An Overview of Whole Grain Regulations, Recommendations and Research across Southeast Asia



Abstract
1. Introduction
2. Methods
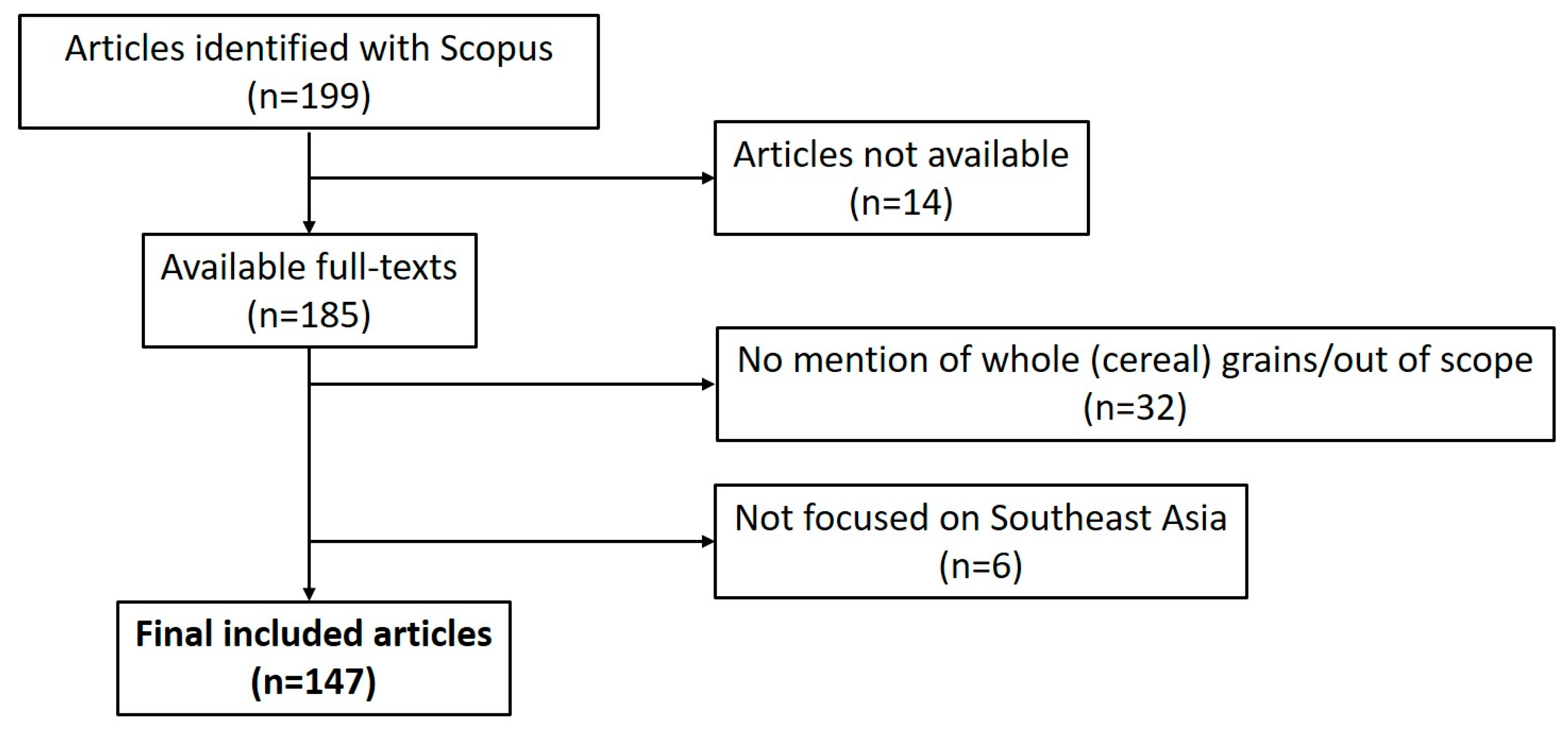
2.1. Literature Search
2.2. Collection of Data on Whole Grain Regulations and Recommendations
3. Results
3.1. Literature Review
3.2. Data on Whole Grain Recommendations, Regulations and Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Food and Agriculture Organization of the United Nations. Food Balance Sheets. Available online: http://www.fao.org/faostat/en/#data/FBS (accessed on 11 May 2018).
