Role of Food Neophobia and Allergen Content in Food Choices for a Polish Cohort of Young Women




Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethics Approval Statement
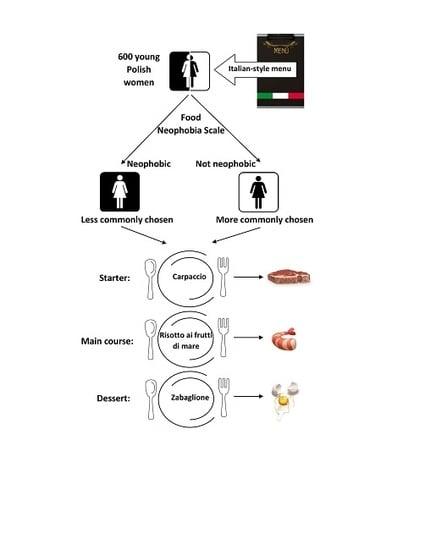
2.2. Study Participants
2.3. Choice Experiment
- −
- Allergen content—defined as a content of ingredients that are among 14 major food allergens listed in Regulation (EU) No 1169/2011 [29]—it was planned to have in each category at least one dish with the noticeable allergen (as one of the main components of the dish) and at least one dish with no allergens at all.
- −
- Neophobic potential—defined as a content of ingredients that for the Polish consumers may cause a neophobic response, due to the fact that they are not commonly consumed and are not typical of the Polish diet (the following were included: raw meat [30], seafood [31], spinach and fennel [32], and egg desserts [33] —these items are, in general, rejected by neophobic individuals)—it was planned to have in each category at least one dish with the noticeable component that may be perceived as unknown/not consumed (as one of the main components of dish) and at least one dish with no such components at all (all components neutral).
- −
- Perceived lack of healthiness—defined as a content of ingredients that for the Polish consumers may be perceived as not healthy (the following were included: meat [34], bread [35], pasta [36], and alcohol [37] — these items are perceived by some consumers as not healthy)—it was planned to have in each category at least one dish with the noticeable component that may be perceived as unhealthy (as one of the main components of dish) and at least one dish with no such components at all (all components neutral).
2.4. Assessment of Food Neophobia
- −
- Low food neophobia level—FNS score < mean value minus SD value.
- −
- Average food neophobia level—FNS score within the range from mean value minus SD to mean value plus SD.
- −
- High food neophobia level—FNS score > mean value plus SD value.
2.5. Statistical Analysis
- −
- The influence of the information with the allergens listed on the consumer choices of dishes was verified (menu A versus menu B)—as no differences were stated, the results obtained for menu A and menu B may have been combined.
- −
- The influence of food neophobia (FNS score) on the consumer choices of dishes was verified—as the influence was stated, a deepened analysis was conducted taking into account the general characteristics of the chosen dishes.
