Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study



 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Dietary Assessment
2.3.1. Chinese Healthy Eating Index
2.3.2. Healthy Eating Index-2015
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
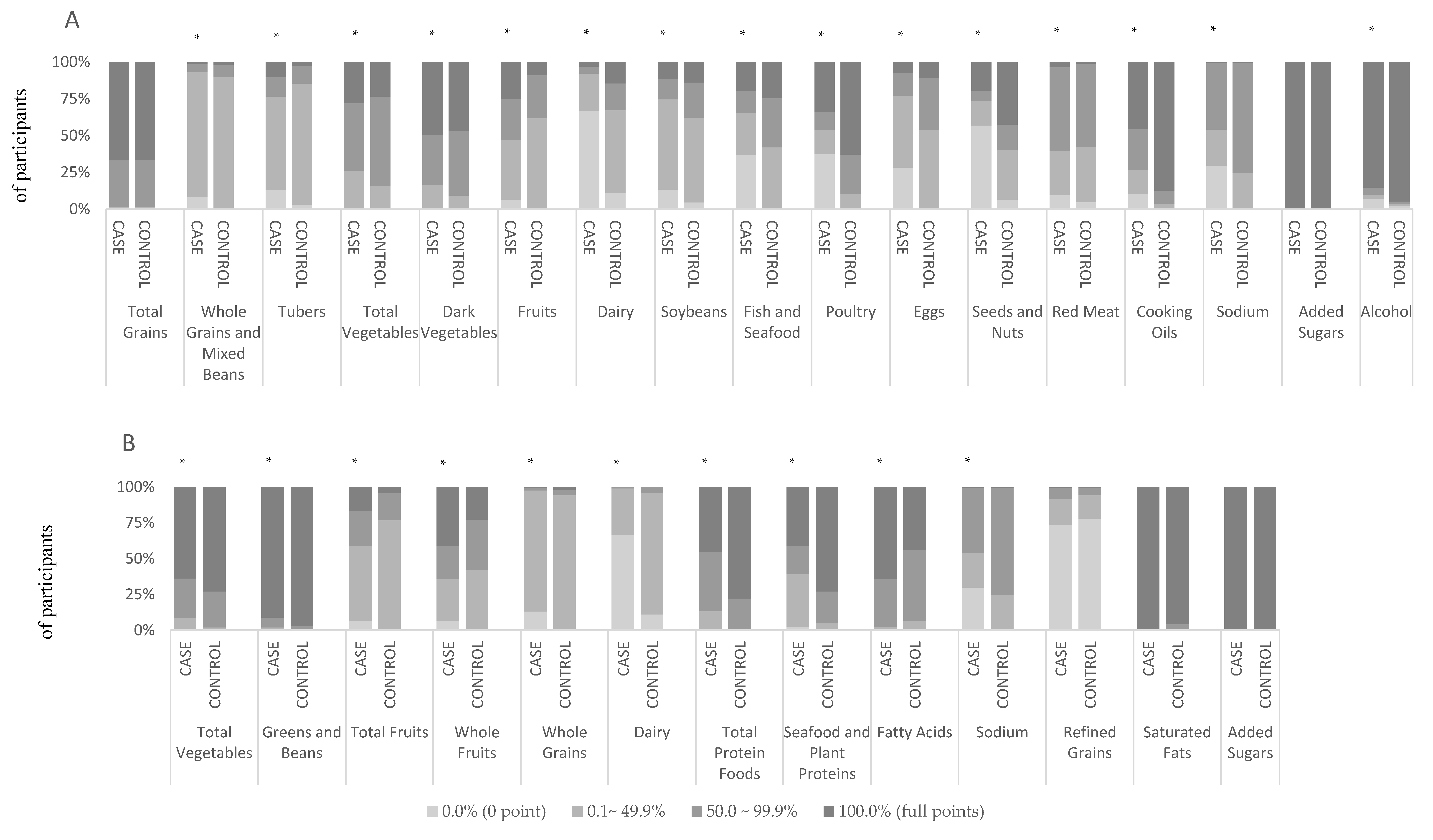
3.2. Percentage Distribution of the Participants for Each Component
3.3. Association of CHEI and HEI-2015 with Primary Liver Cancer Risk
3.4. Association of Components in CHEI and HEI-2015 with Primary Liver Cancer Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions:
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Rudolph, K.L. Hepatocellular carcinoma: Epidemiology and molecular carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef] [PubMed]
- Bamia, C.; Lagiou, P.; Jenab, M.; Aleksandrova, K.; Fedirko, V.; Trichopoulos, D.; Overvad, K.; Tjonneland, A.; Olsen, A.; Clavel-Chapelon, F.; et al. Fruit and vegetable consumption in relation to hepatocellular carcinoma in a multi-centre, European cohort study. Br. J. Cancer 2015, 112, 1273–1282. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Inoue, M.; Iwasaki, M.; Sasazuki, S.; Shimazu, T.; Yamaji, T.; Takachi, R.; Tanaka, Y.; Takachi, R.; Tanaka, Y.; et al. Consumption of n-3 fatty acids and fish reduces risk of hepatocellular carcinoma. Gastroenterology 2012, 142, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Talamini, R.; Polesel, J.; Montella, M.; Dal Maso, L.; Crispo, A.; Tommasi, L.G.; Izzo, F.; Crovatto, M.; La Vecchia, C.; Franceschi, S. Food groups and risk of hepatocellular carcinoma: A multicenter case-control study in Italy. Int. J. Cancer 2006, 119, 2916–2921. [Google Scholar] [CrossRef] [PubMed]
- Sharp, G.B.; Lagarde, F.; Mizuno, T.; Sauvaget, C.; Fukuhara, T.; Allen, N.; Suzuki, G.; Tokuoka, S. Relationship of hepatocellular carcinoma to soya food consumption: A cohort-based, case-control study in Japan. Int. J. Cancer 2005, 115, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Cross, A.J.; McGlynn, K.A.; Abnet, C.C.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A.; Everhart, J.E.; Sinha, R. Association of meat and fat intake with liver disease and hepatocellular carcinoma in the NIH-AARP cohort. J. Natl. Cancer Inst. 2010, 102, 1354–1365. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.T.; Playdon, M.C.; Rock, C.L. Diet, nutrition, and cancer: Past, present and future. Nat. Rev. Clin. Oncol. 