Association between Sleep Disturbances and Liver Status in Obese Subjects with Nonalcoholic Fatty Liver Disease: A Comparison with Healthy Controls


 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Anthropometric and Biochemical Measurements
2.3. Liver Stiffness Assessment
2.4. Sleep Quality Assessment
2.5. Dietary Assessment
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
3.2. Association between Sleep Characteristics and Risk of NAFLD
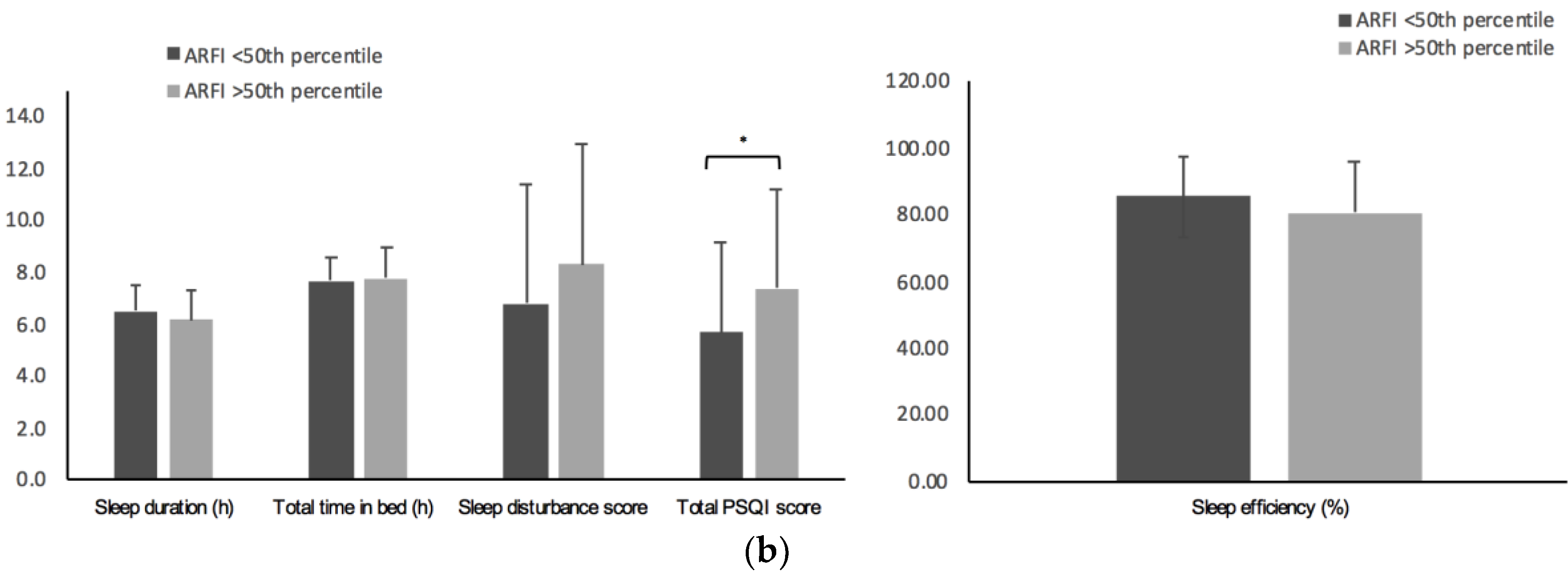
3.3. Association between Sleep Characteristics and Liver Stiffness Assessed by ARFI
3.4. Correlation of Sleep Characteristics and Variables Related to Hepatic Status (S1)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ji, X.; Wang, Q.; Li, J.Z. New insight into inter-organ crosstalk contributing to the pathogenesis of non-alcoholic fatty liver disease (NAFLD). Protein Cell 2018, 9, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Cantero, I.; Abete, I.; Monreal, J.I.; Martinez, J.A.; Zulet, M.A. Fruit fiber consumption specifically improves liver health status in obese subjects under energy restriction. Nutrients 2017, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Bullón-Vela, M.V.; Abete, I.; Martinez, J.A.; Zulet, M.A. Obesity and Nonalcoholic Fatty Liver Disease: Role of Oxidative Stress. In Obesity: Oxidative Stress and Dietary Antioxidants; Marti del Moral, A., García, C.M.A., Eds.; Elsevier: London, UK, 2018; pp. 111–133. ISBN 9780128125052 0128125055. [Google Scholar]
- Leung, C.; Rivera, L.; Furness, J.B.; Angus, P.W. The role of the gut microbiota in NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Targher, G.; Bernardi, M.; Bonino, F.; Bugianesi, E.; Casini, A.; Gastaldelli, A.; Marchesini, G.; Marra, F.; et al. AISF position paper on nonalcoholic fatty liver disease (NAFLD): Updates and future directions. Dig. Liver Dis. 2017, 49, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef]
- Cassinotto, C.; Boursier, J.; de Lédinghen, V.; Lebigot, J.; Lapuyade, B.; Cales, P.; Hiriart, J.B.; Michalak, S.; Le Bail, B.; Cartier, V.; et al. Liver stiffness in nonalcoholic fatty liver disease: A comparison of supersonic shear imaging, FibroScan, and ARFI with liver biopsy. Hepatology 2016, 63, 1817–1827. [Google Scholar] [CrossRef]
- Nascimbeni, F.; Ballestri, S.; Machado, M.V.; Mantovani, A.; Cortez-Pinto, H.; Targher, G.; Lonardo, A. Clinical relevance of liver histopathology and different histological classifications of NASH in adults. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 351–367. [Google Scholar] [CrossRef]
- Itani, O.; Jike, M.; Watanabe, N.; Kaneita, Y. Short sleep duration and health outcomes: A systematic review. Sleep Med. 2017, 32, 246–256. [Google Scholar] [CrossRef]