- −
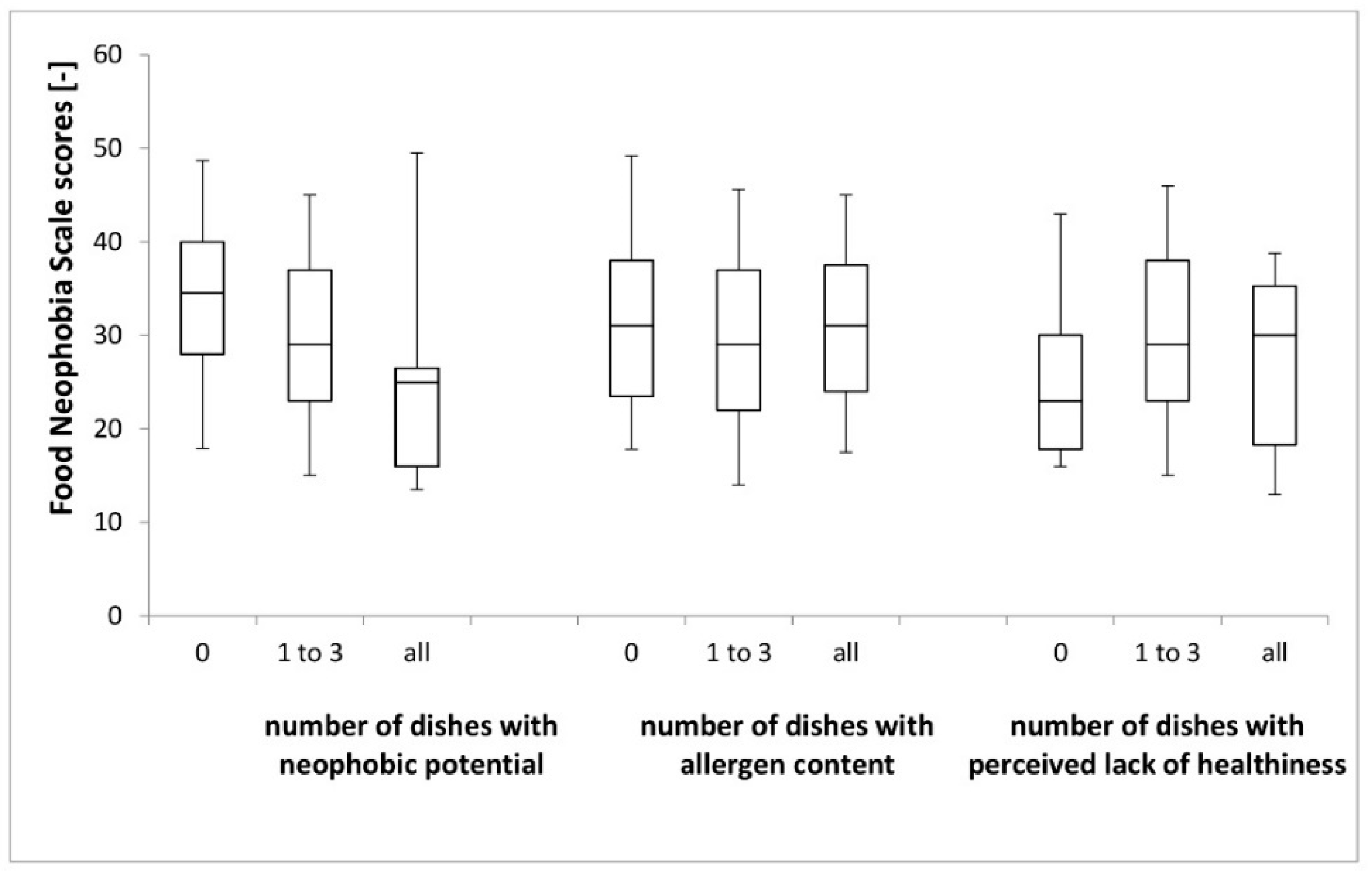
- The influence of food neophobia (FNS score) on the characteristics of chosen dishes—for this analysis, in terms of allergen content, neophobic potential and the perceived lack of healthiness, the choices of each respondent for each course (Table 2) were stratified into the following groups:
- (a)
- Choice of dishes with no allergen content; choice of 1–3 dishes with allergen content; choice of all dishes (4 of them) with allergen content.
- (b)
- Choice of dishes with no neophobic potential; choice of 1–3 dishes with neophobic potential; choice of all dishes (4 of them) with neophobic potential.
- (c)
- Choice of dishes with no perceived lack of healthiness; choice of 1–3 dishes with perceived lack of healthiness; choice of perceived lack of healthiness (4 of them) with perceived lack of healthiness.
