Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Postnatal Dietary Intake
2.3. Maternal Mental Health Status
2.4. Covariates
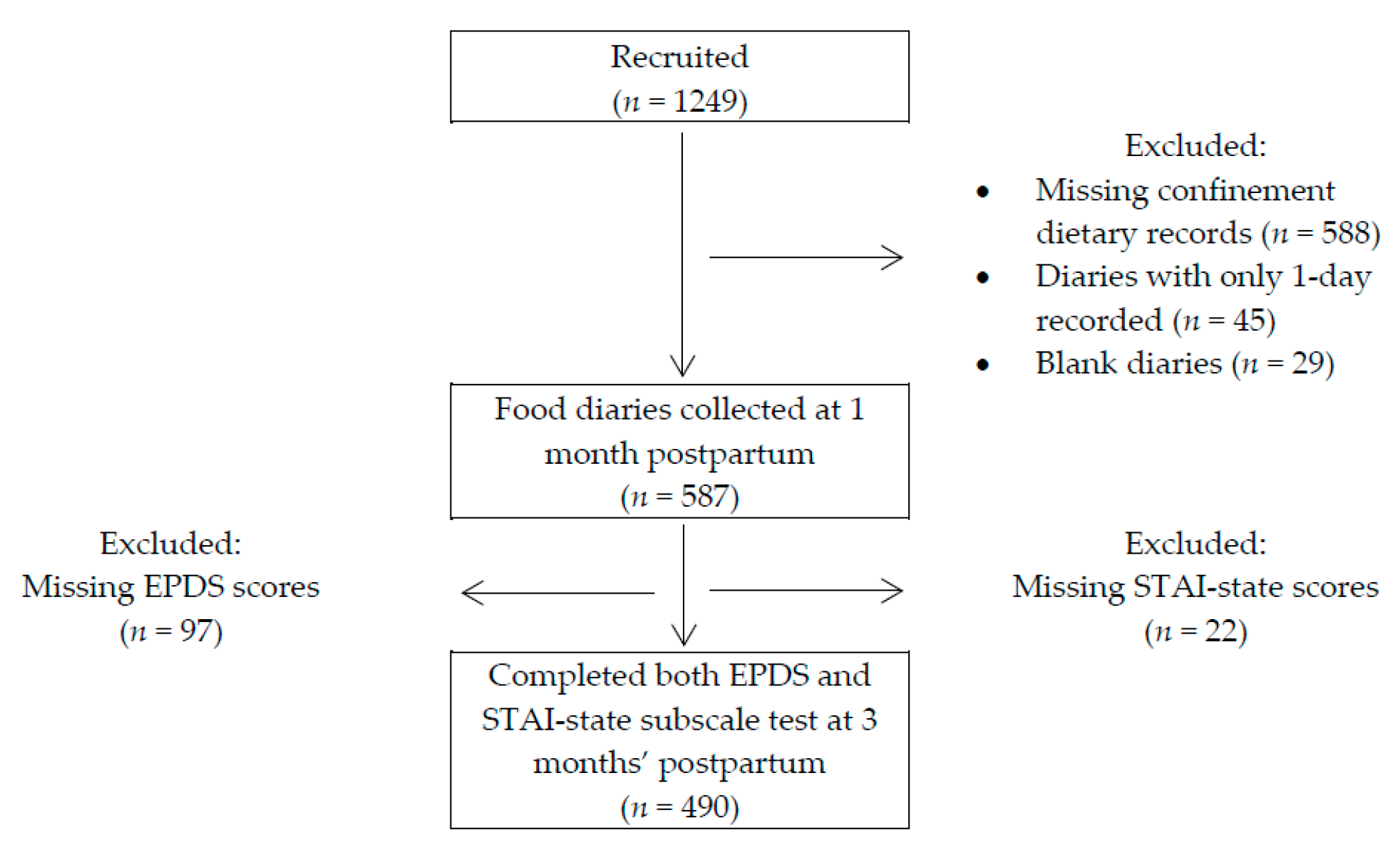
2.5. Participants Included in Analysis
2.6. Derivation of Dietary Patterns
2.7. Statistical Analysis
3. Results
3.1. Postnatal Dietary Patterns
3.2. Characteristics of Participants in Relation to Adherence to Postnatal Dietary Patterns
3.3. Associations between Postnatal Dietary Patterns and Postpartum Mental Health
3.4. Sensitivity Analyses
4. Discussion
4.1. Association between Traditional-Indian-Confinement Diet and PPD
4.2. Association between Soup-Vegetables-Fruits Diet and Maternal Postpartum Mental Health
4.3. Strengths
4.4. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- O’Hara, M.W.; McCabe, J.E. Postpartum depression: Current status and future directions. Ann. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.-L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Bernard-Bonnin, A.-C. Maternal depression and child development. Paediatr. Child Health 2004, 9, 575–583. [Google Scholar]
- Field, T. Postpartum Anxiety Prevalence, Predictors and Effects on Child Development: A Review. J. Psychiatr. Psychiatr. Disord. 2017, 86–102. [Google Scholar] [CrossRef]
- Paul, I.M.; Downs, D.S.; Schaefer, E.W.; Beiler, J.S.; Weisman, C.S. Postpartum Anxiety and Maternal-Infant Health Outcomes. Pediatrics 2013, 131, e1218–e1224. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Chung-Lee, L. Postpartum depression help-seeking barriers and maternal treatment preferences: A qualitative systematic review. Birth 2006, 33, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, K.; Humphries, D. Nutritional Interventions in Depression and Perinatal Depression. Yale J. Biol. Med. 2013, 86, 127–137. [Google Scholar] [PubMed]
- Leung, B.M.; Kaplan, B.J. Perinatal depression: Prevalence, risks, and the nutrition link--a review of the literature. J. Am. Diet. Assoc. 2009, 109, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Popa, T.A.; Ladea, M. Nutrition and depression at the forefront of progress. J. Med. Life 2012, 5, 414–419. [Google Scholar] [PubMed]
- Bodnar, L.M.; Wisner, K.L. Nutrition and depression: Implications for improving mental health among childbearing-aged women. Biol. Psychiatr. 2005, 58, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth-Bowers, E.R.; Corwin, E.J. Nutrition and the psychoneuroimmunology of postpartum depression. Nutr. Res. Rev. 2012, 25, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Etebary, S.; Nikseresht, S.; Sadeghipour, H.R.; Zarrindast, M.R. Postpartum Depression and Role of Serum Trace Elements. Iran. J. Psychiatr. 2010, 5, 40–46. [Google Scholar]
