Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
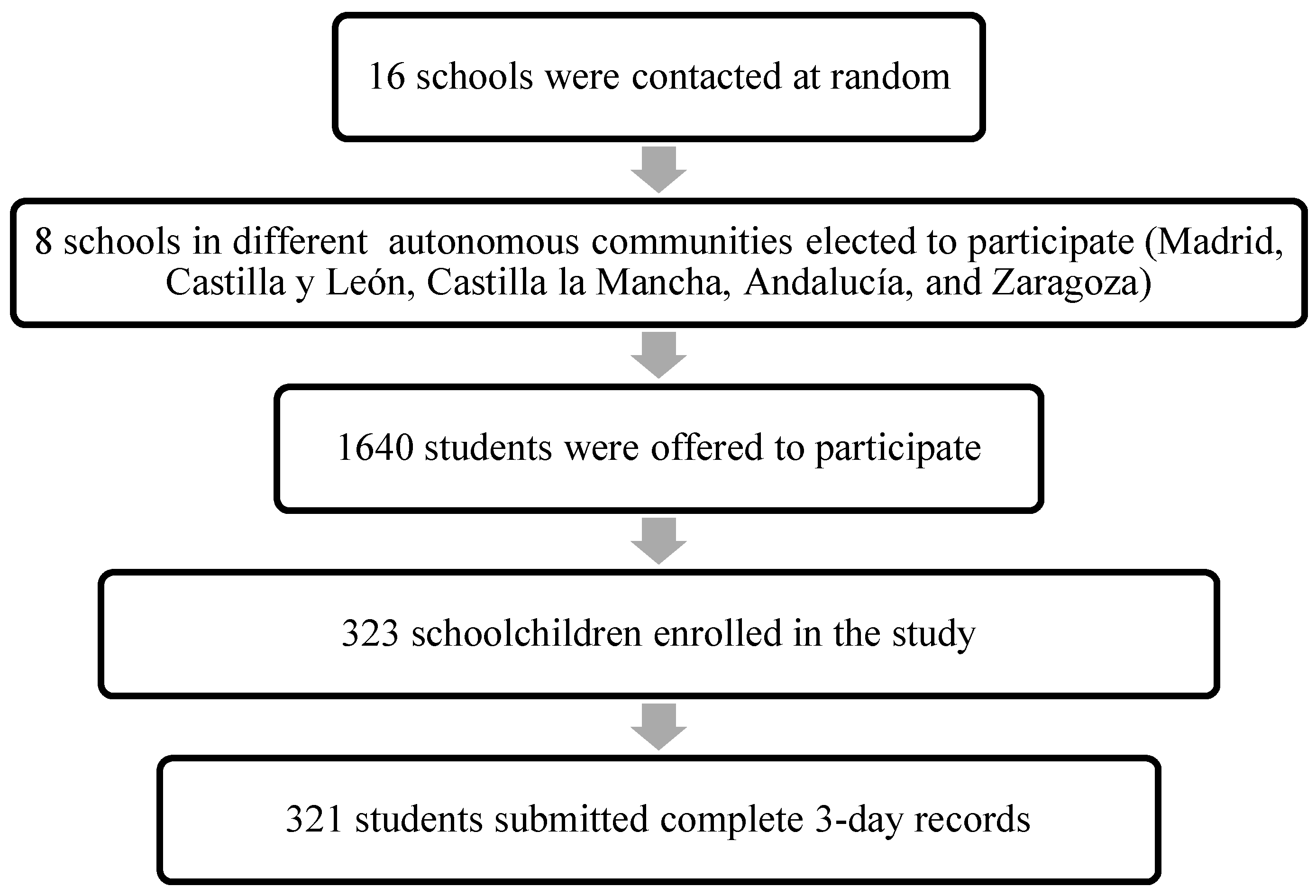
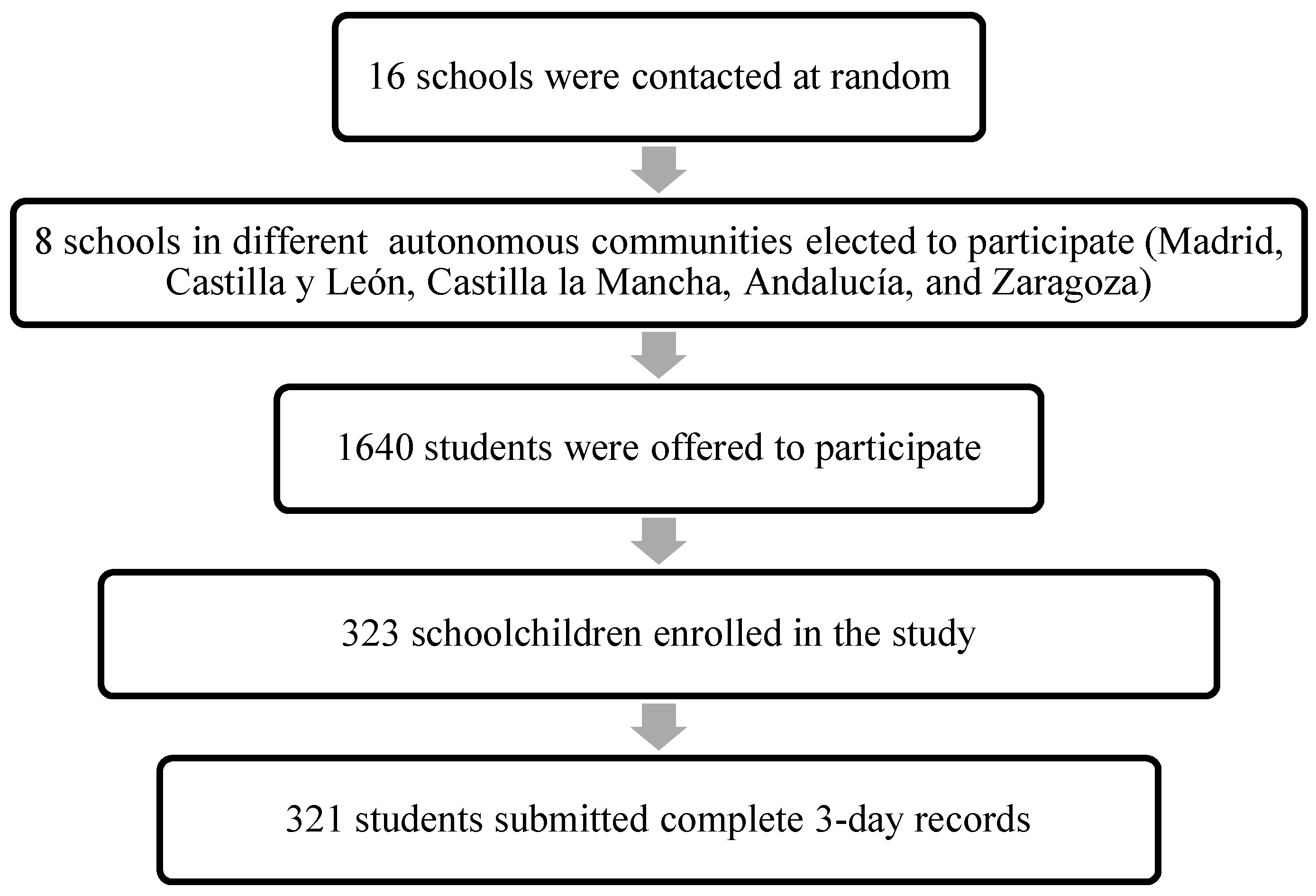
2.1. Study Design
2.2. Subjects
2.3. Collection of Dietary Data
2.4. Sodium Sources and Food Grouping
2.5. Food Classification Based on the Nutritional Profile
- Food fortification did not alter whether food was classified as basic or discretionary. For example, sugar-sweetened beverages with added vitamins were considered discretionary.
