2. Materials and Methods
2.1. Study Desgin
For this population-based study, we used data from the Cancer Barometer conducted in France in 2010 and 2015. This national survey, using computer-assisted telephone interviews, has investigated perceptions and knowledge related to cancer, cancer prevention and cancer risk factors (alcohol, tobacco, and exposure to ultraviolet radiation) since 2005. The questions are consistent throughout the time period; however, further questions about nutritional factors (diet, physical activity, weight status, and breastfeeding) and cancer risks were added in 2010 and asked again in 2015. The survey was conducted in accordance with the Declaration of Helsinki. The complete methodology of the surveys is presented elsewhere [
41,
42].
2.2. Population and Recruitment Method
The study was proposed to people aged between 15–75 years in the 2010 and 2015 Barometers, living in France, speaking fluent French and who had never had a cancer diagnosis. In the 2015 Barometer, subjects aged between 75 and 85 years were also included to be more representative of the French population [
43]. To be included in the study, participants needed to have access to a landline or mobile phone.
A list of potentially eligible participants was generated using random digit dialing using number prefixes corresponding to the blocks of numbers assigned by the French regulator. When several people used the same phone number, the Kish method [
44] was applied to select the eligible person in the household. This method was used to survey a representative sample of the French population. Before starting recruitment, a pilot study was conducted with 100 and 119 subjects, in 2010 and 2015, respectively, to validate the comprehension of the questionnaire and the participant selection method. The recruitment took place Monday to Saturday from 3 April to 7 August 2010, and from 19 May to 13 October 2015 (with a three-week break in August).
2.3. Procedure
An information letter was first sent to all the potentially eligible participants of the survey. They were then contacted by phone and verbal consent was obtained. When the subject was contacted but was unavailable, an appointment was made. When no one answered the phone, at least 40 attempts were made to carry out a survey (at different times of the day and different days of the week). When subjects were contacted and available, inclusion criteria were verified before asking the closed and multiple-choice questions from the list. Computer-Assisted Telephone Interviewing (CATI) Software was used by the interviewers as a phone assistance device to manage phone calls, appointments and the progression of the survey. The subjects’ responses were anonymous and self-reported. The study was conducted in accordance with French Data Protection Commission (CNIL) guidelines and carried out with assistance from the BVA Group who are accredited to conduct population-based phone surveys.
2.4. Survey
