Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Analytical Approach
2.2. Intervention Effect Size
2.3. Health Benefit Modelling
2.4. Intervention Costs
2.5. Cost-Effectiveness Modelling
3. Results
3.1. Intervention Effect Size
3.2. Cost-Effectiveness Modelling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani, A.; Ziaee, A.; Oveisi, S.; Afaghi, A. A Comparison of Health-Related Quality of Life among Normal-Weight, Overweight and Obese Adults in Qazvin Metabolic Diseases Study (QMDS), Iran: Health-Related Quality of Life among Obese Adults. Glob. J. Health Sci. 2013, 5, 156. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M. What is the economic case for treating obesity? Obes. Res. 1998, 6 (Suppl. 1), 2s–7s. [Google Scholar] [CrossRef] [PubMed]
- Trogdon, J.G.; Finkelstein, E.A.; Hylands, T.; Dellea, P.S.; Kamal-Bahl, S.J. Indirect costs of obesity: A review of the current literature. Obes. Rev. 2008, 9, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Goettler, A.; Grosse, A.; Sonntag, D. Productivity loss due to overweight and obesity: A systematic review of indirect costs. BMJ Open 2017, 7, e014632. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Health Expenditure Australia 2012–13; AIHW: Canberra, Australia, 2014. [Google Scholar]
- Price Waterhouse Coopers. Weighing the Cost of Obesity: A Case for Action; PWC: Canberra, Australia, 2015. [Google Scholar]
- Mustajoki, P. Obesogenic food environment explains most of the obesity epidemic. Duodecim 2015, 131, 1345–1352. [Google Scholar] [PubMed]
- Mejean, C.; Macouillard, P.; Péneau, S.; Hercberg, S.; Castetbon, K. Consumer acceptability and understanding of front-of-pack nutrition labels. J. Hum. Nutr. Diet. 2013, 26, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Mejean, C.; Macouillard, P.; Péneau, S.; Hercberg, S.; Castetbon, K. Perception of front-of-pack labels according to social characteristics, nutritional knowledge and food purchasing habits. Public Health Nutr. 2013, 16, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Feunekes, G.I.; Gortemaker, I.A.; Willems, A.A.; Lion, R.; Van Den Kommer, M. Front-of-pack nutrition labelling: Testing effectiveness of different nutrition labelling formats front-of-pack in four European countries. Appetite 2008, 50, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Crino, M.; Dunford, E.; Gao, A.; Greenland, R.; Li, N.; Ngai, J.; Ni Mhurchu, C.; Pettigrew, S.; Sacks, G.; et al. Effects of Different Types of Front-of-Pack Labelling Information on the Healthiness of Food Purchases-A Randomised Controlled Trial. Nutrients 2017, 9, 1284. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, R.; McNeill, L. Does the Australasian “Health Star Rating” Front of Pack Nutritional Label System Work? Nutrients 2016, 8, 327. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.; Warin, L. Impact of food labelling systems on food choices and eating behaviours: A systematic review and meta-analysis of randomized studies. Obes. Rev. 2016, 17, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Rayner, M.; Wood, A.; Lawrence, M.; Mhurchu, C.N.; Albert, J.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; Kumanyika, S.; et al. Monitoring the health-related labelling of foods and non-alcoholic beverages in retail settings. Obes. Rev. 2013, 14 (Suppl. 1), 70–81. [Google Scholar] [CrossRef] [PubMed]
- Cowburn, G.; Stockley, L. Consumer understanding and use of nutrition labelling: A systematic review. Public Health Nutr. 2005, 8, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Campos, S.; Doxey, J.; Hammond, D. Nutrition labels on pre-packaged foods: A systematic review. Public Health Nutr. 2011, 14, 1496–1506. [Google Scholar] [CrossRef] [PubMed]
- Ni Mhurchu, C.; Volkova, E.; Jiang, Y. Effects of interpretive nutrition labels on consumer food purchases: The Starlight randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 695–704. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Vyth, E.L.; Steenhuis, I.H.; Roodenburg, A.J.; Brug, J.; Seidell, J.C. Front-of-pack nutrition label stimulates healthier product development: A quantitative analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Young, L.R.; Nestle, M. The contribution of expanding portion sizes to the US obesity epidemic. Am. J. Public Health 2002, 92, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Dummer, J. Sodium reduction in Canadian food products with the health check program. Can. J. Diet. Pract. Res. 2012, 73, e227–e232. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.A.; Roe, L.S.; Rolls, B.J. Assessment of satiety depends on the energy density and portion size of the test meal. Obesity 2014, 22, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Health Star Rating Advisory Committee. About Health Star Ratings. 2014. Available online: http://healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/content/About-health-stars (accessed on 18 March 2018).
