Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015


 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection
2.3. Assessment of Dietary Zinc Intake
2.4. Grouping Standards
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Dietary Zinc Intake
3.3. Dietary Zinc Intake Level
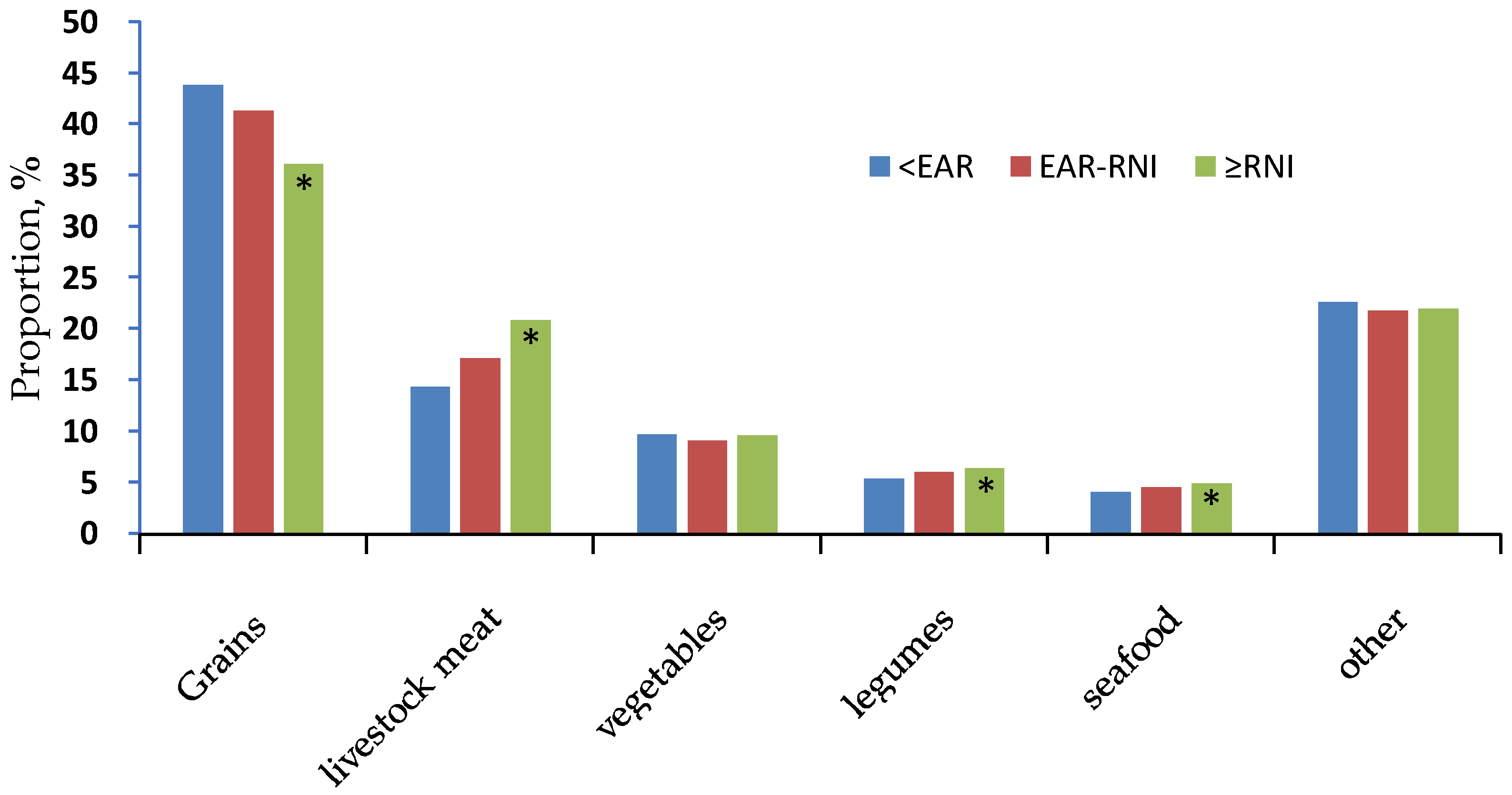
3.4. Food Sources of Dietary Zink
3.5. Relationship between Dietary Zinc Intake and Metabolic Syndrome Indicators
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gibson, R.S.; Ferguson, E.L. An Interactive 24-Hour Recall for Assessing the Adequacy of Iron and Zinc Intakes in Developing Countries; ILSI Press: Washington, DC, USA, 2015. [Google Scholar]
- Zhai, F.-Y.; Yang, X.G. Report on Nutrition and Health Status of Chinese Residents—Dietary and Nutrient Intake in 2002; People’s Health Press: Beijing, China, 2006. [Google Scholar]
- Liu, S.; Li, J.; Song, Y.; Gong, C.-R.; Cheng, M.-W. Dietary intake of zinc and its changing trend among residents in Hubei Province, 1991–2011. Pract. Prev. Med. 2017, 7, 797–800. [Google Scholar] [CrossRef]
- Du, W.; Wang, H.; Chen, S.; Su, C.; Zhang, H.; Zhang, B. Trend of dietary nutrient intake among adult females in 9 provinces in China, 2000–2011. Chin. J. Epidemiol. 2015, 36, 715–719. [Google Scholar] [CrossRef]
- Zhang, J.-G.; Zhang, B.; Wang, H.-J.; Wang, Z.-H.; Du, W.-W.; Su, C.; Zhang, J.; Zhai, F.-Y. Zinc intake trend of Chinese adults aged 50–79 in nine provinces (autonomous regions) from 1991 to 2009. Chin. J. Health Educ. 2012, 28, 707–709. [Google Scholar]
- Zhang, J.-G.; Zhang, B.; Wang, H.-J.; Du, W.-W.; Su, C.; Zhai, F.-Y. Nutrients intake trend of Chinese population in nine provinces from 1989-2009 (VII) Zinc intake trend of Chinese adults aged 18–49 years. Acta Nutr. Sin. 2012, 34, 111–113. [Google Scholar]
- Wang, Z.-H.; Zhai, F.-Y.; He, Y.-N.; Hu, Y.-S.; Wang, H.-J. Dietary zinc intake of Chinese residents and the trend of change. J. Hyg. Res. 2006, 35, 485–486. [Google Scholar] [CrossRef]
- Yu, D.M.; He, Y.N.; Guo, Q.Y.; Fang, H.Y.; Xu, X.L.; Fang, Y.H.; Li, J.; Zhao, L.Y. Trends of energy and nutrients intake among Chinese population in 2002–2012. J. Hyg. Res. 2016, 45, 527–533. [Google Scholar]
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of nutrition for development (bond)-zinc review. J. Nutr. 2016, 146, 858S–885S. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.; Cousins, R.J. Zinc. In Modern Nutrition in Health and Disease, 10th ed.; Shils, M.E., Shike, M., Ross, A.C., Caballero, B., Cousins, R.J., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 271–285. [Google Scholar]
