Dietary Intake and Food Sources of Niacin, Riboflavin, Thiamin and Vitamin B6 in a Representative Sample of the Spanish Population. The ANIBES Study †

 ,
,  ,
,  , , , ,
, , , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Design
2.2. Food Record and Adequacy of Reported Intake
2.3. Evaluation of Misreporting
2.4. Statistical Analysis
3. Results
3.1. Thiamin, Riboflavin, Niacin and Vitamin B6 Reported Intake and Distribution in the Whole Population
3.2. Thiamin, Riboflavin, Niacin and Vitamin B6 Reported Intake in Plausible and Non-Plausible Reporters
3.3. Disparity between Reported Intake and the Level Needed for Adequacy for Thiamin, Riboflavin, Niacin and Vitamin B6 in the Whole Population
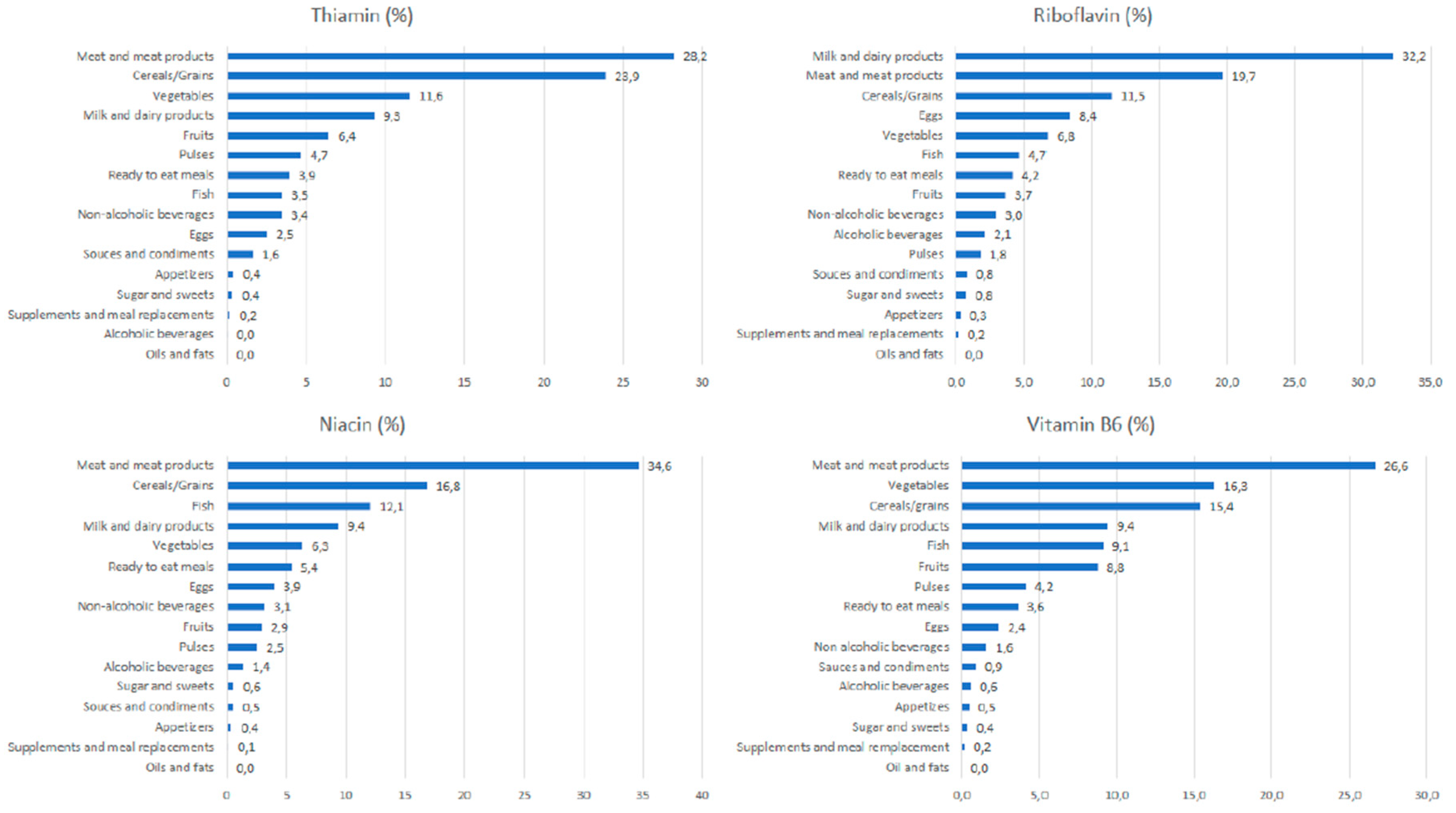
3.4. Contribution of Food Sources to Thiamin, Riboflavin, Niacin and Vitamin B6 Reported Intakes
3.4.1. Thiamin
3.4.2. Riboflavin
3.4.3. Niacin
3.4.4. Vitamin B6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ezzati, M.; Riboli, E. Behavioral and Dietary Risk Factors for Noncommunicable Diseases. N. Engl. J. Med. 2013, 369, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. The B Vitamins and Choline: Overview and Methods; National Academies Press: Washington, DC, USA, 1998. [Google Scholar]
- Ortigoza-Escobar, J.D.; Alfadhel, M.; Molero-Luis, M.; Darin, N.; Spiegel, R.; de Coo, I.F.; Gerards, M.; Taylor, R.W.; Artuch, R.; Nashabat, M.; et al. Thiamine Deficiency in Childhood with Attention to Genetic Causes: Survival and Outcome Predictors. Ann. Neurol. 2017, 82, 317–330. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Dietary Reference Values for Thiamin. EFSA J. 2016, 14, 4653. [Google Scholar]
- Crook, M.A.; Sriram, K. Thiamine Deficiency: The Importance of Recognition and Prompt Management. Nutrition 2014, 30, 953–954. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Lee, M.S.; Wahlqvist, M.L. Prediction of all-Cause Mortality by B Group Vitamin Status in the Elderly. Clin. Nutr. 2012, 31, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy of Sciences: Washington, DC, USA, 1998. [Google Scholar]
- European Food Safety Authority (EFSA). Dietary Reference Values for Riboflavin. EFSA J. 2017, 18, 4919. [Google Scholar]
- Lopez, R.; Schwartz, J.V.; Cooperman, J.M. Riboflavin Deficiency in an Adolescent Population in New York City. Am. J. Clin. Nutr. 1980, 33, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Bogan, K.L.; Brenner, C. Nicotinic Acid, Nicotinamide, and Nicotinamide Riboside: A Molecular Evaluation of NAD+ Precursor Vitamins in Human Nutrition. Annu. Rev. Nutr. 2008, 28, 115–130. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, J.B. Niacin Status, NAD Distribution and ADP-Ribose Metabolism. Curr. Pharm. Des. 2009, 15, 3–11. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Scientific Opinion on Dietary Reference Values for Niacin. EFSA J. 2014, 12, 3759. [Google Scholar]
- Merkiel, S.; Chalcarz, W. Preschool Diets in Children from Pila, Poland, Require Urgent Intervention as Implied by High Risk of Nutrient Inadequacies. J. Health Popul. Nutr. 2016, 35, 11. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Dietary Reference Values for Vitamin B6. EFSA J. 2016, 14, 4487. [Google Scholar]
