Scholar] [PubMed]
- Ames, B.N. Prolonging healthy aging: Longevity vitamins and proteins. Proc. Natl. Acad. Sci. USA 2018, 115, 10836–10844. [Google Scholar] [CrossRef] [PubMed]
- Mankowski, R.T.; Anton, S.D.; Buford, T.W.; Leeuwenburgh, C. Dietary Antioxidants as Modifiers of Physiologic Adaptations to Exercise. Med. Sci. Sports. Exerc. 2015, 47, 1857–1868. [Google Scholar] [CrossRef]
- Franzke, B.; Schober-Halper, B.; Hofmann, M.; Oesen, S.; Tosevska, A.; Henriksen, T.; Poulsen, H.E.; Strasser, E.M.; Wessner, B.; Wagner, K.H. Age and the effect of exercise, nutrition and cognitive training on oxidative stress—The Vienna Active Aging Study (VAAS), a randomized controlled trial. Free Radic. Biol. Med. 2018, 121, 69–77. [Google Scholar] [CrossRef]
- Neubauer, O.; Yfanti, C. Antioxidants in Athlete’s Basic Nutrition. In Antioxidants in Sport Nutrition; Lamprecht, M., Ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015. [Google Scholar]
- Mason, S.A.; Morrison, D.; McConell, G.K.; Wadley, G.D. Muscle redox signalling pathways in exercise. Role of antioxidants. Free Radic. Biol. Med. 2016, 98, 29–45. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am. J. Clin. Nutr. 2004, 79, 362–371. [Google Scholar] [CrossRef]
- Wang, S. Epidemiology of vitamin D in health and disease. Nutr. Res. Rev. 2009, 22, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Jorde, R.; Peasey, A.; Thorand, B.; Jansen, E.H.; Groot, L.; Streppel, M.; Gardiner, J.; Ordóñez-Mena, J.M.; Perna, L.; et al. Vitamin D and mortality: Meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. BMJ 2014, 348, g3656. [Google Scholar] [CrossRef] [PubMed]
- Heath, A.K.; Kim, I.Y.; Hodge, A.M.; English, D.R.; Muller, D.C. Vitamin D Status and Mortality: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public. Health 2019, 16, 383. [Google Scholar] [CrossRef] [PubMed]
- Franzke, B.; Halper, B.; Hofmann, M.; Oesen, S.; Peherstorfer, H.; Krejci, K.; Koller, B.; Geider, K.; Baierl, A.; Tosevska, A.; et al. The influence of age and aerobic fitness on chromosomal damage in Austrian institutionalised elderly. Mutagenesis 2014, 29, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Franzke, B.; Halper, B.; Hofmann, M.; Oesen, S.; Pierson, B.; Cremer, A.; Bacher, E.; Fuchs, B.; Baierl, A.; Tosevska, A.; et al. The effect of six months of elastic band resistance training, nutritional supplementation or cognitive training on chromosomal damage in institutionalized elderly. Exp. Gerontol. 2015, 65, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Halper, B.; Hofmann, M.; Oesen, S.; Franzke, B.; Stuparits, P.; Vidotto, C.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; et al. Influence of age and physical fitness on miRNA-21, TGF-β and its receptors in leukocytes of healthy women. Exerc. Immunol. Rev. 2015, 21, 154–163. [Google Scholar] [PubMed]
- Hofmann, M.; Halper, B.; Oesen, S.; Franzke, B.; Stuparits, P.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; Ploder, M.; et al. Serum concentrations of insulin-like growth factor-1, members of the TGF-beta superfamily and follistatin do not reflect different stages of dynapenia and sarcopenia in elderly women. Exp. Gerontol. 2015, 64, 35–45. [Google Scholar] [CrossRef]