- Prasad, A.S. Discovery and importance of zinc in human nutrition. Fed. Proc. 1984, 43, 2829–2834. [Google Scholar] [PubMed]
- Samman, S. Zinc. Nutr. Diet. 2007, 64, S131–S134. [Google Scholar] [CrossRef]
- Prasad, A.S. Zinc: An overview. Nutrition 1995, 11, 93–99. [Google Scholar] [PubMed]
- Vallee, B.L.; Falchuk, K.H. The biochemical basis of zinc physiology. Physiol. Rev. 1993, 73, 79–118. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.R. The antioxidant properties of zinc. J. Nutr. 2000, 130, 1447S–1454S. [Google Scholar] [CrossRef] [PubMed]
- Hennig, B.; Wang, Y.; Ramasamy, S.; McClain, C.J. Zinc deficiency alters barrier function of cultured porcine endothelial cells. J. Nutr. 1992, 122, 1242–1247. [Google Scholar] [CrossRef] [PubMed]
- Freitas, E.P.; Cunha, A.T.; Aquino, S.L.; Pedrosa, L.F.; Lima, S.C.; Lima, J.G.; Almeida, M.G.; Sena-Evangelista, K. Zinc Status Biomarkers and Cardiometabolic Risk Factors in Metabolic Syndrome: A Case Control Study. Nutrients 2017, 9, 175. [Google Scholar] [CrossRef] [PubMed]
- Olechnowicz, J.; Tinkov, A.; Skalny, A.; Suliburska, J. Zinc status is associated with inflammation, oxidative stress, lipid, and glucose metabolism. J. Physiol. Sci. 2018, 68, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Trame, S.; Wessels, I.; Haase, H.; Rink, L. A short 18 items food frequency questionnaire biochemically validated to estimate zinc status in humans. J. Trace Elem. Med. Biol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obesity Rev. 2014, 15 (Suppl. 1), 2–7. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, G.; Pan, X. Chinese Food Composition Table, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Chinese Nutrition Society. Chinese Dietary Reference Intakes 2013; Science Press: Beijing, China, 2014; pp. 106–108. ISBN 978-7-03-041401-4. [Google Scholar]
- Zhang, Z.-Z. Evolution and Evaluation of the Chinese Economic Regions Division. J. Shanxi Univ. Financ. Econ. (High. Educ. Ed.) 2010, 13, 89–92. [Google Scholar] [CrossRef]
- China’s Nutrition and Health Status Monitoring Comprehensive Report in 2010–2013; Peking University Medical Press: Beijing, China, 2016.
- Ma, G.; Li, Y.; Jin, Y.; Du, S.; Kok, F.J.; Yang, X. Assessment of intake inadequacy and food sources of zinc of people in China. Public Health Nutr. 2007, 10, 848–854. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission Disease Prevention and Control Bureau. Report on Nutrition and Chronic Diseases in China (2015 Report); People’s Health Press: Beijing, China, 2016.