- For breakfast cereals, discretionary foods were defined as breakfast cereals with >30 g of simple sugars per 100 g.
- For breakfast cereals with added fruit, discretionary foods were defined as breakfast cereals with >35 g of simple sugars per 100 g.
- For dishes derived from cereals (e.g., prepared sandwiches) and some ready-to-eat meals (burgers, wrappers, sushi, pizzas, kebab, sausages), discretionary foods were defined as those that exceeded 5 g of saturated fat per 100 g. The subgroup of prepared and pre-cooked dishes was a very varied group in which food had to be classified by the product and not by the group.
- Salt biscuits were classified as basic if they contained less than 430 kcal/100 g.
- Canned soups were considered discretionary because of the high sodium content per 100 g.
2.6. Food Classification Based on the Degree of Processing
2.7. Sociodemographic and Anthropometric Data
2.8. Validity of the Dietary Assessment Method
2.9. Statistical Processing of Data
3. Results
3.1. Descriptive
3.2. Dietary Sodium and Energy Intake by Sex through Two Food Classification Systems
3.3. Top Sources of Dietary Sodium
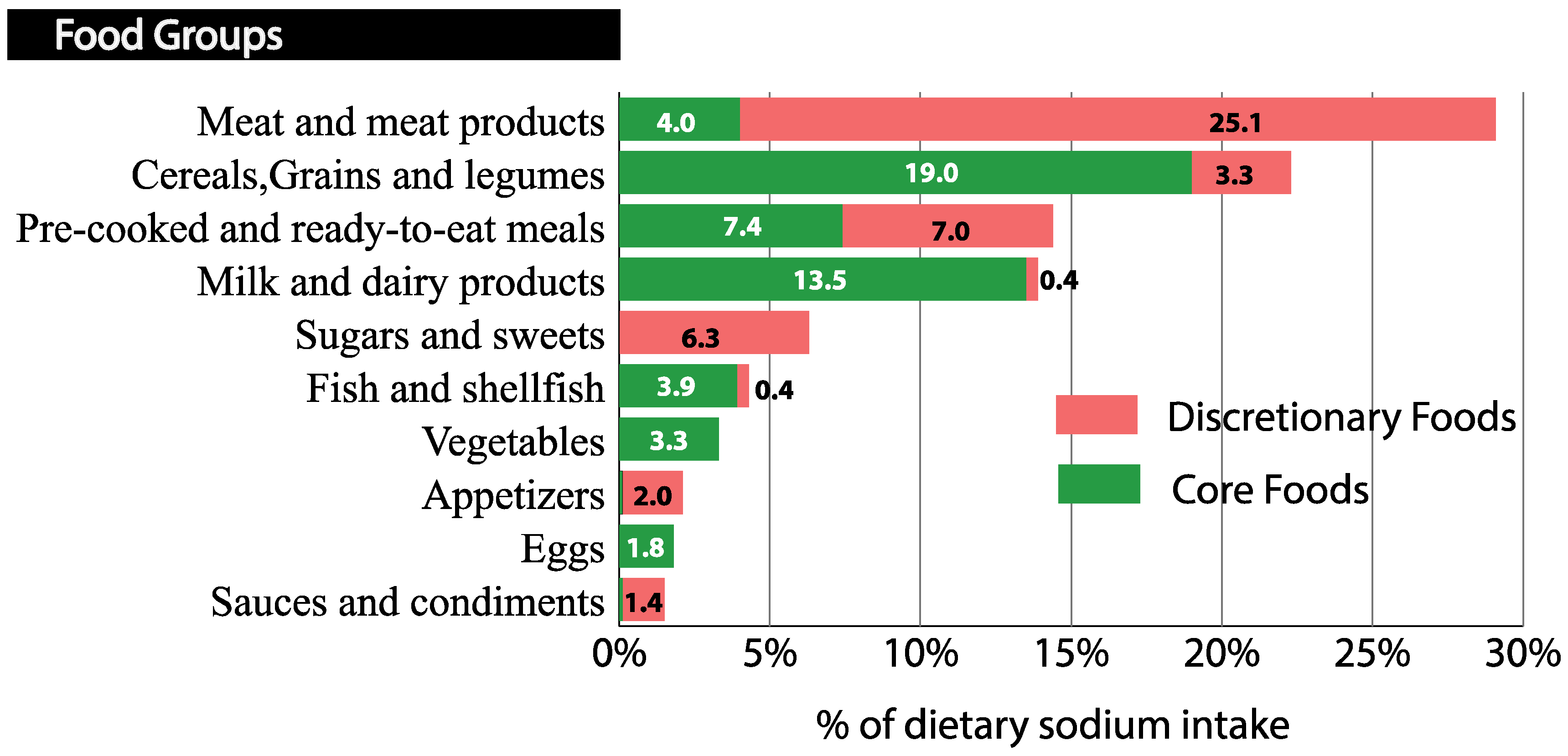
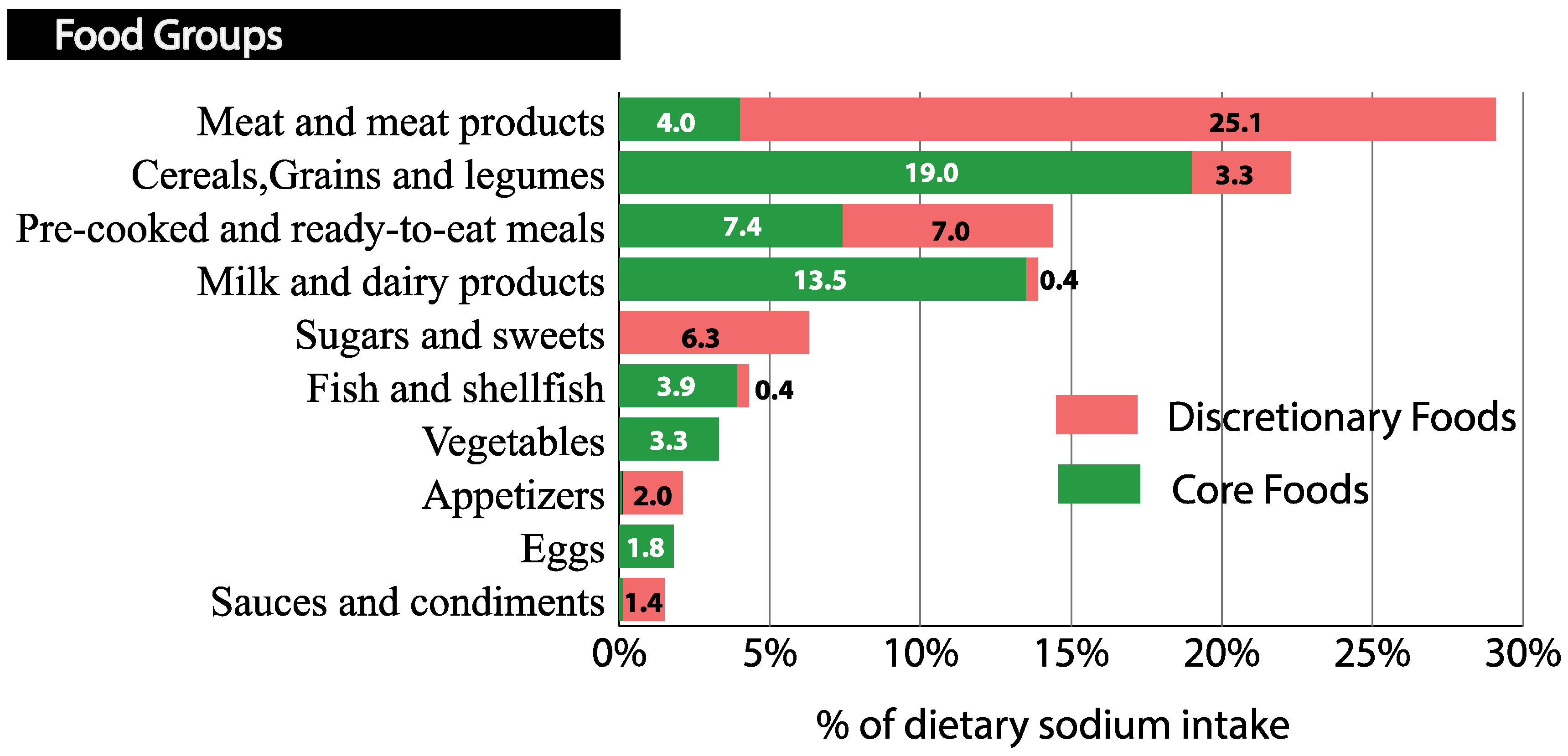
3.3.1. Sources of Dietary Sodium According to Food Groups and Nutritional Profile
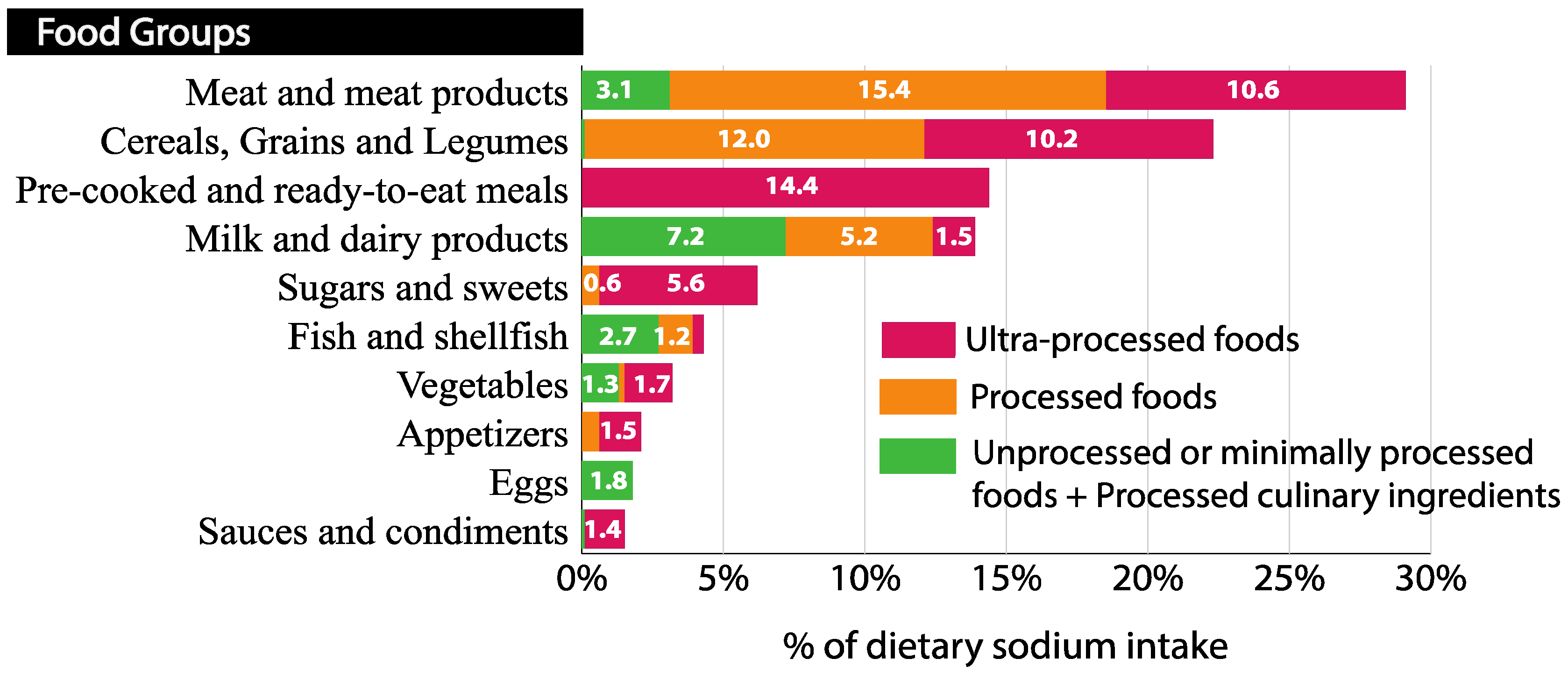
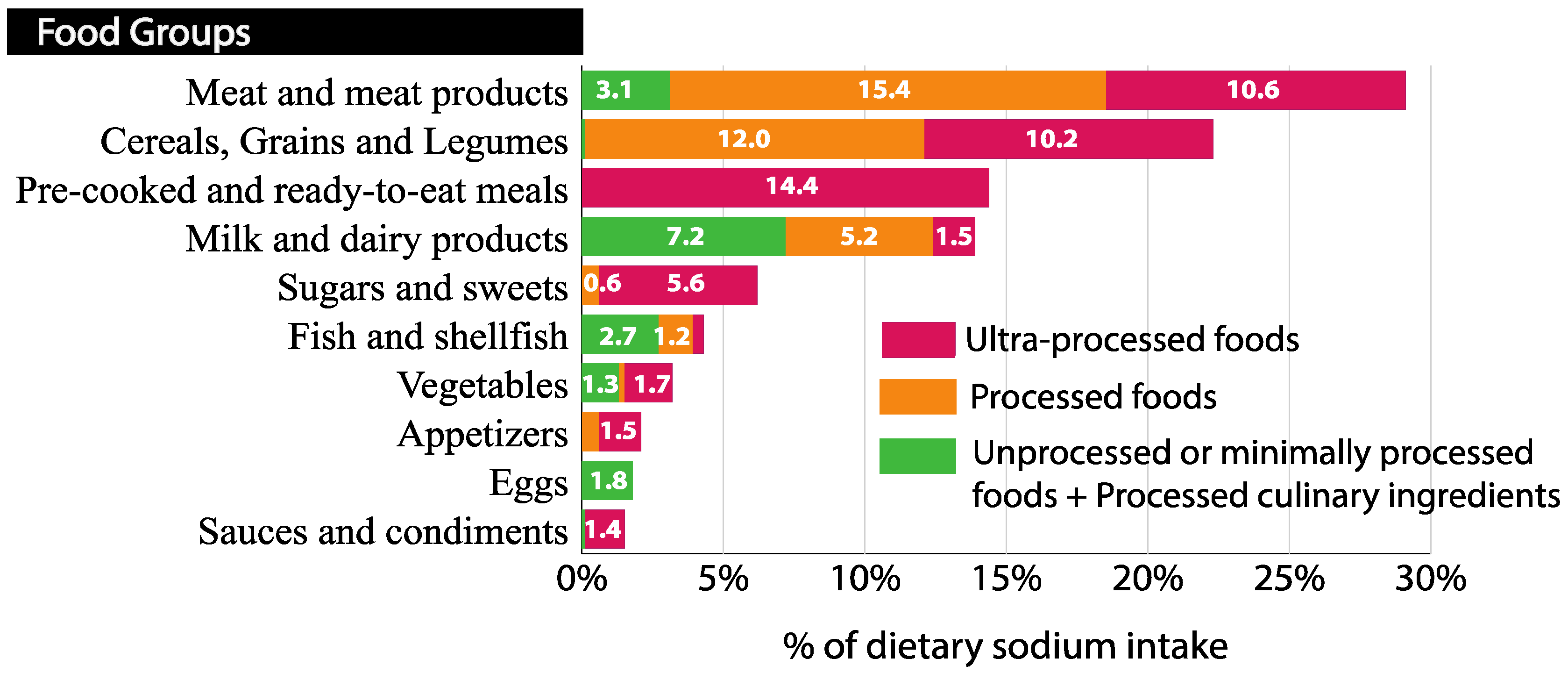
3.3.2. Sources of Dietary Sodium According to Food Groups and Degree of Processing
3.3.3. Sources of Sodium Intake According to Food Subgroups, Nutritional Profile, and Degree of Processing
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010; Secretary of Agriculture and the Secretary of Health and Human Services: Washington, DC, USA, 2010; pp. 492–534. [Google Scholar]
