International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic


 , , ,
, , ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Study Design
3. Advances in Scientific Methodology Related to the Assessment of Physical Activity, Sleep, Dietary Behavior, and the Neighborhood, Home and School Environments
3.1. Physical Activity
3.2. Sleep
3.3. Dietary Behavior
3.4. Neighborhood, Home and School Environments
4. Epidemiological Transitions in Obesity and Related Behaviors
5. Correlates of Obesity and Lifestyle Behaviors at Multiple Levels
5.1. The Socio-Ecological Model
5.2. Obesity
5.3. Physical Activity and Sedentary Behavior
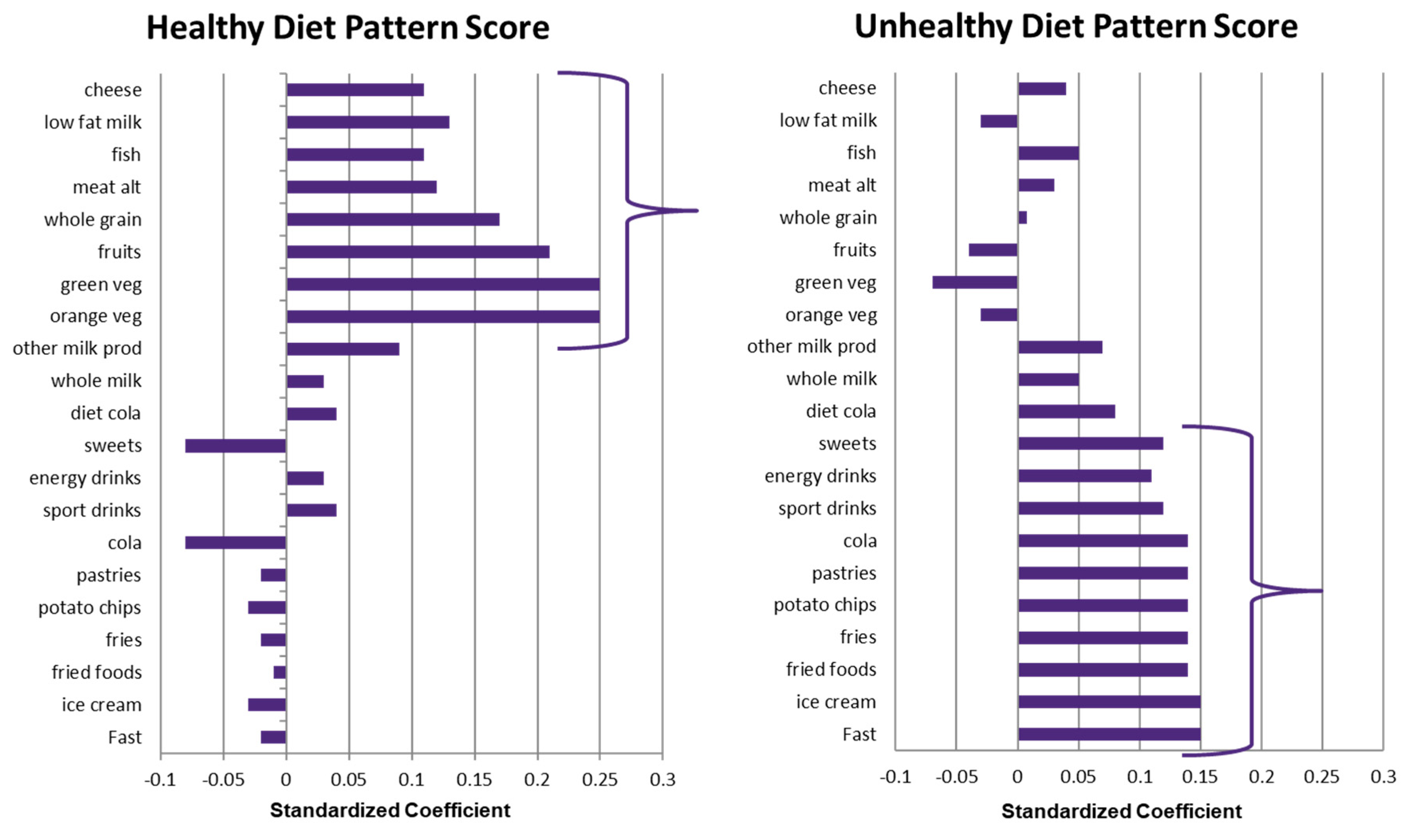
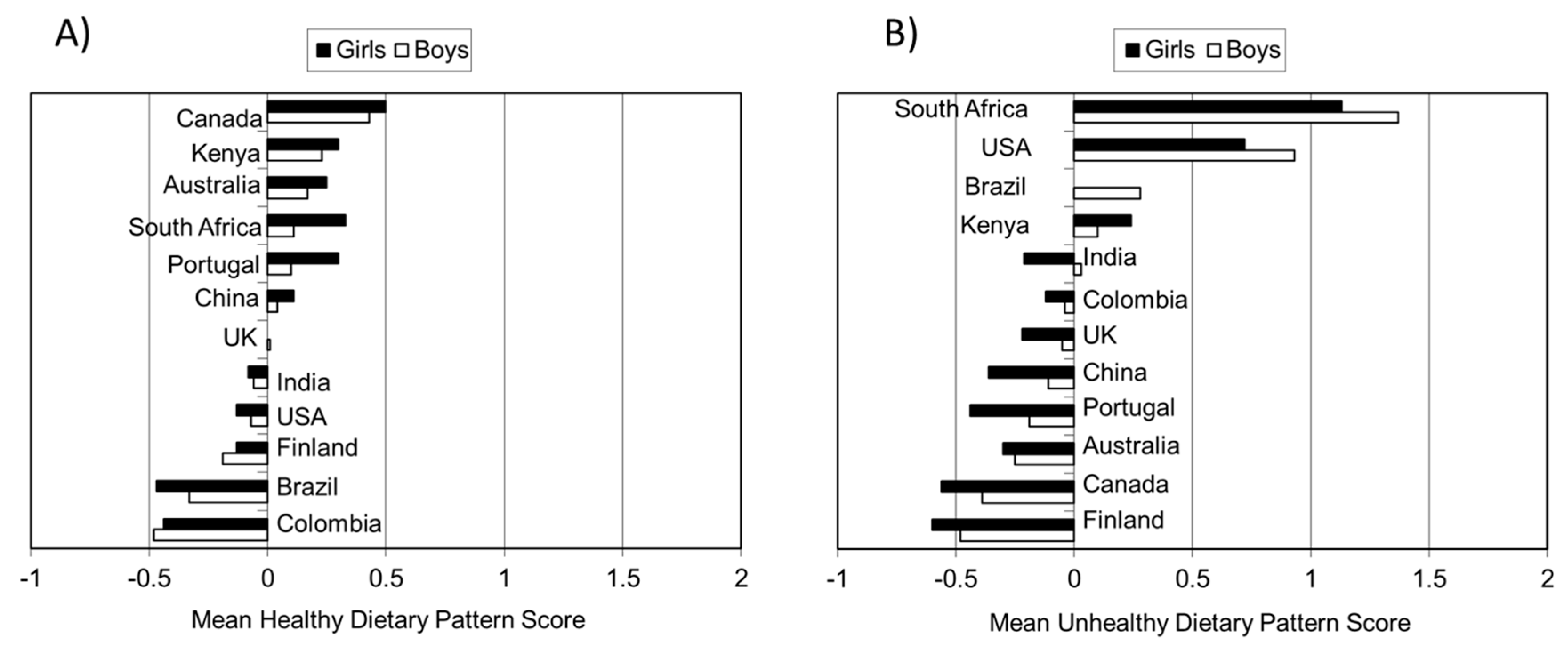
5.4. Dietary Patterns
5.5. Higher-Order Correlates
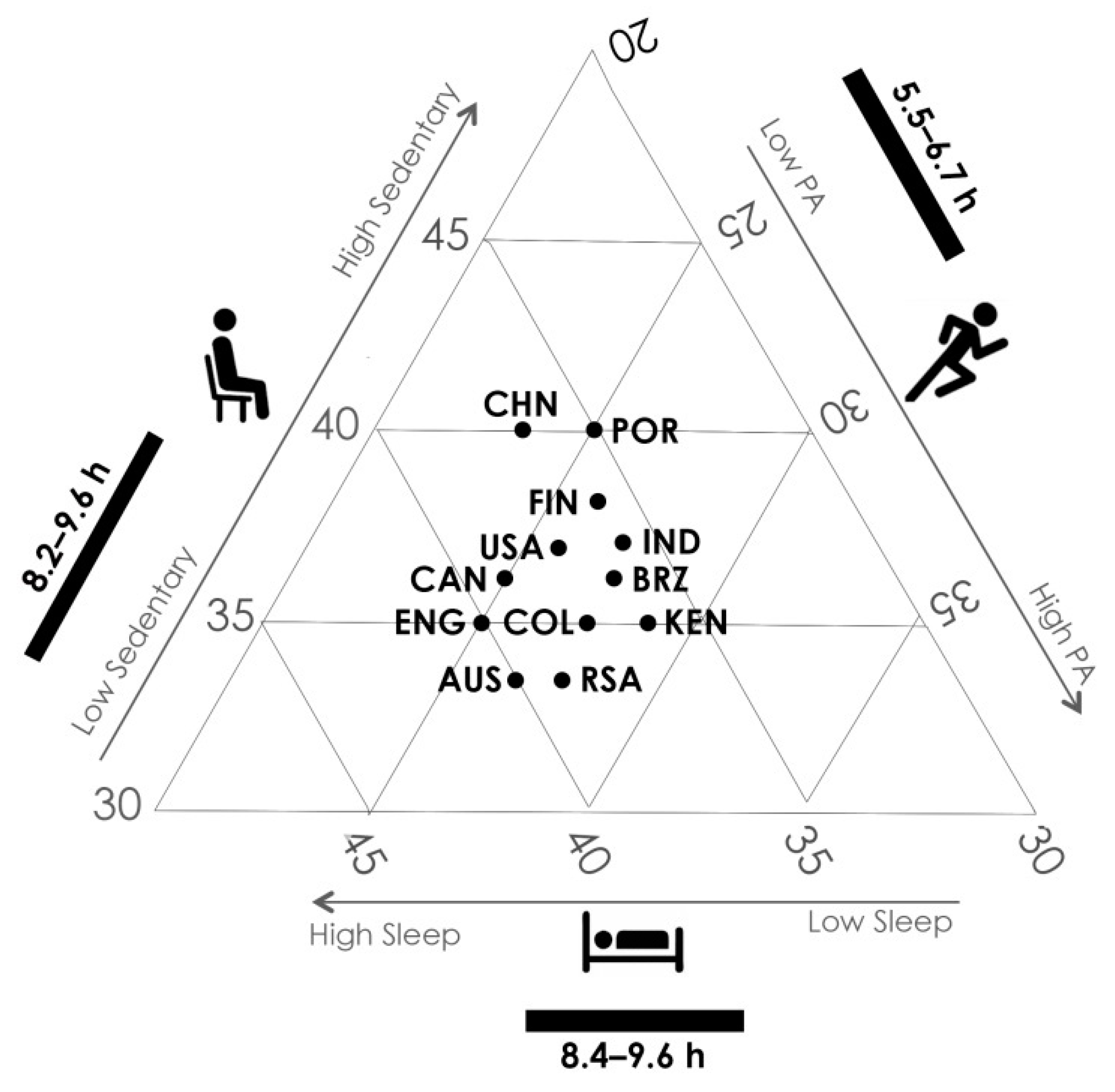
6. The 24-h Movement Behavior Cycle in Relation to Integrated Guidelines and Novel Analytical Techniques
7. Other Novel Contributions of ISCOLE
7.1. Body Composition
7.2. Identification of Physical Activity Thresholds
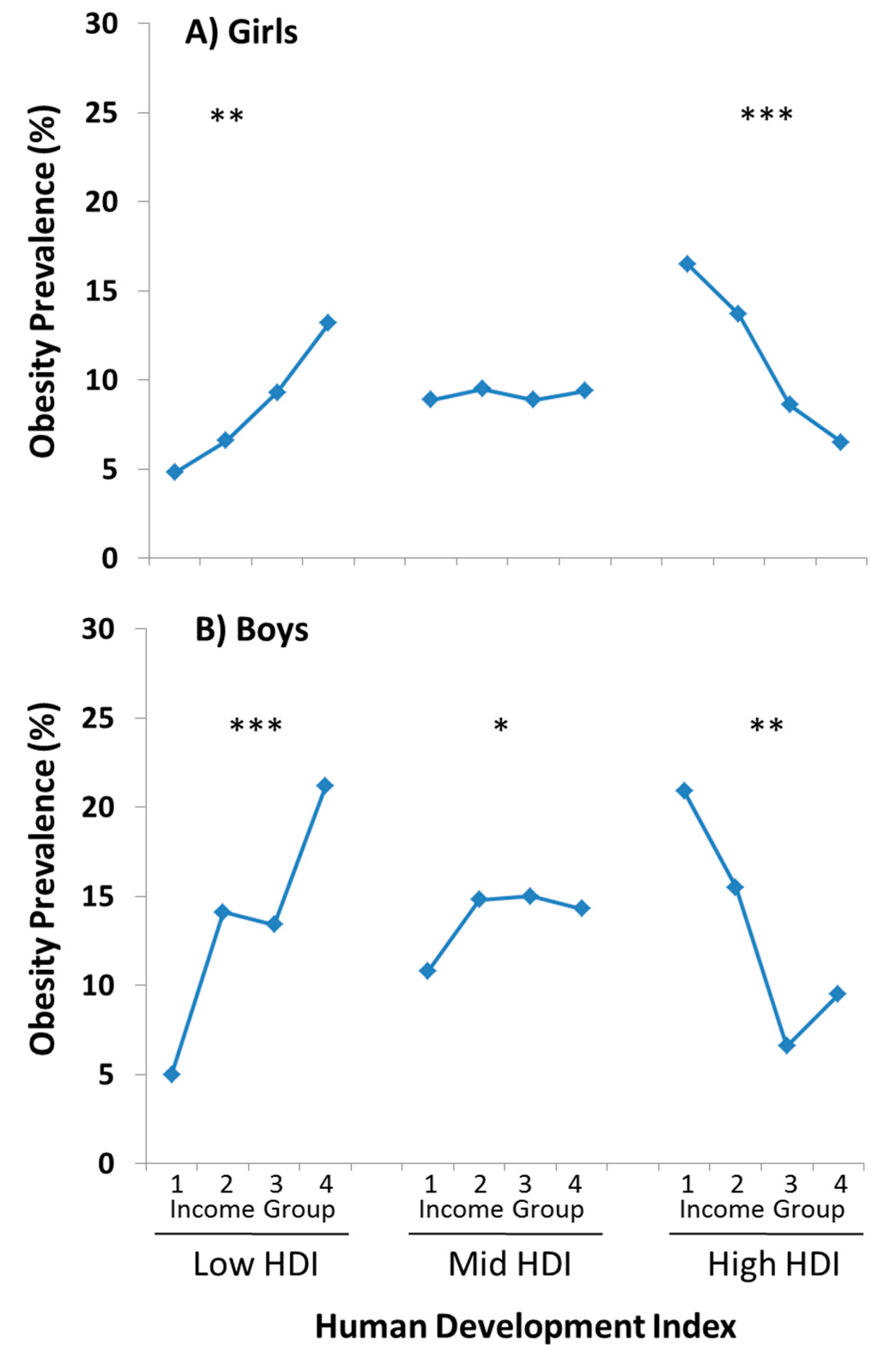
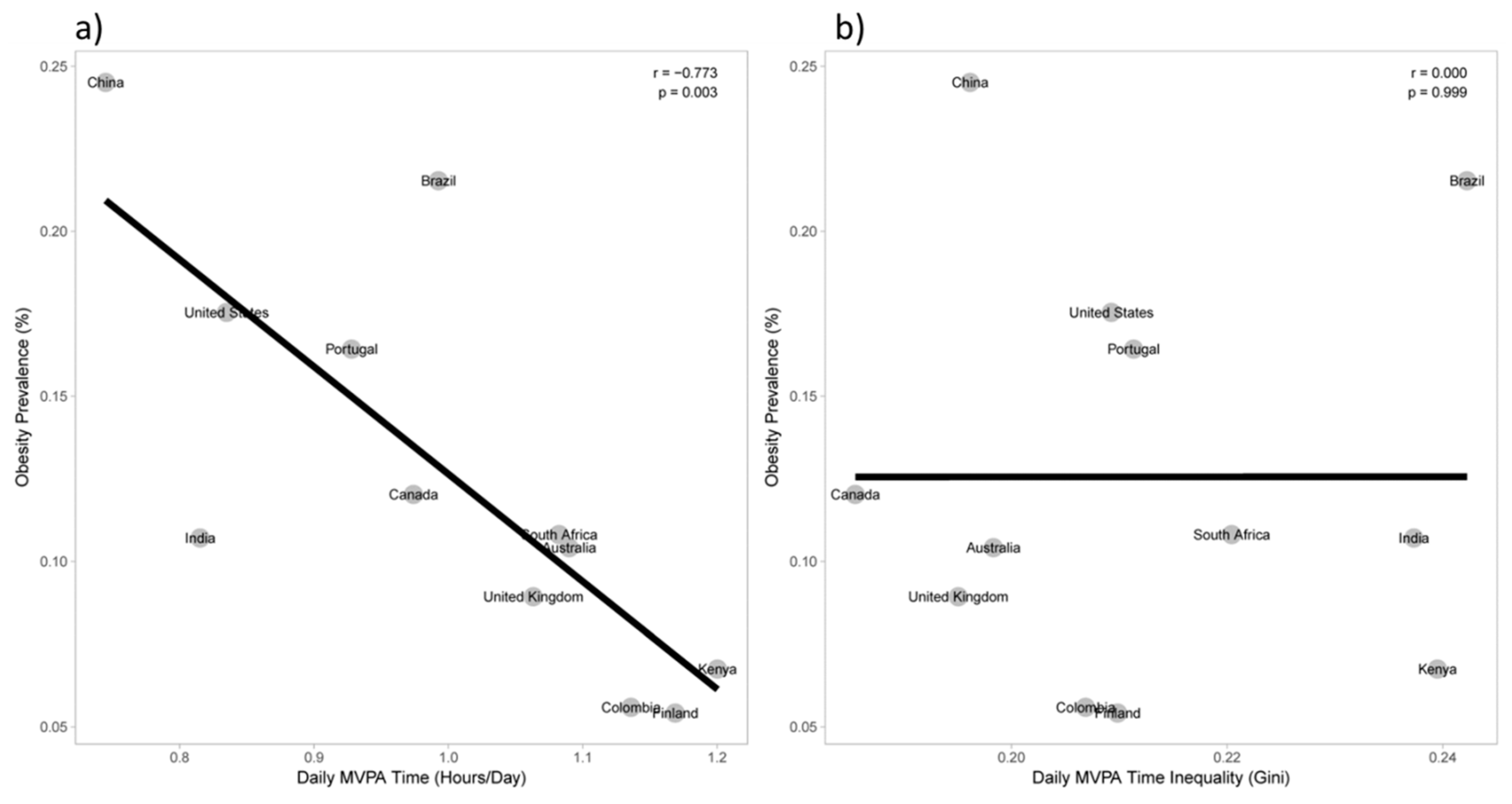
7.3. Inequality in Lifestyle and Obesity
8. Summary of Research Contributions
9. A Platform for International Training, Data Entry, and Data Quality for Multi-Country Research Studies
10. Strengths and Limitations
11. A Transparent Model for Public-Private Research Partnerships
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Riddoch, C.; Edwards, D.; Page, A.S.; Froberg, K.; Anderssen, S.A.; Wedderkopp, N.; Brage, S.; Cooper, A.R.; Sardinha, L.B.; Harro, M.; et al. The European youth heart study—Cardiovascular disease risk factors in children: Rationale, aims, study design, and validation of methods. J. Phys. Act. Health 2005, 2, 115–129. [Google Scholar] [CrossRef]
- Moreno, L.A.; De Henauw, S.; Gonzalez-Gross, M.; Kersting, M.; Molnar, D.; Gottrand, F.; Barrios, L.; Sjostrom, M.; Manios, Y.; Gilbert, C.C.; et al. Design and implementation of the healthy lifestyle in Europe by nutrition in adolescence cross-sectional study. Int. J. Obes. 2008, 32 (Suppl. 5), S4–S11. [Google Scholar] [CrossRef]
- Ahrens, W.; Bammann, K.; Siani, A.; Buchecker, K.; De Henauw, S.; Iacoviello, L.; Hebestreit, A.; Krogh, V.; Lissner, L.; Marild, S.; et al. The IDEFICS cohort: Design, characteristics and participation in the baseline survey. Int. J. Obes. 2011, 35 (Suppl. 1), S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Van Stralen, M.M.; te Velde, S.J.; Singh, A.S.; De Bourdeaudhuij, I.; Martens, M.K.; van der Sluis, M.; Manios, Y.; Grammatikaki, E.; Chinapaw, M.J.; Maes, L.; et al. EuropeaN energy balance research to prevent excessive weight gain among youth (ENERGY) project: Design and methodology of the energy cross-sectional survey. BMC Public Health 2011, 11, 65. [Google Scholar] [CrossRef]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereeken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. The International study of childhood obesity, Lifestyle and the environment (ISCOLE): Design and methods. BMC Public Health 2013, 13, 900. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Relationship between lifestyle behaviors and obesity in children ages 9–11: Results from a 12-country study. Obesity 2015, 23, 1696–1702. [Google Scholar] [CrossRef]