- Lim, K.H.; Riddell, L.J.; Nowson, C.A.; Booth, A.O.; Szymlek-Gay, E.A. Iron and Zinc Nutrition in the Economically-Developed World: A Review. Nutrients 2013, 5, 3184–3211. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.; Goldman, J.; Cleveland, L. What We Eat in America, NHANES 2001–2002: Usual Nutrient Intakes from Food Compared to Dietary Reference Intakes; US Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2005.
- O’Neil, C.E.; Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A. Food sources of energy and nutrients among adults in the US: NHANES 2003–2006. Nutrients 2012, 4, 2097–2120. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture; Agricultural Research Service. 2009–2010 What We Eat in America, NHANES Tables 1–40. 2010. Available online: http://www.ars.usda.gov/SP2UserFiles/Place/12355000/pdf/0910/tables_1-40_2009-2010.pdf (accessed on 29 April 2013).
- Statistics Canada. Canadian Community Health Survey Cycle 2.2, Nutrition 2004; Minister of Health Canada: Ottawa, ON, Canada, 2009.
- University of Otago and Ministry of Health. A Focus on Nutrition: Key Findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011.
- Henderson, L.; Irving, K.; Gregory, J.; Bates, C.; Prentice, A.; Perks, J.; Swan, G.; Farron, M. The National Diet and Nutrition Survey: Adults Aged 19 to 64 Years—Vitamin and Mineral Intake and Urinary Analytes; The Stationery Office: London, UK, 2003. [Google Scholar]
- UK Department of Health. National Diet and Nutrition Survey: Headline Results from Years 1 and 2 (Combined) of the Rolling Programme, 2008/09–2009/10; Headline Results from Years 1 and 2 (Combined) Tables. 2011. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/152237/dh_128556.pdf (accessed on 27 April 2013).
- Olivares, M.; Pizarro, F.; de Pablo, S.; Araya, M.; Uauy, R. Iron, zinc, and copper: Contents in common Chilean foods and daily intakes in Santiago, Chile. Nutrition 2004, 20, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Li, Y.; Jin, Y.; Zhai, F.; Kok, F.J.; Yang, X. Phytate intake and molar ratios of phytate to zinc, iron and calcium in the diets of people in China. Eur. J. Clin. Nutr. 2007, 61, 368. [Google Scholar] [CrossRef] [PubMed]
- Tubek, S. Role of zinc in regulation of arterial blood pressure and in the etiopathogenesis of arterial hypertension. Biol. Trace Elem. Res. 2007, 117, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Tomat, A.L.; Weisstaub, A.R.; Jauregui, A.; Piñeiro, A.; Balaszczuk, A.M.; Costa, M.A.; Arranz, C.T. Moderate zinc deficiency influences arterial blood pressure and vascular nitric oxide pathway in growing rats. Pediatr. Res. 2005, 58, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Bergomi, M.; Rovesti, S.; Vinceti, M.; Vivoli, R.; Caselgrandi, E.; Vivoli, G. Zinc and copper status and blood pressure. J. Trace Elem. Med. Biol. 1997, 11, 166–169. [Google Scholar] [CrossRef]
- Sato, M.; Kurihara, N.; Moridaira, K.; Sakamoto, H.; Tamura, J.; Wada, O.; Yanagisawa, H. Dietary Zn deficiency does not influence systemic blood pressure and vascular nitric oxide signaling in normotensive rats. Biol. Trace Elem. Res. 2003, 91, 157–172. [Google Scholar] [CrossRef]