- ASEAN Socio-Cultural Community Department and UNICEF EAPRO (East Asia and the Pacific Regional Office). Regional Report on Nutrition in ASEAN Volume 1; ASEAN Socio-Cultural Community Department and UNICEF EAPRO (East Asia and the Pacific Regional Office): Bangkok, Thailand, 2016. [Google Scholar]
- ASEAN Socio-Cultural Community Department and UNICEF EAPRO (East Asia and the Pacific Regional Office). Regional Report on Nutrition in ASEAN Volume 2; ASEAN Socio-Cultural Community Department and UNICEF EAPRO (East Asia and the Pacific Regional Office): Bangkok, Thailand, 2016. [Google Scholar]
- International Food Policy Research Institute. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030; International Food Policy Research Institute: Washington, DC, USA, 2016. [Google Scholar]
- International Diabetes Federation. Diabetes Atlas, 7th ed. Available online: http://www.diabetesatlas.org/resources/2015-atlas.html (accessed on 31 October 2017).
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Norat, T.; Romundstad, P.; Vatten, L.J. Whole grain and refined grain consumption and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of cohort studies. Eur. J. Epidemiol. 2013, 28, 845–858. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343, d6617. [Google Scholar] [CrossRef] [PubMed]
- Thielecke, F.; Jonnalagadda, S.S. Can whole grain help in weight management? J. Clin. Gastroenterol. 2014, 48, S70–S77. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Zanovec, M.; Cho, S.S.; Nicklas, T.A. Whole grain and fiber consumption are associated with lower body weight measures in US adults: National Health and Nutrition Examination Survey 1999–2004. Nutr. Res. 2010, 30, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Albertson, A.M.; Reicks, M.; Joshi, N.; Gugger, C.K. Whole grain consumption trends and associations with body weight measures in the United States: Results from the cross sectional National Health and Nutrition Examination Survey 2001–2012. Nutr. J. 2016, 15. [Google Scholar] [CrossRef] [PubMed]
- Devlin, N.F.C.; McNulty, B.A.; Gibney, M.J.; Thielecke, F.; Smith, H.; Nugent, A.P. Whole grain intakes in the diets of Irish children and teenagers. Br. J. Nutr. 2013, 110, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Galea, L.M.; Beck, E.J.; Probst, Y.C.; Cashman, C.J. Whole grain intake of Australians estimated from a cross-sectional analysis of dietary intake data from the 2011–13 Australian Health Survey. Public Health Nutr. 2017, 20, 2166–2172. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.D.; Pearce, M.S.; McKevith, B.; Thielecke, F.; Seal, C.J. Low whole grain intake in the UK: Results from the National Diet and Nutrition Survey rolling programme 2008–11. Br. J. Nutr. 2015, 113, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Seal, C.J.; Brownlee, I.A. Whole-grain foods and chronic disease: Evidence from epidemiological and intervention studies. Proc. Nutr. Soc. 2015, 74, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Global Health Data Exchange. Global Burden of Disease Results Tool. Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2016-permalink/0684f896deb2d178ec1a09e4b125d3ea (accessed on 3 April 2018).
- Association of Southeast Asian Nations. ASEAN Free Trade Area. Available online: http://asean.org/asean-economic-community/asean-free-trade-area-afta-council/ (accessed on 31 October 2017).