- Ho, C.L.; Quay, T.A.; Devlin, A.M.; Lamers, Y. Prevalence and Predictors of Low Vitamin B6 Status in Healthy Young Adult Women in Metro Vancouver. Nutrients 2016, 8, 538. [Google Scholar] [CrossRef] [PubMed]
- Gil, A.; Martinez de Victoria, E.; Olza, J. Indicators for the Evaluation of Diet Quality. Nutr. Hosp. 2015, 31 (Suppl. S3), 128–144. [Google Scholar] [PubMed]
- Elmadfa, I.; Meyer, A.L. Developing Suitable Methods of Nutritional Status Assessment: A Continuous Challenge. Adv. Nutr. 2014, 5, 590S–598S. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Guidance on the EU Menu Methodology. EFSA J. 2014, 12, 3944. [Google Scholar]
- Archer, E.; Hand, G.A.; Blair, S.N. Validity of U.S. Nutritional Surveillance:National Health and Nutrition Examination Survey Caloric Energy Intake Data, 1971–2010. PLoS ONE 2013, 8, e76632. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Example of a Protocol for Identification of Misreporting (Under- and Over-Reporting of Energy Intake) Based on the PILOT-PANEU Project; European Food Safety Authority: Parma, Italy, 2017. [Google Scholar]
- Varela Moreiras, G.; Avila, J.M.; Ruiz, E. Energy Balance, a New Paradigm and Methodological Issues: The ANIBES Study in Spain. Nutr. Hosp. 2015, 31 (Suppl. S3), 101–112. [Google Scholar] [PubMed]
- Ruiz, E.; Ávila, J.M.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L. Macronutrient Distribution and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Olza, J.; Aranceta-Bartrina, J.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, A. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Olza, J.; Aranceta-Bartrina, J.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, A. Reported Dietary Intake and Food Sources of Zinc, Selenium, and Vitamins, A., E and C in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 697. [Google Scholar] [CrossRef] [PubMed]
- Samaniego-Vaesken, M.L.; Partearroyo, T.; Olza, J.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Iron Intake and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 203. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Avila, J.M.; Castillo, A.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Bartrina, J.A.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; et al. The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carbajal, Á.; Cabrera Forneiro, L.; Hoyos, C.; Carmen, M. Ingestas Recomendadas de energía y nutrientes para la población española. In Tablas de Composición de Alimentos: Guía de Prácticas, 17th ed.; Departamento de Nutrición, Universidad Complutense de Madrid: Madrid, Spain, 2015; pp. 258–259. [Google Scholar]
- Partearroyo, T.; Samaniego-Vaesken, M.L.; Ruiz, E.; Olza, J.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary Sources and Intakes of Folates and Vitamin B12 in the Spanish Population: Findings from the ANIBES Study. PLoS ONE 2017, 12, e0189230. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting Basal Metabolic Rate, New Standards and Review of Previous Work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. S1), 5–41. [Google Scholar]