2016, 13, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulos, D.; Lagiou, P. Dietary patterns and mortality. Br. J. Nutr. 2001, 85, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean Diet and Breast Cancer Risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Yu, M.C.; Tseng, C.C.; Stanczyk, F.Z.; Pike, M.C. Dietary patterns and breast cancer risk in Asian American women. Am. J. Clin. Nutr. 2009, 89, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Boushey, C.J.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L. High-Quality Diets Associate With Reduced Risk of Colorectal Cancer: Analyses of Diet Quality Indexes in the Multiethnic Cohort. Gastroenterology 2017, 153, 386.e2–394.e2. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Reedy, J.; Sampson, J.; Jiao, L.; Hollenbeck, A.R.; Risch, H.; Mayne, S.T.; Stolzenberg-Solomon, R.Z. The Healthy Eating Index 2005 and risk for pancreatic cancer in the NIH-AARP study. J. Natl. Cancer Inst. 2013, 105, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Park, Y.; Wu, J.W.; Ren, J.S.; Goldstein, A.M.; Taylor, P.R.; Hollenbeck, A.R.; Freedman, N.D.; Abnet, C.C. Index-based dietary patterns and risk of esophageal and gastric cancer in a large cohort study. Clin. Gastroenterol. Hepatol. 2013, 11, 1130.e2–1136.e2. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lin, X.L.; Fan, Y.Y.; Liu, Y.T.; Zhang, X.L.; Lu, Y.K.; Xu, C.H.; Chen, Y.M. Diet Quality Scores and Risk of Nasopharyngeal Carcinoma in Chinese Adults: A Case-Control Study. Nutrients 2016, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Trichopoulos, D.; Polesel, J.; Bravi, F.; Rossi, M.; Talamini, R.; Franceschi, S.; Montella, M.; Trichopoulou, A.; La Vecchia, C.; et al. Mediterranean diet and hepatocellular carcinoma. J. Hepatol. 2014, 60, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Park, Y.; McGlynn, K.A.; Hollenbeck, A.R.; Taylor, P.R.; Goldstein, A.M.; Freedman, N.D. Index-based dietary patterns and risk of incident hepatocellular carcinoma and mortality from chronic liver disease in a prospective study. Hepatology 2014, 60, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.Q.; Li, F.; Dong, R.H.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. The Development of a Chinese Healthy Eating Index and Its Application in the General Population. Nutrients 2017, 9, 977. [Google Scholar] [CrossRef] [PubMed]
- 2015–2020 Dietary Guidelines for Americans, 8th Edition ed.U.S. Department of Health and Human Services and U.S. Department of Agriculture. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 17 August 2018).