- Siegrist, M.; Leins-Hess, R.; Keller, C. Which front-of-pack nutrition label is the most efficient one? The results of an eye-tracker study. Food Qual. Prefer. 2015, 39, 183–190. [Google Scholar] [CrossRef]
- Young, L.; Swinburn, B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Promot. Int. 2002, 17, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; McMahon, A.; Boustead, R. A case study of sodium reduction in breakfast cereals and the impact of the Pick the Tick food information program in Australia. Health Promot. Int. 2003, 18, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.W.; Bello, N.M.; Sundar, R.P.; Peltier, C.; Bix, L. Front of pack labels enhance attention to nutrition information in novel and commercial brands. Food Policy 2015, 56, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Mhurchu, C.; Eyles, H.; Choi, Y.-H. Effects of a Voluntary Front-of-Pack Nutrition Labelling System on Packaged Food Reformulation: The Health Star Rating System in New Zealand. Nutrients 2017, 9, 918. [Google Scholar] [CrossRef] [PubMed]
- Health Star Rating Advisory Committee. Two Year Progress Review Report on the Implementation of the Health Star Rating System—June 2014–June 2016. Available online: http://healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/reviews (accessed on 8 May 2017).
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Int. J. Technol. Assess. Health Care 2013, 29, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Ello-Martin, J.A.; Ledikwe, J.H.; Rolls, B.J. The influence of food portion size and energy density on energy intake: Implications for weight management. Am. J. Clin. Nutr. 2005, 82 (Suppl. 1), 236s–241s. [Google Scholar] [CrossRef] [PubMed]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400–2409. [Google Scholar] [CrossRef]
- Swinburn, B.; Sacks, G.; Vandevijvere, S.; Kumanyika, S.; Lobstein, T.; Neal, B.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; et al. INFORMAS (International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support): Overview and key principles. Obes. Rev. 2013, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Dunford, E.; Trevena, H.; Goodsell, C.; Ng, K.H.; Webster, J.; Millis, A.; Goldstein, S.; Hugueniot, O.; Neal, B. FoodSwitch: A Mobile Phone App to Enable Consumers to Make Healthier Food Choices and Crowdsourcing of National Food Composition Data. JMIR mHealth uHealth 2014, 2, e37. [Google Scholar] [CrossRef] [PubMed]
- Dunford, E.; Webster, J.; Metzler, A.B.; Czernichow, S.; Mhurchu, C.N.; Wolmarans, P.; Snowdon, W.; L’Abbe, M.; Li, N.; Maulik, P.K.; et al. International collaborative project to compare and monitor the nutritional composition of processed foods. Eur. J. Prev. Cardiol. 2012, 19, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey 2011–12; ABS: Canberra, Australia, 2015.