- Tan, X.; Chapman, C.D.; Cedernaes, J.; Benedict, C. Association between long sleep duration and increased risk of obesity and type 2 diabetes: A review of possible mechanisms. Sleep Med. Rev. 2018, 40, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Cho, K.-H. Total sleep duration and risk of type 2 diabetes: Evidence based on clinical and epidemiological studies. Curr. Drug Metab. 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Altman, N.G.; Izci-Balserak, B.; Schopfer, E.; Jackson, N.; Rattanaumpawan, P.; Gehrman, P.R.; Patel, N.P.; Grandner, M.A. Sleep duration versus sleep insufficiency as predictors of cardiometabolic health outcomes. Sleep Med. 2012, 13, 1261–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imaizumi, H.; Takahashi, A.; Tanji, N.; Abe, K.; Sato, Y.; Anzai, Y.; Watanabe, H.; Ohira, H. The Association between Sleep Duration and Non-Alcoholic Fatty Liver Disease among Japanese Men and Women. Obes. Facts 2015, 8, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Bernsmeier, C.; Weisskopf, D.M.; Pflueger, M.O.; Mosimann, J.; Campana, B.; Terracciano, L.; Beglinger, C.; Heim, M.H.; Cajochen, C. Sleep disruption and daytime sleepiness correlating with disease severity and insulin resistance in non-alcoholic fatty liver disease: A comparison with healthy controls. PLoS ONE 2015, 10, e0143293. [Google Scholar] [CrossRef] [PubMed]
- Poroyko, V.A.; Carreras, A.; Khalyfa, A.; Khalyfa, A.A.; Leone, V.; Peris, E.; Almendros, I.; Gileles-Hillel, A.; Qiao, Z.; Hubert, N.; et al. Chronic Sleep Disruption Alters Gut Microbiota, Induces Systemic and Adipose Tissue Inflammation and Insulin Resistance in Mice. Sci. Rep. 2016, 6, 35405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashti, H.S.; Scheer, F.A.; Jacques, P.F.; Lamon-Fava, S.; Ordovas, J.M. Short Sleep Duration and Dietary Intake: Epidemiologic Evidence, Mechanisms, and Health Implications. Adv. Nutr. Int. Rev. J. 2015, 6, 648–659. [Google Scholar] [CrossRef] [Green Version]
- Benedict, C.; Vogel, H.; Jonas, W.; Woting, A.; Blaut, M.; Schürmann, A.; Cedernaes, J. Gut microbiota and glucometabolic alterations in response to recurrent partial sleep deprivation in normal-weight young individuals. Mol. Metab. 2016, 5, 1175–1186. [Google Scholar] [CrossRef]
- Liu, C.; Zhong, R.; Lou, J.; Pan, A.; Tang, Y.; Chang, J.; Ke, J.; Li, J.; Yuan, J.; Wang, Y.; et al. Nighttime sleep duration and risk of nonalcoholic fatty liver disease: The Dongfeng-Tongji prospective study. Ann. Med. 2016, 48, 468–476. [Google Scholar] [CrossRef]
- Kim, C.-W.; Yun, K.E.; Jung, H.-S.; Chang, Y.; Choi, E.-S.; Kwon, M.-J.; Lee, E.-H.; Woo, E.J.; Kim, N.H.; Shin, H.; et al. Sleep duration and quality in relation to non-alcoholic fatty liver disease in middle-aged workers and their spouses. J. Hepatol. 2013, 59, 351–357. [Google Scholar] [CrossRef]
