Polyunsaturated Fatty Acids and Glycemic Control in Type 2 Diabetes

Abstract
1. Introduction
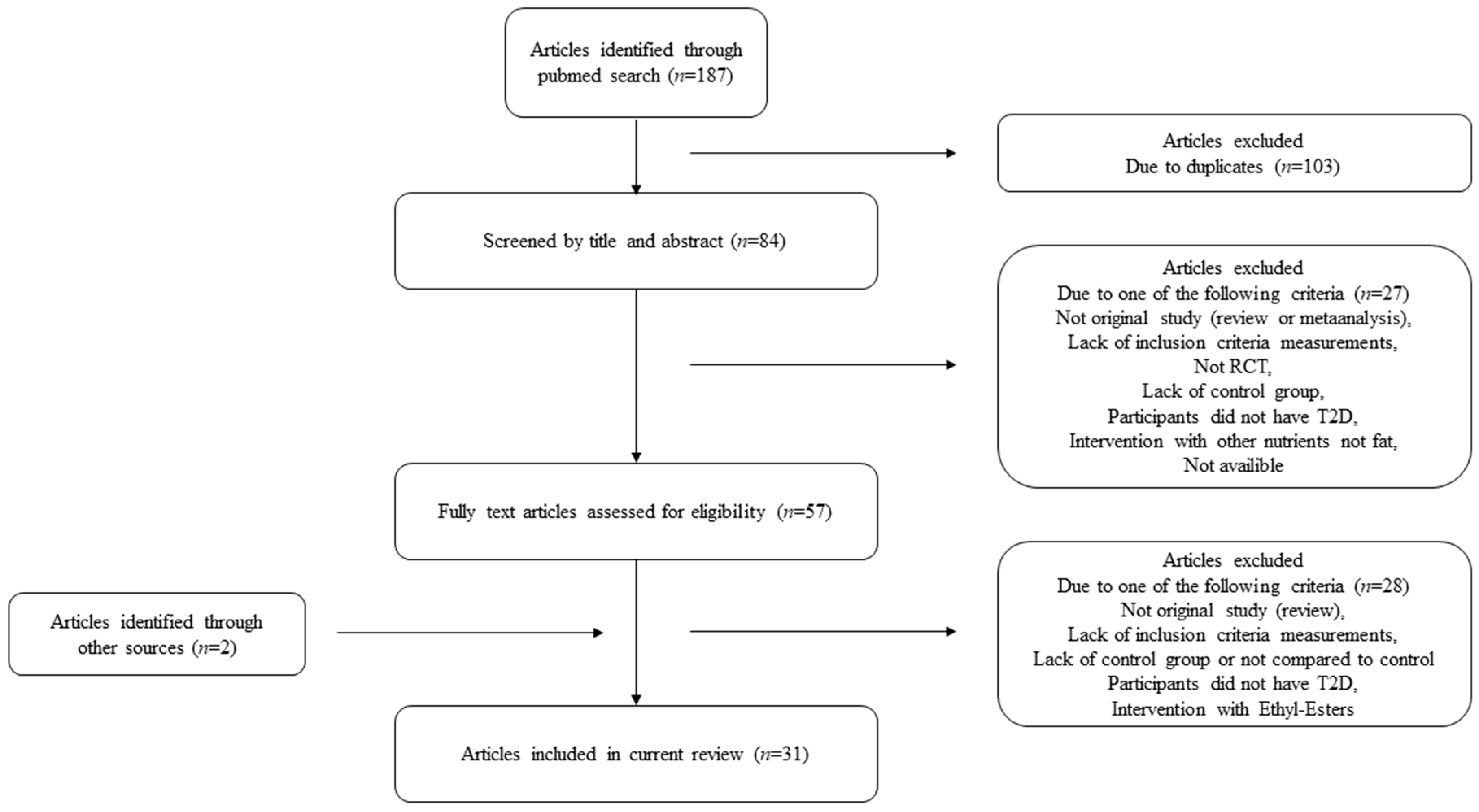
2. Materials and Methods
3. Results and Discussion
3.1. Fish and Fish Oil
3.2. Vegetable Oils
3.3. Nuts
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 30 March 2019).
- World Health Organization. Global Report on Diabetes; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Diabetes. 2018. Available online: https://www.who.int/en/news-room/fact-sheets/detail/diabetes (accessed on 30 March 2019).