- LeBlanc, A.G.; Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Chaput, J.P.; Church, T.S.; Fogelholm, M.; Harrington, D.M.; Hu, G.; Kuriyan, R.; et al. Are participant characteristics from ISCOLE study sites comparable to the rest of their country? Int. J. Obes. Suppl. 2015, 5, S9–S16. [Google Scholar] [CrossRef]
- United Nations Development Programme. Sustainability and Equity: A Better Future for All; Human Development Report 2011; Palgrave Macmillan: New York, NY, USA, 2011. [Google Scholar]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M.; Katzmarzyk, P.T. Unique contributions of ISCOLE to the advancement of accelerometry in large studies. Int. J. Obes. Suppl. 2015, 5, S53–S58. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Mire, E.F.; Dentro, K.N.; Barreira, T.V.; Schuna, J.M., Jr.; Zhao, P.; Tremblay, M.S.; Standage, M.; Sarmiento, O.L.; Onywera, V.; et al. A model for presenting accelerometer paradata in large studies: ISCOLE. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 52. [Google Scholar] [CrossRef]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Improving wear time compliance with a 24 h waist-worn accelerometer protocol in the international study of childhood obesity, lifestyle and the environment (ISCOLE). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 172. [Google Scholar] [CrossRef]
- Barreira, T.V.; Schuna, J.M.; Tudor-Locke, C.; Chaput, J.-P.; Church, T.S.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Reliability of accelerometer-determined physical activity and sedentary behavior in school-aged children: A 12 country study. Int. J. Obes. Suppl. 2015, 5, S29–S35. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep-period time separate from 24 h physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 2014, 39, 53–57. [Google Scholar] [CrossRef]
- Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T.; Chaput, J.P.; Leduc, G.; Tudor-Locke, C. Identifying children’s nocturnal sleep using 24 h waist accelerometry. Med. Sci. Sports Exerc. 2015, 47, 937–943. [Google Scholar] [CrossRef]
- Sadeh, A.; Sharkey, K.M.; Carskadon, M.A. Activity-based sleep-wake identification: An empical test of methodological issues. Sleep 1994, 17, 201–207. [Google Scholar] [CrossRef]
- SAS Programs for Analyzing NHANES 2003-2004 Accelerometer Data. Available online: http://riskfactor.cancer.gov/tools/nhanes_pam/ (accessed on 15 April 2019).
- Fully Automated Waist-worn Accelerometer Algorithm for Children’s Sleep Period Time Separate From 24-h Physical Activity or Sedentary Behaviors. Available online: www.pbrc.edu/SleepPeriodTimeMacro (accessed on 15 April 2019).
- Identifying Children’s Nocturnal Sleep Using 24-h Waist Accelerometry. Available online: http://www.pbrc.edu/pdf/PBRCSleepEpisodeTimeMacroCode.pdf (accessed on 15 April 2019).