- Strasser, E.M.; Hofmann, M.; Franzke, B.; Schober-Halper, B.; Oesen, S.; Jandrasits, W.; Graf, A.; Praschak, M.; Horvath-Mechtler, B.; Krammer, C.; et al. Strength training increases skeletal muscle quality but not muscle mass in old institutionalized adults: A randomized, multi-arm parallel and controlled intervention study. Eur. J. Phys. Rehabil. Med. 2018, 54, 921–933. [Google Scholar] [CrossRef]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly—A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]
- Franzke, B.; Halper, B.; Hofmann, M.; Oesen, S.; Jandrasits, W.; Baierl, A.; Tosevska, A.; Strasser, E.M.; Wessner, B.; Wagner, K.H.; et al. The impact of six months strength training, nutritional supplementation or cognitive training on DNA damage in institutionalised elderly. Mutagenesis 2015, 30, 147–153. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C.; Medicine, A.C.O.S.; Association, A.H. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Gatterer, G.; Croy, A. Mental Fitness in Aging; Springer: Vienna, Australia, 2004; Volumes 1–3, p. 77. [Google Scholar]
- Neubauer, O.; Reichhold, S.; Nics, L.; Hoelzl, C.; Valentini, J.; Stadlmayr, B.; Knasmüller, S.; Wagner, K.H. Antioxidant responses to an acute ultra-endurance exercise: Impact on DNA stability and indications for an increased need for nutritive antioxidants in the early recovery phase. Br. J. Nutr. 2010, 104, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Ratzinger, F.; Haslacher, H.; Stadlberger, M.; Schmidt, R.L.; Obermüller, M.; Schmetterer, K.G.; Perkmann, T.; Makristathis, A.; Marculescu, R.; Burgmann, H. 25(OH)D and 1,25(OH)D vitamin D fails to predict sepsis and mortality in a prospective cohort study. Sci. Rep. 2017, 7, 40646. [Google Scholar] [CrossRef] [PubMed]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- DGE; ÖGE; SGE. D-A-CH Nutritional Reference Values; Deutsche Gesellschaft für Ernährung (DGE); Österreichische Gesellschaft für Ernährung (ÖGE); Schweizerische Gesellschaft für Ernährung (SGE): Bonn, Germany, 2017; Volume 2. [Google Scholar]
- Stuetz, W.; Weber, D.; Dollé, M.E.; Jansen, E.; Grubeck-Loebenstein, B.; Fiegl, S.; Toussaint, O.; Bernhardt, J.; Gonos, E.S.; Franceschi, C.; et al. Plasma Carotenoids, Tocopherols, and Retinol in the Age-Stratified (35–74 Years) General Population: A Cross-Sectional Study in Six European Countries. Nutrients 2016, 8, 614. [Google Scholar] [CrossRef] [PubMed]
- Elmadfa, I.; Hasenegger, V.; Wagner, K.; Putz, P.; Weidl, N.-M.; Wottawa, D.; Kuen, T.; Seiringer, G.; Meyer, A.L.; Sturtzel, B.; et al. Österreichischer Ernährungsbericht 2012 [Austrian Nutrition Report 2012, in German], 1st ed.; Federal Ministry of Health: Vienna, Austria, 2012. [Google Scholar]
- Dawson-Hughes, B.; Mithal, A.; Bonjour, J.P.; Boonen, S.; Burckhardt, P.; Fuleihan, G.E.; Josse, R.G.; Lips, P.; Morales-Torres, J.; Yoshimura, N. IOF position statement: Vitamin D recommendations for older adults. Osteoporos. Int. 2010, 21, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.Y.; Flicker, L. Hypovitaminosis D and frailty: Epiphenomenon or causal? Maturitas 2015, 82, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, O.H.; Lund, B.; Saltin, B.; Andersen, R.B.; Hjorth, L.; Melsen, F.; Mosekilde, L. Myopathy in bone loss of ageing: Improvement by treatment with 1 alpha-hydroxycholecalciferol and calcium. Clin. Sci. (Lond.) 1979, 56, 157–161. [Google Scholar] [CrossRef]