- Benson, A.B., 3rd; Abrams, T.A.; Ben-Josef, E.; Bloomston, P.M.; Botha, J.F.; Clary, B.M.; Covey, A.; Curley, S.A.; D’Angelica, M.I.; Davila, R.; et al. NCCN clinical practice guidelines in oncology: Hepatobiliary cancers. J. Natl. Compr. Canc. Netw. 2009, 7, 350–391. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.X.; Ho, S.C. Validity and reproducibility of a food frequency Questionnaire among Chinese women in Guangdong province. Asia Pac. J. Clin. Nutr. 2009, 18, 240–250. [Google Scholar] [PubMed]
- Yang, Y.X.; Wang, G.Y.; Pan, X.Q. China Food Composition, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Lynch, K.L.; Moshfegh, A.J. Food Patterns Equivalents Database 2013–2014: Methodology and User Guide. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/fped/FPED_1314.pdf (accessed on 18 May 2017).
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xiang, Y.-B.; Li, H.L.; Yang, G.; Cai, H.; Ji, B.T.; Gao, Y.T.; Zheng, W.; Shu, X.-O. Vegetable-based dietary pattern and liver cancer risk: Results from the Shanghai women’s and men’s health studies. Cancer Sci. 2013, 104, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Wong, V.W.; Chu, W.C.; Wong, G.L.; Li, L.S.; Leung, J.; Chim, A.M.; Yeung, D.K.; Sea, M.M.; Woo, J.; et al. Diet-Quality Scores and Prevalence of Nonalcoholic Fatty Liver Disease: A Population Study Using Proton-Magnetic Resonance Spectroscopy. PLoS One 2015, 10, e0139310. [Google Scholar] [CrossRef] [PubMed]
- Beunza, J.J.; Toledo, E.; Hu, F.B.; Bes-Rastrollo, M.; Serrano-Martinez, M.; Sanchez-Villegas, A.; Martinez, J.A.; Martinez-Gonzalez, M.A. Adherence to the Mediterranean diet, long-term weight change, and incident overweight or obesity: The Seguimiento Universidad de Navarra (SUN) cohort. Am. J. Clin. Nutr. 2010, 92, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- de Koning, L.; Chiuve, S.E.; Fung, T.T.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Diet-quality scores and the risk of type 2 diabetes in men. Diabetes Care 2011, 34, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Marengo, A.; Rosso, C.; Bugianesi, E. Liver Cancer: Connections with Obesity, Fatty Liver, and Cirrhosis. Annu. Rev. Med. 2016, 67, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, D.; Feng, N.; Chen, G.; Liu, J.; Chen, G.; Zhu, Y. Increased intake of vegetables, but not fruit, reduces risk for hepatocellular carcinoma: A meta-analysis. Gastroenterology 2014, 147, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Basaranoglu, M.; Basaranoglu, G.; Bugianesi, E. Carbohydrate intake and nonalcoholic fatty liver disease: Fructose as a weapon of mass destruction. Hepatobiliary Surg. Nutr. 2015, 4, 109–116. [Google Scholar] [PubMed]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M.; Nonalcoholic Steatohepatitis Clinical Research, N. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef] [PubMed]