- Tudor-Locke, C.; Mire, E.F.; Barreira, T.V.; Schuna, J.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kurpad, A.; Kuriyan, R.; Lambert, E.V.; et al. Nocturnal sleep-related variables from 24 h free-living waist-worn accelerometry: International Study of Childhood Obesity, Lifestyle and the Environment. Int. J. Obes. Suppl. 2015, 5, S47–S52. [Google Scholar] [CrossRef]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. Social Determinants of Health and Well-Being among Young People; Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; Health Policy for Children and Adolescents WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Saloheimo, T.; Gonzalez, S.A.; Erkkola, M.; Milauskas, D.M.; Meisel, J.D.; Champagne, C.M.; Tudor-Locke, C.; Sarmiento, O.; Katzmarzyk, P.T.; Fogelholm, M. The reliability and validity of a short food frequency questionnaire among 9–11 year olds: A multinational study on three middle-income and high-income countries. Int. J. Obes. Suppl. 2015, 5, S22–S28. [Google Scholar] [CrossRef]
- Mikkila, V.; Vepsalainen, H.; Saloheimo, T.; Gonzalez, S.A.; Meisel, J.D.; Hu, G.; Champagne, C.M.; Chaput, J.P.; Church, T.S.; Katzmarzyk, P.T.; et al. An international comparison of dietary patterns in 9–11 year old children. Int. J. Obes. Suppl. 2015, 5, S17–S21. [Google Scholar] [CrossRef]
- Saelens, B.E.; Sallis, J.F.; Frank, L.D.; Couch, S.C.; Zhou, C.; Colburn, T.; Cain, K.L.; Chapman, J.; Glanz, K. Obesogenic neighborhood environments, child and parent obesity: The neighborhood impact on kids study. Am. J. Prev. Med. 2012, 42, e57–e64. [Google Scholar] [CrossRef] [PubMed]
- Broyles, S.T.; Drazba, K.T.; Church, T.S.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Development and reliability of an audit tool to assess the school physical activity environment across 12 countries. Int. J. Obes. Suppl. 2015, 5, S36–S42. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Omran, A.R. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem. Fund Q. 1971, 49, 509–538. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Nutritional patterns and transitions. Pop. Dev. Rev. 1993, 19, 138–157. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Mason, C. The physical activity transition. J. Phys. Act. Health 2009, 6, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Shrewsbury, V.; Wardle, J. Socioeconomic status and adiposity in childhood: A systematic review of cross-sectional studies 1990–2005. Obesity 2008, 16, 275–284. [Google Scholar] [CrossRef]
- Broyles, S.T.; Denstel, K.D.; Church, T.S.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. The epidemiological transition and the global childhood obesity epidemic. Int. J. Obes. Suppl. 2015, 5, S3–S8. [Google Scholar] [CrossRef]
- Manyanga, T.; Barnes, J.D.; Tremblay, M.S.; Katzmarzyk, P.T.; Broyles, S.T.; Barreira, T.V.; Fogelholm, M.; Hu, G.; Maher, C.; Maia, J.; et al. No evidence for an epidemiological transition in sleep patterns among children: A 12-country study. Sleep Health 2018, 4, 87–95. [Google Scholar] [CrossRef]