- Wong, M.M.Y.; Arcand, J.A.; Leung, A.A.; Raj, T.S.; Trieu, K.; Santos, J.A.; Campbell, N.R.C. The Science of Salt: A Regularly Updated Systematic Review of Salt and Health Outcomes (August to November 2015). J. Clin. Hypertens. 2017, 19, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mapping Salt Reduction Initiatives in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products; Nutrition and Allergies). Opinion of the Scientific Panel on Dietetic products, nutrition and allergies related to the Tolerable Upper Intake Level of Sodium. EFSA J. 2005, 193, 1–19. [Google Scholar] [CrossRef]
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases. Report of a Joint WHO/FAO Expert Consultation; WHO Technical Report Series: Geneva, Switzerland, 2003. [Google Scholar]
- European Commission. Implementation of the EU Salt Reduction Framework—Results of Member States Survey; Publications Office of the European Union: Luxembourg, Luxembourg, 2012. [Google Scholar]
- Campanozzi, A.; Avallone, S.; Barbato, A.; Iacone, R.; Russo, O.; De Filippo, G.; D’Angelo, G.; Pensabene, L.; Malamisura, B.; Cecere, G.; et al. High sodium and low potassium intake among Italian children: Relationship with age, body mass and blood pressure. PLoS ONE 2015, 10, e0121183. [Google Scholar] [CrossRef] [PubMed]
- AFSSA (Agence française de sécurité sanitaire des aliments). Étude individuelle nationale des consommations alimentaires 3 (INCA 3); Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail: Maisons-Alfort, France, 2017. [Google Scholar]
- Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Informe del Comité Científico de la Agencia Española de Consumo, Seguridad Alimentaria y Nutrición Sobre Objetivos y Recomendaciones Nutricionales y de Actividad Física Frente a la Obesidad en el Marco de la Estrategia NAOS; Revista del Comité Científico de la AECOSAN: Madrid, España, 2014. [Google Scholar]
- Aranceta, J.; Miján de la Torre, A.; Moreno Villares, J.M. Clínicas Españolas De Nutrición, 1st ed.; Elsevier Masson: Barcelona, Spain, 2005. [Google Scholar]