- Yoo, J.Y.; Kim, S.S. Probiotics and Prebiotics: Present Status and Future Perspectives on Metabolic Disorders. Nutrients 2016, 8, 173. [Google Scholar] [CrossRef] [PubMed]
- Ulven, S.M.; Leder, L.; Elind, E.; Ottestad, I.; Christensen, J.J.; Telle-Hansen, V.H.; Skjetne, A.J.; Raael, E.; Sheikh, N.A.; Holck, M.; et al. Exchanging a few commercial, regularly consumed food items with improved fat quality reduces total cholesterol and LDL-cholesterol: A double-blind, randomised controlled trial. Br. J. Nutr. 2016, 116, 1383–1393. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 379, 1387–1389. [Google Scholar] [PubMed]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar]
- Lim, E.L.; Hollingsworth, K.G.; Aribisala, B.S.; Chen, M.J.; Mathers, J.C.; Taylor, R. Reversal of type 2 diabetes: Normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011, 54, 2506–2514. [Google Scholar] [CrossRef] [PubMed]
- Barnard, N.D.; Katcher, H.I.; Jenkins, D.J.; Cohen, J.; Turner-McGrievy, G. Vegetarian and vegan diets in type 2 diabetes management. Nutr. Rev. 2009, 67, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Barnard, R.J.; Jung, T.; Inkeles, S.B. Diet and exercise in the treatment of NIDDM. The need for early emphasis. Diabetes Care 1994, 17, 1469–1472. [Google Scholar] [CrossRef] [PubMed]
- O’Flaherty, M.; Flores-Mateo, G.; Nnoaham, K.; Lloyd-Williams, F.; Capewell, S. Potential cardiovascular mortality reductions with stricter food policies in the United Kingdom of Great Britain and Northern Ireland. Bull. World Health Organ. 2012, 90, 522–531. [Google Scholar] [CrossRef]
- Schwab, U.; Lauritzen, L.; Tholstrup, T.; Haldorsson, T.I.; Risérus, U.; Uusitupa, M.; Becker, W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: A systematic review. Food Nutr. Res. 2014, 58, 25145. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Micha, R.; Wallace, S. Effects on Coronary Heart Disease of Increasing Polyunsaturated Fat in Place of Saturated Fat: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS Med. 2010, 7, e1000252. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, M.U.; O’Reilly, E.J.; Heitmann, B.L.; Pereira, M.A.; Bälter, K.; Fraser, G.E.; Goldbourt, U.; Hallmans, G.; Knekt, P.; Liu, S.; et al. Major types of dietary fat and risk of coronary heart disease: A pooled analysis of 11 cohort studies123. Am. J. Clin. Nutr. 2009, 89, 1425–1432. [Google Scholar] [CrossRef]
- Kinsell, L.W.; Michaels, G.D.; Olson, F.E.; Coelho, M.; McBride, Y.; Fukayama, G.; Conklin, J.; Walker, G. Dietary Fats and the Diabetic Patient. N. Engl. J. Med. 1959, 261, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Mann, J. Nutrition Recommendations for the Treatment and Prevention of Type 2 Diabetes and the Metabolic Syndrome: An Evidenced-Based Review. Nutr. Rev. 2006, 64, 422–427. [Google Scholar] [CrossRef]
- Riserus, U.; Willett, W.C.; Hu, F.B. Dietary fats and prevention of type 2 diabetes. Prog. Lipid Res. 2009, 48, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Wu, J.H.Y.; Otto, M.C.D.O.; Otite, F.O.; Abioye, A.I.; Mozaffarian, D. Effects of Saturated Fat, Polyunsaturated Fat, Monounsaturated Fat, and Carbohydrate on Glucose-Insulin Homeostasis: A Systematic Review and Meta-analysis of Randomised Controlled Feeding Trials. PLoS Med. 2016, 13, 1002087. [Google Scholar] [CrossRef]
- Coelho, O.G.L.; da Silva, B.P.; Rocha, D.M.U.P.; Lopes, L.L.; Alfenas, R.C.G. Polyunsaturated fatty acids and type 2 diabetes: Impact on the glycemic control mechanism. Crit. Rev. Food Sci. Nutr. 2017, 57, 3614–3619. [Google Scholar] [CrossRef]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R.; Folsom, A.R. Dietary Fat and Incidence of Type 2 Diabetes in Older Iowa Women. Diabetes Care 2001, 24, 1528–1535. [Google Scholar] [CrossRef]