- Mielgo-Ayuso, J.; Aparicio-Ugarriza, R.; Castillo, A.; Ruiz, E.; Ávila, J.M.; Aranceta-Batrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Physical Activity Patterns of the Spanish Population are mostly Determined by Sex and Age: Findings in the ANIBES Study. PLoS ONE 2016, 11, e0149969. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.A.; Popkin, B.M.; Buckland, G.; Schroder, H.; Amiano, P.; Barricarte, A.; Huerta, J.; Quirós, J.R.; Sánchez, M.; González, C.A. Alternative Methods of Accounting for Underreporting and Overreporting when Measuring Dietary Intake-Obesity Relations. Am. J. Epidemiol. 2011, 173, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of Energy and Micronutrient Intake Estimated by Food Records and 24 Hour Recalls, Control and Adjustment Methods in Practice. Br. J. Nutr. 2009, 101 (Suppl. S2), S73–S85. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, S.R.; Low, M.; Thompson, J.; Farrell, A.; De-Regil, L.M. Iron Supplementation Benefits Physical Performance in Women of Reproductive Age: A Systematic Review and Meta-Analysis. J. Nutr. 2014, 144, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Garcia-Closas, R.; Ribas, L.; Perez-Rodrigo, C.; Aranceta, J. Food Patterns of Spanish Schoolchildren and Adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Sobaler, A.M.; Aparicio, A.; Gonzalez-Rodriguez, L.G.; Cuadrado-Soto, E.; Rubio, J.; Marcos, V.; Sanchidrian, R.; Santos, S.; Perez-Farinos, N.; Dal Re, M.A.; et al. Adequacy of Usual Vitamin and Mineral Intake in Spanish Children and Adolescents: ENALIA Study. Nutrients 2017, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Encuesta Nacional de Ingesta Dietética Española 2011. Available online: http://203.187.160.133:9011/www.laboratoriolcn.com/c3pr90ntc0td/f/docs/Valoracion_nutricional_ENIDE_micronutrientes.pdf (accessed on 28 June 2018).
- Kersting, M.; Clausen, K. Ernährungsphysiologische Auswertung Einer Repräsentativen Verzehrsstudie Bei Säuglingen und Kleinkindern VELS Mit Dem Instrumentarium der Donald Studie; Forschungsinstitut für Kinderernährung: Dortmund, Germany, 2003. [Google Scholar]
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Swan, G. National Diet and Nutrition Survey. Headline Results from Years 1, 2 and 3 (Combined) of the Rolling Programme (2008/2009–2010/11); Department of Health and the Food Standards Agency: London, UK, 2012. [Google Scholar]
- Mensink, G.; Heseker, H.; Richter, A.; Stahl, A.; Vohmann, C. EsKiMo-the Nutrition Module in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Hoppu, U.; Lehtisalo, J.; Kujala, J.; Keso, T.; Garam, S.; Tapanainen, H.; Uutela, A.; Laatikainen, T.; Rauramo, U.; Pietinen, P. The Diet of Adolescents can be Improved by School Intervention. Public Health Nutr. 2010, 13, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Afssa (Agence Française de Sécurité Sanitaire des Aliments). Etude Individuelle Nationale des Consommations Alimentaires 2 (INCA 2) (2006–2007). Available online: https://www.anses.fr/fr/system/files/PASER-Ra-INCA2.pdf (accessed on 28 June 2018).
