Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development



Abstract
1. Becoming Frail: An Upcoming Event
2. Role of Nursing Homes in the Nutritional Status of Residents
3. Dietary Factors Implied in Frailty Development
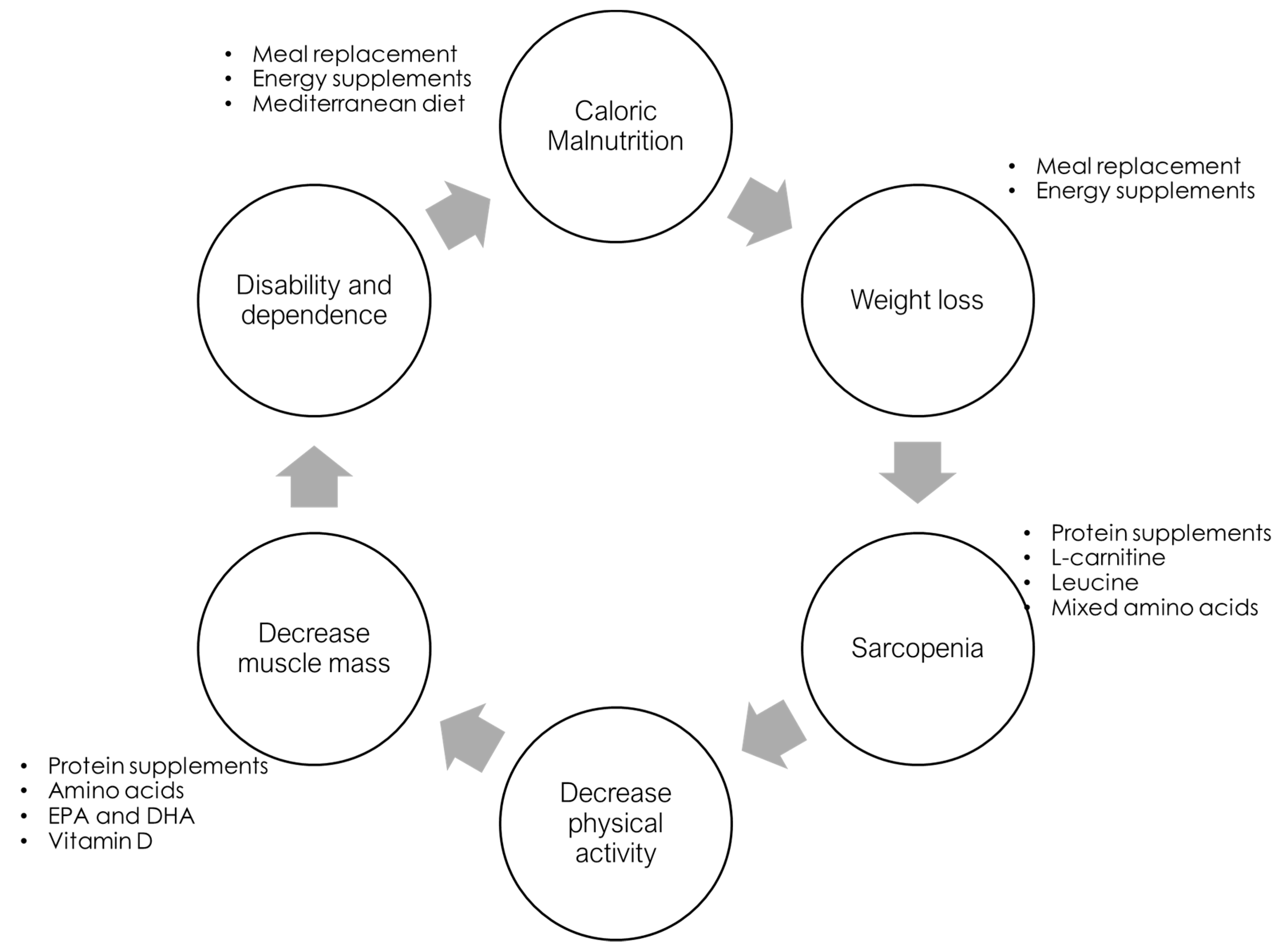
4. Dietary Interventions to Prevent Frailty
4.1. Mediterranean Diet
4.2. Specific Micronutrients
4.2.1. Proteins
4.2.2. Vitamin D
4.2.3. Omega-3
4.2.4. Other Interventions
5. Nondietary Interventions to Prevent Frailty
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tseng, E.; Zhang, A.; Shogbesan, O.; Gudzune, K.A.; Wilson, R.F.; Kharrazi, H.; Cheskin, L.J.; Bass, E.B.; Bennett, W.L. Effectiveness of Policies and Programs to Combat Adult Obesity: A Systematic Review. J. Gen. Intern. Med. 2018, 33, 1990–2001. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Onder, G.; Cesari, M. The geriatric condition of frailty. Eur. J. Intern. Med. 2018, 56, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- King-Kallimanis, B.L.; Kenny, R.A.; Savva, G.M. Factor structure for the frailty syndrome was consistent across Europe. J. Clin. Epidemiol. 2014, 67, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.Y.; Kuha, J.; Murphy, M. Pathways from physical frailty to activity limitation in older people: Identifying moderators and mediators in the English Longitudinal Study of Ageing. Exp. Gerontol. 2017, 98, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Bonaga, B.; Sánchez-Jurado, P.M.; Martínez-Reig, M.; Ariza, G.; Rodríguez-Mañas, L.; Gnjidic, D.; Salvador, T.; Abizanda, P. Frailty, Polypharmacy, and Health Outcomes in Older Adults: The Frailty and Dependence in Albacete Study. J. Am. Med. Dir. Assoc. 2018, 19, 46–52. [Google Scholar] [CrossRef]
- Mohandas, A.; Reifsnyder, J.; Jacobs, M.; Fox, T. Current and Future Directions in Frailty Research. Popul. Health Manag. 2011, 14, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Lopez Casasnovas, G.; Nicodemo, C. Transition and duration in disability: New evidence from administrative data. Disabil. Health J. 2016, 9, 26–36. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Flores Ruano, T.; Martínez-Reig, M.; López-Utiel, M.; Lozoya-Moreno, S.; Dent, E.; Abizanda, P. Socioeconomic Position and Malnutrition Among Older Adults: Results from the FRADEA Study. J. Nutr. Health Aging 2018, 22, 1086–1091. [Google Scholar] [CrossRef]
- Health Quality Ontario Caregiver- and patient-directed interventions for dementia: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2008, 8, 1–98.