- Green, P.; Hermesh, H.; Monselise, A.; Marom, S.; Presburger, G.; Weizman, A. Red cell membrane omega-3 fatty acids are decreased in nondepressed patients with social anxiety disorder. Eur. Neuropsychopharmacol. 2006, 16, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.J. Decreased Zinc and Increased Copper in Individuals with Anxiety. Nutr. Metab. Insights 2011, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.B.; Whittle, N.; Hetzenauer, A.; Singewald, N. Magnesium deficiency induces anxiety and HPA axis dysregulation: Modulation by therapeutic drug treatment. Neuropharmacology 2012, 62, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Vaz Jdos, S.; Kac, G.; Emmett, P.; Davis, J.M.; Golding, J.; Hibbeln, J.R. Dietary patterns, n-3 fatty acids intake from seafood and high levels of anxiety symptoms during pregnancy: Findings from the Avon Longitudinal Study of Parents and Children. PLoS ONE 2013, 8, e67671. [Google Scholar]
- Vilela, A.A.; Farias, D.R.; Eshriqui, I.; Vaz Jdos, S.; Franco-Sena, A.B.; Castro, M.B.; Olinto, M.T.; Machado, S.P.; Moura da Silva, A.A.; Kac, G. Prepregnancy healthy dietary pattern is inversely associated with depressive symptoms among pregnant Brazilian women. J. Nutr. 2014, 144, 1612–1618. [Google Scholar] [CrossRef] [PubMed]
- Chatzi, L.; Melaki, V.; Sarri, K.; Apostolaki, I.; Roumeliotaki, T.; Georgiou, V.; Vassilaki, M.; Koutis, A.; Bitsios, P.; Kogevinas, M. Dietary patterns during pregnancy and the risk of postpartum depression: The mother–child ‘Rhea’ cohort in Crete, Greece. Public Health Nutr. 2011, 14, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Baskin, R.; Hill, B.; Jacka, F.N.; O’Neil, A.; Skouteris, H. Antenatal dietary patterns and depressive symptoms during pregnancy and early post-partum. Matern. Child Nutr. 2017, 13, e12218. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Miyake, Y.; Sasaki, S.; Tanaka, K.; Murakami, K.; Hirota, Y. Dietary patterns during pregnancy and the risk of postpartum depression in Japan: The Osaka Maternal and Child Health Study. Br. J. Nutr. 2011, 105, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Vilela, A.A.; Pinto Tde, J.; Rebelo, F.; Benaim, C.; Lepsch, J.; Dias-Silva, C.H.; Castro, M.B.; Kac, G. Association of Prepregnancy Dietary Patterns and Anxiety Symptoms from Midpregnancy to Early Postpartum in a Prospective Cohort of Brazilian Women. J. Acad. Nutr. Diet. 2015, 115, 1626–1635. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.-R.; de Seymour, J.V.; Colega, M.; Chen, L.-W.; Chan, Y.-H.; Aris, I.M.; Tint, M.-T.; Quah, P.L.; Godfrey, K.M.; Yap, F.; et al. A vegetable, fruit, and white rice dietary pattern during pregnancy is associated with a lower risk of preterm birth and larger birth size in a multiethnic Asian cohort: The Growing Up in Singapore Towards healthy Outcomes (GUSTO) cohort study 1–3. Am. J. Clin. Nutr. 2016, 104, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- George, G.C.; Milani, T.J.; Hanss-Nuss, H.; Freeland-Graves, J.H. Compliance with dietary guidelines and relationship to psychosocial factors in low-income women in late postpartum. J. Am. Diet. Assoc. 2005, 105, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Fung, K.; Grigoriadis, S.; Robinson, G.E.; Romans, S.; Ross, L. Traditional postpartum practices and rituals: A qualitative systematic review. Women Health 2007, 3, 487–502. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, U.K. Traditional practices of women from India: Pregnancy, childbirth, and newborn care. J. Obstet. Gynecol. Neonatal Nurs. 1997, 26, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Pillsbury, B.L.K. “Doing the month”: Confinement and convalescence of Chinese women after childbirth. Soc. Sci. Med. Part B Med. Anthropol. 1978, 12, 11–22. [Google Scholar] [CrossRef]
- Manderson, L. Roasting, smoking and dieting in response to birth: Malay confinement in cross-cultural perspective. Soc. Sci. Med. Part B Med. Anthropol. 1981, 15, 509–520. [Google Scholar] [CrossRef]
- Naser, E.; Mackey, S.; Arthur, D.; Klainin-Yobas, P.; Chen, H.; Creedy, D.K. An exploratory study of traditional birthing practices of Chinese, Malay and Indian women in Singapore. Midwifery 2012, 28, e865–e871. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Low, Y.L.; Fok, D.; Han, W.M.; Chong, Y.S.; Gluckman, P.; Godfrey, K.; Kwek, K.; Saw, S.M.; Soh, S.E.; et al. Dietary changes during pregnancy and the postpartum period in Singaporean Chinese, Malay and Indian women: The GUSTO birth cohort study. Public Health Nutr. 2014, 17, 1930–1938. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.E.; Tint, M.T.; Gluckman, P.D.; Godfrey, K.M.; Rifkin-Graboi, A.; Chan, Y.H.; Stunkel, W.; Holbrook, J.D.; Kwek, K.; Chong, Y.S.; et al. Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int. J. Epidemiol. 2014, 43, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Board, S. Energy and Nutrient Composition of Food. Available online: http://focos.hpb.gov.sg/eservices/ENCF/ (accessed on 23 August 2017).