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C.; INRAN-SCAI 20052006–Study Group. The Third Italian National Food Consumption Survey, INRAN-SCAI 2005–06–part 1: Nutrient Intakes in Italy. Nutr. Metabol. Cardiovasc. Dis. 2011, 21, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Van Rossum, C.; Fransen, H.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.; Ocké, M. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years. Available online: https://www.rivm.nl/bibliotheek/rapporten/350050006.pdf (accessed on 28 June 2018).
- Helldán, A.; Raulio, S.; Kosola, M.; Tapanainen, H.; Ovaskainen, M.; Virtanen, S. Finravinto 2012-Tutkimus-the National FINDIET 2012 Survey. Available online: https://www.julkari.fi/bitstream/handle/10024/110839/THL_RAP2013_016_%26sliitteet.pdf (accessed on 28 June 2018).
- Amcoff, E.; Edberg, A.; Barbieri, H.; Lindroos, A.; Nälsén, C.; Pearson, M.; Lemming, E. Livsmedels-Och Näringsintag Bland Vuxna i Sverige. Resultat Från Matvaneundersökning Utförd 2010–2011 Dietary Habits and Nutrient Intake in Sweden; Livsmedelsverket: Uppsala, Sweden, 2012. [Google Scholar]
- Varela-Moreiras, G.; Ruiz, E.; Valero, T.; Avila, J.M.; del Pozo, S. The Spanish Diet: An Update. Nutr. Hosp. 2013, 28 (Suppl. S5), 13–20. [Google Scholar] [PubMed]
- Powers, H.J. Riboflavin (Vitamin B-2) and Health. Am. J. Clin. Nutr. 2003, 77, 1352–1360. [Google Scholar] [CrossRef] [PubMed]
- Irish Universities Nutrition Alliance. National Adult Nutrition Survey: Summary Report; Irish Universities Nutrition Alliance: Cork, Ireland, 2011. [Google Scholar]


{kind=link}
| PAL | Misreporting Cut-off | |||
|---|---|---|---|---|
| Group Level | Individual Level | |||
| Lower | Upper | Lower | Upper | |
| Children and adolescents | ||||
| 1.6 | 1.55 | 1.66 | 0.93 | 2.76 |
| 1.8 | 1.73 | 1.86 | 1.04 | 3.10 |
| 2.0 | 1.93 | 2.07 | 1.16 | 3.45 |
| Adults and elderly | ||||
| 1.4 | 1.38 | 1.42 | 0.77 | 2.53 |
| 1.6 | 1.58 | 1.62 | 0.88 | 2.89 |
| 1.8 | 1.77 | 2.83 | 1.00 | 3.25 |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | |
| THIAMIN (mg/day) | |||||||||||||||
| Total | 2009 | 1.17 ± 0.02 | 1.07 (0.30–3.44) | 213 | 1.24 ± 0.03 | 1.20 (0.41–3.32) | 211 | 1.28 ± 0.03 | 1.24 (0.41–3.01) | 1655 | 1.18 ± 0.02 | 1.07 (0.30–3.44) | 206 | 1.06 ± 0.03 | 0.97 (0.40–2.69) |
| Men | 1013 | 1.27 ± 0.04 * | 1.15 (0.33–3.44) | 126 | 1.28 ± 0.04 | 1.22 (0.41–3.32) | 137 | 1.35 ± 0.04 | 1.28 (0.41–3.01) | 798 | 1.29 ± 0.05 * | 1.16 (0.33–3.44) | 99 | 1.41 ± 0.04 | 1.00 (0.42–2.69) |