- Haitao, H. The role of trust in China-ASEAN relations—Towards a multi-level trust building for China and ASEAN. Int. J. China Stud. 2017, 8, 45–59. [Google Scholar]
- Phattarakul, N.; Rerkasem, B.; Li, L.J.; Wu, L.H.; Zou, C.Q.; Ram, H.; Sohu, V.S.; Kang, B.S.; Surek, H.; Kalayci, M.; et al. Biofortification of rice grain with zinc through zinc fertilization in different countries. Plant Soil 2012, 361, 131–141. [Google Scholar] [CrossRef]
- Goodman, M.T.; Wilkens, L.R.; Hankin, J.H.; Lyu, L.C.; Wu, A.H.; Kolonel, L.N. Association of soyand fiber consumption with the risk of endometrial cancer. Am. J. Epidemiol. 1997, 146, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Peterman, J.N.; Silka, L.; Bermudez, O.I.; Wilde, P.E.; Rogers, B.L. Acculturation, education, nutrition education, and household composition are related to dietary practices among Cambodian refugee women in Lowell, MA. J. Am. Diet. Assoc. 2011, 111, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- McCrory, M.A.; Jaret, C.L.; Kim, J.H.; Reitzes, D.C. Dietary patterns among vietnamese and hispanic immigrant elementary school children participating in an after school program. Nutrients 2017, 9, 460. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.L.; Juliana, S.; Sakinah, H. Dietary compliance and its association with glycemic control among poorly controlled type 2 diabetic outpatients in Hospital Universiti Sains Malaysia. Malays. J. Nutr. 2011, 17, 287–299. [Google Scholar] [PubMed]
- Randi, G.; Edefonti, V.; Ferraroni, M.; La Vecchia, C.; Decarli, A. Dietary patterns and the risk of colorectal cancer and adenomas. Nutr. Rev. 2010, 68, 389–408. [Google Scholar] [CrossRef] [PubMed]
- Yaw, Y.H.; Shariff, Z.M.; Kandiah, M.; Weay, Y.H.; Saibul, N.; Sariman, S.; Hashim, Z. Diet and physical activity in relation to weight change among breast cancer patients. Asian Pac. J. Cancer Prev. 2014, 15, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Sangthong, R.; Wichaidit, W.; McNeil, E.; Chongsuvivatwong, V.; Chariyalertsak, S.; Kessomboon, P.; Taneepanichskul, S.; Putwatana, P.; Aekplakorn, W. Health behaviors among short- and long- term ex-smokers: Results from the Thai National Health Examination Survey IV, 2009. Prev. Med. 2012, 55, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Rebello, S.A.; Koh, H.; Chen, C.; Naidoo, N.; Odegaard, A.O.; Koh, W.P.; Butler, L.M.; Yuan, J.M.; Van Dam, R.M. Amount, type, and sources of carbohydrates in relation to ischemic heart disease mortality in a Chinese population: A prospective cohort study. Am. J. Clin. Nutr. 2014, 100, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Colega, M.T.; Lim, A.L.; Silva-Zolezzi, I.; Macé, K.; Saw, S.M.; Kwek, K.; Gluckman, P.; Godfrey, K.M.; Chong, Y.S.; et al. Whole grain intake, determined by dietary records and plasma alkylresorcinol concentrations, is low among pregnant women in Singapore. Asia Pac. J. Clin. Nutr. 2015, 24, 674–682. [Google Scholar] [PubMed]
- Whitton, C.; Ma, Y.; Bastian, A.C.; Fen Chan, M.; Chew, L. Fast-food consumers in singapore: Demographic profile, diet quality and weight status. Public Health Nutr. 2014, 17, 1805–1813. [Google Scholar] [CrossRef] [PubMed]
- Aekplakorn, W.; Satheannoppakao, W.; Putwatana, P.; Taneepanichskul, S.; Kessomboon, P.; Chongsuvivatwong, V.; Chariyalertsak, S. Dietary Pattern and Metabolic Syndrome in Thai Adults. J. Nutr. Metab. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Neo, J.E.; Binte Mohamed Salleh, S.; Toh, Y.X.; How, K.Y.L.; Tee, M.; Mann, K.; Hopkins, S.; Thielecke, F.; Seal, C.J.; Brownlee, I.A. Whole-grain food consumption in Singaporean children aged 6–12 years. J. Nutr. Sci. 2016. [Google Scholar] [CrossRef] [PubMed]
- Norimah, A.K.; Koo, H.C.; Hamid Jan, J.M.; Mohd Nasir, M.T.; Tan, S.Y.; Appukutty, M.; Nurliyana, A.R.; Thielecke, F.; Hopkins, S.; Ong, M.K.; et al. Whole grain intakes in the diets of Malaysian children and adolescents-findings from the MyBreakfast study. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Bulatao, R.M.; Romero, M.V. Effects of germination on the proximate composition, antioxidant property and eating quality of brown rice (Oryza sativa L.). Philipp. Agric. Sci. 2014, 97, 19–27. [Google Scholar]
- Charoenthaikij, P.; Jangchud, K.; Jangchud, A.; Prinyawiwatkul, W.; No, H.K.; King, J.M. Physicochemical properties and consumer acceptance of wheat-germinated brown rice bread during storage time. J. Food Sci. 2010, 75, S333–S339. [Google Scholar] [CrossRef] [PubMed]