- USDA. USDA Food Composition Databases. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 22 January 2018).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatr. 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Gibson, J.; McKenzie-McHarg, K.; Shakespeare, J.; Price, J.; Gray, R. A systematic review of studies validating the Edinburgh Postnatal Depression Scale in antepartum and postpartum women. Acta Psychiatr. Scand. 2009, 119, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Zubaran, C.; Schumacher, M.; Roxo, M.R.; Foresti, K. Screening tools for postpartum depression: Validity and cultural dimensions. Afr. J. Psychiatr. 2010, 13, 357–365. [Google Scholar] [CrossRef]
- Murray, D.; Cox, J.L. Screening for depression during pregnancy with the Edinburgh depression scale (EDDS). J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- Barnes, L.L.B.; Harp, D.; Jung, W.S. Reliability Generalization of Scores on the Spielberger State-Trait Anxiety Inventory. Educ. Psychol. Meas. 2002, 62, 603–618. [Google Scholar] [CrossRef]
- Julian, L.J. Measures of Anxiety. Arthritis Care Res. 2011, 63. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet. Med. J. Br. Diabet. Assoc. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Yeh, Y.C.; St John, W.; Venturato, L. Doing the month in a Taiwanese postpartum nursing center: An ethnographic study. Nurs. Health Sci. 2014, 16, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, E.; Twinn, S.; Yim, I.W. Exploring Chinese Women’s Cultural Beliefs and Behaviours Regarding the Practice of “Doing the Month”. Women Health 2005, 40, 109–123. [Google Scholar] [CrossRef]
- Manderson, L. Traditional food beliefs and critical life events in Peninsular Malaysia. Inf. Int. Soc. Sci. Counc. 1981, 20, 947–975. [Google Scholar] [CrossRef]
- Nag, M. Beliefs and Practices about Food during Pregnancy: Implications for Maternal Nutrition. Econ. Political Wkly. 1994, 29, 2427–2438. [Google Scholar]
- Cousik, R.; Hickey, M. Pregnancy and Childbirth Practices among Immigrant Women from India: “Have a Healthy Baby”. Qual. Rep. 2016, 21, 727–743. [Google Scholar]
- Chen, X.; Zhao, D.; Mao, X.; Xia, Y.; Baker, P.N.; Zhang, H. Maternal Dietary Patterns and Pregnancy Outcome. Nutrients 2016, 8, 351. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, A.V.; Whitten, D.L.; Hawrelak, J.A. Herbal medicines, other than St. John’s Wort, in the treatment of depression: A systematic review. Altern. Med. Rev. J. Clin. Ther. 2011, 16, 40–49. [Google Scholar]
- Lopresti, A.L.; Drummond, P.D. Saffron (Crocus sativus) for depression: A systematic review of clinical studies and examination of underlying antidepressant mechanisms of action. Hum. Psychopharmacol. 2014, 29, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Zameer, S.; Najmi, A.K.; Vohora, D.; Akhtar, M. A review on therapeutic potentials of Trigonella foenum graecum (fenugreek) and its chemical constituents in neurological disorders: Complementary roles to its hypolipidemic, hypoglycemic, and antioxidant potential. Nutr. Neurosci. 