- Salmerón, J.; Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.A.; Rimm, E.B.; Willett, W.C. Dietary fat intake and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2001, 73, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Hartweg, J.; Perera, R.; Montori, V.M.; Dinneen, S.F.; Neil, A.H.; Farmer, A.J. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef] [PubMed]
- Wanders, A.J.; Blom, W.A.M.; Zock, P.L.; Geleijnse, J.M.; Brouwer, I.A.; Alssema, M. Plant-derived polyunsaturated fatty acids and markers of glucose metabolism and insulin resistance: A meta-analysis of randomized controlled feeding trials. BMJ Open Diabetes Res. Care 2019, 7, e000585. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Y.; Zhu, Y.; Liu, X.; Xia, H.; Yang, X.; Sun, G. Treatment for 6 months with fish oil-derived n-3 polyunsaturated fatty acids has neutral effects on glycemic control but improves dyslipidemia in type 2 diabetic patients with abdominal obesity: A randomized, double-blind, placebo-controlled trial. Eur. J. Nutr. 2017, 56, 2415–2422. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.S.; Lin, M.; Fang, L.; Yu, Y.; Yuan, L.; Jin, Y.; Feng, J.; Wang, L.; Yang, H.; Chen, W.; et al. Effects of n-3 fatty acid supplements on glycemic traits in Chinese type 2 diabetic patients: A double-blind randomized controlled trial. Mol. Nutr. Food Res. 2016, 60, 2176–2184. [Google Scholar] [CrossRef]
- Balfegó, M.; Canivell, S.; Hanzu, F.A.; Sala-Vila, A.; Martínez-Medina, M.; Murillo, S.; Mur, T.; Ruano, E.G.; Linares, F.; Porras, N.; et al. Effects of sardine-enriched diet on metabolic control, inflammation and gut microbiota in drug-naïve patients with type 2 diabetes: A pilot randomized trial. Lipids Heal. 2016, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Sarbolouki, S.; Javanbakht, M.; Derakhshanian, H.; Hosseinzadeh, P.; Zareei, M.; Hashemi, S.; Dorosty, A.; Eshraghian, M.; Djalali, M. Eicosapentaenoic acid improves insulin sensitivity and blood sugar in overweight type 2 diabetes mellitus patients: A double-blind randomised clinical trial. Singap. Med. J. 2013, 54, 387–390. [Google Scholar] [CrossRef]
- Ogawa, S.; Abe, T.; Nako, K.; Okamura, M.; Senda, M.; Sakamoto, T.; Ito, S. Eicosapentaenoic Acid Improves Glycemic Control in Elderly Bedridden Patients with Type 2 Diabetes. Tohoku J. Exp. Med. 2013, 231, 63–74. [Google Scholar] [CrossRef][Green Version]
- Crochemore, I.C.C.; Souza, A.F.; de Souza, A.C.; Rosado, E.L. Omega-3 polyunsaturated fatty acid supplementation does not influence body composition, insulin resistance, and lipemia in women with type 2 diabetes and obesity. Nutr. Clin. Pract. 2012, 27, 553–560. [Google Scholar] [CrossRef]
- Pooya, S.; Jalali, M.D.; Jazayery, A.D.; Saedisomeolia, A.; Eshraghian, M.R.; Toorang, F. The efficacy of omega-3 fatty acid supplementation on plasma homocysteine and malondialdehyde levels of type 2 diabetic patients. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, H.; Petersen, M.; Major-Pedersen, A.; Jensen, T.; Nielsen, N.S.; Lauridsen, S.T.; Marckmann, P. Influence of fish oil supplementation on in vivo and in vitro oxidation resistance of low-density lipoprotein in type 2 diabetes. Eur. J. Clin. Nutr. 2003, 57, 713–720. [Google Scholar] [CrossRef]
- Luo, J.; Rizkalla, S.W.; Vidal, H.; Oppert, J.-M.; Colas, C.; Boussairi, A.; Guerre-Millo, M.; Chapuis, A.-S.; Chevalier, A.; Durand, G.; et al. Moderate Intake of n-3 Fatty Acids for 2 Months Has No Detrimental Effect on Glucose Metabolism and Could Ameliorate the Lipid Profile in Type 2 Diabetic Men: Results of a controlled study. Diabetes Care 1998, 21, 717–724. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Mori, T.A.; Puddey, I.B.; Beilin, L.J.; Burke, V.; Morton, A.R.; Stanton, K.G. The Independent and Combined Effects of Aerobic Exercise and Dietary Fish Intake on Serum Lipids and Glycemic Control in NIDDM: A randomized controlled study. Diabetes Care 1997, 20, 913–921. [Google Scholar] [CrossRef]