- Charoenthaikij, P.; Jangchud, K.; Jangchud, A.; Prinyawiwatkul, W.; Tungtrakul, P. Germination conditions affect selected quality of composite wheat-germinated brown rice flour and bread formulations. J. Food Sci. 2010, 75, S312–S318. [Google Scholar] [CrossRef] [PubMed]
- Alice, C.L.V.; Wan Rosli, W.I. Effects of brown rice powder addition on nutritional composition and acceptability of two selected Malaysian traditional rice-based local Kuih. Int. Food Res. J. 2015, 22, 1124–1131. [Google Scholar]
- Lestari, L.A.; Huriyati, E.; Marsono, Y. The development of low glycemic index cookie bars from foxtail millet (Setaria italica), arrowroot (Maranta arundinacea) flour, and kidney beans (Phaseolus vulgaris). J. Food Sci. Technol. 2017, 54, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.C.; Poh, B.K.; Ruzita, A.T. Development, validity and reliability of a questionnaire on knowledge, attitude and practice (KAP) towards whole grain among primary school children in Kuala Lumpur, Malaysia. Int. Food Res. J. 2016, 23, 797–805. [Google Scholar]
- Neo, J.E.; Brownlee, I.A. Wholegrain food acceptance in young Singaporean adults. Nutrients 2017, 9, 371. [Google Scholar] [CrossRef] [PubMed]
- Singhato, A.; Banjong, O.; Charoonruk, G. Effectiveness and acceptance of the developed educational media on the application of a Thai ethnic snack, Thong Pub, with calcium fortification. J. Ethn. Foods 2017, 4, 58–63. [Google Scholar] [CrossRef]
- Son, J.S.; Do, V.B.; Kim, K.O.; Cho, M.S.; Suwonsichon, T.; Valentin, D. Consumers’ attitude towards rice cooking processes in Korea, Japan, Thailand and France. Food Qual. Preference 2013, 29, 65–75. [Google Scholar] [CrossRef]
- Shiu, L.K.C.; Loke, W.M.; Vijaya, K.; Sandhu, N.K. Nurturing healthy dietary habits among children and youth in Singapore. Asia Pac. J. Clin. Nutr. 2012, 21, 144–150. [Google Scholar] [PubMed]
- Mohd Yusof, B.N.; Abd Talib, R.; Karim, N.A.; Kamarudin, N.A.; Arshad, F. Glycaemic index of four commercially available breads in Malaysia. Int. J. Food Sci. Nutr. 2009, 60, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Panlasigui, L.N.; Thompson, L.U. Blood glucose lowering effects of brown rice in normal and diabetic subjects. Int. J. Food Sci. Nutr. 2006, 57, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Se, C.H.; Chuah, K.A.; Mishra, A.; Wickneswari, R.; Karupaiah, T. Evaluating crossbred red rice variants for postprandial glucometabolic responses: A comparison with commercial varieties. Nutrients 2016, 8, 308. [Google Scholar] [CrossRef] [PubMed]
- Trinidad, T.P.; Mallillin, A.C.; Sagum, R.S.; Felix, A.D.R.; Tuaño, A.P.P.; Juliano, B.O. Relative effect of apparent amylose content on the glycemic index of milled and brown rice. Philipp. Agric. Sci. 2014, 97, 405–408. [Google Scholar]
- Golloso-Gubat, M.J.; Magtibay, E.V.J.; Nacis, J.S.; Udarbe, M.A.; Santos, N.L.C.; Timoteo, V.J.A. Postprandial satiety responses and ghrelin levels with consumption of white rice and brown rice in selected Filipino adults. Philipp. J. Sci. 2016, 145, 405–412. [Google Scholar]
- Trinidad, T.P.; Kurilich, A.C.; Mallillin, A.C.; Walcyzk, T.; Sagum, R.S.; Singh, N.N.; Harjani, Y.; De Leon, M.P.; Capanzana, M.V.; Fletcher, J. Iron absorption from NaFeEDTA-fortified oat beverages with or without added vitamin C. Int. J. Food Sci. Nutr. 2014, 65, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Trinidad, T.P.; Mallillin, A.C.; Sagum, R.S.; Briones, D.P.; Encabo, R.R.; Juliano, B.O. Iron absorption from brown rice/brown rice-based meal and milled rice/milled rice-based meal. Int. J. Food Sci. Nutr. 2009, 60, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Thongoun, P.; Pavadhgul, P.; Bumrungpert, A.; Satitvipawee, P.; Harjani, Y.; Kurilich, A. Effect of oat consumption on lipid profiles in hypercholesterolemic adults. J. Med. Assoc. Thail. 2013, 96 (Suppl. 5), S25–S32. [Google Scholar]
- Bui, T.N.; Le Hop, T.; Nguyen, D.H.; Tran, Q.B.; Nguyen, T.L.; Le, D.T.; Nguyen, D.V.A.; Vu, A.L.; Aoto, H.; Okuhara, Y.; et al. Pre-germinated brown rice reduced both blood glucose concentration and body weight in vietnamese women with impaired glucose tolerance. J. Nutr. Sci. Vitaminol. 2014, 60, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Kementerian Kesehatan (Indonesian Ministry of Health). Pedoman Gizi Seimbang (Nutritional Guidelines Handbook); Kementerian Kesehatan (Indonesian Ministry of Health): Jakarta, Indonesia, 2014.