- Fedirko, V.; Lukanova, A.; Bamia, C.; Trichopolou, A.; Trepo, E.; Nothlings, U.; Schlesinger, S.; Aleksandrova, K.; Boffetta, P.; Tjønneland, A.; et al. Glycemic index, glycemic load, dietary carbohydrate, and dietary fiber intake and risk of liver and biliary tract cancers in Western Europeans. Ann. Oncol. 2013, 24, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Fedirko, V.; Trichopoulou, A.; Gonzalez, C.A.; Bamia, C.; Trepo, E.; Nothlings, U.; Duarte-Salles, T.; Serafini, M.; Bredsdorff, L.; et al. Dietary flavonoid, lignan and antioxidant capacity and risk of hepatocellular carcinoma in the European prospective investigation into cancer and nutrition study. Int. J. Cancer 2013, 133, 2429–2443. [Google Scholar] [CrossRef] [PubMed]
- Glauert, H.P.; Calfee-Mason, K.; Stemm, D.N.; Tharappel, J.C.; Spear, B.T. Dietary antioxidants in the prevention of hepatocarcinogenesis: A review. Mol. Nutr. Food Res. 2010, 54, 875–896. [Google Scholar] [CrossRef] [PubMed]
- Lan, Q.Y.; Zhang, Y.J.; Liao, G.C.; Zhou, R.F.; Zhou, Z.G.; Chen, Y.M.; Zhu, H.L. The Association between Dietary Vitamin A and Carotenes and the Risk of Primary Liver Cancer: A Case-Control Study. Nutrients 2016, 8, 624. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.P.; Dan, Y.Y.; Goh, G.B.; Jin, A.; Wang, R.; Yuan, J.M. Dietary fatty acids and risk of hepatocellular carcinoma in the Singapore Chinese health study. Liver Int. 2016, 36, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Berasain, C.; Castillo, J.; Perugorria, M.J.; Latasa, M.U.; Prieto, J.; Avila, M.A. Inflammation and liver cancer: New molecular links. Ann. NY Acad. Sci. 2009, 1155, 206–221. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; McCullough, M.L.; Newby, P.K.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Zaichenko, L.; Peter, P.; Davis, C.R.; Crowell, J.A.; Mantzoros, C.S. Diet quality is associated with circulating C-reactive protein but not irisin levels in humans. Metabolism 2014, 63, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nothlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Yang, Y.J.; Yang, Y.K.; Oh, S.Y.; Hong, Y.C.; Lee, E.K.; Kwon, O. Diet quality scores and oxidative stress in Korean adults. Eur J. Clin. Nutr. 2011, 65, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Polesel, J.; Zucchetto, A.; Crispo, A.; Montella, M.; Franceschi, S.; Rossi, M.; La Vecchia, C.; Serraino, D. Inflammatory potential of diet and risk for hepatocellular cancer in a case-control study from Italy. Br. J. Nutr. 2016, 115, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Babio, N.; Balanza, R.; Basulto, J.; Bullo, M.; Salas-Salvado, J. Dietary fibre: influence on body weight, glycemic control and plasma cholesterol profile. Nutr. Hosp. 2010, 25, 327–340. [Google Scholar] [PubMed]