- McManus, R.M.; Jumpson, J.; Finegood, D.T.; Clandinin, M.T.; Ryan, E.A. A Comparison of the Effects of n-3 Fatty Acids from Linseed Oil and Fish Oil in Well-Controlled Type II Diabetes. Diabetes Care 1996, 19, 463–467. [Google Scholar] [CrossRef]
- Morgan, W.A.; Raskin, P.; Rosenstock, J. A Comparison of Fish Oil or Corn Oil Supplements in Hyperlipidemic Subjects with NIDDM. Diabetes Care 1995, 18, 83–86. [Google Scholar] [CrossRef][Green Version]
- Annuzzi, G.; Rivellese, A.; Capaldo, B.; Di Marino, L.; Iovine, C.; Marotta, G.; Riccardi, G. A controlled study on the effects of n − 3 fatty acids on lipid and glucose metabolism in non-insulin-dependent diabetic patients. Atherosclerosis 1991, 87, 65–73. [Google Scholar] [CrossRef]
- Borkman, M.; Chisholm, D.J.; Furler, S.M.; Storlien, L.H.; Kraegen, E.W.; Simons, L.A.; Chesterman, C.N. Effects of Fish Oil Supplementation on Glucose and Lipid Metabolism in NIDDM. Diabetes 1989, 38, 1314–1319. [Google Scholar] [CrossRef]
- Zibaeenezhad, M.; Aghasadeghi, K.; Hakimi, H.; Yarmohammadi, H.; Nikaein, F. The Effect of Walnut Oil Consumption on Blood Sugar in Patients with Diabetes Mellitus Type 2. Int. J. Endocrinol. Metab. 2016, 14, e34889. [Google Scholar]
- Foster, M.; Petocz, P.; Caterson, I.D.; Samman, S. Effects of zinc and α-linolenic acid supplementation on glycemia and lipidemia in women with type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled trial. J. Diabetes Res. Clin. Metab. 2013, 2, 3–9. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kendall, C.W.; Vuksan, V.; Faulkner, D.; Augustin, L.S.; Mitchell, S.; Ireland, C.; Srichaikul, K.; Mirrahimi, A.; Chiavaroli, L.; et al. Effect of Lowering the Glycemic Load With Canola Oil on Glycemic Control and Cardiovascular Risk Factors: A Randomized Controlled Trial. Diabetes Care 2014, 37, 1806–1814. [Google Scholar] [CrossRef]
- Taylor, C.G.; Noto, A.D.; Stringer, D.M.; Froese, S.; Malcolmson, L. Dietary Milled Flaxseed and Flaxseed Oil Improve N-3 Fatty Acid Status and Do Not Affect Glycemic Control in Individuals with Well-Controlled Type 2 Diabetes. J. Am. Nutr. 2010, 29, 72–80. [Google Scholar] [CrossRef]
- Norris, L.E.; Collene, A.L.; Asp, M.L.; Hsu, J.C.; Liu, L.-F.; Richardson, J.R.; Li, D.; Bell, D.; Osei, K.; Jackson, R.D.; et al. Comparison of dietary conjugated linoleic acid with safflower oil on body composition in obese postmenopausal women with type 2 diabetes mellitus1234. Am. J. Clin. Nutr. 2009, 90, 468–476. [Google Scholar] [CrossRef]
- Barre, D.E.; Mizier-Barre, K.A.; Griscti, O.; Hafez, K. High Dose Flaxseed Oil Supplementation May Affect Fasting Blood Serum Glucose Management in Human Type 2 Diabetics. J. Oleo Sci. 2008, 57, 269–273. [Google Scholar] [CrossRef][Green Version]
- Gerhard, G.T.; Ahmann, A.; Meeuws, K.; McMurry, M.P.; Duell, P.B.; Connor, W.E. Effects of a low-fat diet compared with those of a high-monounsaturated fat diet on body weight, plasma lipids and lipoproteins, and glycemic control in type 2 diabetes. Am. J. Clin. Nutr. 2004, 80, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Brynes, A.E.; Edwards, C.M.; Jadhav, A.; Ghatei, M.A.; Bloom, S.R.; Frost, G.S. Diet-induced change in fatty acid composition of plasma triacylglycerols is not associated with change in glucagon-like peptide 1 or insulin sensitivity in people with type 2 diabetes. Am. J. Clin. Nutr. 2000, 72, 1111–1118. [Google Scholar] [CrossRef][Green Version]
- Tsihlias, E.B.; Gibbs, A.L.; McBurney, M.I.; Wolever, T.M. Comparison of high- and low-glycemic-index breakfast cereals with monounsaturated fat in the long-term dietary management of type 2 diabetes. Am. J. Clin. Nutr. 2000, 72, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, E.; Schnider, S.; Palmvig, B.; Tauber-Lassen, E.; Pedersen, O. Intake of a Diet High in Trans Monounsaturated Fatty Acids or Saturated Fatty Acids: Effects on postprandial insulinemia and glycemia in obese patients with NIDDM. Diabetes Care 1997, 20, 881–887. [Google Scholar] [CrossRef]