- Hall, K.D.; Butte, N.F.; Swinburn, B.A.; Chow, C.C. Dynamics of childhood growth and obesity: Development and validation of a quantitative mathematical model. Lancet Diabet. Endocrinol. 2013, 1, 97–105. [Google Scholar] [CrossRef]
- Mantilla Herrera, A.M.; Erskine, H.E.; Ananthapavan, J.; Sacks, G.; Whiteford, H.; Barendregt, J.J.; Lee, Y.Y. Health economic evaluation of obesity interventions: The development and validation of the Centre for Research Excellence in Obesity Policy and Food Systems model (the CRE-Obesity model). 2017. submitted. [Google Scholar]
- Barendregt, J.J.; Van Oortmarssen, G.J.; Van Hout, B.A.; Van Den Bosch, J.M.; Bonneux, L. Coping with multiple morbidity in a life table. Math. Popul. Stud. 1998, 7, 29–49. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Stevenson, D.; Fryback, D.G. HALYs and QALYs and DALYs, Oh My: Similarities and Differences in Summary Measures of Population Health. Annu. Rev. Public Health 2002, 23, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Mantilla-Herrera, A.; Veerman, L.; Backholer, K.; Sacks, G.; Moodie, M.; Siahpush, M.; Carter, R.; Peeters, A. Equity and cost-effectiveness of a sugar sweetened beverage tax across socioeconomic groups. PLoS Med. 2017, 14, e1002326. [Google Scholar] [CrossRef] [PubMed]
- Brown, V.; Moodie, M.; Cobiac, L.; Herrera, A.M.; Carter, R. Obesity-related health impacts of fuel excise taxation—An evidence review and cost-effectiveness study. BMC Public Health 2017, 17, 359. [Google Scholar] [CrossRef] [PubMed]
- Brown, V.; Moodie, M.; Herrera, A.M.; Veerman, J.L.; Carter, R. Active transport and obesity prevention—A transportation sector obesity impact scoping review and assessment for Melbourne, Australia. Prev. Med. 2017, 96, 49–66. [Google Scholar] [CrossRef] [PubMed]
- PricewaterhouseCoopers. Health Star Rating System: Cost Benefit Analysis; PWC: Canberra, Australia, 2014. [Google Scholar]
- PricewaterhouseCoopers. Food Standards Australia New Zealand: Cost Schedule for Food Labelling Changes—Final Report; PWC: Canberra, Australia, 2008. [Google Scholar]
- Australian Institute of Health and Welfare. Disease Costs and Impacts Study Data; AIHW: Canberra, Australia, 2001.
- Robertson, K. Independent Study: Why Label Changes Don’t Affect Food Prices. 2013. Available online: http://www.justlabelit.org/wp-content/uploads/2013/09/Kai-Roberston-Food-Labeling-Study-2013.pdf (accessed on 30 April 2018).
- Australian Institute of Health and Welfare. Health Expenditure Australia 2014-15. Health and Welfare Expenditure Series No. 57. Cat. No. HWE 67; AIHW: Canberra, Australia, 2016.
- Harris, A.H.; Hill, S.R.; Chin, G.; Li, J.J.; Walkom, E. The role of value for money in public insurance coverage decisions for drugs in Australia: A retrospective analysis 1994–2004. Med. Decis. Mak. 2008, 28, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.H.; Weinstein, M.C.; Fenwick, E.A.; Karnon, J.; Sculpher, M.J.; Paltiel, A.D. Model parameter estimation and uncertainty: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-6. Value Health 2012, 15, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modelling for Health Economic Evaluation; OUP Oxford: Oxford, UK, 2006. [Google Scholar]
- EpiGear International. Ersatz Version 1.3. 2016. Available online: http://www.epigear.com/index_files/ersatz.html (accessed on 10 March 2016).
- Briggs, A.; Fenn, P. Confidence intervals or surfaces? Uncertainty on the cost-effectiveness plane. Health Econ. 1998, 7, 723–740. [Google Scholar] [CrossRef]
- EpiGear International. Ersatz User Guide Version 1.35. Available online: https://www.epigear.com/Products/EpigearXL/epigearxl.html (accessed on 18 March 2018).