- Manyanga, T.; Tremblay, M.S.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Socioeconomic status and dietary patterns in children from around the world: Different associations by levels of country human development? BMC Public Health 2017, 17, 457. [Google Scholar] [CrossRef]
- Barreira, T.V.; Broyles, S.T.; Tudor-Locke, C.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Epidemiological transition in physical activity and sedentary time in children. J. Phys. Act. Health 2019, in press. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: Policy and environmental approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef]
- Goldstein, H. Multilevel Statistical Models, 3rd ed.; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Corgeau, D. Methodology and Epistemology of Multilevel Analysis: Approaches from Different Social Sciences; Kluwer Academic Publishers: Dordrecht, The Netherlands, 2003. [Google Scholar]
- Katzmarzyk, P.T.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; et al. Sources of variability in childhood obesity indicators and related behaviors. Int. J. Obes. 2018, 42, 108–110. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Physical activity, sedentary time and obesity in an international sample of children. Med. Sci. Sports Exerc. 2015, 47, 2062–2069. [Google Scholar] [CrossRef]
- Sarmiento, O.L.; Lemoine, P.; Gonzalez, S.A.; Broyles, S.T.; Denstel, K.D.; Larouche, R.; Onywera, V.; Barreira, T.V.; Chaput, J.-P.; Fogelholm, M.; et al. Relationships between active school transport and adiposity indicators in school age children from low-, middle-and high-income countries. Int. J. Obes. Suppl. 2015, 5, S107–S114. [Google Scholar] [CrossRef]
- Zakrzewski, J.K.; Gillison, F.B.; Cumming, S.; Church, T.S.; Katzmarzyk, P.T.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Denstel, K.D.; Fogelholm, M.; et al. Associations between breakfast frequency and adiposity indicators in children from 12 countries. Int. J. Obes. Suppl. 2015, 5, S80–S88. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maia, J.; et al. Relationship between soft drink consumption and obesity in 9–11 year old children in a multi-national study. Nutrients 2016, 8, 770. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Liu, E.; Qiao, Y.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Maternal gestational diabetes and childhood obesity at age 9–11: Results of a multinational study. Diabetologia 2016, 59, 2339–2348. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Ma, J.; Wang, Y.; Li, W.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Birth weight and childhood obesity: A 12-country study. Int. J. Obes. Suppl. 2015, 5, S74–S79. [Google Scholar] [CrossRef]