- Miyake, T.; Kumagi, T.; Furukawa, S.; Hirooka, M.; Kawasaki, K.; Koizumi, M.; Todo, Y.; Yamamoto, S.; Tokumoto, Y.; Ikeda, Y.; et al. Short sleep duration reduces the risk of nonalcoholic fatty liver disease onset in men: a community-based longitudinal cohort study. J. Gastroenterol. 2015, 50, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Cantero, I.; Elorz, M.; Abete, I.; Marin, B.A.; Herrero, J.I.; Monreal, J.I.; Benito, A.; Quiroga, J.; Martínez, A.; Huarte, M.P.; et al. Ultrasound/Elastography techniques, lipidomic and blood markers compared to Magnetic Resonance Imaging in non-alcoholic fatty liver disease adults. Int. J. Med. Sci. 2019, 16, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Park, S.H. Radiologic evaluation of nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 7392–7402. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Brunt, E.M.; Kleiner, D.E.; Kowdley, K.V.; Chalasani, N.; Lavine, J.E.; Ratziu, V.; Mccullough, A. Endpoints and clinical trial design for nonalcoholic steatohepatitis. Hepatology 2011, 54, 344–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Iglesia, R.; Lopez-Legarrea, P.; Abete, I.; Bondia-Pons, I.; Navas-Carretero, S.; Forga, L.; Martinez, J.A.; Zulet, M.A. A new dietary strategy for long-term treatment of the metabolic syndrome is compared with the American Heart Association (AHA) guidelines: the MEtabolic Syndrome REduction in NAvarra (RESMENA) project. Br. J. Nutr. 2014, 111, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Colom, A.; Fiol, M.; Ruiz, M.; Compa, M.; Morey, M.; Moñino, M.; Romaguera, D. Association between access to public open spaces and physical activity in a mediterranean population at high cardiovascular risk. Int. J. Environ. Res. Public Health 2018, 15, 1285. [Google Scholar] [CrossRef]
- Bota, S.; Herkner, H.; Sporea, I.; Salzl, P.; Sirli, R.; Neghina, A.M.; Peck-Radosavljevic, M. Meta-analysis: ARFI elastography versus transient elastography for the evaluation of liver fibrosis. Liver Int. 2013, 33, 1138–1147. [Google Scholar] [CrossRef] [Green Version]
- De Sanidad, S.T.; de Castilla, B.S.J.; Soria, L. Propiedades clinimetricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Zhong, Q.-Y.; Gelaye, B.; Sánchez, S.E.; Williams, M.A. Psychometric Properties of the Pittsburgh Sleep Quality Index (PSQI) in a Cohort of Peruvian Pregnant Women. J. Clin. Sleep Med. 2015, 11, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005–2010. Am. J. Clin. Nutr. 2014, 100, 938–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martn-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galarregui, C.; Zulet, M.; Cantero, I.; Marín-Alejandre, B.; Monreal, J.; Elorz, M.; Benito-Boillos, A.; Herrero, J.; Tur, J.; Abete, I.; et al. Interplay of Glycemic Index, Glycemic Load, and Dietary Antioxidant Capacity with Insulin Resistance in Subjects with a Cardiometabolic Risk Profile. Int. J. Mol. Sci. 2018, 19, 3662. [Google Scholar] [CrossRef]
- Perumpail, B.J.; Khan, M.A.; Yoo, E.R.; Cholankeril, G.; Kim, D.; Ahmed, A. Clinical epidemiology and disease burden of nonalcoholic fatty liver disease. World J. Gastroenterol. 2017, 23, 8263–8276. [Google Scholar] [CrossRef]
- Kahl, S.; Straßburger, K.; Nowotny, B.; Livingstone, R.; Klüppelholz, B.; Keßel, K.; Hwang, J.H.; Giani, G.; Hoffmann, B.; Pacini, G.; et al. Comparison of liver fat indices for the diagnosis of hepatic steatosis and insulin resistance. PLoS ONE 2014, 9, e94059. [Google Scholar] [CrossRef]