| Women | 996 | 1.07 ± 0.01 | 1.00 (0.30–2.70) | 87 | 1.18 ± 0.04 | 1.15 (0.41–2.70) | 74 | 1.14 ± 0.04 | 1.17 (0.52–2.31) | 857 | 1.07 ± 0.01 | 1.01 (0.30–2.68) | 107 | 0.98 ± 0.03 | 0.89 (0.40–2.17) |
| RIBOFLAVIN (mg/day) | |||||||||||||||
| Total | 2009 | 1.44 ± 0.02 | 1.34 (0.37–3.54) | 213 | 1.56 ± 0.03 | 1.54 (0.50–3.41) | 211 | 1.51 ± 0.04 | 1.43 (0.53–3.82) | 1655 | 1.44 ± 0.02 | 1.33 (0.40–3.54) | 206 | 1.39 ± 0.04 | 1.32 (0.37–4.71) |
| Men | 1013 | 1.53 ± 0.04 * | 1.40 (0.42–3.54) | 126 | 1.62 ± 0.04 | 1.56 (0.50–3.41) | 137 | 1.63 ± 0.05 * | 1.51 (0.55–3.82) | 798 | 1.54 ± 0.05 * | 1.39 (0.42–3.54) | 99 | 1.47 ± 0.07 | 1.32 (0.61–4.71) |
| Women | 996 | 1.35 ± 0.01 | 1.29 (0.37–3.08) | 87 | 1.49 ± 0.05 | 1.49 (0.53–2.57) | 74 | 1.29 ± 0.04 | 1.27 (0.53–2.04) | 857 | 1.36 ± 0.02 | 1.28 (0.40 + 3.47) | 107 | 1.33 ± 0.05 | 1.32 (0.37–2.99) |
| NIACIN (mg/day) | |||||||||||||||
| Total | 2009 | 29.1 ± 0.2 | 27.9 (6.7–109.0) | 213 | 28.5 ± 0.5 | 27.5 (8.6–58.4) | 211 | 30.2 ± 0.7 | 30.1 (11.7–73.6) | 1655 | 29.4 ± 0.3 | 28.1 (6.6–109.0) | 206 | 26.0 ± 0.6 | 25.0 (9.1–70.3) |
| Men | 1013 | 31.4 ± 0.3 * | 30.2 (9.8–109.0) | 126 | 29.4 ± 0.7 | 28.9 (8.6–58.4) | 137 | 32.4 ± 0.8 * | 32.0 (11.7–73.6) | 798 | 31.9 ± 0.4 * | 30.6 (12.1–109.0) | 99 | 28.0 ± 1.0 * | 26.2 (9.8–70.3) |
| Women | 996 | 26.7 ± 0.3 | 26.1 (6.7–66.1) | 87 | 27.0 ± 0.8 | 26.1 (13.3–50.6) | 74 | 26.1 ± 0.9 | 26.2 (12.4–45.3) | 857 | 27.1 ± 0.3 | 26.4 (6.7–66.1) | 107 | 24.2 ± 07 | 22.6 (9.1–48.2) |
| VITAMIN B6 (mg/day) | |||||||||||||||
| Total | 2009 | 1.54 ± 0.01 | 1.44 (0.28–9.30) | 213 | 1.51 ± 0.03 | 1.51 (0.49–4.29) | 211 | 1.54 ± 0.04 | 1.47 (0.62–3.62) | 1655 | 1.55 ± 0.02 | 1.44 (0.28–9.30) | 206 | 1.56 ± 0.05 | 1.39 (0.62–5.29) |
| Men | 1013 | 1.64 ± 0.02 * | 1.51 (0.44–9.30) | 126 | 1.54 ± 0.04 | 1.54 (0.56–4.29) | 137 | 1.62 ± 0.05 * | 1.57 (0.63–3.62) | 798 | 1.65 ± 0.03 * | 1.49 (0.44–9.30) | 99 | 1.71 ± 0.08 * | 1.51 (0.73–5.29) |
| Women | 996 | 1.45 ± 0.02 | 1.37 (0.28–3.94) | 87 | 1.46 ± 0.06 | 1.46 (0.49–3.28) | 74 | 1.40 ± 0.05 | 1.31 (0.62–2.86) | 857 | 1.46 ± 0.02 | 1.39 (0.28–3.94) | 107 | 1.42 ± 0.05 | 1.29 (0.62–3.61) |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | |
| THIAMIN (mg/day) | |||||||||||||||
| Plausible reporters | 543 | 1.42 ± 0.02 | 1.32 (0.60–4.88) | 120 | 1.37 ± 0.04 | 1.31 (0.63–3.32) | 76 | 1.48 ± 0.05 | 1.43 (060–3.01) | 433 | 1.43 ± 0.03 | 1.32 (0.65–4.88) | 45 | 1.31 ± 0.05 | 1.26 (0.74–2.31) |
| Men | 232 | 1.60 ± 0.03 | 1.50 (0.63–4.88) | 68 | 1.42 ± 0.05 | 1.28 (0.63–3.32) | 48 | 1.60 ± 0.06 | 1.53 (0.93–3.01) | 158 | 1.70 ± 0.05 | 1.59 (0.83–4.88) | 24 | 1.42 ± 0.09 | 1.39 (0.90–2.31) |
