Levels of Growth Factors and IgA in the Colostrum of Women from Burundi and Italy

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
2.3. Colostrum Samples Collection
2.4. Immune Mediators Measurement
2.5. Data Analysis
3. Results
3.1. Study Participants Demographics
3.2. Quantification of Factors in Colostrum Samples
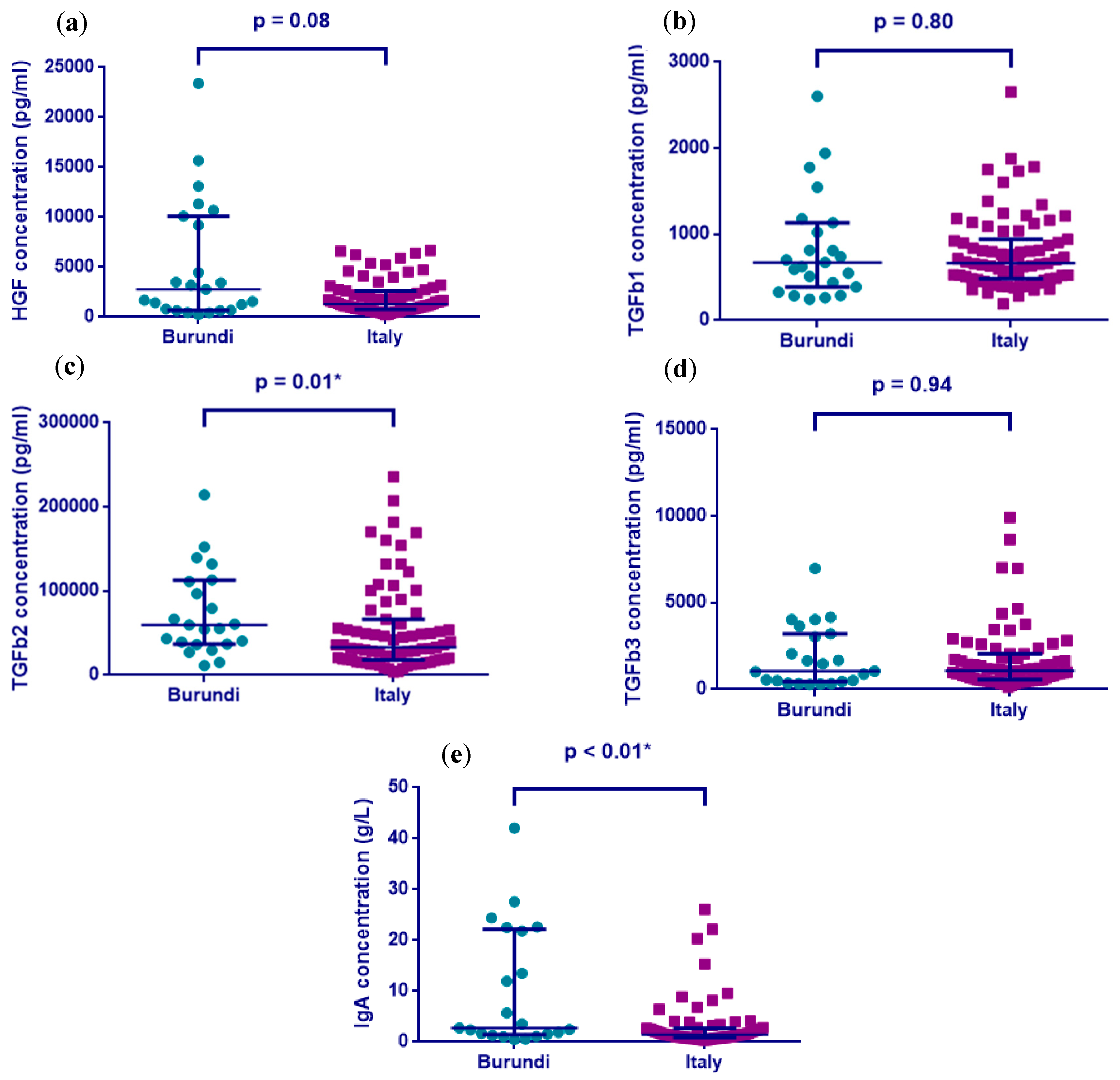
3.2.1. Univariate Analysis Results
3.2.2. Multivariate Analysis Results
3.2.3. Correlation of TGF-β1, 2, and 3 with IgA Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- D’Alessandro, A.; Scaloni, A.; Zolla, L. Human milk proteins: An interactomics and updated functional overview. J. Proteome Res. 2010, 9, 3339–3373. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.M.; Pane, C.A. Human breast milk: Current concepts of immunology and infectious diseases. Curr. Probl. Pediatr. Adolesc. Health Care 2007, 37, 7–36. [Google Scholar] [CrossRef] [PubMed]
- Verhasselt, V. Neonatal tolerance under breastfeeding influence. Curr. Opin. Immunol. 2010, 22, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Verhasselt, V. Allergy prevention by breastfeeding: Possible mechanisms and evidence from human cohorts. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Khodayar-Pardo, P.; Mira-Pascual, L.; Collado, M.C.; Martinez-Costa, C. Impact of lactation stage, gestational age and mode of delivery on breast milk microbiota. J. Perinatol. 2014, 34, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Lodge, C.J.; Tan, D.J.; Lau, M.X.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.J.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Doherty, A.M.; Lodge, C.J.; Dharmage, S.C.; Dai, X.; Bode, L.; Lowe, A.J. Human milk oligosaccharides and associations with immune-mediated disease and infection in childhood: A systematic review. Front. Pediatr. 2018, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Peroni, D.G.; Boix-Amoros, A.; Hsu, P.S.; Land, B.V.; Gay, M.C.L.; Kolotilina, A.; Skevaki, C.; Boyle, R.J.; Collado, M.C.; et al. Human milk and allergic diseases: An unsolved puzzle. Nutrients 2017, 9, 894. [Google Scholar] [CrossRef] [PubMed]
- Kobata, R.; Tsukahara, H.; Ohshima, Y.; Ohta, N.; Tokuriki, S.; Tamura, S.; Mayumi, M. High levels of growth factors in human breast milk. Early Hum. Dev. 2008, 84, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Galimi, F.; Brizzi, M.F.; Comoglio, P.M. The hepatocyte growth factor and its receptor. Stem Cells 1993, 11, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Patki, S.; Patki, U.; Patil, R.; Indumathi, S.; Kaingade, P.; Bulbule, A.; Nikam, A.; Pishte, A. Comparison