- Kew, M.C. Hepatic iron overload and hepatocellular carcinoma. Cancer Lett. 2009, 286, 38–43. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cases (n = 720) | Controls (n = 720) | p-Value | |
|---|---|---|---|
| Age (year) | |||
| Mean | 58.2 ± 8.8 | 58.4 ± 8.1 | 0.718 * |
| Sex, n (%) | |||
| Women | 107 (14.9) | 107 (14.9) | 1.000 + |
| Men | 613 (85.1) | 613 (85.1) | |
| Body mass index (kg/m2) 1 | 22.8 ± 3.2 | 23.7 ± 3.1 | <0.001 * |
| Physical activity (MET-h/d) 1 | 29.3 (25.4, 38.8) | 31.8 (25.6, 48.5) | <0.001 # |
| Marital status, married, n (%) | 701 (97.4) | 676 (93.9) | 0.001 + |
| Education level, n (%) | |||
| Secondary school or below | 382 (53.1) | 214 (29.7) | <0.001 + |
| High school or above | 338 (46.9) | 506 (70.3) | |
| Household monthly income per capita, n (%) | |||
| ≤¥1500 | 110 (15.3) | 207 (28.8) | <0.001 + |
| ¥1501~3000 | 195 (27.1) | 300 (41.7) | |
| ≥¥3001 | 415 (57.6) | 213 (29.6) | |
| Smoker status, n (%) | 412 (56.7) | 356 (49.0) | 0.003 + |
| Never | 307 (42.6) | 380 (52.9) | |
| Former | 98 (13.6) | 65 (9.1) | |
| Current | 315 (43.8) | 273 (38.0) | |
| Alcohol consumption, n (%) | <0.001 + | ||
| No Intake (0 g/day) | 240 (33.3) | 116 (16.1) | |
| Low Intake (1–15 g/day) | 97 (13.5) | 69 (9.6) | |
| High Intake (>15 g/day) | 137 (19.0) | 42 (5.8) | |
| Tea drinking, n (%) | 436 (60.6) | 469 (65.1) | 0.077 |
| History of diabetes, n (%) | 76 (10.6) | 57 (7.9) | 0.212 |
| HBV infection, n (%) 2 | 627 (87.6) | 87 (12.2) | <0.001 + |
| HCC, n (%) | 676 (93.6) | - | |
| CHEI 1 | 51.92 ± 10.31 | 63.95 ± 7.58 | <0.001 * |
| HEI-2015 1 | 56.93 ± 6.68 | 61.43 ± 5.60 | <0.001 * |
| Total Energy (kcal/day) 1,3 | 2021.01 ± 615.52 | 2103.02 ± 662.11 | 0.015 * |
| Crude | Age- and Sex-Adjusted | Multivariable-Adjusted 1 | p-Interaction | ||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| CHEI | |||||||
| Total scores | 0.47 | 0.44, 0.51 | 0.47 | 0.44, 0.51 | 0.43 | 0.38, 0.50 | |
| Sex | . | 0.609 | |||||
| Women | 0.61 | 0.51, 0.73 | 0.61 | 0.51, 0.73 | 0.55 | 0.43, 0.71 | |
| Men | 0.45 | 0.41, 0.49 | 0.48 | 0.41, 0.49 | 0.40 | 0.34, 0.47 | |
| Smokerstatus | 0.810 | ||||||
| Never | 0.51 | 0.45, 0.57 | 0.51 | 0.45, 0.57 | 0.45 | 0.37, 0.55 | |
| Former | 0.45 | 0.34, 0.59 | 0.45 | 0.34, 0.59 | 0.41 | 0.25, 0.67 | |