- Ministry of Health Malaysia. Malaysian Dietary Guidelines Key Message 4—Eat Adequate Amount of Rice, Other Cereal Products (Preferably Whole Grain) and Tubers; Ministry of Health Malaysia: Putrajaya, Malaysia, 2010.
- Republic of the Philippines Food and Nutrition Research Institute. Pinggang Pinoy (Filipino Plate); Food and Nutrition Research Institute Department of Science and Technology: Metro Manila, The Philippines, 2016.
- Health Promotion Board. My Healthy Plate. Available online: https://www.healthhub.sg/programmes/55/my-healthy-plate (accessed on 19 February 2018).
- Health Promotion Board. Whole Grains—The Wise Choice! Available online: https://www.healthhub.sg/live-healthy/183/whole_grains_wise_choice (accessed on 19 February 2018).
- Health Promotion Board. Food-Based Dietary Guidelines for Adults. Available online: https://www.healthhub.sg/live-healthy/15/dietary_guidelines_adults (accessed on 19 February 2018).
- Health Promotion Board. HealthHub Track; Health Promotion Board: Singapore, 2018.
- Nutrition Society of Malaysia. Dietary Guidelines. Available online: http://nsm.nutritionmonthmalaysia.org.my/dietary-guidelines/ (accessed on 7 March 2018).
- Nutrition Society of Malaysia. Wonders of Whole Grains; Nutrition Society of Malaysia: Selangor, Malaysia, 2012. [Google Scholar]
- Nutrition Society of Malaysia. Eat Smart, Get Fit & Feel Great. An infographic Kit—Nutrition Month Malaysia. Available online: http://nutritionmonthmalaysia.org.my/wp-content/uploads/2017/09/NMM%202016%20Info%20Graphic%20Book%20(Final).pdf (accessed on 27 March 2018).
- Nutrition Society of Malaysia. Eat Smart, Move More. Recipe for Healthy Families. An Infographic Kit Volume 2—Nutrition Month Malaysia. Available online: http://nutritionmonthmalaysia.org.my/wp-content/uploads/2017/09/NMM%202017%20Info%20Graphic%20Book%20(Final).pdf (accessed on 27 March 2018).
- Nutrition Society of Malaysia. Your Only Choice: Eat Healthy, Be Active. An Infographic Kit—Nutrition Month Malaysia. Available online: http://nutritionmonthmalaysia.org.my/wp-content/uploads/2018/04/NMM%202018%20Info%20Graphic%20Book%20(FINAL%20PRINT).pdf (accessed on 27 March 2018).
- Singapore Nutrition and Dietetic Association; Health Promotion Board. Advocating Whole Grains Consumption as a Key Approach in Diabetes Prevention; Singapore Nutrition and Dietetic Association; Health Promotion Board: Singapore, 2016.
- Agri-Food and Veterinary Agency of Singapore. Sale of Food Act (Chapter 283, Section 56(1)) Food Regulations; Agri-Food and Veterinary Agency of Singapore: Singapore, 2017.
- Agri-Food and Veterinary Agency of Singapore. A Guide to Food Labelling and Advertisements; Agri-Food and Veterinary Agency of Singapore: Singapore, 2017.
- Ministry of Health Malaysia. Online Public Engagement No 1/2018 Proposed Draft Amendment for Food Regulation 1985; Ministry of Health Malaysia: Putrajaya, Malaysia, 2018.
- Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control). Peraturan Kepala Badan Pengawas Obat Dan Makanan Nomor 21 (Regulation Number 21 of the Chief of the National Agency of Drug and Food Control); Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control): Jakarta, Indonesia, 2016.
- Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control). Peraturan Kepala Badan Pengawas Obat Dan Makanan Nomor 12 (Regulation Number 12 of the Chief of the National Agency of Drug and Food Control Number 12); Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control): Jakarta, Indonesia, 2016.
- Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control). Peraturan Kepala Badan Pengawas Obat Dan Makanan Nomor 13 (Regulation Number 13 of the Chief of the National Agency of Drug and Food Control Number 12); Badan Pengawas Obat Dan Makanan Republik Indonesia (Republic of Indonesia’s National Agency of Drug and Food Control): Jakarta, Indonesia, 2016.
- Health Promotion Board. Healthier Choice Symbol Nutrient Guidelines; Health Promotion Board: Singapore, 2018.
- National Bureau of Agricultural Commodity and Food Standards of Thailand. Database of Food Consumption of Thai People. Available online: http://consumption.acfs.go.th/index.php (accessed on 27 May 2018).
- Republic of the Philippines Food and Nutrition Research Institute. 8th National Nutrition Survey; Republic of the Philippines Food and Nutrition Research Institute: Metro Manila, The Philippines, 2013.
- Health Promotion Board. National Nutrition Survey; Health Promotion Board: Singapore, 2010.
- US Department of Health (Human Services). Dietary Guidelines for Americans 2015–2020; Skyhorse Publishing Inc.: New York, NY, USA, 2017. [Google Scholar]
- Wailes, E.J.; Chavez, E.C. ASEAN and the Global Rice Situation and Outlook; Asian Development Bank: Metro Manila, The Philippines, 2012. [Google Scholar]
- Greve, C.; Neess, R.I. The Evolution of the Whole Grain Partnership in Denmark; Copenhagen Business School and the Danish Whole Grain Partnership: Copenhagen, Denmark, 2014. [Google Scholar]
- Thies, F.; Masson, L.F.; Boffetta, P.; Kris-Etherton, P. Oats and CVD risk markers: A systematic literature review. Br. J. Nutr. 2014, 112, S19–S30. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.Y.; Jones, M.; Barclay, A.W.; Brand-Miller, J.C. Dietary glycaemic index and glycaemic load among Australian adults-results from the 2011–2012 Australian Health Survey. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Kaur, B.; Ranawana, V.; Henry, J. The Glycemic Index of Rice and Rice Products: A Review, and Table of GI Values. Crit. Rev. Food Sci. Nutr. 2016, 56, 215–236. [Google Scholar] [CrossRef] [PubMed]
- Ranawana, D.V.; Henry, C.J.K.; Lightowler, H.J.; Wang, D. Glycaemic index of some commercially available rice and rice products in Great Britain. Int. J. Food Sci. Nutr. 2009, 60, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Zhao, H.; Duan, Z.; Linlin, Z.; Wu, D. Starch digestibility and the estimated glycemic score of different types of rice differing in amylose contents. J. Cereal Sci. 2004, 40, 231–237. [Google Scholar] [CrossRef]
- Food and Agricultural Organization of the United Nations. Food-Based Dietary Guidelines—Thailand. Available online: http://www.fao.org/nutrition/education/food-based-dietary-guidelines/regions/countries/thailand/en/ (accessed on 27 May 2018).
- Food and Agricultural Organization of the United Nations. Food-Based Dietary Guidelines—Vietnam. Available online: http://www.fao.org/nutrition/education/food-based-dietary-guidelines/regions/countries/vietnam/en/ (accessed on 27 May 2018).
- Food and Agricultural Organization of the United Nations. Food-Based Dietary Guidelines—Asia and the Pacific. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/asia-pacific/en/ (accessed on 27 May 2018).