- Kurihara, N.; Yanagisawa, H.; Sato, M.; Tien, C.K.; Wada, O. Increased renal vascular resistance in zinc-deficient rats: Role of nitric oxide and superoxide. Clin. Exp. Pharmacol. Physiol. 2002, 29, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Taittonen, L.; Nuutinen, M.; Räsänen, L.; Mussalo-Rauhamaa, H.; Turtinen, J.; Uhari, M. Lack of association between copper, zinc, selenium and blood pressure among healthy children. J. Hum. Hypertens. 1997, 11, 429–433. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Aydemir, T.B.; Chang, S.M.; Guthrie, G.J.; Maki, A.B.; Ryu, M.S.; Karabiyik, A.; Cousins, R.J. Zinc transporter ZIP14 functions in hepatic zinc, iron and glucose homeostasis during the innate immune response (endotoxemia). PLoS ONE 2012, 7, e48679. [Google Scholar]
- Sinha, S.; Sen, S. Status of zinc and magnesium levels in type 2 diabetes mellitus and its relationship with glycemic status. Int. J. Diabetes Dev. Ctries. 2014, 34, 220–223. [Google Scholar] [CrossRef]
- Olaniyan, O.O.; Awonuga, M.A.M.; Ajetunmobi, A.F.; Adeleke, I.A.; Fagbolade, O.J.; Olabiyi, K.O.; Oyekanmi, B.A.; Osadolor, H.B. Serum copper and zinc levels in Nigerian type 2 diabetic patients. Afr. J. Diabetes Med. 2012, 20, 36–38. [Google Scholar]
- Devi, T.R.; Hijam, D.; Dubey, A.; Debnath, S.; Oinam, P.; Devi, N.G.T.; Singh, W.G. Study of serum zinc and copper levels in type 2 diabetes mellitus. Int. J. Contemp. Med. Res. 2016, 3, 2454–7379. [Google Scholar]
- Kaur, J.; Singh, T. Estimation of serum magnesium and zinc levels in type-2 diabetes mellitus. Int. J. Bioassays 2015, 4, 3654–3656. [Google Scholar]
- Yahya, H.; Yahya, K.M.; Saqib, A. Minerals and type 2 diabetes mellitus—Levels of zinc, magnesium and chromium in diabetic and nondiabetic population. Univ. Med. Dent. Coll. 2011, 2, 34–38. [Google Scholar]
- Jyothirmayi, B.; Vasantha, M. Study of zinc and glycated Hb levels in diabetic complications. Int. J. Pharm. Clin. Res. 2015, 7, 360–363. [Google Scholar]
- Kumar, D.A.; Priya, V.S.; Jaiprabhu, J.; Ramalingam, K. Serum copper and zinc levels significance in type 2 diabetic patients. J. Med. Sci. Technol. 2014, 3, 79–81. [Google Scholar]
- Bao, B.; Prasad, A.S.; Beck, F.W.J.; Fitzgerald, J.T.; Snell, D.; Bao, G.W.; Singh, T.; Cardozo, L.J. Zinc decreases C-reactive protein, lipid peroxidation, and inflammatory cytokines in elderly subjects: A potential implication of zinc as an atheroprotective agent. Am. J. Clim. Nutr. 2010, 91, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Baur, L.A.; Cowell, C.T.; Samman, S.; Garnett, S.P. Zinc status, dietary zinc intake and metabolic risk in Australian children and adolescents; Nepean Longitudinal Study. Eur. J. Nutr. 2017, 56, 2407–2414. [Google Scholar] [CrossRef] [PubMed]
- El-Ashmony, S.M.A.; Morsi, H.K.; Abdelhafez, A.M. Effect of zinc supplementation on glycemic control, lipid profile, and renal functions in patients with type II diabetes: A single blinded, randomized, placebo-controlled, trial. J. Biol. Agric. Health 2012, 2, 33–37. [Google Scholar]
- Kanoni, S.; Nettleton, J.A.; Hivert, M.-F.; Ye, Z.; van Rooij, F.J.A.; Shungin, D.; Sonestedt, E.; Ngwal, J.S.; Wojczynski, M.K.; Lemaitre, R.N.; et al. Total zinc intake may modify the glucose-raising effect of a zinc transporter (SLC30A8) variant a 14-cohort meta-analysis. Diabetes 2011, 60, 2407–2416. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.; Attia, J.; Ali, L.; McEvoy, M.; Selim, S.; Sibbritt, D.; Akhter, A.; Akter, S.; Peel, R.; Faruque, O.; et al. Zinc supplementation for improving glucose handling in pre-diabetes: A double-blind randomized placebo controlled pilot study. Diabetes Res. Clin. Pract. 2016, 115, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Karamali, M.; Heidarzadeh, Z.; Seifati, S.M.; Samimi, M.; Tabassi, Z.; Hajijafari, M.; Asemi, Z.; Esmaillzadeh, A. Zinc supplementation and the effects on metabolic status in gestational diabetes: A randomized, double-blind, placebo-controlled trial. J. Diabetes Complic. 