- Sato, Y.; Iwamoto, J.; Kanoko, T.; Satoh, K. Low-dose vitamin D prevents muscular atrophy and reduces falls and hip fractures in women after stroke: A randomized controlled trial. Cereb. Dis. 2005, 20, 187–192, Retracted in Cerebrovasc. Dis. 2017, 44, 240. [Google Scholar] [CrossRef]
- Ceglia, L.; Niramitmahapanya, S.; da Silva Morais, M.; Rivas, D.A.; Harris, S.S.; Bischoff-Ferrari, H.; Fielding, R.A.; Dawson-Hughes, B. A randomized study on the effect of vitamin D₃ supplementation on skeletal muscle morphology and vitamin D receptor concentration in older women. J. Clin. Endocrinol. Metab. 2013, 98, E1927–E1935. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; Ortega, R.M.; Andrés, P.; Aparicio, A.; González-Rodríguez, L.G.; López-Sobaler, A.M.; Navia, B.; Perea, J.M.; Rodríguez-Rodríguez, P. Antioxidant status in a group of institutionalised elderly people with chronic obstructive pulmonary disease. Br. J. Nutr. 2016, 115, 1740–1747. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Faliva, M.A.; Peroni, G.; Moncaglieri, F.; Infantino, V.; Naso, M.; Perna, S. Focus on Pivotal Role of Dietary Intake (Diet and Supplement) and Blood Levels of Tocopherols and Tocotrienols in Obtaining Successful Aging. Int. J. Mol. Sci. 2015, 16, 23227–23249. [Google Scholar] [CrossRef] [PubMed]
- Sauberlich, H. Laboratory Tests for the Assessment of Nutritional Status, 2nd ed.; CRC Press: Boca Raton, FL, USA; London, UK; New York, NY, USA; Washington, DC, USA, 1999. [Google Scholar]
- Pilleron, S.; Weber, D.; Pérès, K.; Colpo, M.; Gomez-Cabrero, D.; Stuetz, W.; Dartigues, J.F.; Ferrucci, L.; Bandinelli, S.; Garcia-Garcia, F.J.; et al. Patterns of circulating fat-soluble vitamins and carotenoids and risk of frailty in four European cohorts of older adults. Eur. J. Nutr. 2019, 58, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Laird, E.; Ward, M.; McSorley, E.; Strain, J.J.; Wallace, J. Vitamin D and bone health: Potential mechanisms. Nutrients 2010, 2, 693–724. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.R.; Aspray, T.J. The role of vitamin D in maintaining bone health in older people. Adv. Musculoskelet. Dis. 2017, 9, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Burleigh, E.; Potter, J. Vitamin D deficiency in outpatients: A Scottish perspective. Scott. Med. J. 2006, 51, 27–31. [Google Scholar] [CrossRef]
- Pilz, S.; Dobnig, H.; Tomaschitz, A.; Kienreich, K.; Meinitzer, A.; Friedl, C.; Wagner, D.; Piswanger-Sölkner, C.; März, W.; Fahrleitner-Pammer, A. Low 25-hydroxyvitamin D is associated with increased mortality in female nursing home residents. J. Clin. Endocrinol. Metab. 2012, 97, E653–E657. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Plasma Status at Study Entry | Reference Plasma Value | % of Deficient Participants |
|---|---|---|---|
| Subjects [number] | 96 | ||
| Age [years] | 83.1 (65–98) | ||
| Retinol [µmol/L] | 2.20 (1.05–4.16) | >1.05 | 0% |
| Lutein [µmol/L] | 0.25 (0.04–2.03) | ||