- Sieber, C.C. Frailty—From concept to clinical practice. Exp. Gerontol. 2017, 87, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Bernabei, R.; Onder, G.; Marzetti, E. Sarcopenia as the Biological Substrate of Physical Frailty. Clin. Geriatr. Med. 2015, 31, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, S.; Ligthart-Melis, G.C.; Wijers, S.L.J.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. High Prevalence of Physical Frailty Among Community-Dwelling Malnourished Older Adults—A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Abrahamson, K.; Hass, Z.; Arling, G. Shall I Stay or Shall I Go? The Choice to Remain in the Nursing Home Among Residents with High Potential for Discharge. J. Appl. Gerontol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rinnan, E.; André, B.; Drageset, J.; Garåsen, H.; Espnes, G.A.; Haugan, G. Joy of life in nursing homes: A qualitative study of what constitutes the essence of Joy of life in elderly individuals living in Norwegian nursing homes. Scand. J. Caring Sci. 2018. [Google Scholar] [CrossRef] [PubMed]
- Spiers, G.; Matthews, F.E.; Moffatt, S.; Barker, R.O.; Jarvis, H.; Stow, D.; Kingston, A.; Hanratty, B. Impact of social care supply on healthcare utilisation by older adults: A systematic review and meta-analysis. Age Ageing 2018. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Urrea, R.; García-Meseguer, M.J. Relationships between nutritional screening and functional impairment in institutionalized Spanish older people. Maturitas 2014, 78, 323–328. [Google Scholar] [CrossRef]
- Serrano-Urrea, R.; Garcia-Meseguer, M.J. Malnutrition in an Elderly Population without Cognitive Impairment Living in Nursing Homes in Spain: Study of Prevalence Using the Mini Nutritional Assessment Test. Gerontology 2013, 59, 490–498. [Google Scholar] [CrossRef]
- Saghafi-Asl, M.; Vaghef-Mehrabany, E. Comprehensive comparison of malnutrition and its associated factors between nursing home and community dwelling elderly: A case-control study from Northwestern Iran. Clin. Nutr. ESPEN 2017, 21, 51–58. [Google Scholar] [CrossRef]
- Koren-Hakim, T.; Weiss, A.; Hershkovitz, A.; Otzrateni, I.; Anbar, R.; Gross Nevo, R.F.; Schlesinger, A.; Frishman, S.; Salai, M.; Beloosesky, Y. Comparing the adequacy of the MNA-SF, NRS-2002 and MUST nutritional tools in assessing malnutrition in hip fracture operated elderly patients. Clin. Nutr. 2016, 35, 1053–1058. [Google Scholar] [CrossRef]
- Guigoz, Y.; Lauque, S.; Vellas, B.J. Identifying the elderly at risk for malnutrition. The Mini Nutritional Assessment. Clin. Geriatr. Med. 2002, 18, 737–757. [Google Scholar] [CrossRef]
- Törmä, J.; Winblad, U.; Saletti, A.; Cederholm, T. Strategies to implement community guidelines on nutrition and their long-term clinical effects in nursing home residents. J. Nutr. Health Aging 2015, 19, 70–76. [Google Scholar] [CrossRef] [PubMed]
- McConnell, E.S.; Branch, L.G.; Sloane, R.J.; Pieper, C.F. Natural history of change in physical function among long-stay nursing home residents. Nurs. Res. 2003, 52, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; Abellan van Kan, G.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty Consensus: A Call to Action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Bandinelli, S.; Benvenuti, E.; Di Iorio, A.; Macchi, C.; Harris, T.B.; Guralnik, J.M. Subsystems contributing to the decline in ability to walk: Bridging the gap between epidemiology and geriatric practice in the InCHIANTI study. J. Am. Geriatr. Soc. 2000, 48, 1618–1625. [Google Scholar] [CrossRef]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low nutrient intake is an essential component of frailty in older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Lacroix, A.Z.; Neuhouser, M.L.; Huang, Y.; Tinker, L.; Woods, N.; Michael, Y.; Curb, J.D.; Prentice, R.L. Protein intake and incident frailty in the women’s health initiative observational study. J. Am. Geriatr. Soc. 2010, 58, 1063–1071. [Google Scholar] [CrossRef]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; van Loon, L.J.C.; de Groot, L.C.P.G.M. Dietary protein intake in community-dwelling, frail, and institutionalized elderly people: Scope for improvement. Eur. J. Nutr. 2012, 51, 173–179. [Google Scholar] [CrossRef]