2015, 29, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; Rosenkranz, E.; Overbeck, S.; Warmuth, S.; Mocchegiani, E.; Giacconi, R.; Weiskirchen, R.; Karges, W.; Rink, L. Disturbed zinc homeostasis in diabetic patients by in vitro and in vivo analysis of insulinomimetic activity of zinc. J. Nutr. Biochem. 2012, 23, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- Payahoo, L.; Ostadrahimi, A.; Mobasseri, M.; Bishak, Y.K.; Farrin, N.; Jafarabadi, M.A.; Ostadrahimi, A. Effects of zinc supplementation on the anthropometric measurements, lipid profiles and fasting blood glucose in the healthy obese adults. Adv. Pharm. Bull. 2013, 3, 161–165. [Google Scholar] [PubMed]
- El Dib, R.; Gameiro, O.L.; Ogata, M.S.; Mo’dolo, N.S.; Braz, L.G.; Jorge, E.C.; do Nascimento, P., Jr.; Beletate, V. Zinc supplementation for the prevention of type 2 diabetes mellitus in adults with insulin resistance. Cochrane Database Syst. Rev. 2015, 28. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, P.; Wathurapatha, W.S.; Ishara, M.H.; Jayawardana, R.; Galappatthy, P.; Katulanda, P.; Constantine, G.R. Effects of Zinc supplementation on serum lipids: A systematic review and meta-analysis. Nutr. Metab. 2015, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Li, H.T.; Jiao, M.; Chen, J.; Liang, Y. Roles of zinc and copper in modulating the oxidative refolding of bovine copper, zincsuperoxide dismutase. Acta Biochim. Biophys. Sin. (Shanghai) 2010, 42, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Tayeb, W.; Nakbi, A.; Cheraief, I.; Miled, A.; Hammami, M. Alteration of lipid status and lipid metabolism, induction of oxidative stress and lipid peroxidation by 2,4-dichlorophenoxyacetic herbicide in rat liver. Toxicol. Mech. Methods 2013, 23, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Guan, Y.; Shi, X.; Ding, H.; Song, Y.; Li, C.; Liu, R.; Liu, G. Effects of high zinc levels on the lipid synthesis in rat hepatocytes. Biol. Trace Elem. Res. 2013, 154, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Weigand, E.; Egenolf, J. Moderate zinc deficiency does not alter lipid and fatty acid composition in the liver of weanling rats fed diets rich in cocoa butter or safflower oil. J. Nutr. Metab. 2017, 2017, 4798963. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.I.; Siddique, K.U.; Ashfaq, F.; Ali, W.; Reddy, H.D.; Mishra, A. Effect of high-dose zinc supplementation with oral hypoglycemic agents on glycemic control and inflammation in type-2 diabetic nephropathy patients. J. Nat. Sci. Biol. Med. 2013, 4, 336–340. [Google Scholar] [PubMed]
- Gunasekara, P.; Hettiarachchi, M.; Liyanage, C.; Lekamwasam, S. Effects of zinc and multimineral vitamin supplementation on glycemic and lipid control in adult diabetes. Diabetes Metab. Syndr. Obes. 2011, 4, 53–60. [Google Scholar] [PubMed]
- Seo, J.A.; Song, S.W.; Han, K.; Lee, K.J.; Kim, H.N. The associations between serum zinc levels and metabolic syndrome in the Korean population: Findings from the 2010 Korean National Health and Nutrition Examination Survey. PLoS ONE 2010, 9, e105990. [Google Scholar] [CrossRef] [PubMed]
- Jihye, K. Dietary zinc intake is inversely associated with systolic blood pressure in young obese women. Nutr. Res. Pract. 2013, 7, 380–384. [Google Scholar]