| Zeaxanthin [µmol/L] | 0.040 (n.d.–0.19) | ||
| Lycopene [µmol/L] | 0.009 (n.d.–0.37) | ||
| β-Cryptoxanthin [µmol/L] | 0.18 (n.d.–0.80) | ||
| α-Carotene [µmol/L] | 0.05 (n.d.–0.46) | ||
| β-Carotene [µmol/L] | 0.42 (n.d.–2.4) | >0.75 | 73% |
| α-Tocopherol [µmol/L] | 16.51 (n.d.–26.8) | >11.6 | 33% |
| γ-Tocopherol [µmol/L] | 2.63 (1.80–9.14) | ||
| Vitamin D [nmol/L] | 44.0 (9.0–162) | >50/75 | 61%/81% |
| Data are median (Min–Max), n.d. not detectable | |||
| RT | RTS | CT | ||||
|---|---|---|---|---|---|---|
| Baseline | 6 Mo | Baseline | 6 Mo | Baseline | 6 Mo | |
| Subjects [number] | 34 | 30 | 30 | 24 | 32 | 26 |
| BMI [kg/m2] | 29.0 ± 3.7 | 29.0 ± 3.9 | 30.0 ± 6.3 | 30.0 ± 5.4 | 28.6 ± 4.9 | 27.9 ± 5.3 |
| Retinol [µmol/L] | 2.14 ± 0.50 | 2.31 ± 0.49 * | 2.15 ± 0.49 | 2.28 ± 0.66 | 2.46 ± 0.67 | 2.47 ± 0.53 |
| Lutein [µmol/L] | 0.31 ± 0.34 | 0.28 ± 0.23 | 0.33 ± 0.22 | 0.28 ± 0.19 | 0.40 ± 0.39 | 0.50 ± 1.09 |
| Zeaxanthin [µmol/L] | 0.04 ± 0.02 | 0.05 ± 0.03 | 0.05 ± 0.03 | 0.05 ± 0.03 | 0.06 ± 0.04 | 0.07 ± 0.06 |
| Lycopene [µmol/L] | 0.09 ± 0.08 | 0.10 ± 0.08 * | 0.11 ± 0.07 | 0.10 ± 0.07 | 0.12 ± 0.07 | 0.11 ± 0.08 |
| β-Cryptoxanthin [µmol/L] | 0.16 ± 0.10 | 0.16 ± 0.11 | 0.23 ± 0.13 | 0.18 ± 0.15 | 0.24 ± 0.18 | 0.21 ± 0.14 |
| α-Carotene [µmol/L] | 0.05 ± 0.10 | 0.09 ± 0.14 | 0.10 ± 0.12 | 0.12 ± 0.11 | 0.08 ± 0.07 | 0.12 ± 0.12 |
| β-Carotene [µmol/L] | 0.41 ± 0.44 | 0.49 ± 0.43 | 0.61 ± 0.45 | 0.55 ± 0.51 | 0.68 ± 0.51 | 0.67 ± 0.46 |
| α-Tocopherol [µmol/L] | 19.94 ± 13.96 | 21.03 ± 14.62 | 21.47 ± 17.04 | 21.17 ± 19.61 | 19.48 ± 14.50 | 19.73 ± 15.02 |
| γ-Tocopherol [µmol/L] | 4.81 ± 5.84 | 4.72 ± 4.71 | 3.26 ± 3.07 | 2.84 ± 2.54 | 3.52 ± 3.33 | 3.59 ± 3.43 |
| Vitamin D [µmol/L] | 54.12 ± 27.6 | 55.98 ± 25.56 | 59.35 ± 41.48 | 66.33 ± 35.04 | 46.9 ± 31.02 | 53.04 ± 25.13 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzke, B.; Schober-Halper, B.; Hofmann, M.; Oesen, S.; Tosevska, A.; Strasser, E.-M.; Marculescu, R.; Wessner, B.; Wagner, K.-H. Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status—The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial. Nutrients 2019, 11, 1333. https://doi.org/10.3390/nu11061333
Franzke B, Schober-Halper B, Hofmann M, Oesen S, Tosevska A, Strasser E-M, Marculescu R, Wessner B, Wagner K-H. Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status—The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial. Nutrients. 2019; 11(6):1333. https://doi.org/10.3390/nu11061333
Chicago/Turabian StyleFranzke, Bernhard, Barbara Schober-Halper, Marlene Hofmann, Stefan Oesen, Anela Tosevska, Eva-Maria Strasser, Rodrig Marculescu, Barbara Wessner, and Karl-Heinz Wagner. 2019. "Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status—The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial" Nutrients 11, no. 6: 1333. https://doi.org/10.3390/nu11061333
APA StyleFranzke, B., Schober-Halper, B., Hofmann, M., Oesen, S., Tosevska, A., Strasser, E.-M., Marculescu, R., Wessner, B., & Wagner, K.-H. (2019). Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status—The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial. Nutrients, 11(6), 1333. https://doi.org/10.3390/nu11061333