3. Results
3.1. Characteristics of the Studied Group
3.2. Influence of the Information with the Allergens Listed on the Consumer Choices
3.3. Influence of the Food Neophobia on the Consumer Choices
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Manippa, V.; Padulo, C.; van der Laan, L.N.; Brancucci, A. Gender Differences in Food Choice: Effects of Superior Temporal Sulcus Stimulation. Front. Hum. Neurosci. 2017, 11, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Hardcastle, S.J.; Thøgersen-Ntoumani, C.; Chatzisarantis, N.L. Food Choice and Nutrition: A Social Psychological Perspective. Nutrients 2015, 7, 8712–8715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiefer, I.; Rathmanner, T.; Kunze, M. Eating and dieting differences in men and women. J. Men’s Health Gend. 2005, 2, 194–201. [Google Scholar] [CrossRef]
- Murnen, S.K.; Smolak, L. Femininity, masculinity, and disordered eating: A meta-analytic review. Int. J. Eat Disord. 1997, 22, 231–242. [Google Scholar] [CrossRef]
- Charles, N.; Kerr, M. Women, Food and Families; Manchester University Press: Manchester, UK, 1990. [Google Scholar] [CrossRef]
- Krebs, N.; Bagby, S.; Bhutta, Z.A.; Dewey, K.; Fall, C.; Gregory, F.; Hay, W., Jr.; Rhuman, L.; Caldwell, C.W.; Thornburg, K.L. International summit on the nutrition of adolescent girls and young women: Consensus statement. Ann. N. Y. Acad. Sci. 2017, 1400, 3–7. [Google Scholar] [CrossRef]
- Lawrence, W.; Barker, M. A review of factors affecting the food choices of disadvantaged women. Proc. Nutr. Soc. 2009, 68, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Westenhoefer, J. Age and gender dependent profile of food choice. Forum Nutr. 2005, 57, 44–51. [Google Scholar]
- Wilkinson, L.L.; Brunstrom, J.M. Sensory specific satiety: More than just habituation? Appetite 2016, 103, 221–228. [Google Scholar] [CrossRef]
- Dong, D.; Wang, Y.; Jackson, T.; Chen, S.; Wang, Y.; Zhou, F.; Chen, H. Impulse control and restrained eating among young women: Evidence for compensatory cortical activation during a chocolate-specific delayed discounting task. Appetite 2016, 105, 477–486. [Google Scholar] [CrossRef]
- Field, A.E.; Haines, J.; Rosner, B.; Willett, W.C. Weight-control behaviors and subsequent weight change among adolescents and young adult females. Am. J. Clin. Nutr. 2010, 91, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Qian, H.; Fu, H. To be thin but not healthy—The body-image dilemma may affect health among female university students in China. PLoS ONE 2018, 13, 0205282. [Google Scholar] [CrossRef] [PubMed]
- Casazza, K.; Brown, A.; Astrup, A.; Bertz, F.; Baum, C.; Brown, M.B.; Dawson, J.; Durant, N.; Dutton, G.; Fields, D.A.; et al. Weighing the Evidence of Common Beliefs in Obesity Research. Crit. Rev. Food Sci. Nutr. 2015, 55, 2014–2053. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, D.; Kite, J.; Vassallo, A.J.; Chau, J.Y.; Partridge, S.; Freeman, B.; Gill, T. Food Trends and Popular Nutrition Advice Online-Implications for Public Health. Online J. Public Health Inf. 2018, 10, 213. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.L. The Gluten-Free Diet: Fad or Necessity? Diabetes Spectr. 2017, 30, 118–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, D.T.; Slutzky, A.R. Gluten sensitivity: New epidemic or new myth? Procedings (Bayl. Univ. Med. Cent) 2014, 27, 377–378. [Google Scholar] [CrossRef]
- Lebwohl, B.; Cao, Y.; Zong, G.; Hu, F.B.; Green, P.H.R.; Neugut, A.I.; Rimm, E.B.; Sampson, L.; Dougherty, L.W.; Giovannucci, E.; et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: Prospective cohort study. BMJ 2017, 357, j1892. [Google Scholar] [CrossRef]