- Lowe, N.M.; Medina, M.W.; Stammers, A.L.; Patel, S.; Souverein, O.W.; Dullemeijer, C.; Serra-Majem, L.; Nissensohn, M.; Moran, V.H. The relationship between zinc intake and serum/plasma zinc concentration in adults: A systematic review and dose–response meta-analysis by the EURRECA Network. Br. J. Nutr. 2012, 108, 1962–1971. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.J.; Jia, S.S.; Man, Q.Q.; Song, S.; Li, Y.Q.; Song, P.K.; Zhao, W.H.; Zhang, J. Dietary Cholesterol in the Elderly Chinese Population: An Analysis of CNHS 2010–2012. Nutrients 2017, 9, 934. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Cui, Z.; Li, Y.; Hu, X.; Wang, J.; Yang, X. The survey about the use of dietary supplements by Chinese Adults. Acta Nutr. Sin. 2006, 28, 8–10. [Google Scholar]
- Briefel, R.R.; Bialostosky, K.; Kennedy-Stephenson, J.; McDowell, A.M.; Ervin, R.B.; Wright, J.D. Zinc intake of the US population: Findings from the Third National Health and Nutrition Examination Survey, 1988–1994. J. Nutr. 2000, 130, 1367S–1373S. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group | Male | Female | Total |
|---|---|---|---|
| Total | 5665(47.1) | 6363(52.9) | 12028(100.0) |
| Age, % | |||
| 18–49 | 3127(55.2) | 3561(56.0) | 6688(55.6) |
| 50–64 | 2538(44.8) | 2802(44.0) | 5340(44.4) |
| Region, % | |||
| Country | 2520(44.5) | 2773(43.6) | 5293(44.0) |
| County | 1029(18.2) | 1144(18) | 2173(18.1) |
| Suburb | 948(16.7) | 1064(16.7) | 2012(16.7) |
| City | 1168(20.6) | 1382(21.7) | 2550(21.2) |
| Education, % | |||
| Primary/below | 1126(19.9) | 1929(30.3) # | 3055(25.4) |
| Middle school | 2078(36.7) | 2101(33.0) | 4179(34.7) |
| High school | 1509(26.6) | 1386(21.8) | 2895(24.1) |
| University/above | 952(16.8) | 947(14.9) | 1899(15.8) |
| Income, % | |||
| low | 1804(31.8) | 2196(34.5) # | 4000(33.3) |
| Medium | 1912(33.8) | 2088(32.8) | 4000(33.3) |
| High | 1949(34.4) | 2079(32.7) | 4028(33.5) |
| Area, % | |||
| Western | 2006(35.4) | 2246(35.3) | 4252(35.4) |
| Central | 1511(26.7) | 1676(26.3) | 3187(26.5) |
| Eastern | 2148(37.9) | 2441(38.4) | 4589(38.2) |
| Smoke, % | |||
| No | 2454(43.3) | 6251(98.2) | 8705(72.4) |
| Yes | 3211(56.7) | 112(1.8) | 3323(27.6) |
| Alcohol, % | |||
| No | 2494(44.0) | 5928(93.2) | 8422(70.0) |
| Yes | 3171(56.0) | 435(6.8) | 3606(30.0) |
| BMI, kg/m2 | 24.4 ± 3.7 | 24.0 ± 4.2 * | 24.2 ± 4.0 |
| Energy, kcal/day | 2179.8 ± 733.3 | 1841.9 ± 642.0 * | 2001.1 ± 706.9 |
| Protein, g/day | 67.6 ± 25.5 | 57.0 ± 22.0 * | 62.0 ± 24.3 |
| Carbohydrate, g/day | 276.7 ± 119.6 | 236.7 ± 103.1 * | 255.6 ± 113 |
| Fat, g/day | 86.6 ± 44.7 | 73.8 ± 40.2 * | 79.8 ± 42.9 |
| Systol blood presure, mmHg | 127.4 ± 16.8 | 122.8 ± 18.1 * | 124.9 ± 17.7 |
| Diastol blood presure, mmHg | 82.8 ± 11 | 78.9 ± 10.8 * | 80.7 ± 11.1 |
| Fasting glucose, mmol/L | 5.5 ± 1.6 | 5.3 ± 1.3 * | 5.4 ± 1.5 |
| TG, mmol/L | 4.9 ± 1.1 | 4.9 ± 1.1 | 4.9 ± 1.1 |
| Na, mg/day | 5330.2 ± 5419 | 4638.1 ± 5036.8 * | 4964.1 ± 5231.5 |
| Zinc Intake (mg/day) (means ± SD) | Zinc Density (mg/day/1000 kcal) (means ± SD) | |||||
|---|---|---|---|---|---|---|
| Group | Male | Female | Total | Male | Female | Total |
| Total | 11.2 ± 4.2 | 9.4 ± 3.6 | 10.2 ± 4.0 | 5.2 ± 1.3 | 5.2 ± 1.3 | 5.2 ± 1.3 |
| p-values for difference † | <0.001 * | |||||
| Age | ||||||
| 18–49 | 11.4 ± 4.3 | 9.6 ± 3.7 | 10.4 ± 4.1 | 5.3 ± 1.3 | 5.2 ± 1.3 | 5.3 ± 1.3 |
| 50–64 | 10.9 ± 4.0 | 9.2 ± 3.5 | 10.0 ± 3.9 | 5.2 ± 1.3 | 5.1 ± 1.2 | 5.1 ± 1.3 |
| p-values for difference † | <0.001 | <0.001 | <0.001 | <0.05 | <0.001 | <0.001 |
| Region | ||||||
| Country | 11.0 ± 4.2 | 9.2 ± 3.6 | 10.1 ± 4.0 | 5.1 ± 1.2 | 5.0 ± 1.2 | 5.1 ± 1.2 |