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Koh, S.S.H.; Chan, H.W.; Ho, C.Y.X. Clinical Use of Curcumin in Depression: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Al-Karawi, D.; Al Mamoori, D.A.; Tayyar, Y. The Role of Curcumin Administration in Patients with Major Depressive Disorder: Mini Meta-Analysis of Clinical Trials. Phytother. Res. PTR 2016, 30, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Sanmukhani, J.; Satodia, V.; Trivedi, J.; Patel, T.; Tiwari, D.; Panchal, B.; Goel, A.; Tripathi, C.B. Efficacy and safety of curcumin in major depressive disorder: A randomized controlled trial. Phytother. Res. PTR 2014, 28, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Ku, B.; Tie, L.; Yao, H.; Jiang, W.; Ma, X.; Li, X. Curcumin reverses the effects of chronic stress on behavior, the HPA axis, BDNF expression and phosphorylation of CREB. Brain Res. 2006, 1122, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Hausenblas, H.A.; Saha, D.; Dubyak, P.J.; Anton, S.D. Saffron (Crocus sativus L.) and major depressive disorder: A meta-analysis of randomized clinical trials. J. Integr. Med. 2013, 11, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.K.; Bhutani, M.K.; Bishnoi, M. Antidepressant activity of curcumin: Involvement of serotonin and dopamine system. Psychopharmacology 2008, 201, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. Multiple antidepressant potential modes of action of curcumin: A review of its anti-inflammatory, monoaminergic, antioxidant, immune-modulating and neuroprotective effects. J. Psychopharmacol. 2012, 26, 1512–1524. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Sanchez-Villegas, A. Food patterns and the prevention of depression. Proc. Nutr. Soc. 2016, 75, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, M.; Vafa, M.; Esmaillzadeh, A.; Feizi, A.; Majdzadeh, R.; Afshar, H.; Keshteli, A.H.; Adibi, P. Empirically derived dietary patterns in relation to psychological disorders. Public Health Nutr. 2016, 19, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Kingsbury, M.; Dupuis, G.; Jacka, F.; Roy-Gagnon, M.-H.; McMartin, S.E.; Colman, I. Associations between fruit and vegetable consumption and depressive symptoms: Evidence from a national Canadian longitudinal survey. J. Epidemiol. Commun. Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Michel, T.M.; Pulschen, D.; Thome, J. The role of oxidative stress in depressive disorders. Curr. Pharm. Des. 2012, 18, 5890–5899. [Google Scholar] [CrossRef] [PubMed]
- Bouayed, J.; Rammal, H.; Soulimani, R. Oxidative stress and anxiety: Relationship and cellular pathways. Oxid. Med. Cell. Longev. 2009, 2, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Kaur, C.; Kapoor, H.C. Antioxidants in fruits and vegetables—The millennium’s health. Int. J. Food Sci. Technol. 2001, 36, 703–725. [Google Scholar] [CrossRef]