- Kobayashi, S.; Asakura, K.; Suga, H.; Sasaki, S.; Three-generation Study of Women on Diets and Health Study Group. High protein intake is associated with low prevalence of frailty among old Japanese women: A multicenter cross-sectional study. Nutr. J. 2013, 12, 164. [Google Scholar] [CrossRef]
- Boxer, R.S.; Dauser, D.A.; Walsh, S.J.; Hager, W.D.; Kenny, A.M. The Association Between Vitamin D and Inflammation with the 6-Minute Walk and Frailty in Patients with Heart Failure. J. Am. Geriatr. Soc. 2008, 56, 454–461. [Google Scholar] [CrossRef]
- Chang, C.-I.; Chan, D.-C. (Derrick); Kuo, K.-N.; Hsiung, C.A.; Chen, C.-Y. Vitamin D insufficiency and frailty syndrome in older adults living in a Northern Taiwan community. Arch. Gerontol. Geriatr. 2010, 50, S17–S21. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Fredman, L.; Hochberg, M.C.; Cauley, J.A.; Hillier, T.A.; Cummings, S.R.; Yaffe, K.; Cawthon, P.M.; Study of Osteoporotic Fractures Research Group. Circulating 25-Hydroxyvitamin D Levels and Frailty Status in Older Women. J. Clin. Endocrinol. Metab. 2010, 95, 5266–5273. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Blackwell, T.L.; Cauley, J.A.; Cummings, S.R.; Barrett-Connor, E.; Dam, T.-T.L.; Hoffman, A.R.; Shikany, J.M.; Lane, N.E.; Stefanick, M.L.; et al. Circulating 25-Hydroxyvitamin D Levels and Frailty in Older Men: The Osteoporotic Fractures in Men Study. J. Am. Geriatr. Soc. 2011, 59, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Michelon, E.; Blaum, C.; Semba, R.D.; Xue, Q.-L.; Ricks, M.O.; Fried, L.P. Vitamin and carotenoid status in older women: Associations with the frailty syndrome. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Bartali, B.; Zhou, J.; Blaum, C.; Ko, C.-W.; Fried, L.P. Low serum micronutrient concentrations predict frailty among older women living in the community. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 594–599. [Google Scholar] [CrossRef]
- Smit, E.; Winters-Stone, K.M.; Loprinzi, P.D.; Tang, A.M.; Crespo, C.J. Lower nutritional status and higher food insufficiency in frail older US adults. Br. J. Nutr. 2013, 110, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Talegawkar, S.A.; Bandinelli, S.; Bandeen-Roche, K.; Chen, P.; Milaneschi, Y.; Tanaka, T.; Semba, R.D.; Guralnik, J.M.; Ferrucci, L. A Higher Adherence to a Mediterranean-Style Diet Is Inversely Associated with the Development of Frailty in Community-Dwelling Elderly Men and Women. J. Nutr. 2012, 142, 2161–2166. [Google Scholar] [CrossRef]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Dietary Quality Is Related to Frailty in Community-Dwelling Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 483–489. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Rahi, B.; Peres, K.; Colpo, M.; Dartigues, J.-F.; Bandinelli, S.; Feart, C.; Rodríguez-Artalejo, F. Consumption of fruit and vegetables and risk of frailty: A dose-response analysis of 3 prospective cohorts of community-dwelling older adults. Am. J. Clin. Nutr. 2016, 104, 132–142. [Google Scholar] [CrossRef]
- Lorenzo-López, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef]
- Jang, I.-Y.; Jung, H.-W.; Park, H.; Lee, C.K.; Yu, S.S.; Lee, Y.S.; Lee, E.; Glynn, R.; Kim, D.H. A multicomponent frailty intervention for socioeconomically vulnerable older adults: A designed-delay study. Clin. Interv. Aging 2018, 13, 1799–1814. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Hsu, F.-C.; Trombetti, A.; King, A.C.; Liu, C.K.; Manini, T.M.; Fielding, R.A.; Pahor, M.; Newman, A.B.; Kritchevsky, S.; et al. Effect of 24-month physical activity on cognitive frailty and the role of inflammation: The LIFE randomized clinical trial. BMC Med. 2018, 16, 185. [Google Scholar] [CrossRef] [PubMed]