The 2010 and 2015 surveys started with sociodemographic questions and general information-related questions for the participants. The following information was collected: sex, age, city, education level, current or previous employment, and monthly family income in Euros per consumption unit (CU; i.e., one CU is attributed for the first adult in the household, 0.5 for other persons aged 14 or older, and 0.3 for children under 14 years old). In the analysis, three income ranges were considered: €0–1100/CU, €1100–1800/CU, and >€1800/CU. These ranges are based on the minimum wage and national data on individual salaries, representing three social classes: low income, middle income, and high income.
Regarding the links between nutritional factors and cancer risk, three main multiple-choice questions were presented:
- (1)
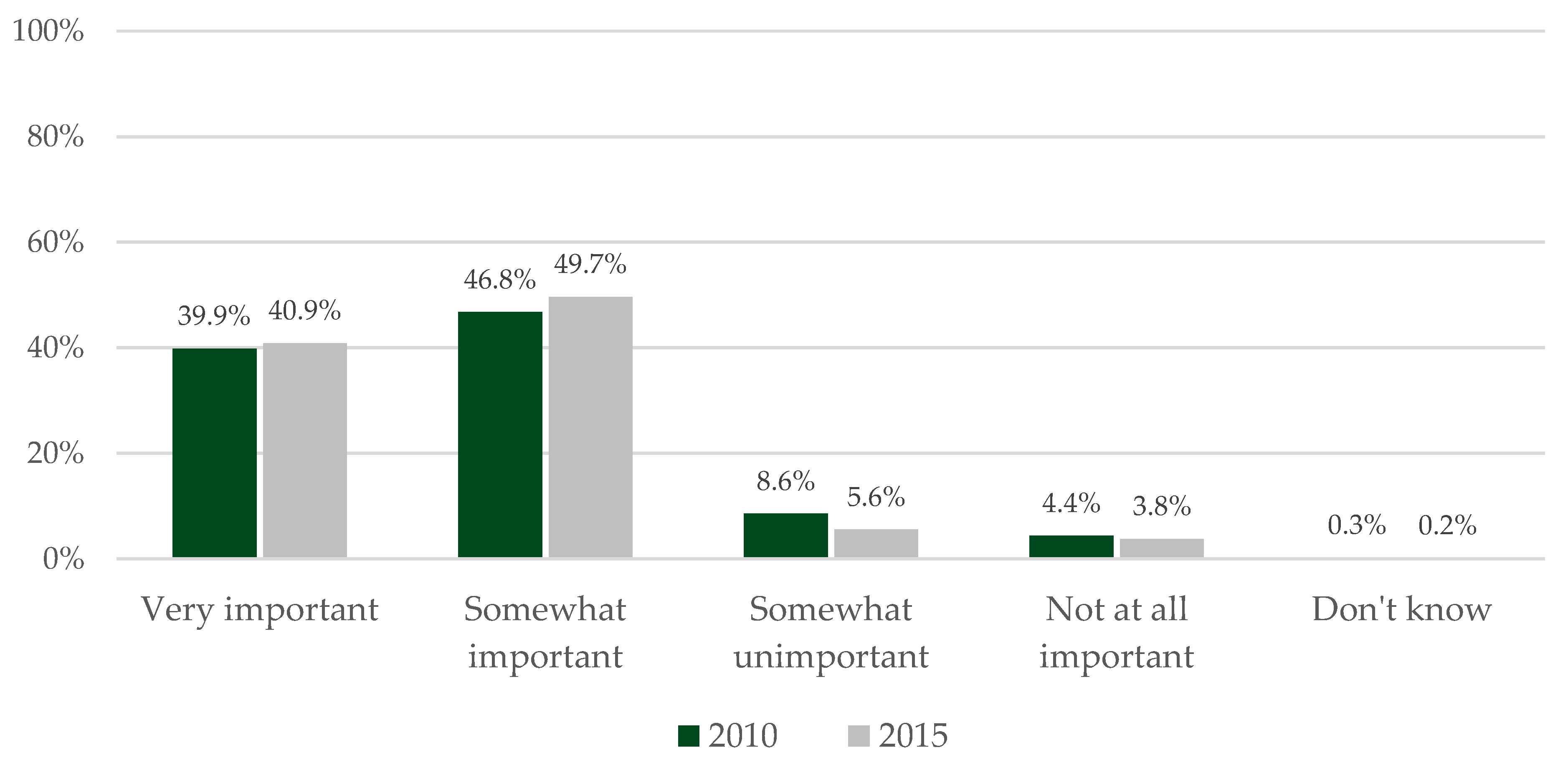
“Do you think that diet has a ‘very important’, ‘somewhat important’, ‘somewhat unimportant’ or ‘not at all important ’role in cancer development?”.
- (2)
“In your opinion: frequent consumption of (‘fruit and vegetables’, ‘red meat’, ‘milk’, ‘cold meats’, ‘white meat’, ‘fish’, ‘salt and salty foods’, ‘potatoes’): (‘can lower’, ‘can increase’, or ‘has no influence on’) cancer risk. The question was repeated for participants who responded ‘Don’t know’. If they still could not answer, the response ‘Don’t know’ was recorded. In our survey, participants were surveyed on cold meats (i.e., ham, salami, dry sausage, lomo Serrano, etc.) and not on processed meat in general as eating cold meats is of cultural significance in France.
Question (2) was adapted for physical activity, overweight and obesity, and breastfeeding (for women only)—“In your opinion, (‘regular physical activity’, ‘overweight & obesity’, ‘breastfeeding’): (‘can lower’, ‘can increase’, or ‘has no influence on’) cancer risk”.
- (3)
“Do you feel that you are ‘very well, ‘somewhat well’, ‘somewhat poorly’ or ‘very poorly’ informed on the health effects of (‘diet’, ‘physical activity’)?”.
2.5. Statistical Analysis
All statistical analyses were conducted using SAS enterprise guide 7.13. First, descriptive analyses were used to describe the participants’ characteristics and perceptions. Proportions were described as ‘very low’ when under 30%, ‘low’ when between 30% and 40%, ‘moderate’ when between 40% and 60%, ‘high’ when between 60% and 70%, and ‘very high’ when higher than 70%. These cut-offs are based on a Gaussian curve, with a theoretical mean of 50, and standard deviation of 10. Chi-squared tests were performed to study differences in sociodemographic variables associated with participants’ perceptions. Finally, logistic regressions were performed to evaluate the associations between sociodemographic variables and the perception of nutritional factors in cancer risk. A stepwise analysis was performed to define the explanatory variables of each regression model. Variables added to the models were: age, sex, monthly family income, education level, occupation, and perceived levels of information on the effects of diet and physical activity on health.