- Priven, M.; Baum, J.; Vieira, E.; Fung, T.; Herbold, N. The Influence of a Factitious Free-From Food Product Label on Consumer Perceptions of Healthfulness. J. Acad. Nutr. Diet. 2015, 115, 1808–1814. [Google Scholar] [CrossRef]
- Asioli, D.; Aschemann-Witzel, J.; Caputo, V.; Vecchio, R.; Annunziata, A.; Næs, T.; Varela, P. Making sense of the “clean label” trends: A review of consumer food choice behavior and discussion of industry implications. Food Res. Int. 2017, 99, 58–71. [Google Scholar] [CrossRef]
- Pali-Schöll, I.; Jensen-Jarolim, E. Gender aspects in food allergy. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 249–255. [Google Scholar] [CrossRef]
- Afify, S.M.; Pali-Schöll, I. Adverse reactions to food: The female dominance-A secondary publication and update. World Allergy Organ J. 2017, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Zysk, W.; Głąbska, D.; Guzek, D. Food Neophobia in Celiac Disease and Other Gluten-Free Diet Individuals. Nutrients 2019, 11, 1762. [Google Scholar] [CrossRef] [PubMed]
- Ostrove, J.M.; Adler, N.E.; Kuppermann, M.; Washington, A.E. Objective and subjective assessments of socioeconomic status and their relationship to self-rated health in an ethnically diverse sample of pregnant women. Health Psychol. 2000, 19, 613–618. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, E.; Newbury, A.; Appleton, K.M. The Psychology of Nutrition with Advancing Age: Focus on Food Neophobia. Nutrients 2019, 11, 151. [Google Scholar] [CrossRef]
- Poland on Plate 2018: More and More Poles Use Gastronomic Facility (Report). Available online: http://www.portalspozywczy.pl/horeca/wiadomosci/polska-na-talerzu-2018-coraz-wiecej-polakow-korzysta-z-lokali-gastronomicznych-raport,159812_2.html (accessed on 29 August 2019).
- Poland on Plate 2018: Sour Flavors and Italian Restaurants are the Culinary Choices of Poles (Report). Available online: http://www.portalspozywczy.pl/horeca/wiadomosci/kwasne-smaki-i-restauracje-wloskie-kulinarnymi-wyborami-polakow,150282.html (accessed on 29 August 2019).
- Głuchowski, A.; Rasińska, E.; Czarniecka-Skubina, E. Rynek usług gastronomicznych w Polsce na przykładzie Warszawy [The Catering Services Market in Poland on the Example of Warsaw]. Handel Wew. 2017, 4, 118–133. [Google Scholar]
- EEA relevance. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004. Off. J. Eur. Union 2011, 20, 18–63. [Google Scholar]
- Cooke, L.; Carnell, S.; Wardle, J. Food neophobia and mealtime food consumption in 4–5 year old children. Int. J. Behav. Nutr. Phys. Act. 2006, 6, 14. [Google Scholar] [CrossRef]
- Knaapila, A.; Silventoinen, K.; Broms, U.; Rose, R.J.; Perola, M.; Kaprio, J.; Tuorila, H.M. Food neophobia in young adults: Genetic architecture and relation to personality, pleasantness and use frequency of foods, and body mass index—A twin study. Behav. Genet. 2011, 41, 512–521. [Google Scholar] [CrossRef]
- Nekitsing, C.; Hetherington, M.M.; Blundell-Birtill, P. Developing Healthy Food Preferences in Preschool Children Through Taste Exposure, Sensory Learning, and Nutrition Education. Curr. Obes. Rep. 2018, 7, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Cooke, L.; Wardle, J.; Gibson, E.L. Relationship between parental report of food neophobia and everyday food consumption in 2-6-year-old children. Appetite 2003, 41, 205–206. [Google Scholar] [CrossRef]
- Frewer, L.; Van Trijp, H. Understanding Consumers of Food Products, 1st ed.; Woodhead Publishing: Cambridge, UK, 2007; p. 696. [Google Scholar]
- Gellynck, X.; Kühne, B.; Van Bockstaele, F.; Van de Walle, D.; Dewettinck, K. Consumer perception of bread quality. Appetite 2009, 53, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. International Trade Commission. Industry and Trade Summary: Pasta; U.S. International Trade Commission: Washington, DC, USA, 2003; p. 47.