- Lerman-Garber, I.; Ichazo-Cerro, S.; Cardoso-Saldaña, G.; Posadas-Romero, C.; Zamora-Gonzalez, J. Effect of a High-Monounsaturated Fat Diet Enriched With Avocado in NIDDM Patients. Diabetes Care 1994, 17, 311–315. [Google Scholar] [CrossRef]
- Heine, R.J.; Mulder, C.; Popp-Snijders, C.; Van Der Meer, J.; Van Der Veen, E.A. Linoleic-acid-enriched diet: Long-term effects on serum lipoprotein and apolipoprotein concentrations and insulin sensitivity in noninsulin-dependent diabetic patients. Am. J. Clin. Nutr. 1989, 49, 448–456. [Google Scholar] [CrossRef]
- Mohan, V.; Gayathri, R.; Lakshmipriya, N.; Anjana, R.M.; Spiegelman, D.; Jeevan, R.G.; Balasubramaniam, K.K.; Jayanthan, M.; Gopinath, V.; Divya, S.; et al. Cashew Nut Consumption Increases HDL Cholesterol and Reduces Systolic Blood Pressure in Asian Indians with Type 2 Diabetes: A 12-Week Randomized Controlled Trial. J. Nutr. 2018, 148, 63–69. [Google Scholar] [CrossRef]
- Sauder, K.A.; McCrea, C.E.; Ulbrecht, J.S.; Kris-Etherton, P.M.; West, S.G.; Kris-Ethertonb, S.G.W.P.M. Effects of pistachios on the lipid/lipoprotein profile, glycemic control, inflammation, and endothelial function in type 2 diabetes: A randomized trial. Metab. Clin. Exp. 2015, 64, 1521–1529. [Google Scholar] [CrossRef]
- Parham, M.; Heidari, S.; Khorramirad, A.; Hozoori, M.; Hosseinzadeh, F.; Bakhtyari, L.; Vafaeimanesh, J. Effects of Pistachio Nut Supplementation on Blood Glucose in Patients with Type 2 Diabetes: A Randomized Crossover Trial. Diabetes Stud. 2014, 11, 190–196. [Google Scholar] [CrossRef]
- Wien, M.; Oda, K.; Sabaté, J. A randomized controlled trial to evaluate the effect of incorporating peanuts into an American Diabetes Association meal plan on the nutrient profile of the total diet and cardiometabolic parameters of adults with type 2 diabetes. Nutr. J. 2014, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Kendall, C.; Esfahani, A.; Josse, A.; Augustin, L.; Vidgen, E.; Jenkins, D. The glycemic effect of nut-enriched meals in healthy and diabetic subjects. Nutr. Metab. Cardiovasc. Dis. 2011, 21, S34–S39. [Google Scholar] [CrossRef]
- Bang, H.O.; Dyerberg, J. Plasma lipids and lipoproteins in Greenlandic west coast Eskimos. Acta Med. Scand. 1972, 192, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Wu, J.H. Omega-3 fatty acids and cardiovascular disease: Effects on risk factors, molecular pathways, and clinical events. J. Am. Coll. Cardiol. 2011, 58, 2047–2067. [Google Scholar] [CrossRef]
- Delany, J.P.; Vivian, V.M.; Snook, J.T.; Anderson, P.A. Effects of fish oil on serum lipids in men during a controlled feeding trial. Am. J. Clin. Nutr. 1990, 52, 477–485. [Google Scholar] [CrossRef]
- Saynor, R.; Verel, D.; Gillott, T. The long-term effect of dietary supplementation with fish lipid concentrate on serum lipids, bleeding time, platelets and angina. Atherosclerosis 1984, 50, 3–10. [Google Scholar] [CrossRef]
- Akinkuolie, A.O.; Ngwa, J.S.; Meigs, J.B.; Djoussé, L. Omega-3 polyunsaturated fatty acid and insulin sensitivity: A meta-analysis of randomized controlled trials. Clin. Nutr. 2011, 30, 702–707. [Google Scholar] [CrossRef]
- Vessby, B.; Aro, A.; Skarfors, E.; Berglund, L.; Salminen, I.; Lithell, H. The Risk to Develop NIDDM Is Related to the Fatty Acid Composition of the Serum Cholesterol Esters. Diabetes 1994, 43, 1353–1357. [Google Scholar] [CrossRef]
- Sacks, F.M.; Campos, H. Polyunsaturated Fatty Acids, Inflammation, and Cardiovascular Disease: Time to Widen Our View of the Mechanisms. J. Clin. Endocrinol. Metab. 2006, 91, 398–400. [Google Scholar] [CrossRef][Green Version]
- Farvid, M.S.; Ding, M.; Pan, A.; Sun, Q.; Chiuve, S.E.; Steffen, L.M.; Willett, W.C.; Hu, F.B. Dietary Linoleic Acid and Risk of Coronary Heart Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Circulation 2014, 130, 1568–1578. [Google Scholar] [CrossRef]