- Qiu, Y.; Wang, S.-F.; Yu, C.; Chen, Q.; Jiang, R.; Pei, L.; Huang, Y.-L.; Pang, N.-Z.; Zhang, Z.; Ling, W.; et al. Association of Circulating Adipsin, Visfatin, and Adiponectin with Nonalcoholic Fatty Liver Disease in Adults: A Case-Control Study. Ann. Nutr. Metab. 2019, 74, 44–52. [Google Scholar] [CrossRef]
- Paschetta, E.; Belci, P.; Alisi, A.; Liccardo, D.; Cutrera, R.; Musso, G.; Nobili, V. OSAS-Related Inflammatory Mechanisms of Liver Injury in Nonalcoholic Fatty Liver Disease. Mediat. Inflamm. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Harrison, G.G.; Galal, O.M.; Ibrahim, N.; Khorshid, A.; Taha, A.S.; Leslie, J. Nadia Taha Saleh Underreporting of Food Intake by Dietary Recall Is Not Universal: A Comparison of Data from Egyptian and American Women. J. Nutr. 2000, 130, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- Eslamparast, T.; Tandon, P.; Raman, M. Dietary composition independent of weight loss in the management of non-alcoholic fatty liver disease. Nutrients 2017, 9, 800. [Google Scholar] [CrossRef] [PubMed]
- Cantero, I.; Abete, I.; Babio, N.; Arós, F.; Corella, D.; Estruch, R.; Fitó, M.; Hebert, J.R.; Martínez-González, M.Á.; Pintó, X.; et al. Dietary Inflammatory Index and liver status in subjects with different adiposity levels within the PREDIMED trial. Clin. Nutr. 2018, 37, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Cross, A.J.; McGlynn, K.A.; Abnet, C.C.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A.; Everhart, J.E.; Sinha, R. Association of meat and fat intake with liver disease and hepatocellular carcinoma in the NIH-AARP cohort. J. Natl. Cancer Inst. 2010, 102, 1354–1365. [Google Scholar] [CrossRef] [PubMed]
- Grandner, M.A.; Kripke, D.F.; Naidoo, N.; Langer, R.D. Relationships among dietary nutrients and subjective sleep, objective sleep, and napping in women. Sleep Med. 2010, 11, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Stern, J.H.; Grant, A.S.; Thomson, C.A.; Tinker, L.; Hale, L.; Brennan, K.M.; Woods, N.F.; Chen, Z. Short sleep duration is associated with decreased serum leptin, increased energy intake and decreased diet quality in postmenopausal women. Obesity 2014, 22, E55–E61. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Dietary nutrients associated with short and long sleep duration. Data from a nationally representative sample. Appetite 2013, 64, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.; Sun, W.; Liu, C.; Wu, S. Structural Validity of the Pittsburgh Sleep Quality Index in Chinese Undergraduate Students. Front. Psychol. 2016, 7, 1126. [Google Scholar] [CrossRef]
- Trovato, F.M.; Martines, G.F.; Brischetto, D.; Trovato, G.; Catalano, D. Neglected features of lifestyle: Their relevance in nonalcoholic fatty liver disease. World J. Hepatol. 2016, 8, 1459–1465. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Panjawatanan, P.; Ungprasert, P. Short sleep duration and risk of nonalcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 1802–1807. [Google Scholar] [CrossRef] [PubMed]