- Rosenberg, G.; Bauld, L.; Hooper, L.; Buykx, P.; Holmes, J.; Vohra, J. New national alcohol guidelines in the UK: Public awareness, understanding and behavioural intentions. J. Public Health 2018, 40, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Pliner, P.; Hobden, K. The development of a scale to measure the trait of food neophobia in humans. Appetite 1992, 19, 105–120. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development; Sage Publications: Newbury Park, NJ, USA, 1991. [Google Scholar]
- Tuorila, H.M.; Lähteenmäki, L.; Pohjalainen, L.; Lotti, L. Food neophobia among the Finns and related responses to familiar and unfamiliar foods. Food Qual. Prefer. 2001, 12, 29–37. [Google Scholar] [CrossRef]
- Falciglia, G.A.; Couch, S.C.; Gribble, L.S.; Pabst, S.M.; Frank, R.A. Food neophobia in childhood affects dietary variety. J. Am. Diet. Assoc. 2000, 100, 1474–1481. [Google Scholar] [CrossRef]
- Guzek, D.; Głąbska, D.; Lange, E.; Jezewska-Zychowicz, M. A Polish study on the influence of food neophobia in children (10–12 years old) on the intake of vegetables and fruits. Nutrients 2017, 9, 563. [Google Scholar] [CrossRef]
- Guzek, D.; Głąbska, D.; Mellová, B.; Zadka, K.; Żywczyk, K.; Gutkowska, K. Influence of Food Neophobia Level on Fruit and Vegetable Intake and Its Association with Urban Area of Residence and Physical Activity in a Nationwide Case-Control Study of Polish Adolescents. Nutrients 2018, 13, 897. [Google Scholar] [CrossRef]
- Watson, E. Health/Weight Conscious Consumers are Driving the Gluten-Free Market, Not Celiac, Says Mintel. Available online: http://www.foodnavigator-usa.com/Markets/Health-weight-consciousconsumers- are-driving-the-gluten-freemarket-not-celiacs-says-Mintel (accessed on 24 September 2019).
- Niland, B.; Cash, B.D. Health Benefits and Adverse Effects of a Gluten-Free Diet in Non-Celiac Disease Patients. Gastroenterol. Hepatol. 2018, 14, 82–91. [Google Scholar]
- Czarnocińska, J.; Jeżewska-Zychowicz, M.; Babicz-Zielińska, E.; Kowalkowska, J.; Wądołowska, L. Postawy Względem Żywności, Żywienia i Zdrowia a Zachowania Żywieniowe Dziewcząt i Młodych Kobiet w Polsce; Wydawnictwo UWM: Olsztyn, Poland, 2013; pp. 1–114. [Google Scholar]
- Missbach, B.; Schwingshackl, L.; Billmann, A.; Mystek, A.; Hickelsberger, M.; Bauer, G.; König, J. Gluten-free food database: The nutritional quality and cost of packaged gluten-free foods. PeerJ 2015, 22, 1337. [Google Scholar] [CrossRef]
- Bailey, R.L.; Denby, N.; Haycock, B.; Sherif, K.; Steinbaum, S.; von Schacky, C. Perceptions of a Healthy Diet: Insights From a 3-Country Survey. Nutr. Today 2015, 50, 282–287. [Google Scholar] [CrossRef]
- Pila, E.; Mond, J.M.; Griffiths, S.; Mitchison, D.; Murray, S.B. A thematic content analysis of #cheatmeal images on social media: Characterizing an emerging dietary trend. Int. J. Eat. Disord. 2017, 50, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Ju, S.; Chang, H. Food allergy knowledge, perception of food allergy labeling, and level of dietary practice: A comparison between children with and without food allergy experience. Nutr. Res. Pr. 2015, 9, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, Y.L.B. Everybody Else Got to Have This Cookie: The Effects of Food Allergen Labels on the Well-Being of Canadians. Master’s Thesis, McMaster University, Hamilton, ON, Canada, 2011. Available online: http://hdl.handle.net/11375/11078 (accessed on 22 October 2019).