- Warensjö, E.; Sundström, J.; Vessby, B.; Cederholm, T.; Risérus, U. Markers of dietary fat quality and fatty acid desaturation as predictors of total and cardiovascular mortality: A population-based prospective study. Am. J. Clin. Nutr. 2008, 88, 203–209. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, Y.; Kim, Y.J.; Park, Y. Conjugated Linoleic Acid: Potential Health Benefits as a Functional Food Ingredient. Annu. Rev. Food Sci. Technol. 2016, 7, 221–244. [Google Scholar] [CrossRef]
- Brouwer, I.A.; Wanders, A.J.; Katan, M.B. Trans fatty acids and cardiovascular health: Research completed? Eur. J. Clin. Nutr. 2013, 67, 541–547. [Google Scholar] [CrossRef]
- Wu, J.H.Y.; Marklund, M.; Imamura, F.; Tintle, N.; Korat, A.V.A.; De Goede, J.; Zhou, X.; Yang, W.-S.; Otto, M.C.D.O.; Kröger, J.; et al. Omega-6 fatty acid biomarkers and incident type 2 diabetes: Pooled analysis of individual-level data for 39 740 adults from 20 prospective cohort studies. Lancet Diabetes Endocrinol. 2017, 5, 965–974. [Google Scholar] [CrossRef]
- Summers, L.K.M.; Fielding, B.A.; Bradshaw, H.A.; Ilic, V.; Beysen, C.; Clark, M.L.; Moore, N.R.; Frayn, K.N. Substituting dietary saturated fat with polyunsaturated fat changes abdominal fat distribution and improves insulin sensitivity. Diabetologia 2002, 45, 369–377. [Google Scholar] [CrossRef]
- Ros, E. Nuts and CVD. Br. J. Nutr. 2015, 113 (Suppl. 2), S111–S120. [Google Scholar] [CrossRef]
- Luo, C.; Zhang, Y.; Ding, Y.; Shan, Z.; Chen, S.; Yu, M.; Hu, F.B.; Liu, L. Nut consumption and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 256–269. [Google Scholar] [CrossRef]
- Jiang, R.; Manson, J.E.; Stampfer, M.J.; Liu, S.; Willett, W.C.; Hu, F.B. Nut and Peanut Butter Consumption and Risk of Type 2 Diabetes in Women. JAMA 2002, 288, 2554–2560. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.Á.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: Results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef]
- Jovanovski, E.; Li, D.; Ho, H.V.T.; Djedovic, V.; Marques, A.D.C.R.; Shishtar, E.; Mejia, S.B.; Sievenpiper, J.L.; De Souza, R.J.; Duvnjak, L.; et al. The effect of alpha-linolenic acid on glycemic control in individuals with type 2 diabetes: A systematic review and meta-analysis of randomized controlled clinical trials. Medicine 2017, 96, e6531. [Google Scholar] [CrossRef]
- Vessby, B.; Uusitupa, M.; Hermansen, K.; Riccardi, G.; Rivellese, A.A.; Tapsell, L.C.; Nälsén, C.; Berglund, L.; Louheranta, A.; Rasmussen, B.M.; et al. Substituting dietary saturated for monounsaturated fat impairs insulin sensitivity in healthy men and women: The KANWU study. Diabetologia 2001, 44, 312–319. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Subject Characteristics | Study Design | Intervention | Glucose | Insulin | HbA1c | Other Markers |
|---|---|---|---|---|---|---|---|
| Wang et al. 2017, European Journal of Nutrition, China | n = 99, T2D, 65 years, M/F | 6 months Parallel | (1) Corn oil (4 g/day) (2) Fish oil (4 g/day (1.34 g EPA and 1.07 g DHA)) | ↔ | ↔ | ↔ | ↔ HOMA-IR |
| Zheng et al. 2016, Mol. Nutr. Food Res, China | n = 166, T2D, 59 years, M/F | 180 days Parallel | (1) Corn oil (1 g/day) (2) Fish oil (1 g/day (500 mg EPA + DHA, EPA:DHA = 3:2)) (3) Flaxseed oil (1 g/day (630 mg ALA)) | ↔ | ↔ | (2) ↓ (3) ↔ | ↔ HOMA-IR |
| Balfegó et al. 2016, Lipids Health Dis, Spain | n = 35, T2D, 60 years, M/F | 6 months Parallel | (1) Standard diet (2) Standard diet enriched with sardines 5 days a week (100 g/day) | ↔ | ↔ Within groups: (1), (2) ↓ | ↔ Within groups: (1) ↓ | ↔ HOMA-IR Within groups: (1), (2) ↓ HOMA-IR |
| Sarbolouki et al. 2013, Singapore Med J, Iran | n = 67, T2D, 45 years, M/F | 3 months Parallel | (1) Corn oil (2 g/day) (2) EPA (2 g/day) | ↓ | ↓ | ↓ | ↓ HOMA-IR |
| Ogawa et al. 2013, Tohoku J Exp Med, Japan | n = 30, T2D, 80 years, M/F | 3 months Parallel | (1) Liquid diet without EPA/DHA (2) Liquid diet containing EPA (25 mg/100 kcal) and DHA (17 mg/100 kcal) | ↓ | ↓ | ||
