Decreased Levels of Circulating Carboxylated Osteocalcin in Children with Low Energy Fractures: A Pilot Study


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Statistical Analysis
3. Results
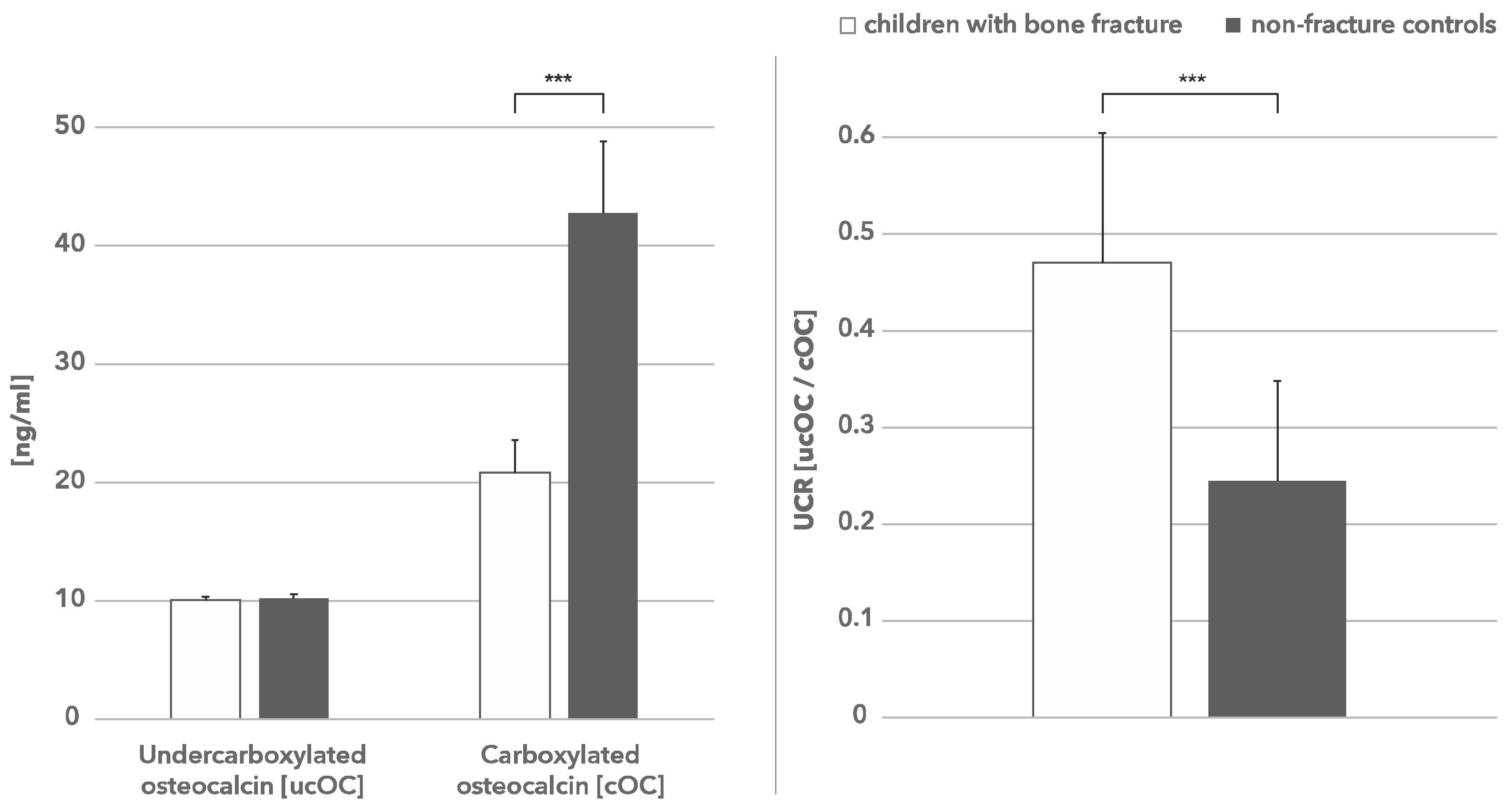
3.1. Bone Turnover Parameters
3.2. Vitamin K Status
3.3. UCR as Predictor of Risk Fracture
3.4. Correlation of Vitamin K Status and Bone Turnover Parameters
3.5. Vitamin D Status
4. Discussion
Author Contributions
Conflicts of Interest
References
- Jones, I.; Williams, S.; Dow, N.; Goulding, A. How Many Children Remain Fracture-Free During Growth? A Longitudinal Study of Children and Adolescents Participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos. Int. 2002, 12, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Alffram, P.A.; Bauer, G.C. Epidemiology of fractures of the forearm. A biomechanical investigation of bone strength. JBJS 1962, 44, 105–114. [Google Scholar] [CrossRef]
- Khosla, S.; Melton, L.J., III; Dekutoski, M.B.; Achenbach, S.J.; Oberg, A.L.; Riggs, B.L. Incidence of childhood distal forearm fractures over 30 years: A population-based study. JAMA 2003, 290, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Hedström, E.M.; Svensson, O.; Bergstrom, U.; Michno, P. Epidemiology of fractures in children and adolescents. Acta Orthop. 2010, 81, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Wilcke, M.K.; Hammarberg, H.; Adolphson, P.Y. Epidemiology and changed surgical treatment methods for fractures of the distal radius: A registry analysis of 42,583 patients in Stockholm County, Sweden, 2004–2010. Acta Orthop. 2013, 84, 292–296. [Google Scholar] [CrossRef] [PubMed]
- De Putter, C.E.; van Beeck, E.F.; Looman, C.W.; Toet, H.; Hovius, S.E.; Selles, R.W. Trends in wrist fractures in children and adolescents, 1997–2009. J. Hand Surg. 2011, 36, 1810–1815. [Google Scholar] [CrossRef] [PubMed]
- Buttazzoni, C.; Rosengren, B.E.; Tveit, M.; Landin, L.; Nilsson, J.A.; Karlsson, M.K. Does a childhood fracture predict low bone mass in young adulthood? A 27-year prospective controlled study. J. Bone Miner. Res. 2013, 28, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.; Melton, L.J., III; Achenbach, S.J.; Atkinson, E.J.; Dekutoski, M.B.; Kirmani, S.; Fischer, P.R.; Khosla, S. A distal forearm fracture in childhood is associated with an increased risk for future fragility fractures in adult men, but not women. J. Bone Miner. Res. 2013, 28, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, M.; Popko, J.; Żelazowska-Rutkowska, B. Prevalence of vitamin D insufficiency in children with low-energy fractures. Endokrynol Ped. 2011, 2, 9–16. [Google Scholar]
- Karpiński, M.; Galicka, A.; Milewski, R.; Popko, J.; Badmaev, V.; Stohs, S.J. Association between vitamin D receptor polymorphism and serum vitamin D levels in children with low-energy fractures. J. Am. Coll. Nutr. 2017, 36, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Lian, J.; Stewart, C.; Puchacz, E.; Mackowiak, S.; Shalhoub, V.; Collart, D.; Zambetti, G.; Stein, G. Structure of the rat osteocalcin gene and regulation of vitamin D-dependent expression. Proc. Natl. Acad. Sci. USA 1989, 86, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, E.; Molgaard, C.; Michaelsen, K.; Jakobsen, J.; Lamberg-Allardt, C.; Cashman, K. Serum percentage undercarboxylated osteocalcin, a sensitive measure of vitamin K status, and its relationship to bone health indices in Danish girls. Br. J. Nutr. 2007, 97, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Cranenburg, E.C.; Schurgers, L.J.; Vermeer, C. Vitamin K: The coagulation vitamin that became omnipotent. Thromb. Haemost. 2007, 97, 20–25. [Google Scholar] [CrossRef]