of the levels of the growth factors in umbilical cord serum and human milk and its clinical significance. Cytokine 2012, 59, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Min, J.K.; Lee, Y.M.; Kim, J.H.; Kim, Y.M.; Kim, S.W.; Lee, S.Y.; Gho, Y.S.; Oh, G.T.; Kwon, Y.G. Hepatocyte growth factor suppresses vascular endothelial growth factor-induced expression of endothelial icam-1 and vcam-1 by inhibiting the nuclear factor-kappab pathway. Circ. Res. 2005, 96, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Cummins, A.G.; Thompson, F.M. Postnatal changes in mucosal immune response: A physiological perspective of breast feeding and weaning. Immunol. Cell Biol. 1997, 75, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Donnet-Hughes, A.; Duc, N.; Serrant, P.; Vidal, K.; Schiffrin, E.J. Bioactive molecules in milk and their role in health and disease: The role of transforming growth factor-beta. Immunol. Cell Biol. 2000, 78, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Penttila, I.A. Milk-derived transforming growth factor-beta and the infant immune response. J. Pediatr. 2010, 156, S21–S25. [Google Scholar] [CrossRef] [PubMed]
- Tiemessen, M.M.; Kunzmann, S.; Schmidt-Weber, C.B.; Garssen, J.; Bruijnzeel-Koomen, C.A.; Knol, E.F.; van Hoffen, E. Transforming growth factor-beta inhibits human antigen-specific CD4+ T cell proliferation without modulating the cytokine response. Int. Immunol. 2003, 15, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Jarvinen, K.M.; Suomalainen, H. Development of cow’s milk allergy in breast-fed infants. Clin. Exp. Allergy 2001, 31, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Rosales, F. A systematic review of the importance of milk TGF-beta on immunological outcomes in the infant and young child. Pediatr. Allergy Immunol. 2010, 21, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Campos-Alberto, E.; Yamaide, F.; Nakano, T.; Ohnisi, H.; Kawamoto, M.; Kawamoto, N.; Matsui, E.; Kondo, N.; Kohno, Y.; et al. TGF-beta concentration in breast milk is associated with the development of eczema in infants. Front. Pediatr. 2018, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Treneva, M.; Peroni, D.G.; Colicino, S.; Chow, L.Y.; Dissanayeke, S.; Pampura, A.; Boner, A.L.; Geddes, D.T.; Boyle, R.J.; et al. Immune components in human milk are associated with early infant immunological health outcomes: A prospective three-country analysis. Nutrients 2017, 9, 532. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, J.; Sasahara, A.; Yoshida, T.; Sira, M.M.; Futatani, T.; Kanegane, H.; Miyawaki, T. Role of transforming growth factor-beta in breast milk for initiation of IgA production in newborn infants. Early Hum. Dev. 2004, 77, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, S.R.; Walker, W.A. Immune factors in breast milk and the development of atopic disease. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Arnould, V.M.; Soyeurt, H. Genetic variability of milk fatty acids. J. Appl. Genet. 2009, 50, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Kondo, N.; Suda, Y.; Nakao, A.; Oh-Oka, K.; Suzuki, K.; Ishimaru, K.; Sato, M.; Tanaka, T.; Nagai, A.; Yamagata, Z. Maternal psychosocial factors determining the concentrations of transforming growth factor-beta in breast milk. Pediatr. Allergy Immunol. 2011, 22, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, M.; Kukkonen, A.K.; Savilahti, E. Impact of maternal allergy and use of probiotics during pregnancy on breast milk cytokines and food antibodies and development of allergy in children until 5 years. Int. Arch. Allergy Immunol. 2012, 159, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Treneva, M.; Peroni, D.G.; Colicino, S.; Chow, L.; Dissanayeke, S.; Abrol, P.; Sheth, S.; Pampura, A.; Boner, A.L.; et al. Colostrum and mature human milk of women from London, Moscow, and Verona: Determinants of immune composition. Nutrients 2016, 8, 695. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, U.; Amoudruz, P.; Johansson, M.A.; Haileselassie, Y.; Ongoiba, A.; Kayentao, K.; Traore, B.; Doumbo, S.; Schollin, J.; Doumbo, O.; et al. Maternal country of origin, breast milk characteristics and potential influences on immunity in offspring. Clin. Exp. Immunol. 2010, 162, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Aihara, Y.; Oh-oka, K.; Kondo, N.; Sharma, J.; Ishimaru, K.; Hara, M.; Yamagata, Z.; Nakao, A. Comparison of colostrum TGF-β2 levels between lactating women in Japan and Nepal. Asian Pac. J. Allergy Immunol. 2014, 32, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, L.; Espinosa-Martos, I.; Garcia-Carral, C.; Manzano, S.; McGuire, M.K.; Meehan, C.L.; McGuire, M.A.; Williams, J.E.; Foster, J.; Sellen, D.W.; et al. What’s normal? Immune profiling of human milk from healthy women living in different geographical and socioeconomic settings. Front. Immunol. 2017, 8, 696. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Country Statistics-Burundi. 2013. Available online: https://www.unicef.org/infobycountry/burundi_statistics.html (accessed on 17 April 2014).