- Qiao, Y.; Zhang, T.; Liu, H.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Joint association of birth weight and physical activity/sedentary behavior with obesity in children ages 9–11 years from 12 countries. Obesity 2017, 25, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, S.K.; Onywera, V.O.; Tremblay, M.S.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Relationships between parental education and overweight with childhood overweight and physical activity in 9–11 year old children: Results from a 12-country study. PLoS ONE 2016, 11, e0147746. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Gomes, T.N.; Katzmarzyk, P.T.; Hedeker, D.; Fogelholm, M.; Standage, M.; Onywera, V.; Lambert, E.V.; Tremblay, M.S.; Chaput, J.P.; Tudor-Locke, C.; et al. Correlates of compliance with recommended levels of physical activity in children. Sci. Rep. 2017, 7, 16507. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Maher, C.; Olds, T.; Onywera, V.; Sarmiento, O.L.; Standage, M.; et al. Physical education classes, physical activity, and sedentary behavior in children. Med. Sci. Sports Exerc. 2018, 50, 995–1004. [Google Scholar] [CrossRef]
- Denstel, K.D.; Broyles, S.T.; Larouche, R.; Sarmiento, O.L.; Barreira, T.V.; Chaput, J.-P.; Church, T.S.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. Active school transport and weekday physical activity in 9–11 year old children from 12 countries. Int. J. Obes. Suppl. 2015, 5, S100–S106. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Sarmiento, O.L.; Broyles, S.T.; Denstel, K.D.; Church, T.S.; Barreira, T.V.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. Are the correlates of active school transport context-specific? Int. J. Obes. Suppl. 2015, 5, S89–S99. [Google Scholar] [CrossRef]
- Harrington, D.M.; Gillison, F.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; LeBlanc, A.G.; Maher, C.; et al. Household-level correlates of children’s physical activity levels in and across 12 countries. Obesity 2016, 24, 2150–2157. [Google Scholar] [CrossRef]
- Sullivan, S.M.; Broyles, S.T.; Barreira, T.V.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Associations of neighborhood social environment attributes and physical activity among 9-11 year old children from 12 countries. Health Place 2017, 46, 183–191. [Google Scholar] [CrossRef]
- LeBlanc, A.G.; Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Chaput, J.P.; Church, T.S.; Fogelholm, M.; Harrington, D.M.; Hu, G.; Kuriyan, R.; et al. Correlates of total sedentary time and screen time in 9-11 year-old children around the world: The international study of childhood obesity, lifestyle and the environment. PLoS ONE 2015, 10, e0129622. [Google Scholar] [CrossRef]
- Chaput, J.P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of all movement behaviors in a 24 hour period for overall health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef]
- Chaput, J.P.; Katzmarzyk, P.T.; LeBlanc, A.G.; Tremblay, M.S.; Barreira, T.V.; Broyles, S.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; et al. Associations between sleep patterns and lifestyle behaviors in children: An international comparison. Int. J. Obes. Suppl. 2015, 5, S59–S65. [Google Scholar] [CrossRef]
- Lin, Y.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Sarmiento, O.L.; et al. Temporal and bi-directional associations between sleep duration and physical activity/sedentary time in children: An international comparison. Prev. Med. 2018, 111, 436–441. [Google Scholar] [CrossRef]