- Ju, S.Y.; Park, J.H.; Kwak, T.K.; Kim, K.E. Attitudes and preferences of consumers toward food allergy labeling practices by diagnosis of food allergies. Nutr. Res. Pr. 2015, 9, 517–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelisse-Vermaat, J.R.; Voordouw, J.; Yiakoumaki, V.; Theodoridis, G.; Frewer, L.J. Food-allergic consumers’ labelling preferences: A cross-cultural comparison. Eur. J. Public Health 2008, 18, 115–120. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Committee on Military Nutrition Research. In Not Eating Enough: Overcoming Underconsumption of Military Operational Rations; Marriott, B.M., Ed.; Eating Situations, Food Appropriateness, and Consumption; National Academies Press (US): Washington, DC, USA, 1995; p. 18. Available online: https://www.ncbi.nlm.nih.gov/books/NBK232460 (accessed on 24 September 2019).
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 210, 413. [Google Scholar] [CrossRef]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C. Food neophobia and picky/fussy eating in children: A review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef]
- Koivisto-Hursti, U.-K.; Sjödén, P.O. Food and general neophobia and their relationship with self-reported food choice: Familial resemblance in Swedish families with children of ages 7–17 years. Appetite 1997, 29, 89–103. [Google Scholar] [CrossRef]
- Nicklaus, S.; Boggio, V.; Chababnet, C.; Issanchou, S. Prospective study of food variety seeking in childhood, adolescence and early adult life. Appetite 2005, 44, 289–297. [Google Scholar] [CrossRef]
- Knaapila, A.J.; Sandell, M.A.; Vaarno, J.; Hoppu, U.; Puolimatka, T.; Kaljonen, A.; Lagström, H. Food neophobia associates with lower dietary quality and higher BMI in Finnish adults. Public Health Nutr. 2015, 18, 2161–2171. [Google Scholar] [CrossRef]
- Perry, R.A.; Mallan, K.M.; Koo, J.; Mauch, C.E.; Daniels, L.A.; Magarey, A.M. Food neophobia and its association with diet quality and weight in children aged 24 months: A cross sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 13, 13. [Google Scholar] [CrossRef]
- Cooke, L.J.; Wardle, J.; Gibson, E.L.; Sapochnik, M.; Sheiham, A.; Lawson, M. Demographic, familial and trait predictors of fruit and vegetable consumption by pre-school children. Public Health Nutr. 2004, 7, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Camarena, D.; Sanjuán, A.; Philippidis, G. Influence of ethnocentrism and neo-phobia on ethnic food consumption in Spain. Appetite 2011, 57, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Martins, Y.; Pliner, P. Human food choices: An examination of the factors underlying acceptance/rejection of novel and familiar animal and nonanimal foods. Appetite 2005, 45, 214–224. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Dishes and Descriptions Provided in a Mock Italian-Style Menu | Defined Categories of Dishes Based on the Ingredients | ||||
|---|---|---|---|---|---|