- Shen, N.; Wang, P.; Yan, W. Sleep Duration and the Risk of Fatty Liver Disease: A Systematic Review and Meta-analysis. Sci. Rep. 2016, 6, 31956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cespedes, E.M.; Hu, F.B.; Redline, S.; Rosner, B.; Alcantara, C.; Cai, J.; Hall, M.H.; Loredo, J.S.; Mossavar-Rahmani, Y.; Ramos, A.R.; et al. Comparison of Self-Reported Sleep Duration With Actigraphy: Results From the Hispanic Community Health Study/Study of Latinos Sueño Ancillary Study. Am. J. Epidemiol. 2016, 183, 561–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, M.; Li, Y.; Rueschman, M.N.; Winkelman, J.W.; Ellenbogen, J.M.; Solet, J.M.; Dulin, H.; Berkman, L.F.; Buxton, O.M. Measuring sleep: Accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep 2013, 36, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.; Lin, L.; Wang, Z.; Ding, L.; Huang, Y.; Wang, P.; Xu, Y.; Lu, J.; Xu, M.; Bi, Y.; et al. Short sleep duration and longer daytime napping are associated with non-alcoholic fatty liver disease in Chinese adults. J. Diabetes 2017, 9, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief communication: Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Chen, P.Y.; Chuang, L.P.; Chen, N.H.; Tu, Y.K.; Hsieh, Y.J.; Wang, Y.C.; Guilleminault, C. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: A bivariate meta-analysis. Sleep Med. Rev. 2017, 36, 57–70. [Google Scholar] [CrossRef]
- Faria, A.C.; da Costa, C.H.; Rufino, R. Sleep Apnea Clinical Score, Berlin Questionnaire, or Epworth Sleepiness Scale: which is the best obstructive sleep apnea predictor in patients with COPD? Int. J. Gen. Med. 2015, 8, 275–281. [Google Scholar] [CrossRef]
- Khassawneh, B.; Ghazzawi, M.; Khader, Y.; Alomari, M.; Amarin, Z.; Shahrour, B.; Hammouda, M. Symptoms and risk of obstructive sleep apnea in primary care patients in Jordan. Sleep Breath 2009, 13, 227–232. [Google Scholar] [CrossRef]
- Agrawal, S.; Duseja, A.; Aggarwal, A.; Das, A.; Mehta, M.; Dhiman, R.K.; Chawla, Y. Obstructive sleep apnea is an important predictor of hepatic fibrosis in patients with nonalcoholic fatty liver disease in a tertiary care center. Hepatol. Int. 2015, 9, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Petta, S.; Marrone, O.; Torres, D.; Buttacavoli, M.; Cammà, C.; Di Marco, V.; Licata, A.; Lo Bue, A.; Parrinello, G.; Pinto, A.; et al. Obstructive Sleep Apnea Is Associated with Liver Damage and Atherosclerosis in Patients with Non-Alcoholic Fatty Liver Disease. PLoS ONE 2015, 10, e0142210. [Google Scholar] [CrossRef] [PubMed]