- Vepsalainen, H.; Mikkila, V.; Erkkola, M.; Broyles, S.T.; Chaput, J.P.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Association between home and school food environments and dietary patterns among 9–11-year-old children in 12 countries. Int. J. Obes. Suppl. 2015, 5, S66–S73. [Google Scholar] [CrossRef]
- Chaput, J.P.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; Sarmiento, O.L.; et al. Sleep patterns and sugar-sweetened beverage consumption among children from around the world. Public Health Nutr. 2018, 21, 2385–2393. [Google Scholar] [CrossRef]
- Chaput, J.P.; Weippert, M.; LeBlanc, A.G.; Hjorth, M.F.; Michaelsen, K.F.; Katzmarzyk, P.T.; Tremblay, M.S.; Barreira, T.V.; Broyles, S.T.; Fogelholm, M.; et al. Are children like werewolves? Full moon and its association with sleep and activity behaviors in an international sample of children. Front. Pediatr. 2016, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Lewis, L.K.; Maher, C.; Belanger, K.; Tremblay, M.; Chaput, J.P.; Olds, T. At the mercy of the gods: Associations between weather, physical activity, and sedentary time in children. Pediatr. Exerc. Sci. 2016, 28, 152–163. [Google Scholar] [CrossRef]
- Chaput, J.P.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Mikkila, V.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; et al. Outdoor time and dietary patterns in children around the world. J. Public Health (Oxf) 2018, 40, e493–e501. [Google Scholar] [CrossRef]
- Larouche, R.; Mire, E.F.; Belanger, K.; Barreira, T.V.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; et al. Relationships between outdoor time, physical activity, sedentary time, and body mass index in children: A 12-country study. Pediatr. Exerc. Sci. 2018, 31, 118–129. [Google Scholar] [CrossRef]
- Triana Reyes, C.A.; Bravo-Balado, A.; Gonzalez, S.A.; Bolivar, M.A.; Lemoine, P.; Meisel, J.D.; Grijalba, C. Active streets for children: The case of the ciclovia of Bogota. PLoS ONE 2019, in press. [Google Scholar]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24 h movement Guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Maher, C.; Lewis, L.K.; Stanford, T.E.; Martin Fernandez, J.A.; Ratcliffe, J.; Katzmarzyk, P.T.; Barreira, T.V.; Chaput, J.P.; Fogelholm, M.; et al. Human development index, children’s health-related quality of life and movement behaviors: A compositional data analysis. Qual. Life Res. 2018, 27, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Roman-Vinas, B.; Chaput, J.P.; Katzmarzyk, P.T.; Fogelholm, M.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; Sarmiento, O.L.; et al. Proportion of children meeting recommendations for 24 h movement guidelines and associations with adiposity in a 12-country study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 123. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H.; Standage, M.; Tremblay, M.S.; Katzmarzyk, P.T.; Hu, G.; Kuriyan, R.; Maher, C.; Maia, J.; Olds, T.; Sarmiento, O.L.; et al. Associations between meeting combinations of 24 h movement guidelines and health-related quality of life in children from 12-countries. Public Health 2017, 153, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Thivel, D.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Maher, C.; Maia, J.; Olds, T.; Sarmiento, O.L.; Standage, M.; et al. Associations between meeting combinations of 24-hour movement recommendations and dietary patterns of children: A 12-country study. Prev. Med. 2018, 118, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Stanford, T.E.; Pedisic, Z.; Maher, C.; Lewis, L.K.; Martin-Fernandez, J.A.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Standage, M.; et al. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z. Measurement issues and poor adjustments for physical activity and sleep undermine sedentary behaviour research—The focus should shift to the balance between sleep, sedentary behaviour, standing and activity. Kinesiology 2014, 46, 135–146. [Google Scholar]
- Dumuid, D.; Stanford, T.E.; Martin-Fernandez, J.A.; Pedisic, Z.; Maher, C.A.; Lewis, L.K.; Hron, K.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; et al. Compositional data analysis for physical activity, sedentary time and sleep research. Stat. Methods Med. Res. 2017, 27. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Olds, T.; Lewis, L.K.; Martin-Fernandez, J.A.; Barreira, T.; Broyles, S.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; et al. The adiposity of children is associated with their lifestyle behaviours: A cluster analysis of school-aged children from 12 nations. Pediat.r Obes. 2018, 13, 111–119. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; et al. Association between body mass index and body fat in 9–11-year-old children from countries spanning a range of human development. Int. J. Obes. Suppl. 2015, 5, S43–S46. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chaput, J.-P.; Katzmarzyk, P.T.; Barnes, J.D.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; Maher, C.; Maia, J.; et al. Mid-upper arm circumference as a screening tool for identifying children with obesity: A 12-country study. Pediatric. Obes. 2017, 12, 439–445. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Barnes, J.D.; Tremblay, M.S.; Fogelholm, M.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; et al. Thresholds of physical activity associated with obesity by level of sedentary behaviour in children. Pediatr. Obes. 2018, 13, 450–457. [Google Scholar] [CrossRef]
- Althoff, T.; Sosic, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef]
- Chaput, J.P.; Barnes, J.D.; Tremblay, M.S.; Fogelholm, M.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; Onywera, V.; et al. Inequality in physical activity, sedentary behaviour, sleep duration and risk of obesity in children: A 12-country study. Obes. Sci. Pract. 