| Current | 0.42 | 0.37, 0.49 | 0.42 | 0.37, 0.48 | 0.41 | 0.32, 0.51 | |
| Alcohol Consumption | 0.850 | ||||||
| No Intake | 0.48 | 0.44, 0.53 | 0.48 | 0.44, 0.53 | 0.43 | 0.37, 0.50 | |
| Low Intake | 0.43 | 0.33, 0.56 | 0.43 | 0.33, 0.56 | 0.32 | 0.17, 0.58 | |
| High Intake | 0.55 | 0.44, 0.68 | 0.55 | 0.44, 0.68 | 0.37 | 0.21, 0.66 | |
| HBV infection | 0.686 | ||||||
| Yes | 0.45 | 0.38, 0.53 | 0.45 | 0.38, 0.53 | 0.42 | 0.34, 0.51 | |
| No | 0.45 | 0.39, 0.53 | 0.45 | 0.38, 0.53 | 0.46 | 0.37, 0.54 | |
| HCC | - | ||||||
| Yes | 0.47 | 0.44, 0.51 | 0.47 | 0.44, 0.52 | 0.42 | 0.37,0.49 | |
| No | 0.44 | 0.36, 0.54 | 0.45 | 0.36, 0.54 | 0.41 | 0.31, 0.53 | |
| HEI-2015 | |||||||
| Total scores | 0.55 | 0.50, 0.61 | 0.55 | 0.50, 0.60 | 0.47 | 0.40, 0.55 | |
| Sex | 0.583 | ||||||
| Women | 0.65 | 0.53, 0.80 | 0.65 | 0.52, 0.80 | 0.55 | 0.39, 0.76 | |
| Men | 0.53 | 0.47, 0.59 | 0.53 | 0.48, 0.59 | 0.46 | 0.38, 0.55 | |
| Smokerstatus | 0.704 | ||||||
| Never | 0.61 | 0.54,0.70 | 0.61 | 0.53, 0.70 | 0.53 | 0.42, 0.66 | |
| Former | 0.53 | 0.40, 0.72 | 0.53 | 0.39, 0.71 | 0.52 | 0.31, 0.86 | |
| Current | 0.49 | 0.42, 0.58 | 0.49 | 0.42, 0.58 | 0.40 | 0.30, 0.53 | |
| Alcohol consumption | 0.533 | ||||||
| No Intake | 0.58 | 0.52, 0.65 | 0.57 | 0.51, 0.64 | 0.47 | 0.39, 0.56 | |
| Low Intake | 0.42 | 0.30, 0.59 | 0.42 | 0.30, 0.60 | 0.34 | 0.16, 0.71 | |
| High Intake | 0.57 | 0.43, 0.76 | 0.58 | 0.43, 0.77 | 0.55 | 0.33, 0.91 | |
| HBV infection | 0.552 | ||||||
| Yes | 0.49 | 0.40, 0.59 | 0.50 | 0.41, 0.61 | 0.45 | 0.36, 0.57 | |
| No | 0.49 | 0.40, 0.61 | 0.49 | 0.40, 0.61 | 0.51 | 0.41, 0.65 | |
| HCC | - | ||||||
| Yes | 0.56 | 0.51, 0.61 | 0.55 | 0.50, 0.61 | 0.46 | 0.39, 0.55 | |
| No | 0.44 | 0.31, 0.63 | 0.44 | 0.31, 0.63 | 0.44 | 0.32, 0.62 | |
| Maximum Score | Criteria for Maximum Score 1 | Criteria for Minimum Score | OR 2 | 95% CI | |
|---|---|---|---|---|---|
| CHEI | |||||
| Total Grains | 5 | ≥2.5 SP /1000 Kcal | No Total Grains | 1.15 | 0.87, 1.53 |
| Whole Gains and Mixed Beans | 5 | ≥0.6 SP/1000 kcal | No Whole Grains and Mixed Beans | 0.60 | 0.51, 0.70 |
| Tubers | 5 | ≥0.3 SP/1000 kcal | No Tubers | 1.13 | 1.00, 1.28 |
| Total Vegetables | 5 | ≥1.9 SP/1000 kcal | No Vegetables | 0.82 | 0.71, 0.96 |
| Dark Vegetables | 5 | ≥0.9 SP/1000 kcal | No Dark Vegetables | 0.87 | 0.75, 1.01 |
| Fruits | 10 | ≥1.1 SP/1000 kcal | No Fruit | 1.09 | 1.03, 1.15 |
| Dairy | 5 | ≥0.5 SP/1000 kcal | No Dairy | 0.54 | 0.48, 0.61 |
| Soybeans | 5 | ≥0.4 SP/1000 kcal | No Soybeans | 0.86 | 0.78, 0.96 |
| Fish and Seafood | 5 | ≥0.6 SP/1000 kcal | No Fish and Seafood | 0.68 | 0.61, 0.75 |
| Poultry | 5 | ≥0.3 SP/1000 kcal | No Poultry | 0.50 | 0.44, 0.56 |