- Tee, E.; Hardinsyah, R.; Fiorentino, R.; Ismail, M.; Suthutvoravut, U.; Hop, L. Food-based dietary guidelines of Southeast Asian countries: Part 1-A compilation and analysis of key messages. Malays. J. Nutr. 2016, 22, S1–S47. [Google Scholar]
- Ross, A.B.; Kristensen, M.; Seal, C.J.; Jacques, P.; McKeown, N.M. Recommendations for reporting whole-grain intake in observational and intervention studies. Am. J. Clin. Nutr. 2015, 101, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Seal, C.J.; Nugent, A.P.; Tee, E.S.; Thielecke, F. Whole-grain dietary recommendations: The need for a unified global approach. Br. J. Nutr. 2016, 115, 2031–2038. [Google Scholar] [CrossRef] [PubMed]
- Korczak, R.; Marquart, L.; Slavin, J.L.; Ringling, K.; Chu, Y.; O’Shea, M.; Harriman, C.; Toups, K.; De Vries, J.; Jacques, P.; et al. Thinking critically about whole-grain definitions: Summary report of an interdisciplinary roundtable discussion at the 2015 Whole Grains Summit1. Am. J. Clin. Nutr. 2016, 104, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; van der Kamp, J.W.; King, R.; Lê, K.A.; Mejborn, H.; Seal, C.J.; Thielecke, F. Perspective: A definition for whole-grain food products—Recommendations from the Healthgrain Forum. Adv. Nutr. 2017, 8, 525–531. [Google Scholar] [PubMed]
- Devadason, E.S.; Chandran, V.G.R.; Kalirajan, K. Harmonization of food trade standards and regulations in ASEAN: The case of Malaysia’s food imports. Agric. Econ. 2018, 49, 97–109. [Google Scholar] [CrossRef]
- Association of Southeast Asian Nations. External Trade Statistics: Top Ten ASEAN Trade Partner Countries/Regions 2015; Association of Southeast Asian Nations: Jakarta, Indonesia, 2016. [Google Scholar]
- Food and Agricultural Organization of the United Nations. Food-Based Dietary Guidelines—China. Available online: http://www.fao.org/nutrition/education/food-dietary-guidelines/regions/asia-pacific/en/ (accessed on 27 May 2018).
- Chinese Nutrition Society. Chinese Dietary Guidelines 2016; Chinese Nutrition Society: Beijing, China, 2016. [Google Scholar]
- He, Y.; Zhao, L.; Yu, D.; Hu, J.; Yang, Y.; Yang, X. The status of coarse food intakes among Chinese adults. Acta Nutr. Sin. 2016, 2016, 115–118. [Google Scholar]


{kind=link}
| Country | Nutrition | Consumer Studies | Food Science and Technology | Food Production | Total |
|---|---|---|---|---|---|
| Brunei Darussalam | 0 | 0 | 0 | 0 | 0 |
| Cambodia | 1 | 0 | 0 | 1 | 2 |
| Indonesia | 1 | 1 | 9 | 5 | 16 |
| LPDR | 0 | 0 | 0 | 0 | 0 |
| Malaysia | 5 | 2 | 18 | 4 | 29 |
| Myanmar | 0 | 0 | 0 | 0 | 0 |
| The Philippines | 6 | 1 | 6 | 1 | 14 |
| Singapore | 5 | 2 | 0 | 0 | 7 |
| Thailand | 13 | 4 | 60 | 5 | 82 |
| Vietnam | 1 | 0 | 4 | 2 | 7 |
| Multiple countries | 1 | 0 | 2 | 3 | 6 |
| Total | 33 | 10 | 99 | 21 | 163 * |
| Questions | |||||
|---|---|---|---|---|---|
| Country | Are There Country-Specific, Food-Based Whole Grain Recommendations from Public Health Agencies (e.g., Ministry of Health)? | Are There Suggestions for Wholegrain Food Portion Size or Amounts of Whole Grains in These Food-Based Recommendations? | Has the Public Health Agency Suggested (Scientific or Other) Rationale for Increasing Whole Grain Intake? | Do the Above Recommendations Suggest One or More scientific/Other Rationale is Suggested for Increasing Whole Grain Intake? | Are the Public Health Agencies Using Specific Tools, Educational Materials or Other Approaches to Increase Whole Grain Intake? |
| Brunei | |||||
| Cambodia | |||||
| Indonesia | Y [52] | N | N | N | N |
| LPDR | |||||
| Malaysia | Y [53] | Y [53] | Y [53] | Y [53] | N |
| Myanmar | |||||
| The Philippines | Y [54] | Y [54] | Y [54] | N | Y [53] |
| Singapore | Y [55] | Y [56] | Y [56] | Y [57] | Y [56,58] |
| Thailand | N | N | N | N | N |
| Vietnam | N | N | N | N | N |
| Questions | ||||
|---|---|---|---|---|