- Veerman, J.L.; Barendregt, J.J.; Beeck, E.F.; Seidell, J.C.; Mackenbach, J.P. Stemming the obesity epidemic: A tantalizing prospect. Obesity 2007, 15, 2365–2370. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013, 380, 2224–2260. [Google Scholar] [CrossRef]
- Sacks, G.; Veerman, J.L.; Moodie, M.; Swinburn, B. ‘Traffic-light’nutrition labelling and ‘junk-food’tax: A modelled comparison of cost-effectiveness for obesity prevention. Int. J. Obes. 2011, 35, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Crino, M.; Herrera, A.M.M.; Ananthapavan, J.; Wu, J.H.; Neal, B.; Lee, Y.Y.; Zheng, M.; Lal, A.; Sacks, G. Modelled Cost-Effectiveness of a Package Size Cap and a Kilojoule Reduction Intervention to Reduce Energy Intake from Sugar-Sweetened Beverages in Australia. Nutrients 2017, 9, 983. [Google Scholar] [CrossRef] [PubMed]
- Vyth, E.L.; Steenhuis, I.H.; Brandt, H.E.; Roodenburg, A.J.; Brug, J.; Seidell, J.C. Methodological quality of front-of-pack labeling studies: A review plus identification of research challenges. Nutr. Rev. 2012, 70, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.H. Handling uncertainty in cost-effectiveness models. Pharmacoeconomics 2000, 17, 479–500. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.A.; Dickie, S.; Woods, J.L. Do Nutrient-Based Front-of-Pack Labelling Schemes Support or Undermine Food-Based Dietary Guideline Recommendations? Lessons from the Australian Health Star Rating System. Nutrients 2018, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- System, H.S.R. Formal Review of the System after Five Years of Implementation (June 2014 to June 2019). Available online: http://healthstarrating.gov.au/internet/healthstarrating/publishing.nsf/Content/formal-review-of-the-system-after-five-years (accessed on 26 March 2018).