| Women | 311 | 1.27 ± 0.02 | 1.23 (0.60–2.70) | 52 | 1.30 ± 0.05 | 1.28 (0.79–2.70) | 28 | 1.27 ± 0.07 | 1.27 (0.60–2.31) | 275 | 1.27 ± 0.02 | 1.21 (0.65–2.61) | 21 | 1.18 ± 0.05 | 1.21 (0.74–1.64) |
| Non-Plausible reporters | 1466 | 1.09 ± 0.02 | 0.99 (0.30–3.44) | 93 | 1.08 ± 0.04 | 1.02 (0.41–2.60) | 135 | 1.16 ± 0.03 | 1.11 (0.41–2.48) | 1222 | 1.09 ± 0.03 | 0.99 (0.33–3.44) | 161 | 0.99 ± 0.03 | 0.89 (0.40–2.69) |
| Men | 781 | 1.18 ± 0.04 | 1.07 (0.33–3.44) | 58 | 1.12 ± 0.06 | 1.01 (0.41–2.60) | 89 | 1.22 ± 0.05 | 1.15 (0.41–2.48) | 640 | 1.19 ± 0.05 | 1.08 (0.3–3.4) | 75 | 1.05 ± 0.05 | 0.97 (0.42–2.69) |
| Women | 685 | 0.98 ± 0.01 | 0.92 (0.03–2.68) | 35 | 1.01 ± 0.06 | 1.04 (0.41–1.83) | 46 | 1.06 ± 0.04 | 1.07 (0.52–1.68) | 582 | 0.98 ± 0.01 | 0.92 (0.30–2.68) | 86 | 0.93 ± 0.04 | 0.85 (0.40–2.17) |
| RIBOFLAVIN (mg/day) | |||||||||||||||
| Plausible reporters | 543 | 1.74 ± 0.02 | 1.65 (0.69–6.13) | 120 | 1.72 ± 0.04 | 1.67 (0.96–3.41) | 76 | 1.79 ± 0.06 | 1.77 (0.78–3.46) | 433 | 1.73 ± 0.03 | 1.63 (0.9–6.13) | 45 | 1.77 ± 0.10 | 1.68 (0.85–4.18) |
| Men | 232 | 1.93 ± 0.03 | 1.84 (0.92–6.13) | 68 | 1.77 ± 0.05 | 1.73 (1.04–3.41) | 48 | 1.95 ± 0.08 | 1.92 (1.09–3.46) | 158 | 1.98 ± 0.05 | 1.88 (0.93–6.13) | 24 | 1.96 ± 0.14 | 1.72 (0.92–4.18) |
| Women | 311 | 1.59 ± 0.02 | 1.54 (0.69–3.08) | 52 | 1.65 ± 0.06 | 1.58 (0.96–2.57) | 28 | 1.52 ± 0.06 | 1.51 (0.78–2.04) | 275 | 1.59 ± 0.03 | 1.52 (0.69–3.08) | 21 | 1.56 ± 0.11 | 1.56 (0.85–2.99) |
| Non-Plausible reporters | 1466 | 1.34 ± 0.02 | 1.25 (0.37–3.53) | 93 | 1.36 ± 0.04 | 1.35 (0.50–3.04) | 135 | 1.35 ± 0.04 | 1.34 (0.53–3.82) | 1222 | 1.34 ± 0.03 | 1.24 (0.40–3.54) | 161 | 1.29 ± 0.04 | 1.22 (0.37–4.71) |
| Men | 781 | 1.42 ± 0.04 | 1.30 (0.42–3.53) | 58 | 1.43 ± 0.06 | 1.35 (0.50–3.04) | 89 | 1.45 ± 0.06 | 1.38 (0.55–3.82) | 640 | 1.43 ± 0.06 | 1.30 (0.42–3.54) | 75 | 1.31 ± 0.07 | 1.20 (0.61–4.71) |
| Women | 685 | 1.25 ±0.02 | 1.19 (0.37–2.47) | 35 | 1.25 ± 0.07 | 1.32 (0.53–1.83) | 46 | 1.15 ± 0.05 | 1.09 (0.53–1.84) | 582 | 1.25 ± 0.02 | 1.18 (0.40–3.47) | 86 | 1.27 ± 0.05 | 1.25 (0.37–2.61) |
| NIACIN (mg/day) | |||||||||||||||
| Plausible reporters | 543 | 34.1 ± 0.4 | 33.0 (13.3–105.9) | 120 | 31.2 ± 0.6 | 31.1 (18.8–58.4) | 76 | 34.0 ± 1.1 | 33.1 (13.9–68.3) | 433 | 35.1 ± 0.5 | 33.8 (13.3–105.9) | 45 | 32.6 ± 1.5 | 32.9 (16.0–70.3) |
| Men | 232 | 38.1 ± 0.6 | 36.1 (16.0–105.8) | 68 | 32.4 ± 0.8 | 31.6 (18.8–58.4) | 48 | 37.3 ± 1.2 | 35.7 (17.7–68.3) | 158 | 41.1 ± 1.0 | 39.0 (19.8–105.9) | 24 | 35.7 ± 2.3 | 34.1 (16.0–70.3) |