- Liem, D.G. Infants’ and Children’s Salt Taste Perception and Liking: A Review. Nutrients 2017, 9, 1011. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A.; Finkbeiner, S.; Lipchock, S.V.; Hwang, L.-D.; Reed, D.R. Preferences for salty and sweet tastes are elevated and related to each other during childhood. PLoS ONE 2014, 9, e92201. [Google Scholar] [CrossRef] [PubMed]
- Dossier Resumen: Plan de Colaboración Para de los Alimentos y Bebidas y Otras Medidas 2017–2020. Available online: http://www.aecosan.msssi.gob.es/AECOSAN/docs/documentos/nutricion/DOSSIER_PLAN_2020.pdf (accessed on 29 November 2018).
- Ahmed, A.; Ahmad, A.; Khalid, N.; David, A.; Sandhu, M.A.; Randhawa, M.A.; Suleria, H.A.R. A Question Mark on Iron Deficiency in 185 Million People of Pakistan: Its Outcomes and Prevention. Crit. Rev. Food Sci. Nutr. 2014, 54, 1617–1635. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Anjum, F.M.; Butt, M.S.; Huma, N.; Suleria, H.A.R. Concept of double salt fortification; a tool to curtail micronutrient deficiencies and improve human health status. J. Sci. Food Agric. 2014, 94, 2830–2838. [Google Scholar] [CrossRef]
- Grieger, J.A.; Wycherley, T.P.; Johnson, B.J.; Golley, R.K. Discrete strategies to reduce intake of discretionary food choices: A scoping review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 57. [Google Scholar] [CrossRef]
- Aparicio, A.; Rodríguez-Rodríguez, E.; Cuadrado-Soto, E.; Navia, B.; López-Sobaler, A.M.; Ortega, R.M. Estimation of salt intake assessed by urinary excretion of sodium over 24 h in Spanish subjects aged 7–11 years. Eur. J. Nutr. 2015, 56, 171–178. [Google Scholar] [CrossRef] [Green Version]
- DIAL (for Windows, version 3.0.0.12); DIAL software for assessing diets and food calculations. Department of Nutrition (UCM) & Alceingeniería, S.A.: Madrid, Spain, 2018.