| Course | Dish | Provided Description | Content of Ingredients that are Among 14 Major Food Allergens Listed in Regulation (EU) No 1169/2011 [29] | Content of Ingredients that for the Consumers may Cause the Neophobic Response | Content of Ingredients that for the Consumers may be Perceived as not Healthy |
| Starter | Carpaccio | Paper-thin raw beef slices | – | Raw meat | Meat |
| Caprese | Slices of tomatoes and mozzarella | Milk and products thereof (including lactose) (annex 2, pt. 7) | – | – | |
| Soup | Minestrone | Vegetable soup with zucchini, green beans, carrot, spinach and fennel | – | Spinach and fennel | – |
| Pappa al pomodoro | Tomato bread soup | Cereals containing gluten (annex 2, pt. 1) | – | Bread | |
| Main course | Risotto ai frutti di mare | Seafood risotto with parmesan | Crustaceans and products thereof (annex 2, pt. 2); milk and products thereof (including lactose) (annex 2, pt. 7); molluscs and products thereof (annex 2, pt. 14); | Seafood | – |
| Spaghetti alla siciliana | Spaghetti with tomatoes and roasted eggplant | Cereals containing gluten (annex 2, pt. 1) | – | Pasta | |
| Bistecca alla fiorentina | Beef steak served with rosemary roasted potatoes | – | – | Meat | |
| Dessert | Tiramisu | Espresso-dipped ladyfingers with mascarpone-egg cream | Cereals containing gluten (annex 2, pt. 1); eggs and products thereof (including lactose) (annex 2, pt. 3); milk and products thereof (including lactose) (annex 2, pt. 7) | Egg cream | – |
| Zabaglione | Egg yolk dessert with alcohol | Eggs and products thereof (including lactose) (annex 2, pt. 3) | Egg dessert | Alcohol | |
| Granita | Frozen fruit dessert | – | – | – | |
| Variables | Planned Dish | Course | ||
|---|---|---|---|---|
| Allergen Content | Neophobic Potential | Perceived Lack of Healthiness | ||
| − | − | − | Granita | Dessert |
| + | − | − | Caprese | Starter |
| − | + | − | Minestrone | Soup |
| − | − | + | Bistecca alla fiorentina | Main course |
| + | + | + | Zabaglione | Dessert |
| + | + | − | Risotto ai frutti di mare | Main course |
| Tiramisu | Dessert | |||
| + | − | + | Pappa al pomodoro | Soup |
| Spaghetti alla siciliana | Main course | |||
| − | + | + | Carpaccio | Starter |
| Characteristics | Results | |
|---|---|---|
| Age (years) | Mean ± SD | 21.2 ± 1.9 |
| Median (range) | 21 * (18–30) | |
| Place of residence | Village | 72 (12.0%) |
| Towns and cities <500,000 inhabitants | 153 (25.5%) | |
| Cities >500,000 inhabitants | 375 (62.5%) | |
| Economic status | Very bad and bad | 36 (6.0%) |
| Average | 234 (39.0%) | |
| Good and very good | 330 (55.0%) | |
| FNS Score | Total (n = 600) | Food Neophobia Level | ||
|---|---|---|---|---|
| Low 1 (n = 104) | Average 2 (n = 407) | High 3 (n = 89) | ||
| Mean ± SD | 30.2 ± 10.1 | 16.1 ± 2.4 | 30.3 ± 5.7 | 46.3 ± 5.9 |
| 95% CI | 29.4–31.0 | 15.6–16.5 | 29.8–30.9 | 45.1–47.5 |
| Median | 29 * | 16 * | 30 * | 44 * |
| Range | 10–70 | 10–19 | 20–40 | 41–70 |
| 25th–75th | 23–37 | 14–18 | 26–35 | 42–49 |
| Characteristics | Mean ± SD | Median (range) | P-Value | |