| Women | 311 | 30.9 ± 0.4 | 30.7 (13.3–66.1) | 52 | 29.7 ± 1.0 | 28.4 (19.5–50.6) | 28 | 28.2 ± 1.5 | 28.2 (13.9–45.3) | 275 | 31.6 ± 0.5 | 30.8 (13.3–66.1) | 21 | 29.0 ± 1.5 | 29.8 (16.6–39.9) |
| Non-Plausible reporters | 1466 | 27.0 ± 0.2 | 25.8 (6.7–109.0) | 93 | 25.0 ± 0.8 | 24.3 (8.6–46.1) | 135 | 28.1 ± 0.8 | 27.6 (11.7–73.6) | 1222 | 27.4 ± 0.3 | 26.1 (6.7–109.0) | 161 | 24.2 ± 0.6 | 22.8 (9.1–61.8) |
| Men | 781 | 29.1 ± 0.3 | 27.6 (8.6–1090.) | 58 | 26 ± 1 | 26 (9–46) | 89 | 29.7 ± 1.0 | 28.5 (11.7–73.6) | 640 | 29.6 ± 0.4 | 28.1 (12.1–109.0) | 75 | 25.5 ± 0.9 | 24.9 (9.8–61.8) |
| Women | 685 | 24.7 ± 0.3 | 24.1 (6.7–53.2) | 35 | 46 | 24.9 ± 1.1 | 24.5 (12.4–43.5) | 582 | 25.0 ± 0.3 | 24.6 (6.7–53.2) | 86 | 23.1 ± 0.7 | 21.9 (9.1–48.2) | ||
| VITAMIN B6 (mg/day) | |||||||||||||||
| Plausible reporters | 543 | 1.83 ± 0.03 | 1.72 (0.57–7.71) | 120 | 1.66 ± 0.04 | 1.63 (0.83–4.29) | 76 | 1.80 ± 0.06 | 1.81 (0.62–3.62) | 433 | 1.85 ± 0.03 | 1.73 (0.57–7.71) | 45 | 2.06 ± 0.12 | 1.89 (0.99–5.29) |
| Men | 232 | 2.05 ± 0.04 | 1.90 (0.85–7.71) | 68 | 1.71 ± 0.06 | 1.68 (0.87–4.29) | 48 | 1.92 ± 0.07 | 1.86 (1.05–3.62) | 158 | 2.20 ± 0.07 | 2.06 (0.85–7.71) | 24 | 2.35 ± 0.19 | 2.11 (1.12–5.29) |
| Women | 311 | 1.7 ± 0.0 | 1.65 (0.57–3.94) | 52 | 1.58 ± 0.06 | 1.53 (0.83–3.16) | 28 | 1.60 ± 0.10 | 1.49 (0.62–2.86) | 275 | 1.66 ± 0.03 | 1.60 (0.57–3.94) | 21 | 1.74 ± 0.10 | 1.71 (0.99–3.01) |
| Non-Plausible reporters | 1466 | 1.43 ± 0.01 | 1.33 (0.28–9.30) | 93 | 1.32 ± 0.05 | 1.30 (0.49–3.28) | 135 | 1.39 ± 0.04 | 1.34 (0.63–3.16) | 1222 | 1.44 ± 0.02 | 1.33 (0.28–9.30) | 161 | 1.42 ± 0.04 | 1.31 (0.62–3.72) |
| Men | 781 | 1.49 ± 0.02 | 1.39 (0.44–9.30) | 58 | 1.34 ± 0.06 | 1.37 (0.56–2.50) | 89 | 1.46 ± 0.06 | 1.39 (0.63–3.16) | 640 | 1.51 ± 0.03 | 1.39 (0.44–9.30) | 75 | 1.50 ± 0.06 | 1.39 (0.73–3.72) |
| Women | 685 | 1.35 ± 0.02 | 1.26 (0.28–3.61) | 35 | 1.28 ± 0.09 | 1.25 (0.49–3.28) | 46 | 1.28 ± 0.05 | 1.2 (0.70–2.21) | 582 | 1.36 ± 0.02 | 1.28 (0.28–3.17) | 86 | 1.34 ± 0.05 | 1.21 (0.62–3.61) |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | |
|---|---|---|---|---|---|
| EFSA | EFSA | EFSA | EFSA | EFSA | |
| THIAMIN (%) | |||||
| Whole population | 71.2 | 91.5 | 77.7 | 70.8 | 61.2 |
| Men | 75.9 | 92.9 | 81.8 | 74.9 | 70.7 |
| Women | 66.5 | 89.7 | 70.3 | 67.0 | 52.3 |
| Plausible reporters | 93.6 | 99.2 | 90.8 | 91.9 | 93.3 |
| Men | 98.3 | 98.5 | 95.8 | 97.5 | 100.0 |
| Women | 90.0 | 100.0 | 82.1 | 88.7 | 85.7 |
| RIBOFLAVIN (%) | |||||