- Ortega, R.M.; López-Sobaler, A.M.; Requejo, A.M.; Andrés, P. Food Composition. A Basic Tool for Assessing Nutritional Status; Editorial Complutense: Madrid, Spain, 2010. [Google Scholar]
- Krebs-Smith, S.M.; Kott, P.S.; Guenther, P.M. Mean proportion and population proportion: Two answers to the same question? J. Am. Diet. Assoc. 1989, 89, 671–676. [Google Scholar]
- O’Halloran, S.A.; Grimes, C.A.; Lacy, K.E.; Nowson, C.A.; Campbell, K.J. Dietary sources and sodium intake in a sample of Australian preschool children. BMJ Open 2016, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ziauddeen, N.; Almiron-Roig, E.; Penney, T.; Nicholson, S.; Kirk, S.; Page, P. Eating at Food Outlets and “On the Go” Is Associated with Less Healthy Food Choices in Adults: Cross-Sectional Data from the UK National Diet and Nutrition Survey Rolling Programme (2008–2014). Nutrients 2017, 9, 1315. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; van Jaarsveld, C.H.; Wardle, J. Individual and family environment correlates differ for consumption of core and non-core foods in children. Br. J. Nutr. 2011, 105, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Fayet-Moore, F.; Petocz, P.; McConnell, A.; Tuck, K.; Mansour, M. The cross-sectional association between consumption of the recommended five food group “Grain (Cereal)”, dietary fibre and anthropometric measures among australian adults. Nutrients 2017, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Australian Dietary Guidelines; NHMRC: Canberra, Australia, 2013; ISBN1 1864965754. ISBN2 1864965746. [Google Scholar]
- Australian Bureau of Statistics Discretionary Food List—Australian Health Survey: Users’ Guide, 2011–2013. Available online: http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4363.0.55.0012011-13?OpenDocument (accessed on 24 January 2018).