| Country | Are There Country-Specific, Food-Based Whole Grain Recommendations From Professional Groups or Non-Governmental Organisations (e.g., Nutrition Society/Whole Grains Council etc.)? | Are There Suggestions for Wholegrain Food Portion Size or Amounts of Whole Grains In The Above Mentioned Guideline? | Do The Above Recommendations Suggest (Scientific or Other) Rationale for Increasing Whole Grain Intake? | Are the Above Professional Bodies or Non-Governmental Organisations Using Specific Tools, Educational Materials or Other Approaches to Increase Whole Grain Intake? |
| Brunei | ||||
| Cambodia | ||||
| Indonesia | N | N | N | N |
| LPDR | ||||
| Malaysia | Y [53,59] | Y [53,60] | Y [53,59] | Y [60,61,62,63] |
| Myanmar | ||||
| The Philippines | N | N | N | N |
| Singapore | Y [64] | N | Y [64] | N |
| Thailand | N | N | N | N |
| Vietnam | N | N | N | N |
| Questions | |||||
|---|---|---|---|---|---|
| Country | Are There Existing Regulations Related to the Definition of Whole Grains and Wholegrain Foods? | Do the Regulations Include Requirements for Minimum Amounts of Whole Grains in Various Foods? | Are There Labelling Requirements or Options for Whole Grains and Wholegrain Foods? | Do the Regulations Allow Content Claims Related to Whole Grains? | Do the Regulations Allow Any Health Claims Related to Whole Grains? |
| Brunei | |||||
| Cambodia | |||||
| Indonesia | Y [68] | Y [68] | Y [69] | Y [69] | N [70] |
| LPDR | |||||
| Malaysia | Y a | Y | Y a | N | N |
| Myanmar | |||||
| The Philippines | N | N | N | N | N |
| Singapore | Y [65] | N | Y [71] | Y b [66] | Y b [66] |
| Thailand | N | N | N | N | Y c |
| Vietnam | N | N | N | Yc | Y c |
| Questions | |||||||
|---|---|---|---|---|---|---|---|
| Country | Are There Estimates of Whole Grain Intake Data Available For Adults From The Last 10 Years? | Are There (Recent) Estimates of Whole Grain Intake Data Available for Children for The Last Ten Years? | Are There Data Available for Changes in Whole Grain Intake over Time for Adults? | Are There Data Available for Changes in Whole Grain Intake over Time for Children? | Are There Data on the Percentage of Adults that Meet the Public Health Recommendations (Either in Amounts or Servings) for This Country? | Are There Data on the Percentage of Children That Meet the Public Health Recommendations for This Country? | Do Data Exist (From Market or Nutritional Surveys) on the Types of Wholegrain Foods That Are Consumed and the Proportion That They Are Consumed in? |
| Brunei | |||||||
| Cambodia | |||||||
| Indonesia | N | N | N | N | N | N | N |
| LDPR | |||||||
| Malaysia | N | Y [32] | N | N | Na | N | N |
| Myanmar | |||||||
| The Philippines | Y [73] | Y [73] | N | N | Y [73] | ||
| Singapore | Y [74] | Y [31] | Y [74] | N | Y [74] | N | Y b [31] |
| Thailand | N | N | N | N | N | N | N |
| Vietnam | N | N | N | N | N | N | N |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brownlee, I.A.; Durukan, E.; Masset, G.; Hopkins, S.; Tee, E.-S. An Overview of Whole Grain Regulations, Recommendations and Research across Southeast Asia. Nutrients 2018, 10, 752. https://doi.org/10.3390/nu10060752
Brownlee IA, Durukan E, Masset G, Hopkins S, Tee E-S. An Overview of Whole Grain Regulations, Recommendations and Research across Southeast Asia. Nutrients. 2018; 10(6):752. https://doi.org/10.3390/nu10060752
Chicago/Turabian StyleBrownlee, Iain A, Ece Durukan, Gabriel Masset, Sinead Hopkins, and E-Siong Tee. 2018. "An Overview of Whole Grain Regulations, Recommendations and Research across Southeast Asia" Nutrients 10, no. 6: 752. https://doi.org/10.3390/nu10060752
APA StyleBrownlee, I. A., Durukan, E., Masset, G., Hopkins, S., & Tee, E.-S. (2018). An Overview of Whole Grain Regulations, Recommendations and Research across Southeast Asia. Nutrients, 10(6), 752. https://doi.org/10.3390/nu10060752