- Pulixi, E.A.; Tobaldini, E.; Battezzati, P.M.; D’Ingianna, P.; Borroni, V.; Fracanzani, A.L.; Maggioni, M.; Pelusi, S.; Bulgheroni, M.; Zuin, M.; et al. Risk of obstructive sleep apnea with daytime sleepiness is associated with liver damage in non-morbidly obese patients with nonalcoholic fatty liver disease. PLoS ONE 2014, 9, e96349. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; De Pittà, C.; De Rui, M.; Corrias, M.; Turco, M.; Merkel, C.; Amodio, P.; Costa, R.; Skene, D.J.; Gatta, A. Sleep-wake abnormalities in patients with cirrhosis. Hepatology 2014, 59, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.E.; AL-Jahdali, F.; Ahmed, A.E.; Shirbini, N.; Abdullah, A.H.; Salim, B.; Ali, Y.Z.; Abdulrahman, A.; Khan, M.; Khaleid, A.; et al. Symptoms of Daytime Sleepiness and Sleep Apnea in Liver Cirrhosis Patients. Ann. Hepatol. 2017, 16, 591–598. [Google Scholar] [CrossRef]
- Kendzerska, T.B.; Smith, P.M.; Brignardello-Petersen, R.; Leung, R.S.; Tomlinson, G.A. Evaluation of the measurement properties of the Epworth sleepiness scale: A systematic review. Sleep Med. Rev. 2014, 18, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Herbert, V.; Pratt, D.; Emsley, R.; Kyle, S.D. Predictors of Nightly Subjective-Objective Sleep Discrepancy in Poor Sleepers over a Seven-Day Period. Brain Sci. 2017. [Google Scholar] [CrossRef]
- Okifuji, A.; Hare, B.D. Nightly analyses of subjective and objective (actigraphy) measures of sleep in fibromyalgia syndrome: what accounts for the discrepancy? Clin. J. Pain 2011, 27, 289–296. [Google Scholar] [CrossRef]
- Lugari, S.; Mantovani, A.; Nascimbeni, F.; Lonardo, A. Hypothyroidism and nonalcoholic fatty liver disease—A chance association? Horm. Mol. Biol. Clin. Investig. 2018. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls Mean ± SD | NAFLD Mean ± SD | p | Controls # Mean ± SE | NAFLD # Mean ± SE | p# | |
|---|---|---|---|---|---|---|
| Age (years) | 41.5 ± 9.8 | 51.4 ± 8.9 | <0.001 | 39.4 ± 9.8 | 51.4 ± 8.9 | <0.001 |
| Weight (kg) | 62.1 ± 10.0 | 94.6 ± 13.6 | <0.001 | - | - | - |
| BMI (kg/m2) | 22.1 ± 1.8 | 33.7 ± 3.9 | <0.001 | - | - | - |
| Sex (men/women) | 14/26 | 53/41 | 0.023 | - | - | - |
| SBP (mmHg) | 108 ± 17 | 132 ± 15 | <0.001 | 114 ± 4 | 129 ± 2 | 0.005 |
| DBP (mmHg) | 69 ± 10 | 87 ± 9 | <0.001 | 72.8 ± 2.3 | 85.3 ± 8 | <0.001 |
| Waist circumference (cm) | 75.6 ± 7.3 | 109.0 ± 8.8 | <0.001 | 90.7 ± 1.5 | 102.7 ± 0.8 | <0.001 |
| DXA Total adipose tissue (%) | 26.8 ± 7.6 | 42.3 ± 6.5 | <0.001 | 33.4 ± 1.7 | 39.6 ± 0.9 | 0.006 |
| DXA Visceral fat mass (kg) | 0.2 ± 0.21 | 2.3 ± 1.08 | <0.001 | 0.3 ± 0.25 | 2.3 ± 0.13 | <0.001 |
| Total cholesterol (mg/dL) | 191.5 ± 30.6 | 192.4 ± 39.5 | 0.906 | 183.7 ± 9.7 | 196.2 ± 5.0 | 0.344 |
| HDL cholesterol (mg/dL) | 63.1 ± 11.7 | 51.8 ± 14.3 | <0.001 | 56.5 ± 3.5 | 54.5 ± 1.8 | 0.682 |
| LDL cholesterol (mg/dL) | 114.7 ± 26.9 | 113.8 ± 35.7 | 0.896 | 114.7 ± 26.9 | 113.8 ± 35.7 | 0.607 |
| Triglycerides (mg/dL) | 68.8 ± 40.4 | 135.4 ± 77.9 | <0.001 | 86.0 ± 18.1 | 128.1 ± 9.4 | 0.086 |
| Fasting glucose (mg/dL) | 85.4 ± 6.6 | 106.4 ± 31.1 | <0.001 | 104.3 ± 6.6 | 98.5 ± 3.5 | 0.511 |
| Insulin (mU/L) | 4.3 ± 2.0 | 18.6 ± 10.7 | <0.001 | 12.2 ± 2.2 | 15.3 ± 1.1 | 0.312 |
| HOMA-IR | 0.9 ± 0.5 | 5.1 ± 4.8 | <0.001 | 4.7 ± 1.5 | 3.6 ± 0.5 | 0.416 |