|---|---|---|---|---|
| Place of residence | Village | 33.5 ± 9.9 | 32 (15–56) a | 0.0070 |
| Towns and cities <500,000 inhabitants | 30.2 ± 9.6 | 29 (10–56) b | ||
| Cities >500,000 inhabitants | 29.6 ± 10.2 | 29 * (11–70) b | ||
| Economic status | Good and very good | 29.9 ± 10.4 | 29 *(10–70) | 0.1775 |
| Average | 31.0 ± 9.6 | 31 (11–58) | ||
| Very bad and bad | 28.2 ± 10.3 | 30 (13–50) | ||
| Course | Dish | Total | Menu A 1 (n = 300) | Menu B 2 (n = 300) | p-Value |
|---|---|---|---|---|---|
| Starters | Carpaccio | 193 (34.8) | 97 (35.3) | 96 (34.4) | 0.8302 |
| Caprese | 361 (65.2) | 178 (64.7) | 183 (65.6) | ||
| Soup | Minestrone | 178 (33.9) | 92 (35.0) | 86 (32.8) | 0.6671 |
| Pappa al pomodoro | 347 (66.1) | 171 (65.0) | 176 (67.2) | ||
| Main course | Risotto ai frutti di mare | 149 (24.2) | 70 (21.8) | 79 (23.5) | 0.4499 |
| Spaghetti alla siciliana | 281 (45.8) | 131 (40.8) | 150 (44.7) | 0.1408 | |
| Bistecca alla fiorentina | 184 (30.0) | 120 (37.4) | 107 (31.8) | 0.3125 | |
| Dessert | Tiramisu | 377 (55.1) | 182 (53.8) | 195 (56.4) | 0.3106 |
| Zabaglione | 90 (13.2) | 39 (11.5) | 51 (14.7) | 0.2085 | |
| Granita | 217 (31.7) | 117 (34.6) | 100 (28.9) | 0.1740 |
| Course | Dish | Total | Level of Food Neophobia | p-Value | ||
|---|---|---|---|---|---|---|
| Low 1 | Average 2 | High 3 | ||||
| Starters | Carpaccio | 193 (34.8) | 49 (48.0) | 123 (32.7) | 21 (27.6) | 0.0058 |
| Caprese | 361 (65.2) | 53 (52.0) | 253 (67.3) | 55 (72.4) | ||
| Soup | Minestrone | 178 (33.9) | 27 (31.0) | 125 (34.9) | 26 (32.5) | 0.7581 |
| Pappa al pomodoro | 347 (66.1) | 60 (69.0) | 233 (65.1) | 54 (67.5) | ||
| Main course | Risotto ai frutti di mare | 149 (22.7) | 49 (40.8) | 92 (20.6) | 8 (8.9) | <0.0001 |
| Spaghetti alla siciliana | 281 (42.7) | 36 (30.0) | 200 (44.7) | 45 (50.0) | ||
| Bistecca alla fiorentina | 227 (34.6) | 35 (29.2) | 155 (34.7) | 37 (41.1) | ||
| Dessert | Tiramisu | 377 (55.1) | 61 (51.7) | 264 (57.0) | 52 (50.5) | <0.0001 |
| Zabaglione | 90 (13.2) | 19 (16.1) | 63 (13.6) | 8 (7.8) | ||
| Granita | 217 (31.7) | 38 (32.2) | 136 (29.4) | 43 (41.7) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzek, D.; Pęska, J.; Głąbska, D. Role of Food Neophobia and Allergen Content in Food Choices for a Polish Cohort of Young Women. Nutrients 2019, 11, 2622. https://doi.org/10.3390/nu11112622
Guzek D, Pęska J, Głąbska D. Role of Food Neophobia and Allergen Content in Food Choices for a Polish Cohort of Young Women. Nutrients. 2019; 11(11):2622. https://doi.org/10.3390/nu11112622
Chicago/Turabian StyleGuzek, Dominika, Joanna Pęska, and Dominika Głąbska. 2019. "Role of Food Neophobia and Allergen Content in Food Choices for a Polish Cohort of Young Women" Nutrients 11, no. 11: 2622. https://doi.org/10.3390/nu11112622
APA StyleGuzek, D., Pęska, J., & Głąbska, D. (2019). Role of Food Neophobia and Allergen Content in Food Choices for a Polish Cohort of Young Women. Nutrients, 11(11), 2622. https://doi.org/10.3390/nu11112622