- Brown, J.; Delmas, P.D.; Malaval, L.; Edouard, L.; Chapuy, M.C.; Meunier, P.J. Serum bone Gla-protein: A specific marker for bone formation in postmenopausal osteoporosis. Lancet 1984, 323, 1091–1093. [Google Scholar] [CrossRef]
- Shearer, M.J. Role of vitamin K and Gla proteins in the pathophysiology of osteoporosis and vascular calcification. Curr. Opin. Clin. Nutr. Metab. Care 2000, 3, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Vermeer, C. Determination of phylloquinone and menaquinones in food. Effect of food matrix on circulating vitamin K concentrations. Haemostasis 2000, 30, 298–307. [Google Scholar] [PubMed]
- Karpiński, M.; Popko, J.; Maresz, K.; Badmaev, V.; Stohs, S.J. Roles of vitamins D and K, nutrition, and lifestyle in low-energy bone fractures in children and young adults. J. Am. Coll. Nutr. 2017, 36, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Sokoll, L.J.; Sadowski, J.A. Comparison of biochemical indexes for assessing vitamin K status in healthy adult population. Am. J. Clin. Nutr. 1996, 63, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.C.; Krueger, D.C.; Engelke, J.A.; Foley, A.L.; Suttie, J.W. Vitamin K supplementation reduces serum concentration of under-γ-carboxylated osteocalcin in healthy young and elderly adults. Am. J. Clin. Nutr. 2000, 72, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Mayranpaa, M.K.; Viljakainen, H.T.; Toiviainen-Salo, S.; Kallio, P.E.; Makitie, O. Impaired bone health and asymptomatic vertebral compressions in fracture-prone children: A case-control study. J. Bone Miner. Res. 2012, 27, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Goulding, A.; Jones, I.E.; Williams, S.M.; Grant, A.M.; Taylor, R.W.; Manning, P.J.; Langley, J. First fracture is associated with increased risk of new fracture during growth. J. Pediatr. 2005, 146, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.M.; Ness, A.R.; Bishop, N.J.; Tobias, J.H. Association between bone mass and fractures in children: A prospective cohort study. J. Bone Miner. Res. 2006, 21, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Goulding, A.; Rockell, J.E.; Black, R.E.; Grant, A.M.; Jones, I.E.; Williams, S.M. Children who avoid drinking cow’s milk are at increased risk for prepubertal bone fractures. J. Am. Diet. Assoc. 2004, 104, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M. Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D deficiency in children and its management review of current knowledge and recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [PubMed]