| Leptin (ng/mL) | 10.0 ± 8.0 | 40.1 ± 33.5 | <0.001 | 43.7 ± 6.5 | 25.7 ± 3.4 | 0.043 |
| Adiponectin (µg/mL) | 13.5 ± 4.7 | 6.8 ± 2.3 | <0.001 | 11.9 ± 0.8 | 7.5 ± 4.2 | <0.001 |
| C-reactive protein (mg/dL) | 0.47 ± 0.6 | 0.45 ± 0.6 | 0.853 | 0.72 ± 0.2 | 0.34 ± 0.1 | 0.061 |
| AST (IU/L) | 21.4 ± 6.4 | 24.5 ± 9.9 | 0.035 | 19.9 ± 2.4 | 25.3 ± 1.2 | 0.094 |
| ALT (IU/L) | 17.2 ± 13.5 | 33.7 ± 18.2 | <0.001 | 17.9 ± 4.5 | 33.5 ± 2.3 | 0.010 |
| Hepatic Steatosis Index (HSI) | 29.6 ± 3.1 | 45.4 ± 45.4 | <0.001 | - | - | - |
| ARFI liver stiffness (m/s) | 1.34 ± 0.2 | 1.86 ± 0.7 | <0.001 | 1.82 ± 0.1 | 1.65 ± 0.8 | 0.396 |
| Controls Mean ± SD | NAFLD Mean ± SD | p | |
|---|---|---|---|
| Energy and macronutrients | |||
| Total energy (kcal) | 2677 ± 749 | 2697 ± 1089 | 0.906 |
| Carbohydrates (%) | 43 ± 6.6 | 43 ± 7.0 | 0.922 |
| Proteins (%) | 16 ± 3.2 | 17 ± 3.8 | 0.212 |
| Lipids (%) | 39 ± 5.5 | 37 ± 7.0 | 0.159 |
| Dietary fiber (g) | 33 ± 16 | 25 ± 9 | 0.001 |
| Food groups | |||
| Fruit (g) | 345 ± 179 | 290 ± 197 | 0.141 |
| Vegetables (g) | 431 ± 236 | 285 ± 120 | <0.001 |
| Legumes (g) | 21 ± 14 | 21 ± 10 | 0.738 |
| Fish (g) | 99 ± 46 | 88 ± 45 | 0.232 |
| Meat products (g) | 154 ± 80 | 190 ± 78 | 0.019 |
| Micronutrients | |||
| Vitamin A (µg) | 1526 ± 650 | 1119 ± 893 | 0.014 |
| Vitamin C (mg) | 250 ± 76 | 192 ± 98 | 0.001 |
| Vitamin D (µg) | 8 ± 3.8 | 6 ± 4.0 | 0.041 |
| Vitamin E (mg) | 12 ± 4.1 | 10 ± 4.3 | 0.017 |
| Vitamin B9 (µg) | 445 ± 132 | 360 ± 151 | 0.003 |
| Marine Omega-3 (g) | 0.90 ± 0.5 | 0.62 ± 0.5 | 0.003 |
| Lifestyle factors | |||
| Physical Activity (METs-min/week) | 5801 ± 4225 | 3049 ± 2440 | <0.001 |
| Smokers (%) | 35.0 | 20.7 | 0.080 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Sleep duration ≤6 h or >6 h | 0.33 (0.13; 0.84) * | 0.37 (0.14; 0.98) * | 0.39 (0.09; 1.71) | 0.34 (0.13; 0.85) * | 0.15 (0.02; 1.04) |
| Sleep efficiency (%) | 0.974 (0.94; 1.009) | 0.981 (0.94; 1.01) | 0.979 (0.93; 1.02) | 0.975 (0.94; 1.01) | 0.981 (0.93; 1.03) |
| Total time in bed (h) | 1.19 (0.75; 1.88) | 1.11 (0.67; 1.83) | 1.79 (0.75; 4.29) | 1.20 (0.76; 1.89) | 1.29 (0.50; 3.32) |
| Sleep disturbance score | 1.23 (1.08; 1.39) ** | 1.21 (1.06; 1.38) ** | 1.38 (1.08; 1.75) ** | 1.22 (1.08; 1.39) ** | 1.59 (1.11; 2.28) * |
| Sleep quality (Total PSQI score) | 1.15 (1.01; 1.33) * | 1.13 (0.98; 1.31) | 1.14 (0.93; 1.39) | 1.15 (0.99; 1.32) | 1.10 (0.88; 1.38) |
| β (95% IC) | p | Adjusted R2 | p Model | ||
|---|---|---|---|---|---|
| Sleep duration ≤6 h or >6 h | Model 1 | −0.30 (−0.57; −0.02) | 0.034 | ||
| Model 2 | −0.28 (−0.56; −0.002) | 0.048 | 0.028 | 0.135 | |
| Model 3 | −0.25 (−0.54; 0.02) | 0.078 | 0.099 | 0.022 | |
| Model 4 | −0.22 (−0.53; 0.08) | 0.154 | 0.058 | 0.123 | |
| Model 5 | −0.27 (−0.55; 0.01) | 0.059 | 0.188 | 0.002 | |
| Model 6 | −0.22 (−0.50; 0.06) | 0.114 | 0.205 | <0.001 | |
| Sleep Efficiency | Model 1 | −0.01 (−0.02; −0.0002) | 0.045 | ||
| Model 2 | −0.009 (−0.01; 0.0005) | 0.063 | 0.023 | 0.165 | |