- Yarla, N.S.; Polito, A.; Peluso, I. Effects of Olive Oil on TNF-α and IL-6 in Humans: Implication in Obesity and Frailty. Endocr. Metab. Immune Disord. Drug Targets 2017, 18, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-O.; Lee, K.-R. Preventive effect of protein-energy supplementation on the functional decline of frail older adults with low socioeconomic status: A community-based randomized controlled study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Porter Starr, K.N.; Pieper, C.F.; Orenduff, M.C.; McDonald, S.R.; McClure, L.B.; Zhou, R.; Payne, M.E.; Bales, C.W. Improved Function With Enhanced Protein Intake per Meal: A Pilot Study of Weight Reduction in Frail, Obese Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.; Longhurst, G.; Roschel, H.; Gualano, B. Resistance Training and Co-supplementation with Creatine and Protein in Older Subjects with Frailty. J. Frail. Aging 2016, 5, 126–134. [Google Scholar] [CrossRef]
- Fernandes, A.L.; Hayashi, A.P.; Jambassi-Filho, J.C.; de Capitani, M.D.; de Santana, D.A.; Gualano, B.; Roschel, H. Different protein and derivatives supplementation strategies combined with resistance training in pre-frail and frail elderly: Rationale and protocol for the “Pro-Elderly” Study. Nutr. Health 2017, 23, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, S.; Kolobov, A.; Bon, T.; Rafilovich, S.; Munro, H.; Tanner, K.; Pearson, T.; Lees, S.J. Whey Protein Supplementation Improves Rehabilitation Outcomes in Hospitalized Geriatric Patients: A Double Blinded, Randomized Controlled Trial. J. Nutr. Gerontol. Geriatr. 2017, 36, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Dirks, M.L.; Tieland, M.; Verdijk, L.B.; Losen, M.; Nilwik, R.; Mensink, M.; de Groot, L.C.P.G.M.; van Loon, L.J.C. Protein Supplementation Augments Muscle Fiber Hypertrophy but Does Not Modulate Satellite Cell Content During Prolonged Resistance-Type Exercise Training in Frail Elderly. J. Am. Med. Dir. Assoc. 2017, 18, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Vojciechowski, A.S.; Biesek, S.; Melo Filho, J.; Rabito, E.I.; do Amaral, M.P.; Gomes, A.R.S. Effects of physical training with the Nintendo Wii Fit Plus((R)) and protein supplementation on musculoskeletal function and the risk of falls in pre-frail older women: Protocol for a randomized controlled clinical trial (the WiiProtein study). Maturitas 2018, 111, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef]
- Latham, N.K.; Anderson, C.S.; Lee, A.; Bennett, D.A.; Moseley, A.; Cameron, I.D. A randomized, controlled trial of quadriceps resistance exercise and vitamin D in frail older people: The Frailty Interventions Trial in Elderly Subjects (FITNESS). J. Am. Geriatr. Soc. 2003, 51, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Boxer, R.S.; Kenny, A.M.; Schmotzer, B.J.; Vest, M.; Fiutem, J.J.; Pina, I.L. A randomized controlled trial of high dose vitamin D3 in patients with heart failure. JACC. Heart Fail. 2013, 1, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.T.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Leon-Munoz, L.M.; Garcia-Esquinas, E.; Lopez-Garcia, E.; Banegas, J.R.; Rodriguez-Artalejo, F. Major dietary patterns and risk of frailty in older adults: A prospective cohort study. BMC Med. 2015, 13, 11. [Google Scholar] [CrossRef]
- Hutchins-Wiese, H.L.; Kleppinger, A.; Annis, K.; Liva, E.; Lammi-Keefe, C.J.; Durham, H.A.; Kenny, A.M. The impact of supplemental n-3 long chain polyunsaturated fatty acids and dietary antioxidants on physical performance in postmenopausal women. J. Nutr. Health Aging 2013, 17, 76–80. [Google Scholar] [CrossRef]