- UNICEF. Unicef-Italy Population Statistics. 2013. Available online: https://www.unicef.org/infobycountry/italy_statistics.html (accessed on 5 April 2014).
- Munblit, D.; Boyle, R.J.; Warner, J.O. Factors affecting breast milk composition and potential consequences for development of the allergic phenotype. Clin. Exp. Allergy 2015, 45, 583–601. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Boyle, R.J. Modulating breast milk composition-the key to allergy prevention? Int. Arch. Allergy Immunol. 2012, 159, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Le Doare, K.; Bellis, K.; Faal, A.; Birt, J.; Munblit, D.; Humphries, H.; Taylor, S.; Warburton, F.; Heath, P.T.; Kampmann, B.; et al. SIgA, TGF-β1, IL-10, and TNFα in colostrum are associated with infant group B streptococcus colonization. Front. Immunol. 2017, 8, 1269. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Sheth, S.; Abrol, P.; Treneva, M.; Peroni, D.G.; Chow, L.Y.; Boner, A.L.; Pampura, A.; Warner, J.O.; Boyle, R.J. Exposures influencing total IgA level in colostrum. J. Dev. Orig. Health Dis. 2016, 7, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Ismail, I.H.; Licciardi, P.V.; Oppedisano, F.; Boyle, R.J.; Tang, M.L. Relationship between breast milk scd14, TGF-beta1 and total IgA in the first month and development of eczema during infancy. Pediatr. Allergy Immunol. 2013, 24, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Amoudruz, P.; Holmlund, U.; Schollin, J.; Sverremark-Ekström, E.; Montgomery, S.M. Maternal country of birth and previous pregnancies are associated with breast milk characteristics. Pediatr. Allergy Immunol. 2009, 20, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Peroni, D.G.; Pescollderungg, L.; Piacentini, G.L.; Rigotti, E.; Maselli, M.; Watschinger, K.; Piazza, M.; Pigozzi, R.; Boner, A.L. Immune regulatory cytokines in the milk of lactating women from farming and urban environments. Pediatr. Allergy Immunol. 2010, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Tomicic, S.; Johansson, G.; Voor, T.; Bjorksten, B.; Bottcher, M.F.; Jenmalm, M.C. Breast milk cytokine and iga composition differ in estonian and swedish mothers-relationship to microbial pressure and infant allergy. Pediatr. Res. 2010, 68, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Jenmalm, M.C. Childhood immune maturation and allergy development: Regulation by maternal immunity and microbial exposure. Am. J. Reprod. Immunol. 2011, 66, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Chatterton, D.E.; Nguyen, D.N.; Bering, S.B.; Sangild, P.T. Anti-inflammatory mechanisms of bioactive milk proteins in the intestine of newborns. Int. J. Biochem. Cell Biol. 2013, 45, 1730–1747. [Google Scholar] [CrossRef] [PubMed]
- Rogier, E.W.; Frantz, A.L.; Bruno, M.E.; Wedlund, L.; Cohen, D.A.; Stromberg, A.J.; Kaetzel, C.S. Secretory antibodies in breast milk promote long-term intestinal homeostasis by regulating the gut microbiota and host gene expression. Proc. Natl. Acad. Sci. USA 2014, 111, 3074–3079. [Google Scholar] [CrossRef] [PubMed]
- Trend, S.; Strunk, T.; Lloyd, M.L.; Kok, C.H.; Metcalfe, J.; Geddes, D.T.; Lai, C.T.; Richmond, P.; Doherty, D.A.; Simmer, K.; et al. Levels of innate immune factors in preterm and term mothers’ breast milk during the 1st month postpartum. Br. J. Nutr. 2016, 115, 1178–1193. [Google Scholar] [CrossRef] [PubMed]