| Crochemore et al. 2012, Nutr Clin Pract, Brazil | n = 41, T2D, 61 years, F | 30 days Parallel | (1) Gelatin (500 mg/capsule) (2) Fish oil (2.5 g/day (547.5 mg EPA + 352.5 mg DHA)) (3) Fish oil (1.5 g/day (328.5 mg EPA + 211.5 mg DHA)) | ↔ | ↔ | ↔ | ↔ HOMA-IR ↔ QUICKI |
| Pooya et al. 2010, Nutrition, Metabolism & Cardiovascular Disease, Iran | n = 81, T2D, Control: 53 years Treatment: 56 years M/F | 2 months Parallel | (1) Sunflower oil (2100 mg/day (12% SFA, 71% linoleic acid (LA), 16% MUFA)) (2) n-3 (3 g/day (1584 mg/day EPA, 828 mg/day DHA, 338 mg other n-3)) | ↔ | ↓ | ||
| Pedersen et al. 2003, EJCN, Denmark | n = 44, T2D, 63 years, M/F | 8 weeks Parallel | (1) Corn oil (4 g/day) (2) Fish oil (4 g/day (2.6 g EPA + DHA)) | ↔ Within groups: (2) ↑ | ↔ | ||
| Luo et al. 1998, Diabetes Care, France | n = 10, T2D, 54 years, M | 2 × 2 months Crossover | (1) Sunflower oil (6 g/day(65% n-6, 0,2% n-3, 24% MUFA, 11% SFA)) (2) Fish oil (6 g/day (1.8 g n-3: 18% EPA, 12% DHA, 4% n-6, 36% MUFA, 30% SFA)) | ↔ | ↔ | ↔ | ↔ euglycemic-hyperinsulinemic clamp |
| Dunstan et al. 1997, Diabetes Care, Australia | n = 49, NIDDM, 52–54 years, M/F | 8 weeks parallel | (1) Light exercise (2) Fish (3.6 g n-3/day) and light exercise (3) Fish (3.6 g n-3/day) and moderate exercise (4) Moderate exercise | ↔ | (2) ↓ (3) (4) ↔ | (2) ↑ (3) (4) ↔ | |
| McManus et al. 1996, Diabetes Care, Canada | n = 11, T2D, 62 years, M/F | 3 × 3 months Crossover | (1) Linseed oil (35 mg FA/kg body weight/day) (2) Fish oil (35 mg FA/kg body weight/day) | ↔ | ↔ | ↔ | ↔ Insulin sensitivity ↔ Glucose effectiveness ↔ Acute insulin response to glucose |
| Morgan et al. 1995, Diabetes Care, USA | n = 40, NIDDM, 54 years, M/F | 12 weeks Parallel | (1) Corn oil (9 g/day) (2) Corn oil (18 g/day) (3) Fish oil (9 g/day) (4) Fish oil (18 g/day) | ↔ | ↔ | ||
| Annuzzi et al. 1991, Atherosclerosis, Italy | n = 8, NIDDM, 51 years, M | 2 × 2 weeks Crossover | (1) Olive oil (10 g) (2) Fish oil (10 g (1.8 g EPA + 1.2 g DHA)) | ↔ ↔ daily average | ↔ insulin sensitivity | ↔ hyperglycemic clamp | |
| Borkman et al. 1989 Diabetes, Austrailia | n = 10, NIDDM, 57 years, M/F | 3 × 3 weeks Crossover | (1) Standard diabetic diet (2) Standard diabetic diet + Safflower oil (10 g) (3) Standard diabetic diet + Fish oil (10 g) | (2) (3) ↑ | ↔ | ↔ hyperinsulinemic-euglycemic clamp |
| Study | Subject Characteristics | Study Design | Intervention | Glucose | Insulin | HbA1c | Other Markers |
|---|---|---|---|---|---|---|---|
| Zibaeenezhad et al. 2016, Int J Endocrin Metab, Iran | n = 90, T2D, 55 years, M/F | 3 months Parallel | (1) No oil (2) Walnut oil (15 g/day) | ↓ | ↓ | ||
| Foster et al. 2013, Journal of Diabetes Research and Clinical Metabolism, Australia | n = 43, T2D, 65 years, F | 12 weeks Parallel | (1) Olive oil (2000 mg/day + 40 mg/day zinc) (2) Zink (40 mg/d) (3) Flaxseed oil (2000 mg/day (1200 mg ALA)) (4) Zinc and flaxseed oil (40 mg/day zinc + 2000 mg/day flaxseed oil) | ↔ | ↔ Within groups: (1) ↓ | ↔ | ↔ HOMA-IR Within groups: (1) ↓ HOMA-IR |
| Jenkins et al. 2014, Diabetes Care, Canada | n = 141, T2D, 59 years, M/F | 3 months Parallel | (1) whole-wheat bread without canola oil (500 kcal/day) (2) low-GL diet with a canola oil-enriched bread (500 kcal/day) | ↔ | ↓ | ||
| Taylor et al. 2010, AJCN, Canada | n = 34, T2D, 52 years, M/F | 12 weeks Parallel | (1) Bakery products with no flaxseed (2) Bakery products with milled flaxseed (32 g/day) (3) Bakery products with flaxseed oil (13 g/day) | ↔ | ↔ | ↔ | ↔ HOMA-IR ↔ QUICKI |
| Norris et al. 2009, AJCN, United States | n = 35, T2D, 60 years, F | 2 × 16 weeks crossover | (1) Safflower oil (8 g/day) (2) CLA (c9t11 and t10c12) (8 g/day) | ↑ Within groups: (1) ↓ | ↔ | ↑ HOMA-IR Within groups: (1) ↓ HOMA-IR | |
| Barre et al. 2008, J Ole Sci, Canada | n = 32, T2D, 60 years, M/F | 3 months Parallel | (1) Safflower oil 10 g/day (control) (2) Flaxseed oil 10 g/day (60 mg ALA/kg body weight/day) | ↔ | ↔ | ↔ | |