- Moubarac, J.-C. Ultra-Processed Food and Drink Products in Latin America: Trends, Impact on Obesity, Policy Implications; Pan American Health Organization: Washington DC, USA, 2015. [Google Scholar]
- Moubarac, J.-C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar]
- Goldberg, G.; Black, A.; Jebb, S.; Colte, T.; Murgatroyd, P.; Coward, W.; Prentice, A. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Moosavian, S.P.; Haghighatdoost, F.; Surkan, P.J.; Azadbakht, L. Salt and obesity: A systematic review and meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 265–277. [Google Scholar] [CrossRef]
- Black, A. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Colin-Ramirez, E.; Espinosa-Cuevas, Á.; Miranda-Alatriste, P.V.; Tovar-Villegas, V.I.; Arcand, J.; Correa-Rotter, R. Food Sources of Sodium Intake in an Adult Mexican Population: A Sub-Analysis of the SALMEX Study. Nutrients 2017, 9, 810. [Google Scholar] [CrossRef]
- López-Sobaler, A.M.; Aparicio, A.A.; González-Rodríguez, L.G.; Cuadrado-Soto, E.; Rubio, J.; Marcos, V.; Sanchidrián, R.; Santos, S.; Pérez-Farinós, N.; Ángeles, M.; et al. Adequacy of Usual Vitamin and Mineral Intake in Spanish Children and Adolescents: ENALIA Study. Nutrients 2017, 9, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Obesity Epidemiology; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Vainik, U.; Konstabel, K.; Lätt, E.; Mäestu, J.; Purge, P.; Jürimäe, J. Diet misreporting can be corrected: Confirmation of the association between energy intake and fat-free mass in adolescents. Br. J. Nutr. 2016, 116, 1425–1436. [Google Scholar] [CrossRef] [PubMed]
- Desor, J.A.; Greene, L.S.; Maller, O. Preferences for sweet and salty in 9- to 15-year-old and adult humans. Science 1975, 190, 686–687. [Google Scholar] [CrossRef] [PubMed]
- Jaenke, R.; Barzi, F.; McMahon, E.; Webster, J.; Brimblecombe, J. Consumer acceptance of reformulated food products: A systematic review and meta-analysis of salt-reduced foods. Crit. Rev. Food Sci. Nutr. 2017, 57, 3357–3372. [Google Scholar] [CrossRef] [PubMed]
- Marrero, N.M.; He, F.J.; Whincup, P.; MacGregor, G.A. Salt intake of children and adolescents in south London consumption levels and dietary sources. Hypertension 2014, 63, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Eloranta, A.M.; Venäläinen, T.; Soininen, S.; Jalkanen, H.; Kiiskinen, S.; Schwab, U.; Lakka, T.A.; Lindi, V. Food sources of energy and nutrients in Finnish girls and boys 6–8 years of age—The PANIC study. Food Nutr. Res. 2016, 60, 32444. [Google Scholar] [CrossRef] [PubMed]
- Gaitán, D.A.; Estrada, A.; Lozano, G.A.; Luz, Y.; Manjarres, M. Food sources of sodium: Analysis Based on a national survey in Colombia. Nutr. Hosp. 2015, 3232, 2338–2345. [Google Scholar] [CrossRef]
- Grimes, C.A.; Campbell, K.J.; Riddell, L.J.; Nowson, C.A. Sources of sodium in Australian children’s diets and the effect of the application of sodium targets to food products to reduce sodium intake. Br. J. Nutr. 2011, 105, 468–477. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; Pearson, S. Interpreting the Australian dietary guideline to “limit” into practical and personalised advice. Nutrients 2015, 7, 2026–2043. [Google Scholar] [CrossRef]
- Sarmugam, R.; Worsley, A. Current Levels of Salt Knowledge: A Review of the Literature. Nutrients 2014, 6, 5534–5559. [Google Scholar] [CrossRef] [Green Version]
- Aranceta Bartrina, J.; Arija Val, V.; Maíz Aldalur, E.; Martínez de Victoria Muñoz, E.; Ortega Anta, R.M.; Pérez-Rodrigo, C.; Quiles Izquierdo, J.; Rodríguez Martín, A.; Román Viñas, B.; Salvador Castell, G.; et al. Guías alimentarias para la población española (SENC, diciembre 2016); la nueva pirámide de la alimentación saludable. Nutr. Hosp. 2016, 33, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Magriplis, E.; Farajian, P.; Pounis, G.D.; Risvas, G.; Panagiotakos, D.B.; Zampelas, A. High sodium intake of children through “hidden” food sources and its association with the Mediterranean diet: The GRECO study. J. Hypertens. 2011, 29, 10691076. [Google Scholar] [CrossRef]
- Gonçalves, C.; Abreu, S.; Padrão, P.; Pinho, O.; Graça, P.; Breda, J.; Santos, R.; Moreira, P. Sodium and potassium urinary excretion and dietary intake: A cross-sectional analysis in adolescents. Food Nutr. Res. 2016, 60, 2944. [Google Scholar] [CrossRef] [PubMed]
- Regional Expert Group for Cardiovascular Disease. Prevention through Population-Wide Dietary Salt Reduction 2010. Available online: https://www.paho.org/hq/dmdocuments/2013/Metodos-determinar-fuentes-sodio-Eng.pdf (accessed on 15 October 2018).
- Dötsch-Klerk, M.; Goossens, W.P.; Meijer, G.; Van Het Hof, K. Reducing salt in food; setting product-specific criteria aiming at a salt intake of 5 g per day. Eur. J. Clin. Nutr. 2015, 69, 799–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Nova Group | Characteristics | Processes Included |