- Umetsu, D.T. Early exposure to germs and the hygiene hypothesis. Cell Res. 2012, 22, 1210–1211. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hawkes, J.S.; Bryan, D.L.; Gibson, R.A. Variations in transforming growth factor beta in human milk are not related to levels in plasma. Cytokine 2002, 17, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Reed, J.R.; Schwertfeger, K.L. Immune cell location and function during post-natal mammary gland development. J. Mammary Gland Biol. Neoplasia 2010, 15, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Bottcher, M.F.; Jenmalm, M.C.; Garofalo, R.P.; Bjorksten, B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr. Res. 2000, 47, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Stavnezer, J. Regulation of antibody production and class switching by TGF-beta. J. Immunol. 1995, 155, 1647–1651. [Google Scholar] [PubMed]
- Ehrhardt, R.O.; Strober, W.; Harriman, G.R. Effect of transforming growth factor (TGF)-beta 1 on IgA isotype expression. TGF-beta 1 induces a small increase in sIgA+ B cells regardless of the method of B cell activation. J. Immunol. 1992, 148, 3830–3836. [Google Scholar] [PubMed]
- Sonoda, E.; Hitoshi, Y.; Yamaguchi, N.; Ishii, T.; Tominaga, A.; Araki, S.; Takatsu, K. Differential regulation of IgA production by TGF-β and IL-5: TGF-β induces surface IgA -positive cells bearing IL -5 receptor, whereas IL-5 promotes their survival and maturation into IgA-secreting cells. Cell. Immunol. 1992, 140, 158–172. [Google Scholar] [CrossRef]
- Jain, S.K.; Baggerman, E.W.; Mohankumar, K.; Namachivayam, K.; Jagadeeswaran, R.; Reyes, V.E.; Maheshwari, A. Amniotic fluid-borne hepatocyte growth factor protects rat pups against experimental necrotizing enterocolitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 306, G361–G369. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Verhasselt, V.; Milcent, V.; Cazareth, J.; Kanda, A.; Fleury, S.; Dombrowicz, D.; Glaichenhaus, N.; Julia, V. Breast milk-mediated transfer of an antigen induces tolerance and protection from allergic asthma. Nat. Med. 2008, 14, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Shahid, N.S.; Steinhoff, M.C.; Roy, E.; Begum, T.; Thompson, C.M.; Siber, G.R. Placental and breast transfer of antibodies after maternal immunization with polysaccharide meningococcal vaccine: A randomized, controlled evaluation. Vaccine 2002, 20, 2404–2409. [Google Scholar] [CrossRef]
- Orivuori, L.; Loss, G.; Roduit, C.; Dalphin, J.C.; Depner, M.; Genuneit, J.; Lauener, R.; Pekkanen, J.; Pfefferle, P.; Riedler, J.; et al. Soluble immunoglobulin a in breast milk is inversely associated with atopic dermatitis at early age: The pasture cohort study. Clin. Exp. Allergy 2014, 44, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Battersby, C.; Santhalingam, T.; Costeloe, K.; Modi, N. Incidence of neonatal necrotising enterocolitis in high-income countries: A systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F182–F189. [Google Scholar] [PubMed]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6, CD002971. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.A. Storage of human milk and the influence of procedures on immunological components of human milk. Acta. Paediatr. Suppl. 1999, 88, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.A. Milk banking: The influence of storage procedures and subsequent processing on immunologic components of human milk. Adv. Nutr. Res. 2001, 10, 389–404. [Google Scholar] [PubMed]