- Strike, S.C.; Carlisle, A.; Gibson, E.L.; Dyall, S.C. A High Omega-3 Fatty Acid Multinutrient Supplement Benefits Cognition and Mobility in Older Women: A Randomized, Double-blind, Placebo-controlled Pilot Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 236–242. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Abe, S.; Ezaki, O.; Suzuki, M. Medium-Chain Triglycerides in Combination with Leucine and Vitamin D Increase Muscle Strength and Function in Frail Elderly Adults in a Randomized Controlled Trial. J. Nutr. 2016, 146, 1017–1026. [Google Scholar] [CrossRef]
- Badrasawi, M.; Shahar, S.; Zahara, A.M.; Nor Fadilah, R.; Singh, D.K.A. Efficacy of L-carnitine supplementation on frailty status and its biomarkers, nutritional status, and physical and cognitive function among prefrail older adults: A double-blind, randomized, placebo-controlled clinical trial. Clin. Interv. Aging 2016, 11, 1675–1686. [Google Scholar] [CrossRef]
- Wu, S.; Ms, L.H.; Hsu, C.; Hsieh, T.; Ms, S.S.; Ms, Y.P.; Guo, T.; Kang, Y. Dietary education with customised dishware and food supplements can reduce frailty and improve mental well-being in elderly people: A single-blind randomized controlled study. Asia Pac. J. Clin. Nutr. 2018, 27, 1018–1030. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.-C.D.; Tsou, H.-H.; Yang, R.-S.; Tsauo, J.-Y.; Chen, C.-Y.; Hsiung, C.A.; Kuo, K.N. A pilot randomized controlled trial to improve geriatric frailty. BMC Geriatr. 2012, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Manal, B.; Suzana, S.; Singh, D.K.A. Nutrition and Frailty: A Review of Clinical Intervention Studies. J. Frail. Aging 2015, 4, 100–106. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Population and Study Design | Age Range * | Intervention | Outcome Measure | Results |
|---|---|---|---|---|---|
| Kim et al. 2013 [44] | n = 87; Randomised controlled trial. | 79 ± 6 | Two 200-mL liquid formula (400 kcal, 25 g of protein, 9.4 g of essential amino acids, 400 mL of water) per day for 12 weeks | Change of the physical functioning and SPPB | Physical functioning increased by 5.9% in the intervention group |
| Porter Starr et al. 2016 [45] | n = 67; 6-month randomised controlled trial | 68 ± 5 | Regimen with higher protein intake (>30 g) at each meal | Physical function and lean mass | The increase in the protein content was greater than in the control (p = 0.02) |
| Collins et al. 2016 [46] | n = 18; a 14-week, double-blind, randomised, parallel-group, placebo controlled exploratory trial. | 70 ± 5 | Whey protein and creatine co-supplementation or whey protein supplementation | Muscle function and body composition | Both groups were similarly effective in improving muscle function |
| Fernandes et al. 2017 [47] | n = 90 (projected); a double-blind, randomised, placebo-controlled, parallel-group clinical trial | ND | Isolated leucine supplementation (study 1); protein source (whey vs. soy–study 2); combination of whey protein and creatine (study 3) | Muscle cross-sectional area, fibre cross-sectional area, body composition | Not finished yet |
| Niccoli et al. 2017 [48] | n = 47; Randomised clinical trial | 82 ± 2 | An oral dietary product containing 24 g of whey protein per day in addition to their usual diet | Frailty criteria | Whey protein significantly increases grip strength |
| Dirks et al. 2017 [49] | n = 34; Randomised, double-blind, placebo-controlled trial with 2 arms in parallel. | 77 ± 1 | 6-month progressive resistance-type exercise training supplemented with milk protein (2 × 15 g/day) | Type I and type II muscle fibre specific cross-sectional area | Protein supplementation augmented muscle fibre hypertrophy following prolonged resistance-type exercise training in frail older people |