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Costing Items | Value in 2010 A$ | |
|---|---|---|
| Voluntary | Mandatory | |
| 1. Cost to industry a | 2.5 m (1.2 m, 3.7 m) | 37.0 m (18.5 m, 55.4 m) |
| 2. Cost to government b | 1.2 m (0.6 m, 1.8 m) | 17.8 m (8.9 m, 26.7 m) |
| 2.1 Cost of legislation c | not applicable | 1.1 m (1.0 m, 1.2 m) |
| Input Parameters | Uncertainty Distribution | Assumptions | Data Sources |
|---|---|---|---|
| Change in weight resulting from the intervention | Normal | The point estimate was the mean obtained from the data source. A standard deviation was assigned to this point estimate that was equal to the mean in the absence of relevant data. | Based on data from the Food Switch database and the Australian Health survey |
| Intervention costs to industry | Pert | The point estimate (obtained from the data source) was assigned a range of likely minimum and maximum values based on expert opinion. | Based on the projected costs from the HSR report [24] |
| Intervention costs to government | Pert | The point estimate (obtained from the data source) was assigned a range of likely minimum and maximum values based on expert opinion [53,56]. | Based on the projected costs from the HSR report [24]. Costs to the government related to passing a legislation were only applied to the mandatory scenario and were modelled using a gamma distribution [43] |