- Scapagnini, G.; Davinelli, S.; Drago, F.; De Lorenzo, A.; Oriani, G. Antioxidants as antidepressants: Fact or fiction? CNS Drugs 2012, 26, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically Derived Eating Patterns Using Factor or Cluster Analysis: A Review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Chee, C.Y.; Lee, D.T.; Chong, Y.S.; Tan, L.K.; Ng, T.P.; Fones, C.S. Confinement and other psychosocial factors in perinatal depression: A transcultural study in Singapore. J. Affect. Disord. 2005, 89, 157–166. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Food Groups | TCC Diet | TIC Diet | Eat-Out Diet | SVF Diet |
|---|---|---|---|---|
| Traditional dried fruits 2,3 | 0.70 | |||
| Herbal tea | 0.67 | |||
| Rhizomes 2 | 0.64 | |||
| Traditional Chinese herbs 2,4 | 0.56 | |||
| Foods cooked with wine or alcohol 2 | 0.56 | |||
| Herbal-based soup | 0.50 | |||
| Pig trotter/tail/skin dishes | 0.50 | |||
| Sesame oil 2 | 0.46 | |||
| Poultry (NF) | 0.45 | |||
| Foods cooked with vinegar 2 | 0.43 | |||
| Red meat (NF) | 0.34 | |||
| Ethnic bread 5 | 0.64 | |||
| Indian herbs 2,6 | 0.58 | |||
| Whole milk | 0.49 | |||
| Seed herbs 2,7 | 0.48 | |||
| Butter/ghee | 0.47 | |||
| Curry-based gravies | 0.46 | |||
| Legumes/pulses | 0.44 | |||
| Allium 2 | 0.43 | |||
| Coffee and tea | 0.35 | |||
| Garlic 2 | 0.35 | |||
| White bread | 0.30 | |||
| Deep-fried/mashed potato | 0.48 | |||
| Sweetened and cordial drinks 8 | 0.46 | |||
| Ice-cream | 0.41 | |||
| Chips/crisps | 0.40 | |||
| Dim sum and local savoury snacks (F) | 0.38 | |||
| Meat (F) | 0.38 | |||
| Soya bean drinks | 0.36 | |||
| Flavoured rice | 0.33 | |||
| Burgers | 0.32 | |||
| Pizza | 0.31 | |||
| Flavoured noodles | 0.31 | |||
| Carbonated drinks | 0.30 | |||
| Vegetable/meat/fish/seafood soup | 0.53 | |||
| Noodles (in soup) | 0.38 | |||
| Vegetables—Cruciferous, Leafy, Yellow/Orange/Red | 0.37 | |||
| Other vegetables 9 and stir fried/boiled potato | 0.35 | |||
| Fish (NF) | 0.35 | |||
| Sweet spreads | −0.33 | |||
| Fresh fruits | 0.33 | |||
| Milk-based drinks | −0.30 |
| Characteristics | Traditional Chinese Confinement Diet | Traditional Indian Confinement Diet | Eat-Out Diet | Soup, Vegetables and Fruits Diet | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | p-Trend | T1 | T2 | T3 | p-Trend | T1 | T2 | T3 | p-Trend | T1 | T2 | T3 | p-Trend | |
| Mother’s age, years | 30.3 ± 5.2 | 31.4 ± 4.8 | 32.3 ± 4.3 | <0.001 | 30.9 ± 5.1 | 30.9 ± 4.7 | 32.2 ± 4.6 | 0.01 | 31.2 ± 4.7 | 31.8 ± 4.6 | 31.0 ± 5.2 | 0.49 | 30.2 ± 5.2 | 31.4 ± 4.9 | 32.4 ± 4.0 | <0.001 |
| Ethnicity, % | <0.001 | <0.001 | <0.001 | <0.001 | ||||||||||||
| Chinese | 15 | 36 | 49 | 40 | 35 | 26 | 38 | 37 | 26 | 21 | 33 | 46 | ||||
| Malay | 72 | 21 | 7 | 33 | 43 | 25 | 26 | 25 | 50 | 58 | 33 | 10 | ||||
| Indian | 52 | 43 | 5 | 3 | 12 | 85 | 26 | 32 | 42 | 51 | 35 | 14 | ||||
| Education, % | <0.001 | 0.01 | 0.53 | <0.001 | ||||||||||||
| Primary and Secondary | 46 | 30 | 23 | 40 | 37 | 23 | 40 | 22 | 38 | 60 | 32 | 8 | ||||