| Gerhard 2004, AJCN, United States | n = 11, T2D, 50 years, M/F | 6 weeks Parallel | (1) Low-fat diet (total fat 20 E%, carbohydrates 65 E%, higher in fiber) (2) High MUFA diet (total fat 40 E%, MUFA 26 E%, carbohydrates 45 E%) | ↔ | ↔ | ↔ Fructosamin | |
| Brynes et al. 2000, AJCN, United Kingdom | n = 9, T2D, 56 years, M/F | 2 × 3 weeks Crossover | (1) high-MUFA isoenergetic diet (olive oil) (2) high-PUFA isoenergetic diet (corn oil) | ↔ ↔ iAUC | ↔ ↔ iAUC | ↔ | ↔ short insulin tolerance test (SITT) |
| Tsihlias et al. 2000, AJCN, Canada | n = 72, T2D, 42–79 years, M/F | 6 months Parallel | (1) High-GI diet (cereals) (10% of energy) (2) Low-GI diet (cereals) (10% of energy) (3) High MUFA diet (margarine and olive oil) (10% of energy) | ↔ | (3) ↓ mean 8-h insulin (2) ↔ mean 8h insulin | ↔ | |
| Christiansen et al. 1997, Diabetes Care, Denmark | n = 16, NIDDM, 55 years, M/F | 3 × 6 weeks Crossover | (1) SAT diet (20 E% SFA, 5 E% PUFA, 5 E% MUFA) (2) Cis-MUFA diet (20 E% cis-MUFA, 5 E% PUFA, 5 E% SFA) (3) Trans-MUFA diet (20 E% trans-MUFA, 5 E% PUFA, 5 E% SFA) | ↔ ↔ AUC | ↔ (2) ↓ iAUC | ↔ | (2) ↓ C-peptide iAUC |
| Lerman-Garber et al., 1994, Diabetes Care, Mexico | n = 12, NIDDM, 56 years, F | 2 × 4 weeks Crossover | (1) Diet high in MUFA (HMUFA) (olive oil) (2) Diet high in complex carbohydrates (high-CHO) | ↔ Within groups: (1), (2) ↓ | ↔ Within groups: (1), (2) ↓ | ↔ Fructosamine | |
| Heine et al. 1989, AJCN, USA | n = 14, NIDDM, 52 years, M/F | 2 × 30 weeks Crossover | (1) Low P:S diet (P:S ratio 0.3) (2) High P:S diet (P:S ratio 1.0) | ↔ ↔ iAUC | ↔ | ↔ | ↑ Metabolic clearance rate of glucose ↔ C-peptide |
| Study | Subject Characteristics | Study Design | Intervention | Glucose | Insulin | HbA1c | Other Markers |
|---|---|---|---|---|---|---|---|
| Mohan et al. 2018, J Nutr, India | n = 269, T2D, 51 years, M/F | 12 weeks Parallel | (1) Standard diabetic diet (2) Standard diabetic diet plus cashew nuts (30 g/day) | ↔ | ↔ | ↔ | ↔ HOMA-IR |
| Sauder et al. 2015, Metabolism, USA | n = 30, T2D, 40–74 years, M/F | 2 × 4 weeks Crossover | (1) Control diet; based on the American Heart Association’s Therapeutic Lifestyle Changes diet (26.9% total fat, 6.7% saturated fat, 186 mg/day cholesterol) (2) Pistachios added to the control diet (20 % of daily energy) | ↔ | ↔ | ↔ | ↔ HOMA-IR ↔ Matsuda ↓ Fructosamine |
| Parham et al. 2014, Rev Diabet Study, Iran | n = 48, T2D, 50–53 years, M/F | 2 × 12 weeks Crossover | (1) Diet without nuts (2) Pistachio nuts (50 g/day) | ↓ | ↓ | ||
| Wien et al. 2014, Nutr Journal, USA | n = 60, T2D, 34–84 years, M/F | 24 weeks Parallel | (1) ADA meal plan without nuts (2) ADA meal plan with peanuts (20% of total energy (mean 46 g/day)) | ↔ | ↔ | ||
| Kendall et al. 2011, Nutrition, Metabolism & Cardiovascular Diseases, Canada | n = 24 T2D: 68 years Healthy: 36 years M/F | 2-h Postprandial Crossover | (1) White bread (50 g available carbohydrate) (2) Mixed nuts (30 g) (3) Mixed nuts (60 g) (4) Mixed nuts (90 g) (5) White bread + mixed nuts (30 g) (6) White bread + mixed nuts (60 g) (7) White bread + mixed nuts (90 g) | (2), (3), (4) ↓ iAUC (healthy and T2D) (6), (7) ↓ iAUC (healthy) (7) ↓ iAUC (T2D) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Telle-Hansen, V.H.; Gaundal, L.; Myhrstad, M.C.W. Polyunsaturated Fatty Acids and Glycemic Control in Type 2 Diabetes. Nutrients 2019, 11, 1067. https://doi.org/10.3390/nu11051067
Telle-Hansen VH, Gaundal L, Myhrstad MCW. Polyunsaturated Fatty Acids and Glycemic Control in Type 2 Diabetes. Nutrients. 2019; 11(5):1067. https://doi.org/10.3390/nu11051067
Chicago/Turabian StyleTelle-Hansen, Vibeke H., Line Gaundal, and Mari C.W. Myhrstad. 2019. "Polyunsaturated Fatty Acids and Glycemic Control in Type 2 Diabetes" Nutrients 11, no. 5: 1067. https://doi.org/10.3390/nu11051067
APA StyleTelle-Hansen, V. H., Gaundal, L., & Myhrstad, M. C. W. (2019). Polyunsaturated Fatty Acids and Glycemic Control in Type 2 Diabetes. Nutrients, 11(5), 1067. https://doi.org/10.3390/nu11051067