For Question (1) and (2), the responses ‘very important/well and ‘rather important/well’ were combined, as were the responses ‘somewhat unimportant/poorly’ and ‘not at all important/very badly’, to obtain a clear result on the number of participants perceiving the cancer risks linked to nutritional factors and their level of information (well informed versus poorly informed) or not.
4. Discussion
There is a greater perception of risk factors linked to nutrition, physical activity, overweight and obesity, and breastfeeding in 2015 than in 2010. This finding is encouraging and highlights that French people are more aware of cancer risks. However, the findings should be interpreted with caution in national surveys comparing two different samples (i.e., the participants surveyed in the second survey are not the same as those in the first survey) as this could lead to misinterpretations [
26,
27]. Participants surveyed in 2015 had stronger opinions (i.e., less use of the response “Don’t know”) and had a greater perception of the impact of diet (essentially for salt and salty foods, red meat and cold meats), physical activity, and overweight/obesity on cancer risk. However, there was a greater perception of foods for which consumption has a protective effect (i.e., milk and fruit and vegetables) among participants in 2015 than in 2010.
The strengths of the Cancer Barometer lie essentially in two points: (1) a representative sample of the French population is surveyed, and (2) a review is conducted every five years. The findings of this study are thus generalizable to the French population and can be used to adapt cancer prevention programs by improving community-wide interventions. Regarding the exploration of cancer risks attributed to nutritional factors, this is also one of the first studies investigating public awareness on this subject in such detail.
Physical activity, weight status, and diet are perceived by the majority of the participants as having an important role in cancer development. However, when we look at each food group known to be associated with cancer risk [
4], the awareness of participants differed. Participants had a good perception of the role of cold meats (increasing risk), according to other findings of the Cancer Barometer [
45], but to a lesser extent than those for fruit and vegetables, and salt and salty foods (lowering and increasing risk, respectively). There was little perception of milk consumption as increasing cancer risk. There is a greater perception of cold meat consumption as a cancer risk factor as it is also associated with an increase in other diseases (e.g., diabetes, cardiovascular diseases) [
46,
47,
48]. For fruit and vegetables and salt and salty food, links with cancer risk were not well identified by participants, whereas these food groups are recognized by individuals as good and bad for health, respectively [
49,
50,
51]. In 2007 [
52], the influence of milk on the development of cancer was not known, while in 2018 [
4], milk consumption was highlighted as lowering cancer risk. A potential explanation of people’s perceptions might be that French prevention campaigns have broadcast messages to encourage or limit the consumption of certain foods but have not mentioned the rationale regarding cancer prevention. It could be of interest for future research to investigate why such differences are observed between food groups and whether raising the perception of the links between food consumption and cancer might encourage people to change their food habits.
Breastfeeding is ultimately the nutritional factor with the lowest perception as lowering cancer risk. This could be due to a lack of communication in France about the benefits of breastfeeding for women. Breastfeeding is beneficial for the baby (e.g., helps the baby fight off viruses and bacteria), but it also lower women’s cancer risk, risk of osteoporosis, and can be helpful for post-childbirth recovery (e.g., to reduce uterine bleeding) [
53]. However, the many health benefits for breastfeeding women seem to be unknown to women [
54,
55,
56]. In addition to a lack of knowledge, breastfeeding is associated with the fear linked with this behavior, demographic factors, social norms, employment, lactation problems, and culture [
57,
58,
59]. In France, women breastfeed their child 17 weeks on average [
60], which is less than the international guidelines of 6 months [
4]. This finding underlines the need to better understand individuals’ perceptions about breastfeeding in France and to develop national prevention campaigns. Qualitative studies investigating women’s perceptions of the health benefits represented by breastfeeding for both women and their babies need to be conducted first. To our knowledge, studies essentially focus on women’s knowledge of breastfeeding benefits for babies rather than for women.
Perception of the impact of nutritional factors on the onset of cancer is linked with sociodemographic characteristics. In our study, sex, age, education, occupation, and monthly income were frequently associated with participants’ perceptions. For example, there was a lower perception of the benefits of physical activity and the risks of overweight and obesity among participants over 24 years of age, less educated people, and those with low incomes. In France, as in many other countries, the prevalence of overweight and obesity has remained higher among the least educated [
61]. It appears that those most affected have a lower perception of the risks that their condition can represent. Thus, it is necessary to continue to provide information on the health benefits of physical activity and the risks represented by overweight/obesity, in particular by indicating the health risks. However, individuals perceptions are not necessarily in keeping with their behavior. Different variables are likely to influence behavioral change in individuals (e.g., level of knowledge, attitudes, influence of the information provider) [
62,
63,
64,
65]. Several theories and models have been proposed to help design prevention interventions targeting behavioral change [
62,
63,
64,
66,
67] and can be used to design new interventions. It seems of interest to conduct national and longitudinal studies to highlight potential barriers to behavioral change [
26,
27].