| Whole population | 72.0 | 92.5 | 83.4 | 70.2 | 66.5 |
| Men | 75.4 | 95.2 | 86.9 | 74.3 | 67.7 |
| Women | 68.5 | 88.5 | 77.0 | 66.4 | 65.4 |
| Plausible reporters | 91.3 | 100.0 | 98.7 | 89.6 | 84.4 |
| Men | 97.8 | 100.0 | 100.0 | 97.5 | 95.8 |
| Women | 68.5 | 100.0 | 96.4 | 85.1 | 71.4 |
| NIACIN (%) | |||||
| Whole population | 99.0 | 100.0 | 99.5 | 98.9 | 97.6 |
| Men | 99.6 | 100.0 | 100.0 | 99.7 | 98.0 |
| Women | 98.3 | 100.0 | 98.6 | 98.1 | 97.2 |
| Plausible reporters | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| Men | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| Women | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| VITAMIN B6 (%) | |||||
| Whole population | 77.2 | 89.7 | 83.4 | 76.0 | 78.6 |
| Men | 79.9 | 92.1 | 87.6 | 78.2 | 86.9 |
| Women | 74.5 | 86.2 | 75.7 | 74.0 | 71.0 |
| Plausible reporters | 93.4 | 97.5 | 93.4 | 91.9 | 97.8 |
| Men | 99.1 | 98.5 | 100.0 | 99.4 | 100.0 |
| Women | 89.1 | 96.2 | 82.1 | 87.6 | 95.2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mielgo-Ayuso, J.; Aparicio-Ugarriza, R.; Olza, J.; Aranceta-Bartrina, J.; Gil, Á.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; González-Gross, M. Dietary Intake and Food Sources of Niacin, Riboflavin, Thiamin and Vitamin B6 in a Representative Sample of the Spanish Population. The ANIBES Study. Nutrients 2018, 10, 846. https://doi.org/10.3390/nu10070846
Mielgo-Ayuso J, Aparicio-Ugarriza R, Olza J, Aranceta-Bartrina J, Gil Á, Ortega RM, Serra-Majem L, Varela-Moreiras G, González-Gross M. Dietary Intake and Food Sources of Niacin, Riboflavin, Thiamin and Vitamin B6 in a Representative Sample of the Spanish Population. The ANIBES Study. Nutrients. 2018; 10(7):846. https://doi.org/10.3390/nu10070846
Chicago/Turabian StyleMielgo-Ayuso, Juan, Raquel Aparicio-Ugarriza, Josune Olza, Javier Aranceta-Bartrina, Ángel Gil, Rosa M. Ortega, Lluis Serra-Majem, Gregorio Varela-Moreiras, and Marcela González-Gross. 2018. "Dietary Intake and Food Sources of Niacin, Riboflavin, Thiamin and Vitamin B6 in a Representative Sample of the Spanish Population. The ANIBES Study" Nutrients 10, no. 7: 846. https://doi.org/10.3390/nu10070846
APA StyleMielgo-Ayuso, J., Aparicio-Ugarriza, R., Olza, J., Aranceta-Bartrina, J., Gil, Á., Ortega, R. M., Serra-Majem, L., Varela-Moreiras, G., & González-Gross, M. (2018). Dietary Intake and Food Sources of Niacin, Riboflavin, Thiamin and Vitamin B6 in a Representative Sample of the Spanish Population. The ANIBES Study. Nutrients, 10(7), 846. https://doi.org/10.3390/nu10070846