| Vojciechowski et al. 2018 [50] | A randomised controlled clinical trial with a sample of pre-frail older women (n not defined) | ND | Physical training combined with protein supplementation | Strength and power of the lower limbs and body composition | Not finished yet |
| Reference | Population and Study Design | Age Range * | Intervention | Outcome Measure | Results |
|---|---|---|---|---|---|
| Latham et al. 2003 [52] | n = 243; Multicenter, randomized, controlled trial with a factorial design | 79 ± 2 | Single dose of vitamin D (calciferol, 300,000 IU) | Physical health according to the short-form health survey (SPPB) | There was no effect of either intervention on physical health or falls |
| Boxer et al. 2013 [53] | n = 64; Parallel-design, double-blind randomised controlled trial | 66 ± 10 | Weekly Vitamin D3 50,000 IU | The primary outcome was peak oxygen uptake | Vitamin D3 did not improve physical performance |
| Bauer et al. 2015 [54] | n = 380; Multicenter, randomized, controlled, double-blind, 2 parallel-group trial | 77 ± 7 | A vitamin D and leucine-enriched whey protein nutritional supplement | Handgrip strength and SPPB score | Improvements in muscle mass among sarcopenic older adults |
| Hutchins-Wiese et al. 2013 [56] | n = 126; Randomized, double blind pilot study. | 75 ± 6 | 2 fish oil (1.2 g eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA)) or 2 placebo (olive oil) capsules | Frailty assessment | Physical performance was significantly improved by fish oil supplementation |
| Strike et al. 2016 [57] | n = 27; Stratified block randomisation design | ND | 1g DHA, 160 mg eicosapentaenoic acid, 240 mg Ginkgo biloba, 60 mg phosphatidylserine, 20 mg d-α tocopherol, 1mg folic acid, and 20 µg vitamin B12 | Mobility assessed motion capture camera system | Multinutrient supplementation improved mobility in older females |
| Ng et al. 2015 [58] | n = 250; Randomised 5-arms clinical trial | 70 ± 5 | Combined nutritional supplement (iron, folate, vitamin B6, vitamin B12, vitamin D and calcium | Frailty status | Frailty index score was significantly improved in subjects supplemented with the combined nutritional supplement |
| Badrasawi et al. 2016 [60] | n = 50; Randomised, double-blind, placebo-controlled clinical trial | 68 ± 6 | L-carnitine | Frailty status | Frailty index score was significantly improved in subjects supplemented with L-carnitine |
| Wu et al. 2018 [61] | n = 40; 3-month, single-blind, parallel group, randomised controlled trial | 73 ± 2 | Multiple micronutrient supplements, multiple micronutrients plus isolated soy protein supplements and individualised nutrition education | Frailty score | Only individualised nutrition education decreases frailty score |
| Chan et al. 2012 [62] | n = 117; 3-month single site randomised controlled trial | 71 ± 4 | Exercise and nutrition (EN) or problem-solving therapy | Cardiovascular health study phenotypic classification of frailty | EN intervention resulted in short-term frailty status improvement |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández Morante, J.J.; Gómez Martínez, C.; Morillas-Ruiz, J.M. Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development. Nutrients 2019, 11, 102. https://doi.org/10.3390/nu11010102
Hernández Morante JJ, Gómez Martínez C, Morillas-Ruiz JM. Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development. Nutrients. 2019; 11(1):102. https://doi.org/10.3390/nu11010102
Chicago/Turabian StyleHernández Morante, Juan José, Carmelo Gómez Martínez, and Juana María Morillas-Ruiz. 2019. "Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development" Nutrients 11, no. 1: 102. https://doi.org/10.3390/nu11010102
APA StyleHernández Morante, J. J., Gómez Martínez, C., & Morillas-Ruiz, J. M. (2019). Dietary Factors Associated with Frailty in Old Adults: A Review of Nutritional Interventions to Prevent Frailty Development. Nutrients, 11(1), 102. https://doi.org/10.3390/nu11010102