| County | 11.0 ± 4.1 | 9.3 ± 3.3 | 10.1 ± 3.8 | 5.2 ± 1.2 | 5.2 ± 1.2 | 5.2 ± 1.2 |
| Suburb | 11.2 ± 4.3 | 9.5 ± 3.9 | 10.3 ± 4.1 | 5.4 ± 1.4 | 5.3 ± 1.4 | 5.3 ± 1.4 |
| City | 11.5 ± 4.1 | 9.8 ± 3.8 | 10.6 ± 4.0 | 5.4 ± 1.4 | 5.4 ± 1.4 | 5.4 ± 1.4 |
| p-values for linear trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Education | ||||||
| Primary/below | 11.0 ± 3.9 | 9.2 ± 3.4 | 9.9 ± 3.7 | 5.2 ± 1.4 | 5.1 ± 1.2 | 5.1 ± 1.3 |
| Middle school | 11.1 ± 4.3 | 9.4 ± 3.8 | 10.3 ± 4.2 | 5.2 ± 1.3 | 5.1 ± 1.3 | 5.1 ± 1.3 |
| High school | 11.2 ± 4.2 | 9.5 ± 3.6 | 10.4 ± 4.0 | 5.2 ± 1.3 | 5.3 ± 1.3 | 5.2 ± 1.3 |
| University/above | 11.5 ± 4.2 | 9.6 ± 3.6 | 10.6 ± 4.0 | 5.5 ± 1.3 | 5.4 ± 1.3 | 5.5 ± 1.3 |
| p-values for linear trend ‡ | <0.05 | <0.05 | <0.001 | <0.001 | <0.001 | <0.001 |
| Income | ||||||
| low | 11.1 ± 4.2 | 9.5 ± 3.8 | 10.2 ± 4.1 | 5.1 ± 1.3 | 5.1 ± 1.3 | 5.1 ± 1.3 |
| Medium | 10.9 ± 4.1 | 9.2 ± 3.5 | 10.0 ± 3.9 | 5.2 ± 1.3 | 5.2 ± 1.2 | 5.2 ± 1.3 |
| High | 11.5 ± 4.2 | 9.5 ± 3.6 | 10.5 ± 4.0 | 5.4 ± 1.3 | 5.3 ± 1.3 | 5.3 ± 1.3 |
| p-values for linear trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Area | ||||||
| Western | 11.3 ± 4.3 | 9.7 ± 3.9 | 10.5 ± 4.1 | 5.2 ± 1.3 | 5.2 ± 1.3 | 5.2 ± 1.3 |
| Central | 11.0 ± 4.1 | 9.1 ± 3.5 | 10.0 ± 3.9 | 5.0 ± 1.3 | 5.0 ± 1.2 | 5.0 ± 1.2 |
| Eastern | 11.1 ± 4.1 | 9.3 ± 3.5 | 10.2 ± 3.9 | 5.3 ± 1.3 | 5.3 ± 1.3 | 5.3 ± 1.3 |
| p-values for linear trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|
| Group | N | <EAR | EAR-RNI | ≥RNI | N | <EAR | EAR-RNI | ≥RNI |
| Total | 5665 | 49.2 | 20.1 | 30.7 | 6363 | 14.8 | 18.3 | 67.0 |
| p-values for difference † | <0.05 * | <0.05 * | ||||||
| Age | ||||||||
| 18–49 | 3127 | 45.9 | 20.7 | 33.5 | 3561 | 13.8 | 17.4 | 68.8 |
| 50–64 | 2538 | 53.3 | 19.4 | 27.3 | 2802 | 16.1 | 19.3 | 64.6 |
| p-values for difference † | <0.05 | <0.05 | <0.05 | <0.05 | ||||
| Region | ||||||||
| Country | 2520 | 50.3 | 19.9 | 29.8 | 2773 | 16.7 | 19.1 | 64.3 |
| County | 1029 | 50.2 | 19.8 | 29.9 | 1144 | 15.1 | 15.9 | 69.0 |
| Suburb | 948 | 49.2 | 20.4 | 30.5 | 1064 | 14.7 | 18.6 | 66.7 |
| City | 1168 | 45.9 | 20.5 | 33.7 | 1382 | 10.8 | 18.4 | 70.8 |
| p-values for trend ‡ | <0.05 | <0.05 | <0.05 | <0.05 | ||||
| Education | ||||||||
| Primary/below | 1126 | 50.1 | 20.7 | 29.2 | 1929 | 16.2 | 18.1 | 65.7 |
| Middle school | 2078 | 49.8 | 20.0 | 30.2 | 2101 | 15.3 | 19.0 | 65.7 |
| High school | 1509 | 50.3 | 19.8 | 29.9 | 1386 | 14.1 | 18.0 | 68.0 |
| University/above | 952 | 45.1 | 20.0 | 35.0 | 947 | 11.8 | 17.4 | 70.8 |
| p-values for trend ‡ | <0.05 | <0.05 | <0.05 | |||||
| Income | ||||||||
| low | 1804 | 50.9 | 19.2 | 29.9 | 2196 | 15.3 | 18.0 | 66.8 |
| Medium | 1912 | 51.1 | 19.6 | 29.3 | 2088 | 16.9 | 18.3 | 64.9 |
| High | 1949 | 45.8 | 21.4 | 32.8 | 2079 | 12.2 | 18.6 | 69.3 |
| p-values for trend ‡ | <0.05 | 0.0497 | <0.05 | |||||
| Area | ||||||||
| Western | 2006 | 47.5 | 19.2 | 33.3 | 2246 | 14.3 | 15.7 | 70.1 |
| Central | 1511 | 50.4 | 20.3 | 29.3 | 1676 | 16.8 | 20.3 | 63.0 |
| Eastern | 2148 | 49.9 | 20.7 | 29.4 | 2441 | 13.9 | 19.3 | 66.8 |
| p-values for trend ‡ | <0.05 | <0.05 | <0.05 | <0.05 | ||||
| Group | Grains | Livestock Meat | Vegetables | Legumes | Seafood | Other |
|---|---|---|---|---|---|---|
| Total | 38.8 | 18.7 | 9.5 | 6.1 | 4.7 | 22.2 |
| Gender | ||||||
| Male | 39.2 | 19.6 | 9.3 | 6.0 | 4.8 | 21.1 |
| Female | 38.4 | 17.8 | 9.8 | 6.3 | 4.7 | 23.0 |
| p-values for difference † | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Age | ||||||
| 18–49 | 38.3 | 19.8 | 9.2 | 5.8 | 4.7 | 22.1 |