|---|---|---|
| Group 1: Unprocessed or minimally processed foods (NP + MPF) | Minimally processed foods and beverages, without adding new ingredients from other groups. | To conserve food and make it suitable for storage (freezing, packaging, fractioning…), facilitate its culinary preparation (crushing, filtering, roasting…) and improve its nutritional quality. |
| Group 2: Processed culinary Ingredients (PCI) | These ingredients are extracted from group 1 foods or nature. They are usually not consumed on their own. * | Pressing, refining, grinding, milling, and spray drying. |
| May contain additives such as preservatives or stabilizing agents. | ||
| Group 3: Processed foods (PF) | They are relatively simple products produced by adding sugar, oil, salt or other substances from Group 2 to Group 1 foods. | Addition of substances like sugar, oil or salt to group 1 foods. |
| Non-alcoholic fermentation (breads and cheese). | ||
| May contain additives such as preservatives or stabilizing agents. | ||
| Group 4: Ultra-processed food and drink products (UPF) | These are industrially manufactured foods and beverages that usually contain five or more substances as ingredients. They contain some of the ingredients present in processed foods (salt, sugar, oils and fats); however, UPF also includes ingredients that are not commonly used in cooking preparations, such as hydrolyzed proteins, modified starches and hydrogenated oils and additives. | Several industrial processes are used without equivalents in domestic or traditional cuisine. |
| The main objective of industrial ultra-processing is to create ready-to-eat, ready-to-drink or ready-to-heat products that can replace unprocessed or minimally processed foods and freshly prepared dishes. |
| Variables | Categories | Total % (n) * | Girls % (n) * | Boys % (n) * | p ** |
|---|---|---|---|---|---|
| n | 100 (321) | 51.4 (165) | 48.6 (156) | ||
| Age (years) | 8.8 ± 1.2 | 8.9 ± 1.2 | 8.8 ± 1.2 | 0.686 *** | |
| Age groups | |||||
| 7–8 years | 42.4 (136) | 43.0 (71) | 41.7 (65) | 0.805 | |
| 9–11 years | 57.6 (185) | 57.0 (94) | 58.3 (91) | ||
| Residence | |||||
| >50,000 inhabitants | |||||
| Capital of the province | 43.3 (139) | 44.2 (73) | 42.3 (66) | 0.727 | |
| <50,000 inhabitants | 56.7 (182) | 55.8 (92) | 57.7 (90) | ||
| Annual household income | |||||
| Less than 18,000 € | 27.0 (86) | 29.9 (49) | 23.9 (37) | 0.568 | |
| 18,001–36,000 € | 17.9 (57) | 19.5 (32) | 16.1 (25) | ||
| 36,001–48,000 € | 21.3 (68) | 19.5 (32) | 23.2 (36) | ||
| 48,000 € | 19.7 (63) | 17.7 (29) | 21.9 (34) | ||
| DK/NA | 14.1 (45) | 13.4 (22) | 14.8 (23) | ||
| Father’s education level | |||||
| No school/primary school | 24.0 (75) | 22.2 (36) | 26.0 (39) | 0.190 | |
| Secondary/VT | 40.1 (125) | 46.3 (75) | 33.3 (50) | ||
| Graduated | 31.1 (97) | 26.5 (43) | 36 (54) | ||
| Master’s/Ph.D. | 4.8 (15) | 4.9 (8) | 4.7 (7) | ||
| Mother’s education level | |||||
| No school/primary school | 18.2 (58) | 17.8 (29) | 18.7 (29) | 0.448 | |
| Secondary/VT | 38.4 (122) | 41.1 (67) | 35.5 (55) | ||
| Graduated | 38.7 (123) | 38 (62) | 39.4 (61) | ||
| Master’s/Ph.D. | 4.7 (15) | 3.1 (5) | 6.5 (10) | ||
| Anthropometric measurements | |||||
| Weight (kg) | 35.4 ± 8.5 | 35.0 ± 8.5 | 35.7 ± 8.6 | 0.55 *** | |
| Height (cm) | 136.9 ± 9 | 136.2 ± 9.6 | 137.7 ± 8.4 | 0.144 | |
| BMI | 18.7 ± 3.2 | 18.7 ± 3.1 | 18.7 ± 3.3 | 0.761 *** |
| Dietary Component | Food Classification | Total Population (n = 321) | Girls (n = 165) | Boys (n = 156) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | P50 (P25,P75) | % total | Mean ± SD | P50 (P25,P75) | % total | Mean ± SD | P50 (P25,P75) | % total | p | ||
| Energy | Total | 8761 ± 1347 | 8778 (7853,9791) | 100 | 8565 ± 1372 | 8485 (7560,9678) | 100 | 8950 ± 1301 | 9083 (8092,9904) | 100 | 0.011 |
| (kJ/day) | CF * | 6021 ± 1121 | 6033 (5096,6740) | 68.7 | 5904 ± 1119 | 5949 (5042,6550) | 68.9 | 6130 ± 1118 | 6175 (5196,6899) | 68.5 | 0.745 |
| DF | 2745 ± 954 | 2686 (2013,3431) | 31.3 | 2660 ± 962 | 2607 (1915,3351) | 31.1 | 2821 ± 939 | 2751 (2074,3467) | 31.5 | 0.157 | |
| NP + MPF | 3163 ± 828 | 3105 (2598,3711) | 36.1 | 3117 ± 824 | 3059 (2548,3694) | 36.4 | 3209 ± 833 | 3159 (2632,3745) | 35.9 | 0.890 | |
| PCI * | 1042 ± 427 | 975 (749,1301) | 11.8 | 1038 ± 439 | 975 (699,1310) | 11.9 | 1050 ± 411 | 975 (774,1289) | 11.7 | 0.597 | |
| PF * | 1452 ± 623 | 1423 (975,1787) | 16.3 | 1418 ± 636 | 1397 (929,1741) | 16.3 | 1485 ± 611 | 1452 (1050,1870) | 16.3 | 0.296 | |
| UPF | 3138 ± 1155 | 3079 (2377,3870) | 35.8 | 3033 ± 1121 | 3046 (2218,3665) | 35.4 | 3238 ± 1180 | 3209 (2423,3962) | 36.1 | 0.257 | |
| Dietary sodium | Total * | 2026 ± 504 | 1990 (1676,2309) | 100 | 1952 ± 461 | 1926 (1656,2217) | 100 | 2099 ± 530 | 2044 (1743,2391) | 100 | 0.010 |