| Eggs | 5 | ≥0.5 SP/1000 kcal | No Eggs | 0.61 | 0.54, 0.68 |
| Seeds and Nuts | 5 | ≥0.4 SP/1000 kcal | No Seeds and Nuts | 0.64 | 0.59, 0.70 |
| Red Meat | 5 | ≤0.4 SP/1000 kcal | ≥3.5 SP/1000 kcal | 1.00 | 0.88, 1.14 |
| Cooking Oil | 10 | ≤15.6 g/1000 kcal | ≥32.6 g/1000 kcal | 0.71 | 0.65, 0.77 |
| Sodium | 10 | ≤1000 mg/1000 kcal | ≥3608 mg/1000 kcal | 0.69 | 0.64, 0.75 |
| Alcohol | 5 | 25 g (men)/15 g (women) | ≥60 g (men)/40 g (women) | 0.73 | 0.62, 0.85 |
| HEI-2015 | |||||
| Total Fruits | 5 | ≥0.8 cup eq./1000 kcal | No Fruit | 1.25 | 1.11, 1.41 |
| Whole Fruits | 5 | ≥0.4 cup eq./1000 kcal | No Whole Fruit | 1.11 | 1.00, 1.23 |
| Total Vegetables | 5 | ≥1.1 cup eq./1000 kcal | No Vegetables | 0.66 | 0.53, 0.83 |
| Greens and Beans | 5 | ≥0.2 cup eq./1000 kcal | No Dark Green Vegetables or Legumes | 0.59 | 0.41, 0.86 |
| Whole Grains | 10 | ≥1.5 oz eq./1000 kcal | No Whole Grains | 0.66 | 0.59, 0.74 |
| Dairy | 10 | ≥1.3 cup eq./1000 kcal | No Dairy | 0.52 | 0.45, 0.61 |
| Total Protein Foods | 5 | ≥2.5 oz eq./1000 kcal | No Protein Foods | 0.37 | 0.29, 0.47 |
| Seafood and Plant Proteins | 5 | ≥0.8 oz eq./1000 kcal | No Seafood or Plant Proteins | 0.49 | 0.43, 0.57 |
| Refined Grains | 10 | ≤1.8 oz eq./1000 kcal | ≥4.3 oz eq./1000 kcal | 0.98 | 0.89, 1.07 |
| Fatty Acids | 10 | (PUFAs + MUFAs)/SFAs ≥ 2.5 3 | (PUFAs + MUFAs)/SFAs ≤ 1.2 | 1.33 | 1.20, 1.47 |
| Sodium | 10 | ≤1.1g/1000 kcal | ≥2.0g/1000 kcal | 0.69 | 0.64, 0.75 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-Y.; Fang, A.-P.; Wang, X.-Y.; Lan, Q.-Y.; Liao, G.-C.; Liu, Z.-Y.; Zhang, D.-M.; Zhang, Y.-Y.; Chen, Y.-M.; Zhu, H.-L. Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study. Nutrients 2018, 10, 1113. https://doi.org/10.3390/nu10081113
Chen P-Y, Fang A-P, Wang X-Y, Lan Q-Y, Liao G-C, Liu Z-Y, Zhang D-M, Zhang Y-Y, Chen Y-M, Zhu H-L. Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study. Nutrients. 2018; 10(8):1113. https://doi.org/10.3390/nu10081113
Chicago/Turabian StyleChen, Pei-Yan, Ai-Ping Fang, Xiao-Yan Wang, Qiu-Ye Lan, Gong-Cheng Liao, Zhao-Yan Liu, Dao-Ming Zhang, Yao-Yun Zhang, Yu-Ming Chen, and Hui-Lian Zhu. 2018. "Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study" Nutrients 10, no. 8: 1113. https://doi.org/10.3390/nu10081113
APA StyleChen, P.-Y., Fang, A.-P., Wang, X.-Y., Lan, Q.-Y., Liao, G.-C., Liu, Z.-Y., Zhang, D.-M., Zhang, Y.-Y., Chen, Y.-M., & Zhu, H.-L. (2018). Adherence to the Chinese or American Dietary Guidelines is Associated with a Lower Risk of Primary Liver Cancer in China: A Case-Control Study. Nutrients, 10(8), 1113. https://doi.org/10.3390/nu10081113