- Shea, M.K.; Booth, S.L. Update on role of vitamin K in skeletal health. Nutr. Rev. 2008, 66, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Kalkwarf, H.J.; Khoury, J.C.; Bean, J.; Elliot, J.G. Vitamin, K, bone turnover, and bone mass in girls. Am. J. Clin. Nutr. 2004, 80, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Van Summeren, M.J.H.; Braam, L.; Noirt, F.; Kuis, W.; Vermeer, C. Pronounced elevation of undercarboxylated osteocalcin in healthy children. Pediatr. Res. 2007, 61, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Van Summeren, M.J.; Braam, L.A.; Lilien, M.R.; Schurgers, L.J.; Kuis, W.; Vermeer, C. The effect of menaquinone-7 (vitamin K2) supplementation on osteocalcin carboxylation in healthy prepubertal children. Br. J. Nutr. 2009, 102, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Van Summeren, M.J.; van Coeverden, S.C.; Schurgers, L.J.; Braam, L.A.; Noirt, F.; Uiterwaal, C.S.; Kuis, W.; Vermeer, C. Vitamin K status is associated with childhood bone mineral content. Br. J. Nutr. 2008, 100, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Kirmani, S.; Atkinson, E.J.; Melton, L.J.; Riggs, B.L.; Amin, S.; Khosla, S. Relationship of testosterone and osteocalcin levels during growth. Bone Miner. Res. 2011, 26, 2212–2216. [Google Scholar] [CrossRef] [PubMed]
- Theuwissen, E.; Magdeleyns, E.J.; Braam, L.A.; Teunissen, K.J.; Knapen, M.H.; Binnekamp, I.A.; van Summeren, M.J.; Vermeer, C. Vitamin K status in healthy volunteers. Food Funct. 2014, 5, 229–234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Fracture (n =20) | Non-Fracture (n = 19) | p | ||
|---|---|---|---|---|---|
| Median (Q2) | Q1–Q3 | Median (Q2) | Q1–Q3 | ||
| Age (years) | 12.0 | 8.0–13.0 | 13.5 | 11.0–15.5 | 0.08 |
| Boys | |||||
| n | 14 | 9 | |||
| Girls | |||||
| n | 6 | 10 | |||
| Weight (kg) | 45.7 | 26.3–55.5 | 60.5 | 41.0–67.0 | 0.04 |
| Bone markers | |||||
| BALP, ng/mL | 37.19 | 30.75–53.30 | 50.75 | 36.39–114.5 | 0.06 |
| NTX, ng/mL | 0.483 | 0.438–0.546 | 0.523 | 0.469–0.732 | 0.13 |
| Undercarboxylated osteocalcin (ucOC), ng/mL | |||||
| Median | 10.104 | 9.356–10.350 | 10.252 | 9.677–10.552 | 0.16 |
| Carboxylated osteocalcin (cOC), ng/mL | |||||
| Median | 20.866 | 16.390–23.612 | 42.762 | 29.980–48.808 | <0.0001 |
| UCR (ucOC/cOC) | 0.471 | 0.404–0.605 | 0.245 | 0.202–0.348 | <0.0001 |
| Vitamin D (reference value range 30–74 ng/mL) | 18.00 | 10.00–30.00 | 25.00 | 15.50–32.50 | 0.22 |
| Concentration Ca mmol/L (reference value range 1.10–150 mmol/L) | 1.25 | 1.18–1.36 | 1.23 | 1.23–1.32 | 0.81 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popko, J.; Karpiński, M.; Chojnowska, S.; Maresz, K.; Milewski, R.; Badmaev, V.; Schurgers, L.J. Decreased Levels of Circulating Carboxylated Osteocalcin in Children with Low Energy Fractures: A Pilot Study. Nutrients 2018, 10, 734. https://doi.org/10.3390/nu10060734
Popko J, Karpiński M, Chojnowska S, Maresz K, Milewski R, Badmaev V, Schurgers LJ. Decreased Levels of Circulating Carboxylated Osteocalcin in Children with Low Energy Fractures: A Pilot Study. Nutrients. 2018; 10(6):734. https://doi.org/10.3390/nu10060734
Chicago/Turabian StylePopko, Janusz, Michał Karpiński, Sylwia Chojnowska, Katarzyna Maresz, Robert Milewski, Vladimir Badmaev, and Leon J. Schurgers. 2018. "Decreased Levels of Circulating Carboxylated Osteocalcin in Children with Low Energy Fractures: A Pilot Study" Nutrients 10, no. 6: 734. https://doi.org/10.3390/nu10060734
APA StylePopko, J., Karpiński, M., Chojnowska, S., Maresz, K., Milewski, R., Badmaev, V., & Schurgers, L. J. (2018). Decreased Levels of Circulating Carboxylated Osteocalcin in Children with Low Energy Fractures: A Pilot Study. Nutrients, 10(6), 734. https://doi.org/10.3390/nu10060734