| Model 3 | −0.008 (−0.01; 0.001) | 0.087 | 0.097 | 0.023 | |
| Model 4 | −0.008 (−0.02; 0.002) | 0.131 | 0.061 | 0.114 | |
| Model 5 | 0.008 (−0.01; 0.0008) | 0.075 | 0.184 | 0.002 | |
| Model 6 | −0.005 (−0.01; 0.004) | 0.248 | 0.195 | 0.001 | |
| Total time in bed | Model 1 | 0.02 (−0.11; 0.15) | 0.750 | ||
| Model 2 | 0.01 (−0.12; 0.15) | 0.805 | −0.014 | 0.646 | |
| Model 3 | 0.002 (−0.13; 0.13) | 0.974 | 0.064 | 0.072 | |
| Model 4 | −0.01 (−0.16; 0.13) | 0.863 | 0.031 | 0.233 | |
| Model 5 | −0.01 (−0.14; 0.11) | 0.868 | 0.150 | 0.007 | |
| Model 6 | −0.02 (−0.14; 0.10) | 0.781 | 0.182 | 0.002 | |
| Sleep disturbance score | Model 1 | 0.03 (0.001; 0.06) | 0.037 | ||
| Model 2 | 0.02 (−0.001; 0.06) | 0.064 | 0.023 | 0.166 | |
| Model 3 | 0.02 (−0.002; 0.05) | 0.069 | 0.102 | 0.020 | |
| Model 4 | 0.04 (0.005; 0.07) | 0.024 | 0.097 | 0.042 | |
| Model 5 | 0.04 (0.005; 0.07) | 0.024 | 0.203 | 0.001 | |
| Model 6 | 0.03 (0.004; 0.07) | 0.081 | 0.212 | <0.001 | |
| Sleep quality (Total PSQI score) | Model 1 | 0.04 (0.004; 0.07) | 0.029 | ||
| Model 2 | 0.03 (−0.0002; 0.07) | 0.051 | 0.027 | 0.142 | |
| Model 3 | 0.04 (0.006; 0.08) | 0.022 | 0.123 | 0.009 | |
| Model 4 | 0.04 (0.002; 0.09) | 0.039 | 0.086 | 0.057 | |
| Model 5 | 0.04 (0.006; 0.08) | 0.023 | 0.204 | 0.001 | |
| Model 6 | 0.03 (−0.005; 0.07) | 0.085 | 0.211 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Riezu-Boj, J.I.; Milagro, F.I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; et al. Association between Sleep Disturbances and Liver Status in Obese Subjects with Nonalcoholic Fatty Liver Disease: A Comparison with Healthy Controls. Nutrients 2019, 11, 322. https://doi.org/10.3390/nu11020322
Marin-Alejandre BA, Abete I, Cantero I, Riezu-Boj JI, Milagro FI, Monreal JI, Elorz M, Herrero JI, Benito-Boillos A, Quiroga J, et al. Association between Sleep Disturbances and Liver Status in Obese Subjects with Nonalcoholic Fatty Liver Disease: A Comparison with Healthy Controls. Nutrients. 2019; 11(2):322. https://doi.org/10.3390/nu11020322
Chicago/Turabian StyleMarin-Alejandre, Bertha Araceli, Itziar Abete, Irene Cantero, Jose I. Riezu-Boj, Fermín I. Milagro, J. Ignacio Monreal, Mariana Elorz, José Ignacio Herrero, Alberto Benito-Boillos, Jorge Quiroga, and et al. 2019. "Association between Sleep Disturbances and Liver Status in Obese Subjects with Nonalcoholic Fatty Liver Disease: A Comparison with Healthy Controls" Nutrients 11, no. 2: 322. https://doi.org/10.3390/nu11020322
APA StyleMarin-Alejandre, B. A., Abete, I., Cantero, I., Riezu-Boj, J. I., Milagro, F. I., Monreal, J. I., Elorz, M., Herrero, J. I., Benito-Boillos, A., Quiroga, J., Martinez-Echeverria, A., Uriz-Otano, J. I., Huarte-Muniesa, M. P., Tur, J. A., Martínez, J. A., & Zulet, M. A. (2019). Association between Sleep Disturbances and Liver Status in Obese Subjects with Nonalcoholic Fatty Liver Disease: A Comparison with Healthy Controls. Nutrients, 11(2), 322. https://doi.org/10.3390/nu11020322