| 2010 Australian population BMI by age and sex | Lognormal | The mean and standard deviation for each population cohort (by age and sex) was obtained from the data source. A lognormal distribution was used to: restrict the occurrence of values between the interval [0, +∞]; and account for the positively skewed BMI distribution observed in the population [57]. | Sourced from the Australian Bureau of Statistics [38] |
| Relative risks of obesity-related diseases per 5-unit increase of BMI | Lognormal | The mean was obtained from the data source and the standard deviation was calculated as the lognormal of the mean. A lognormal distribution was used to restrict the occurrence of values between [0, +∞]. | Sourced from the Global Burden of Disease study [58] |
| Food Category | Average Energy Density (kJ per 100 g) in 2013 | Average Energy Density (kJ per 100 g) in 2016 | Change in Average Energy Density between 2013 and 2016 | % Change in kJ per 100 g (from Baseline) | % Change in kJ per 100 g Attributable to HSR | ||||
|---|---|---|---|---|---|---|---|---|---|
| With HSR | Without HSR | With HSR | Without HSR | With HSR | Without HSR | With HSR | Without HSR | ||
| Bread and bakery products | 1585 | 1588 | 1581 | 1586 | −3.3 | −2.2 | −0.2 | −0.1 | −0.1 |
| Cereal and grain products | 1521 | 1370 | 1513 | 1360 | −7.9 | −10.4 | −0.5 | −0.8 | 0.2 |
| Confectionery | 2070 | 1720 | 2089 | 1724 | 19.7 | 4.0 | 1.0 | 0.2 | 0.7 |
| Convenience foods | 444 | 512 | 433 | 509 | −10.9 | −3.2 | −2.5 | −0.6 | −1.8 |
| Dairy | 608 | 933 | 594 | 932 | −13.4 | −0.9 | −2.2 | −0.1 | −2.1 |