| 50–64 | 39.3 | 17.4 | 9.9 | 6.6 | 4.7 | 22.0 |
| p-values for difference † | <0.001 | <0.001 | <0.001 | <0.001 | ||
| Region | ||||||
| Country | 44.2 | 15.3 | 10.3 | 6.9 | 3.9 | 19.5 |
| County | 39.7 | 18.9 | 9.5 | 5.9 | 5.1 | 21.0 |
| Suburb | 36.0 | 20.5 | 10.1 | 6.1 | 4.7 | 22.7 |
| City | 31.2 | 23.0 | 8.1 | 5.2 | 5.7 | 26.8 |
| p-values for trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Education | ||||||
| Primary/below | 44.7 | 14.4 | 10.8 | 7.2 | 3.7 | 19.2 |
| Middle school | 40.8 | 17.7 | 9.9 | 6.6 | 4.2 | 20.8 |
| High school | 36.2 | 20.4 | 9.1 | 5.7 | 5.1 | 23.5 |
| University/above | 31.9 | 23.2 | 8.0 | 4.9 | 6.2 | 25.8 |
| p-values for trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Income | ||||||
| low | 42.7 | 16.7 | 9.3 | 6.6 | 3.9 | 20.8 |
| Medium | 40.7 | 16.6 | 10.6 | 6.5 | 4.5 | 21.0 |
| High | 35.1 | 21.4 | 9.0 | 5.6 | 5.3 | 23.7 |
| p-values for trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |
| Area | ||||||
| Western | 34.1 | 30.4 | 9.8 | 3.3 | 3.8 | 18.6 |
| Central | 43.4 | 17.4 | 11.5 | 6.2 | 3.1 | 18.4 |
| Eastern | 36.0 | 18.8 | 8.2 | 6.3 | 5.8 | 24.9 |
| p-values for trend ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| β | SE | t | P | |
|---|---|---|---|---|
| systolic blood pressure | ||||
| <EAR | ref | |||
| EAR-RNI | 0.506 | 0.4763 | 1.06 | 0.288 |
| ≥RNI | 0.280 | 0.570 | 1.49 | 0.623 |
| diastolic blood pressure | ||||
| <EAR | ref | |||
| EAR-RNI | 0.030 | 0.318 | 0.10 | 0.924 |
| ≥RNI | −0.366 | 0.380 | −0.96 | 0.335 |
| fasting glucose | ||||
| <EAR | ref | |||
| EAR-RNI | −0.120 | 0.067 | −1.78 | 0.075 |
| ≥RNI | −0.155 | 0.080 | −1.93 | 0.054 |
| TG | ||||
| <EAR | ref | |||
| EAR-RNI | 0.083 | 0.063 | 1.31 | 0.190 |
| ≥RNI | 0.219 | 0.076 | 2.90 | 0.004 |
| β | SE | t | P | |
|---|---|---|---|---|
| systolic blood pressure | ||||
| <EAR | ref | |||
| EAR-RNI | 0.268 | 0.550 | 0.49 | 0.627 |
| ≥RNI | 0.413 | 0.546 | 0.76 | 0.450 |
| diastolic blood pressure | ||||
| <EAR | ref | |||
| EAR-RNI | −0.011 | 0.344 | −0.03 | 0.976 |
| ≥RNI | −0.963 | 0.341 | −2.82 | 0.005 |
| fasting glucose | ||||
| <EAR | ref | |||
| EAR-RNI | −0.052 | 0.063 | −0.82 | 0.411 |
| ≥RNI | −0.187 | 0.063 | −2.98 | 0.003 |
| TG | ||||
| <EAR | ref | |||
| EAR-RNI | 0.097 | 0.043 | 2.24 | 0.025 |
| ≥RNI | 0.120 | 0.042 | 2.81 | 0.005 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Jia, X.-F.; Zhang, B.; Wang, Z.-H.; Zhang, J.-G.; Huang, F.-F.; Su, C.; Ouyang, Y.-F.; Zhao, J.; Du, W.-W.; et al. Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015. Nutrients 2018, 10, 572. https://doi.org/10.3390/nu10050572
Wang Y, Jia X-F, Zhang B, Wang Z-H, Zhang J-G, Huang F-F, Su C, Ouyang Y-F, Zhao J, Du W-W, et al. Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015. Nutrients. 2018; 10(5):572. https://doi.org/10.3390/nu10050572
Chicago/Turabian StyleWang, Yun, Xiao-Fang Jia, Bing Zhang, Zhi-Hong Wang, Ji-Guo Zhang, Fei-Fei Huang, Chang Su, Yi-Fei Ouyang, Jian Zhao, Wen-Wen Du, and et al. 2018. "Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015" Nutrients 10, no. 5: 572. https://doi.org/10.3390/nu10050572
APA StyleWang, Y., Jia, X.-F., Zhang, B., Wang, Z.-H., Zhang, J.-G., Huang, F.-F., Su, C., Ouyang, Y.-F., Zhao, J., Du, W.-W., Li, L., Jiang, H.-R., Zhang, J., & Wang, H.-J. (2018). Dietary Zinc Intake and Its Association with Metabolic Syndrome Indicators among Chinese Adults: An Analysis of the China Nutritional Transition Cohort Survey 2015. Nutrients, 10(5), 572. https://doi.org/10.3390/nu10050572