2018, 4, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Stuckler, D.; Ruskin, G.; McKee, M. Complexity and conflicts of interest statements: A case-study of emails exchanged between Coca-Cola and the principal investigators of the International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE). J. Public Health Pol. 2018, 39, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Church, T.S. Letter to the editors. J. Public Health Pol. 2018, 39, 254–257. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Site | HDI * | Boys (n) | Girls (n) | Age (year) ** | NW (%) | OV (%) | OB (%) | Parent Education (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||||||
| China (Tianjin) | 0.687 | 293 | 259 | 9.9 (0.4) | 58.9 | 17.4 | 23.7 | 33.0 | 44.4 | 22.6 |
| Brazil (Sao Paulo) | 0.718 | 287 | 297 | 10.5 (0.5) | 56.3 | 22.8 | 20.9 | 24.3 | 52.8 | 22.9 |
| United States (Baton Rouge) | 0.910 | 281 | 370 | 10.0 (0.6) | 58.8 | 22.4 | 18.7 | 8.9 | 44.6 | 46.6 |
| Portugal (Porto) | 0.809 | 358 | 419 | 10.4 (0.3) | 52.8 | 29.7 | 17.5 | 46.7 | 32.8 | 20.5 |
| Canada (Ottawa) | 0.908 | 239 | 328 | 10.5 (0.4) | 69.3 | 18.9 | 11.8 | 2.0 | 27.7 | 70.4 |
| South Africa (Cape Town) | 0.619 | 223 | 327 | 10.3 (0.7) | 73.6 | 15.6 | 10.7 | 48.0 | 39.0 | 12.9 |
| Australia (Adelaide) | 0.929 | 243 | 285 | 10.7 (0.4) | 62.1 | 27.5 | 10.4 | 11.4 | 47.7 | 40.9 |
| India (Bangalore) | 0.547 | 292 | 328 | 10.4 (0.5) | 66.3 | 23.4 | 10.3 | 4.8 | 21.7 | 73.4 |
| United Kingdom (Bath) | 0.863 | 237 | 288 | 10.9 (0.5) | 69.7 | 20.6 | 9.7 | 3.0 | 51.6 | 45.4 |
| Kenya (Nairobi) | 0.509 | 262 | 301 | 10.2 (0.7) | 78.9 | 14.6 | 6.6 | 13.9 | 45.7 | 40.4 |
| Colombia (Bogota) | 0.710 | 454 | 465 | 10.5 (0.6) | 77.2 | 17.1 | 5.8 | 31.8 | 50.7 | 17.5 |
| Finland (Helsinki) | 0.882 | 253 | 283 | 10.5 (0.4) | 76.3 | 18.3 | 5.4 | 2.8 | 55.1 | 42.1 |
| Research Area | Major Contribution |
|---|---|
| Global Patterns of Obesity and Related Behaviors |
|
| Correlates of Obesity |
|
| Correlates of Physical Activity & Sedentary Behavior |
|
| Correlates of Dietary Intake |
|
| Methodological Advances |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Maher, C.; Maia, J.; Olds, T.; Sarmiento, O.L.; Standage, M.; Tremblay, M.S.; et al. International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic. Nutrients 2019, 11, 848. https://doi.org/10.3390/nu11040848
Katzmarzyk PT, Chaput J-P, Fogelholm M, Hu G, Maher C, Maia J, Olds T, Sarmiento OL, Standage M, Tremblay MS, et al. International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic. Nutrients. 2019; 11(4):848. https://doi.org/10.3390/nu11040848
Chicago/Turabian StyleKatzmarzyk, Peter T., Jean-Philippe Chaput, Mikael Fogelholm, Gang Hu, Carol Maher, Jose Maia, Timothy Olds, Olga L. Sarmiento, Martyn Standage, Mark S. Tremblay, and et al. 2019. "International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic" Nutrients 11, no. 4: 848. https://doi.org/10.3390/nu11040848
APA StyleKatzmarzyk, P. T., Chaput, J.-P., Fogelholm, M., Hu, G., Maher, C., Maia, J., Olds, T., Sarmiento, O. L., Standage, M., Tremblay, M. S., & Tudor-Locke, C. (2019). International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic. Nutrients, 11(4), 848. https://doi.org/10.3390/nu11040848