| Edible oils and oil emulsions | 2724 | 3066 | 2706 | 3071 | −18.1 | 5.0 | −0.7 | 0.2 | −0.8 |
| Fish and fish products | 721 | 693 | 720 | 693 | −1.0 | 0.0 | −0.1 | 0.0 | −0.1 |
| Fruit and vegetables | 881 | 998 | 881 | 999 | −0.6 | 0.6 | −0.1 | 0.1 | −0.1 |
| Meat and meat products | 828 | 878 | 824 | 882 | −4.1 | 3.9 | −0.5 | 0.4 | −0.9 |
| Non-alcoholic beverages | 213 | 197 | 208 | 195 | −4.6 | −2.1 | −2.1 | −1.1 | −1.1 |
| Sauces, dressings, spreads and dips | 1046 | 816 | 981 | 810 | −64.7 | −5.5 | −6.2 | −0.7 | −5.5 |
| Snack foods | 2013 | 1883 | 2079 | 1882 | 65.8 | −0.8 | 3.3 | 0.0 | 3.3 |
| Sugars, honey and related products | 1454 | 1404 | 1435 | 1406 | −19.7 | 1.6 | −1.4 | 0.1 | −1.5 |
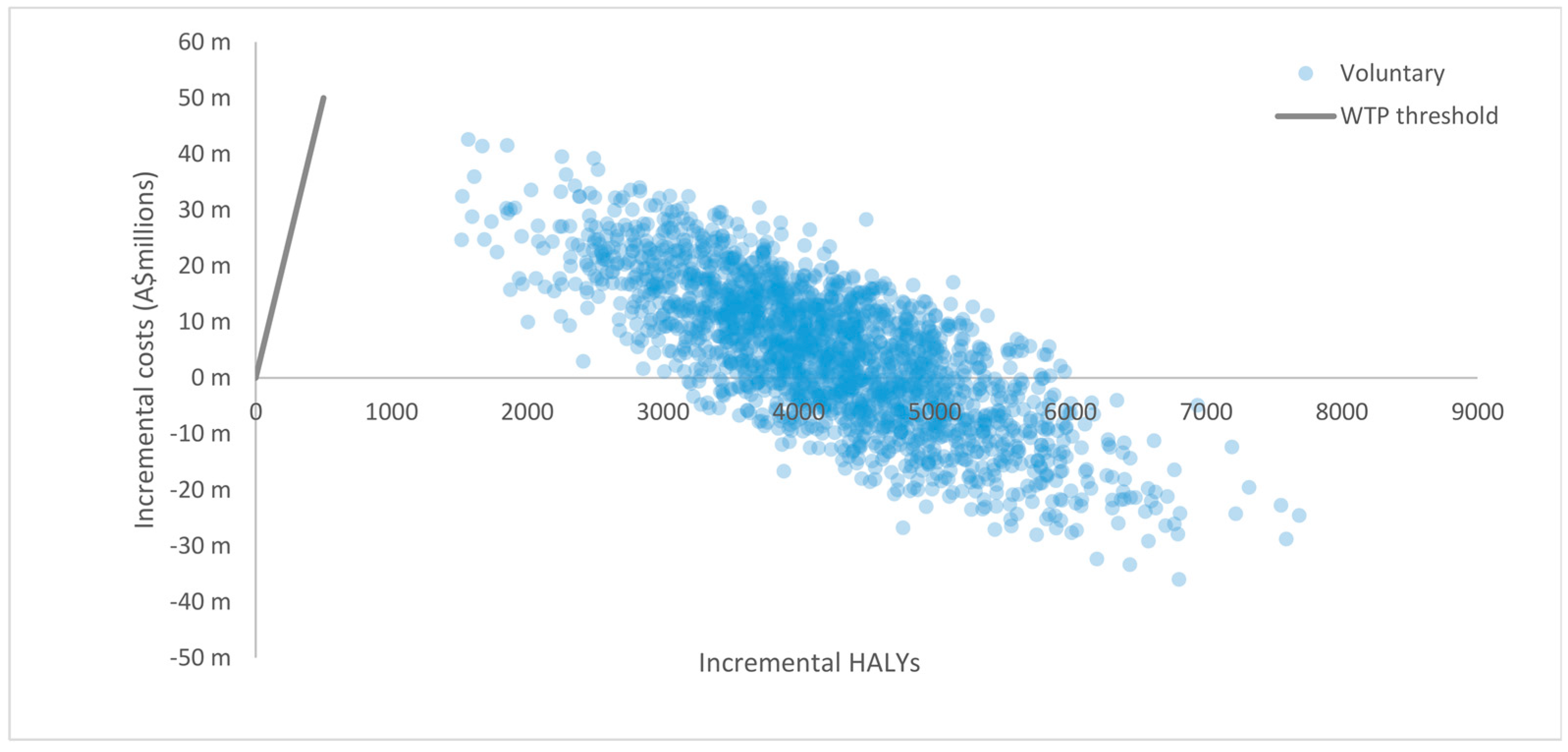
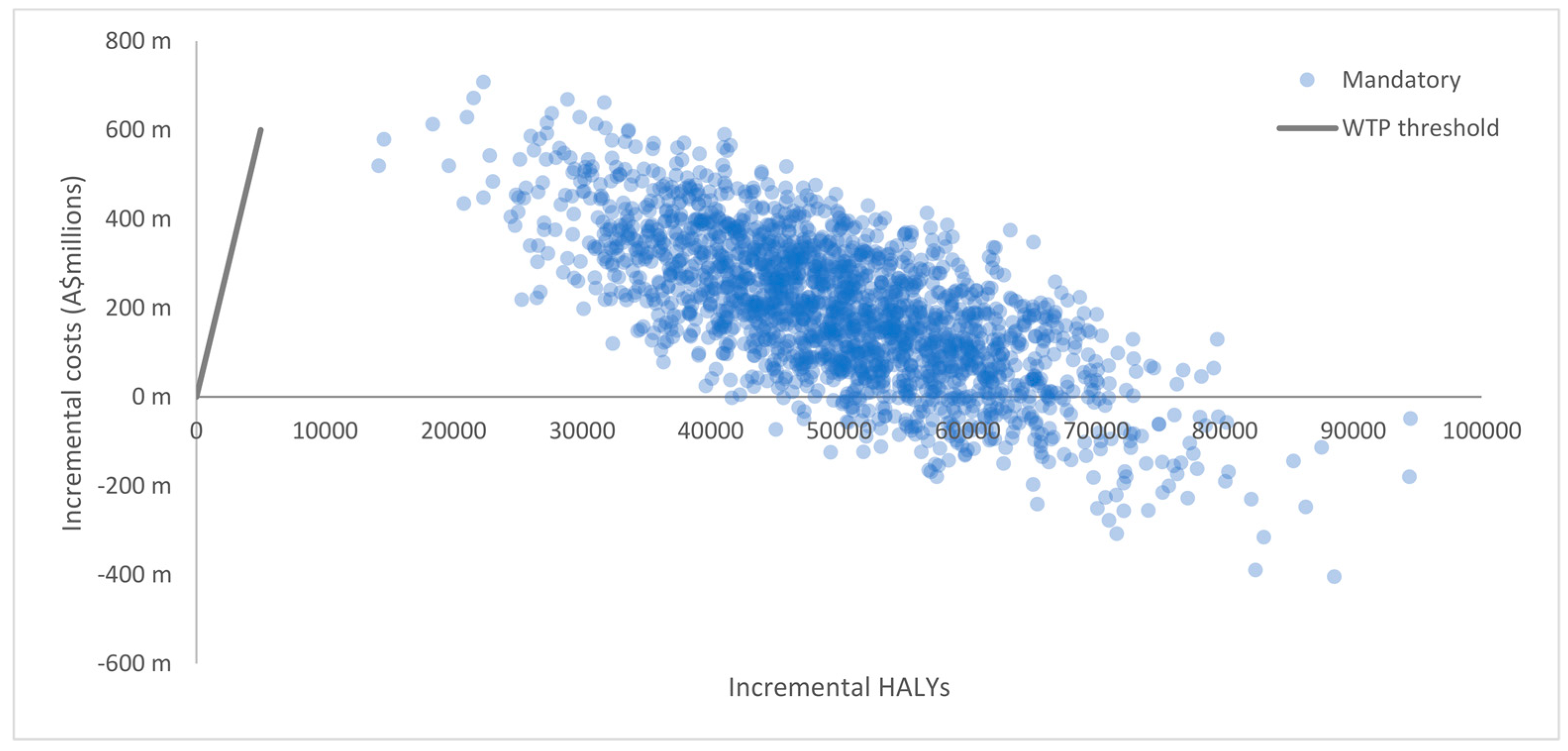
| Outputs | Voluntary Scenario * (6.7% HSR Uptake) | Mandatory Scenario * (100% HSR Uptake) |
|---|---|---|
| Incremental intervention costs (95% UI) in 2010 A$ millions | 46.1 m (32.0 m to 60.2 m) | 686.4 m (483.5 m to 894.9 m) |
| Cost offsets ** (95% UI) in 2010 A$ millions | −41.6 m (−61.6 m to −22.1 m) | −488.7 m (−722.8 m to −265.9 m) |
| Net incremental costs (95% UI) in 2010 A$ millions | 4.5 m (−21.2 m to 28.2 m) | 197.7 m (−123.2 m to 513.3 m) |
| Incremental HALYs (95% UI) | 4207 (2438 to 6081) | 49,949 (29,291 to 72,153) |
| Mean ICER (95% UI) in 2010 A$ per HALY | 1728 (dominant to 10,445) | 4752 (dominant to 16,236) |
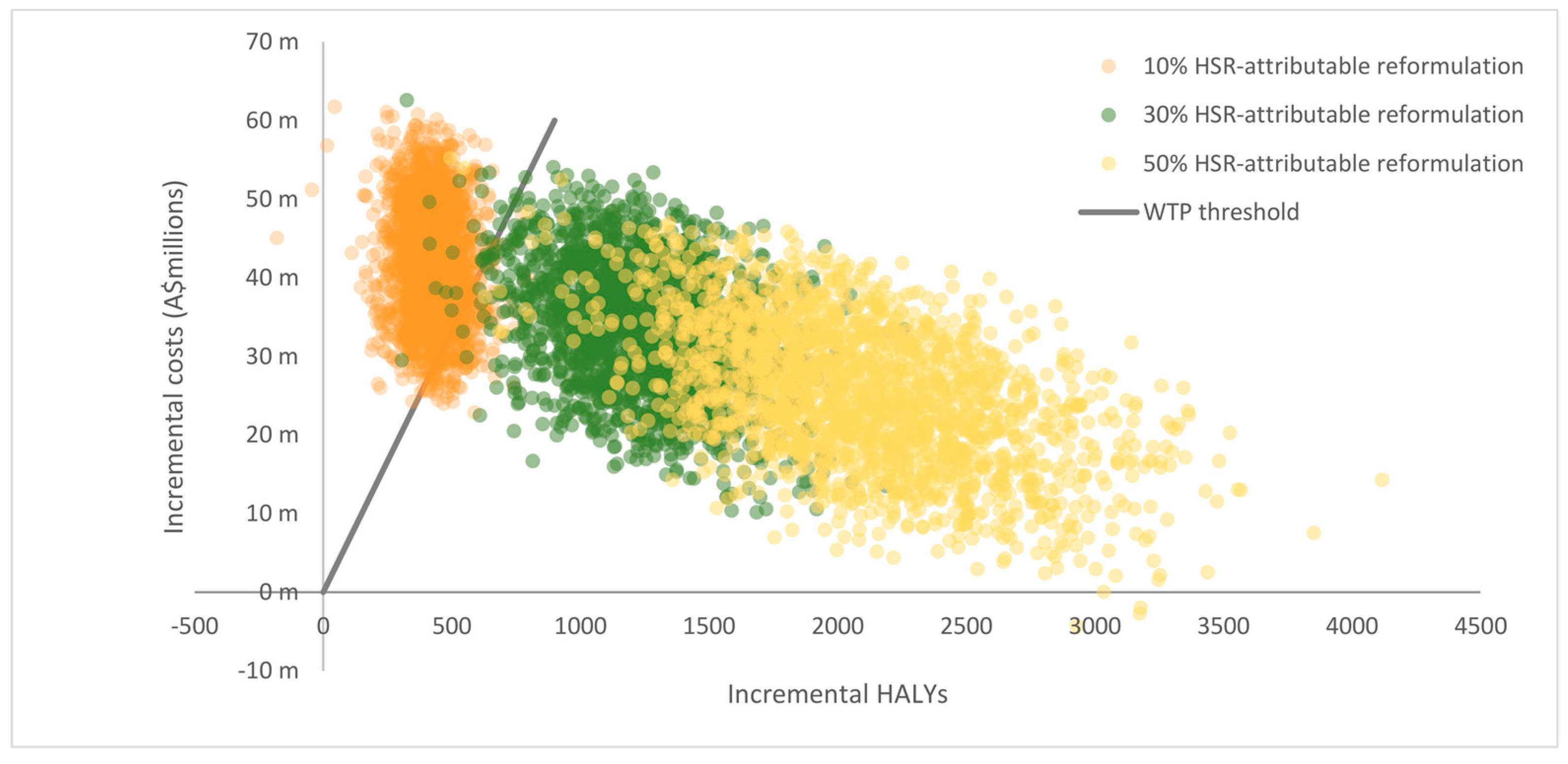
| Outputs | 50% HSR-Attributable Reformulation | 30% HSR-Attributable Reformulation | 10% HSR-Attributable Reformulation |
|---|---|---|---|