| Post-sec | 34 | 35 | 31 | 31 | 37 | 32 | 31 | 35 | 34 | 42 | 35 | 23 | ||||
| University | 26 | 34 | 40 | 31 | 29 | 39 | 32 | 38 | 30 | 12 | 33 | 55 | ||||
| Nulliparous,% | 32 | 37 | 31 | 0.6 | 36 | 37 | 28 | 0.02 | 34 | 34 | 32 | 0.62 | 26 | 35 | 40 | 0.001 |
| Probable depression at 26 weeks gestation, % | 56 | 22 | 22 | 0.03 | 39 | 31 | 30 | 0.53 | 37 | 40 | 22 | 0.22 | 45 | 37 | 18 | 0.07 |
| High level of state anxiety at 26 weeks gestation, % | 42 | 29 | 28 | 0.06 | 35 | 41 | 24 | 0.05 | 31 | 35 | 34 | 0.67 | 49 | 31 | 20 | <0.001 |
| Past history of miscarriage, % | 31 | 38 | 32 | 0.68 | 35 | 41 | 24 | 0.15 | 35 | 33 | 32 | 0.37 | 23 | 37 | 40 | 0.08 |
| Mode of infant feeding at 1st Month, % | 0.06 | <0.001 | 0.02 | <0.001 | ||||||||||||
| Exclusively Breastfeed | 32 | 31 | 36 | 24 | 31 | 46 | 25 | 35 | 40 | 24 | 33 | 43 | ||||
| Partially Breastfeed | 32 | 33 | 34 | 36 | 35 | 29 | 34 | 36 | 30 | 32 | 34 | 33 | ||||
| Formula Feed | 44 | 40 | 16 | 47 | 31 | 21 | 51 | 14 | 34 | 70 | 27 | 3 | ||||
| Dietary Patterns | EPDS Scores | Probable PPD (EPDS ≥ 13) (n = 48) 2 | STAI-State Subscale Scores | |||
|---|---|---|---|---|---|---|
| β (95% CI) | p | OR (95% CI) | p | β (95% CI) | p | |
| Traditional Chinese Confinement diet | 0.38 (−0.11 to 0.87) | 0.13 | 1.3 (0.85 to 2.00) | 0.22 | −0.34 (−1.40 to 0.73) | 0.54 |
| Traditional Indian Confinement diet | −0.62 (−1.16 to −0.09) | 0.02 | 0.56 (0.31 to 1.01) | 0.05 | −0.51 (−1.66 to 0.64) | 0.39 |
| Eat Out diet | −0.04 (−0.44 to 0.36) | 0.84 | 0.87 (0.59 to 1.29) | 0.49 | 0.06 (−0.80 to 0.93) | 0.89 |
| Soup, Vegetables and Fruits diet | −0.48 (−0.97 to 0.02) | 0.06 | 0.92 (0.58 to 1.45) | 0.73 | −1.49 (−2.56 to −0.42) | 0.006 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teo, C.; Chia, A.-R.; Colega, M.T.; Chen, L.-W.; Fok, D.; Pang, W.W.; Godfrey, K.M.; Tan, K.H.; Yap, F.; Shek, L.P.-C.; et al. Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study. Nutrients 2018, 10, 299. https://doi.org/10.3390/nu10030299
Teo C, Chia A-R, Colega MT, Chen L-W, Fok D, Pang WW, Godfrey KM, Tan KH, Yap F, Shek LP-C, et al. Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study. Nutrients. 2018; 10(3):299. https://doi.org/10.3390/nu10030299
Chicago/Turabian StyleTeo, Cherlyen, Ai-Ru Chia, Marjorelee T. Colega, Ling-Wei Chen, Doris Fok, Wei Wei Pang, Keith M. Godfrey, Kok Hian Tan, Fabian Yap, Lynette Pei-Chi Shek, and et al. 2018. "Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study" Nutrients 10, no. 3: 299. https://doi.org/10.3390/nu10030299
APA StyleTeo, C., Chia, A.-R., Colega, M. T., Chen, L.-W., Fok, D., Pang, W. W., Godfrey, K. M., Tan, K. H., Yap, F., Shek, L. P.-C., Chong, Y.-S., Meaney, M., Chen, H., & Chong, M. F.-F. (2018). Prospective Associations of Maternal Dietary Patterns and Postpartum Mental Health in a Multi-Ethnic Asian Cohort: The Growing up in Singapore towards Healthy Outcomes (GUSTO) Study. Nutrients, 10(3), 299. https://doi.org/10.3390/nu10030299