The first report on ‘Food, nutrition and the prevention of cancer’ was published in 1997 by the WCRF and AICR. This report was subsequently updated in 2007 and in 2018 [
4]. The importance of providing national prevention campaigns on this subject appeared after 2007 in France [
67], following the publication of the WCRF and AICR reports [
4]. National public health policies are different and, thus, we can assume that national campaigns on nutrition and cancer appeared at different times worldwide. Surveys highlighting peoples’ attitudes, knowledge, and/or perceptions should be conducted in each country to develop prevention campaigns adapted to the population. To date, few countries have conducted health surveys or cancer barometers to study populations’ attitudes, knowledge and/or perceptions about cancer risk factors. We found seven studies conducted in Belgium, Ireland, Japan, Oman, Spain, the United Kingdom, and the United States [
35,
36,
37,
38,
39,
40,
68]. Cancer risk attributed to nutritional factors is not explored extensively in these studies. For example, in Spain, in 2012, 27% and 54% of the respondents respectively perceived weight status and diet as important risk factors in cancer [
38]. In the United States, a national opinion survey conducted in 2017 highlighted that only 31% and 28% of respondents perceived obesity and food choices as cancer risk factors [
36]. In comparison to these two national studies, respondents to the French Cancer Barometer, both in 2010 and 2015, appear to be more aware of the impact of nutritional factors on the onset of cancer. However, the investigation of these risk factors remains relatively recent.
International nutritional guidelines for cancer prevention exist [
69] and are consistent with guidelines aimed at the prevention of other chronic diseases [
70,
71]. However, nutritional guidelines for cancer prevention are not clearly integrated into national prevention campaigns. In France, cancer prevention campaigns have, in the past, had a strong or more frequent focus on tobacco, as this is the main factor associated with cancer development [
23]. Prevention campaigns concerning nutrition are more focused on the benefits for overall health. These French Barometers highlight the need for national prevention campaigns on the impact of nutritional factors on the onset of cancer to be developed. Following the Cancer Barometer study conducted in 2010 and 2015, national campaigns focusing on nutrition and alcohol were implemented for the first time. Information on cancer is provided on the
French National Cancer Institute website (
www.e-cancer.fr) and updated as needed. Information on nutritional factors, alcohol and tobacco, and cancer risks has also been provided through posters, print media, television and radio each year. For example, in 2016, posters were displayed in pharmacies to raise people’s awareness. In 2019, television commercials were broadcast. Furthermore, the survey’s findings have been made available to French public health agencies such as the
French National Authority for Health. Unfortunately, we have had no feedback on how public health agencies have used the findings. In the future, we should establish a method to evaluate how useful the findings of the Cancer Barometer are and how they are used by public health agencies.
Due to the importance of demographic factors on individuals’ perceptions, community-wide and health education interventions can be designed to increase knowledge and awareness of those less aware of the cancer risk associated with diet. Proof-of-concept and feasibility studies [
72], using qualitative study designs, could be used to develop adapted interventions.
Some limitations need to be pointed out. During the study, a national report on nutrition and cancer risk was published in France [
73]. Participants may have consulted this report, which may have influenced their answers. To limit this bias in future studies, researchers should request the number of days/months/years since respondents last perceived information about nutrition and cancer risk or health. Furthermore, it is not always clear if the Cancer Barometer studies investigated perceptions and/or knowledge, as knowledge can influence beliefs and perceptions. The questions asked in this survey also do not allow us to identify the exact reason for the improvement in French people’s awareness of cancer risk. Nevertheless, the findings help identify factors with a lower perception among the population as increasing or lowering cancer risk. In addition, the question related to breastfeeding was only put to women. Future surveys should also survey men as individuals’ behaviors are influenced by those close to them [
74,
75,
76]. Regarding participant recruitment, one limitation can be pointed out. Participants’ ethnic or religious origins were not recorded. In France, it is not ethically possible to record a person’s ethnic or religious origin. However, culture (including ethnicity and religion) can impact peoples’ perceptions [
77]. Thus, the participants’ culture should be surveyed in future studies when ethics committees allow such questions. Finally, the methodology of the study can be improved for future surveys (2020 and beyond). The findings of the French Cancer Barometer would gain in robustness if participants’ behaviors and levels of confidence in their responses were assessed. This would make it possible to assess whether people’s behaviors are in line with their perceptions or not, and vice versa, to improve cancer prevention programs.

 ,
, 

{kind=link}