| Incremental intervention costs (95% UI) in A$ millions | 46.1 m (32.0 m to 59.7 m) | 46.0 m (31.7 m to 59.9 m) | 46.0 m (32.4 m to 60.0 m) |
| Cost offsets (95% UI) in A$ millions | −20.9 m (−31.4 m to −11.3 m) | −12.5 m (−18.3 m to −6.5 m) | −4.2 m (−6.3 m to −2.2 m) |
| Net incremental costs (95% UI) in A$ millions | 25.3 m (7.9 m to 42.4 m) | 33.5 m (18.0m to 48.5 m) | 41.8 m (28.2 m to 56.2 m) |
| Incremental HALYs (95% UI) | 2101 (1226 to 3116) | 1253 (702 to 1840) | 424 (235 to 618) |
| Mean ICER (95% UI) A$ per HALY | 13,374 (3044 to 31,940) | 29,006 (11,427 to 59,863) | 106,368 (54,072 to 191,145) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantilla Herrera, A.M.; Crino, M.; Erskine, H.E.; Sacks, G.; Ananthapavan, J.; Mhurchu, C.N.; Lee, Y.Y. Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia. Nutrients 2018, 10, 614. https://doi.org/10.3390/nu10050614
Mantilla Herrera AM, Crino M, Erskine HE, Sacks G, Ananthapavan J, Mhurchu CN, Lee YY. Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia. Nutrients. 2018; 10(5):614. https://doi.org/10.3390/nu10050614
Chicago/Turabian StyleMantilla Herrera, Ana Maria, Michelle Crino, Holly E. Erskine, Gary Sacks, Jaithri Ananthapavan, Cliona Ni Mhurchu, and Yong Yi Lee. 2018. "Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia" Nutrients 10, no. 5: 614. https://doi.org/10.3390/nu10050614
APA StyleMantilla Herrera, A. M., Crino, M., Erskine, H. E., Sacks, G., Ananthapavan, J., Mhurchu, C. N., & Lee, Y. Y. (2018). Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia. Nutrients, 10(5), 614. https://doi.org/10.3390/nu10050614