{kind=link}
| Characteristics | Burundi | Italy | p-Value |
|---|---|---|---|
| Maternal age (years), mean (SD) 1 | 24.30 (5.57) | 37.39 (5.38) | <0.01 |
| Birth weight (grams), mean (SD) 1 | 2831 (746.8) | 3328 (476.9) | <0.01 |
| Gestational age (weeks), mean (SD) 1 | 36.48 (1.12) | 39.36 (1/34) | <0.01 |
| Gender (male), n (%) 2 | 15/25 (60) | 41/76 (54) | 0.60 |
| Mode of delivery (c-section), n (%) 3 | 7/21 (33) | 14/76 (18) | 0.14 |
| Parity, mean (SD) 4 | 2.04 (1.15) | 0.81 (0.80) | <0.01 |
| Maternal smoking, n (%) 5 | 2/23 (9) | 3/76 (4) | 0.33 |
| Antenatal infections 6 | 6/23 (26) | 29/76 (38) | 0.29 |
| Regular animal contact 6 | 10/23 (43) | 27/76 (36) | 0.49 |
| Time of colostrum collection (hours), mean (SD) 1 | 58.29 (26.4) | 51.13 (32.61) | 0.28 |
| Immune Factor | Burundi Median (IQR) | Italy Median (IQR) | Unadjusted p-Values 1 | Adjusted Analysis 2 | |
|---|---|---|---|---|---|
| Most Important Factor 3 | p-Value | ||||
| HGF (pg/mL) | 2785 (697.4–10,107) | 1316 (785–2628) | 0.08 | Country of residence | <0.01 |
| TGFβ1 (pg/mL) | 673.1 (387.5–1133) | 663 (483.1–940.4) | 0.80 | Parity | 0.13 |
| TGFβ2 (pg/mL) | 59,708 (36,865–113,221) | 33,176 (18,046–66,520) | 0.01 | Country of residence | 0.03 |
| TGFβ3 (pg/mL) | 1056 (456.5–3212) | 1066 (566.3–2038) | 0.94 | Parity | 0.11 |
| IgA (g/L) | 2.78 (1.45–22.2) | 1.48 (0.89–2.67) | <0.01 | Country of residence | <0.01 |
| Correlating Factors | Burundi (r 1) | Italy (r) |
|---|---|---|
| HGF/IgA | 0.71 ** | 0.38 ** |
| TGF-β1/IgA | 0.52 * | 0.28 * |
| TGF-β2/IgA | 0.68 ** | 0.32 ** |
| TGF-β3/IgA | 0.72 ** | 0.51 ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munblit, D.; Abrol, P.; Sheth, S.; Chow, L.Y.; Khaleva, E.; Asmanov, A.; Lauriola, S.; Padovani, E.M.; Comberiati, P.; Boner, A.L.; et al. Levels of Growth Factors and IgA in the Colostrum of Women from Burundi and Italy. Nutrients 2018, 10, 1216. https://doi.org/10.3390/nu10091216
Munblit D, Abrol P, Sheth S, Chow LY, Khaleva E, Asmanov A, Lauriola S, Padovani EM, Comberiati P, Boner AL, et al. Levels of Growth Factors and IgA in the Colostrum of Women from Burundi and Italy. Nutrients. 2018; 10(9):1216. https://doi.org/10.3390/nu10091216
Chicago/Turabian StyleMunblit, Daniel, Priya Abrol, Shreya Sheth, Li Yan Chow, Ekaterina Khaleva, Alan Asmanov, Silvana Lauriola, Ezio M. Padovani, Pasquale Comberiati, Attilio L. Boner, and et al. 2018. "Levels of Growth Factors and IgA in the Colostrum of Women from Burundi and Italy" Nutrients 10, no. 9: 1216. https://doi.org/10.3390/nu10091216
APA StyleMunblit, D., Abrol, P., Sheth, S., Chow, L. Y., Khaleva, E., Asmanov, A., Lauriola, S., Padovani, E. M., Comberiati, P., Boner, A. L., Warner, J. O., Boyle, R. J., & Peroni, D. G. (2018). Levels of Growth Factors and IgA in the Colostrum of Women from Burundi and Italy. Nutrients, 10(9), 1216. https://doi.org/10.3390/nu10091216