| (mg/day) | CF * | 1090 ± 306 | 1057 (873,1271) | 53.8 | 1059 ± 301 | 1025 (852,1237) | 54.2 | 1120 ± 309 | 1080 (910,1292) | 53.4 | 0.063 |
| DF * | 937 ± 382 | 865 (637,1174) | 46.2 | 893 ± 350 | 847 (620,1118) | 45.8 | 978 ± 406 | 903 (661,1201) | 46.6 | 0.110 | |
| NP + MPF | 337 ± 114 | 337 (261,411) | 16.6 | 335 ± 117 | 337 (252,414) | 17.2 | 340 ± 113 | 335 (277,403) | 16 | 0.720 | |
| PCI * | 1.12 ± 2.1 | 0.02 (0.1,33) | 0.1 | 0.87 ± 1.55 | 0.01 (0.1,1) | 0.1 | 1.36 ± 2.5 | 0.02 (0.1,6) | 0.1 | 0.188 | |
| PF * | 730 ± 380 | 680 (448,944) | 35.5 | 712 ± 360 | 706 (423,942) | 35.9 | 747 ± 398 | 643 (462,946) | 35 | 0.688 | |
| UPF * | 970 ± 394 | 921 (679,1216) | 47.8 | 916 ± 378 | 881 (673,1123) | 46.9 | 1021 ± 403 | 999 (687,1260) | 49 | 0.017 | |
| Classification of Foods According to Their Nutritional Profile | Classification of Foods According to Their Processing Level | ||||||
|---|---|---|---|---|---|---|---|
| Sodium Ranking | % Energy | % Sodium | Sodium Ranking | % Energy | % Sodium | ||
| Core Foods and Beverages | Unprocessed or Minimally Processed Foods and Beverages | ||||||
| 1 | White Bread | 6.9 | 11.6 | ||||
| 2 | Milk | 7.7 | 6.5 | 1 | Milk | 7.7 | 6.5 |
| 3 | Pizzas | 2.0 | 4.8 | 2 | Eggs | 2.0 | 1.8 |
| 4 | Sliced Bread | 1.9 | 3.6 | 3 | Poultry meat | 2.6 | 1.2 |
| 5 | Pre-cooked and ready-to-eat meals | 1.1 | 2.6 | 4 | Fresh shellfish and mollusks | 0.5 | 1.2 |
| 6 | Semicured and cured cheeses | 1.5 | 2.6 | 5 | Bovine meat | 2.4 | 1.0 |
| 7 | Yogurts and fermented milk | 3.0 | 2.1 | 6 | Whitefish | 0.6 | 0.9 |
| 8 | Vegetable preserves | 0.3 | 1.9 | 7 | Fresh vegetables | 1.0 | 0.9 |
| 9 | Eggs | 2.0 | 1.8 | 8 | Pork meat | 2.3 | 0.8 |
| 10 | Breakfast cereals | 1.0 | 1.4 | 9 | Plain yogurts and fermented milk | 0.6 | 0.7 |
| 11 | Poultry meat | 2.6 | 1.2 | 10 | Bluefish | 0.8 | 0.5 |
| 12 | Fresh shellfish and mollusks | 0.5 | 1.2 | Processed culinary ingredients | |||
| 13 | Bovine meat | 2.4 | 1.0 | ||||
| 14 | Sausages | 0.2 | 1.0 | 1 | Butter | 0.7 | 0.1 |
| 15 | Fish preserves | 0.4 | 0.9 | 2 | Oils | 10.3 | 0.0 |
| 16 | Fresh vegetables | 1.0 | 0.9 | 2 | Sugars | 0.5 | 0.0 |
| 17 | Whitefish | 0.6 | 0.9 | 3 | Lard | 0.3 | 0.0 |
| 18 | Toasted bread | 0.3 | 0.9 | ||||
| 19 | Milkshakes | 0.9 | 0.7 | Processed foods and beverages | |||
| 20 | Hamburger bread | 0.4 | 0.6 | 1 | White bread | 6.9 | 11.6 |
| Discretionary foods and beverages | 2 | Serrano ham | 0.6 | 8.2 | |||
| 1 | Serrano ham | 0.6 | 8.2 | 3 | Cured cold meats | 1.8 | 6.6 |
| 2 | Cured cold meats | 1.8 | 6.6 | 4 | Semicured and cured cheeses | 1.5 | 2.6 |
| 3 | Cube soup | 0.1 | 6.1 | 5 | Sugared and with fruit yogurts | 2.4 | 1.4 |
| 4 | Cold meat | 1.6 | 5.4 | 6 | Canned fish | 0.4 | 0.9 |
| 5 | Sausages | 1.1 | 3.5 | 7 | Bakery products | 0.7 | 0.6 |
| 6 | Buns, sweet bread, etc. | 5.7 | 3.4 | 8 | Pickled vegetables | 0.1 | 0.6 |
| 7 | Biscuits | 5.8 | 2.6 | 9 | Spread cheese and cheese in portions | 0.3 | 0.4 |
| 8 | Chocolates | 3.6 | 2.1 | 10 | Smoked pork meat | 0.4 | 0.4 |
| 9 | Snacks | 1.5 | 1.4 | 11 | Fresh cheese | 0.2 | 0.4 |
| 10 | Sauces | 0.7 | 1.4 | Ultra-processed foods and beverages | |||
| 11 | Breakfast cereals | 1.0 | 0.8 | 1 | Cube soup | 0.1 | 6.1 |
| 12 | Pre-cooked and ready-to-eat meals | 0.5 | 0.7 | 2 | Cold meat | 1.6 | 5.4 |
| 13 | Bakery products | 0.8 | 0.7 | 3 | Pizzas | 2.1 | 4.9 |
| 14 | Pickling vegetables | 0.1 | 0.6 | 4 | Sausages | 1.3 | 4.5 |
| 15 | Pâté | 0.3 | 0.6 | 5 | Sliced bread | 1.9 | 3.6 |
| 16 | Semi-fat pork meat and bacon | 0.9 | 0.4 | 6 | Buns, sweet bread, etc. | 5.7 | 3.4 |
| 17 | Smoked pork meat | 0.4 | 0.4 | 7 | Pre-cooked and ready-to-eat meals | 1.6 | 3.3 |
| 18 | Surimi | 0.1 | 0.4 | 8 | Biscuits | 5.8 | 2.6 |
| 19 | Dairy desserts | 0.8 | 0.4 | 9 | Breakfast cereals | 1.9 | 2.1 |
| 20 | Isotonic drinks | 0.2 | 0.2 | 10 | Chocolates | 3.6 | 2.1 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuadrado-Soto, E.; Peral-Suarez, Á.; Aparicio, A.; Perea, J.M.; Ortega, R.M.; López-Sobaler, A.M. Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile. Nutrients 2018, 10, 1880. https://doi.org/10.3390/nu10121880
Cuadrado-Soto E, Peral-Suarez Á, Aparicio A, Perea JM, Ortega RM, López-Sobaler AM. Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile. Nutrients. 2018; 10(12):1880. https://doi.org/10.3390/nu10121880
Chicago/Turabian StyleCuadrado-Soto, Esther, África Peral-Suarez, Aránzazu Aparicio, Jose M. Perea, Rosa M. Ortega, and Ana M. López-Sobaler. 2018. "Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile" Nutrients 10, no. 12: 1880. https://doi.org/10.3390/nu10121880
APA StyleCuadrado-Soto, E., Peral-Suarez, Á., Aparicio, A., Perea, J. M., Ortega, R. M., & López-Sobaler, A. M. (2018). Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile. Nutrients, 10(12), 1880. https://doi.org/10.3390/nu10121880