Are Gluten-Free Diets More Nutritious? An Evaluation of Self-Selected and Recommended Gluten-Free and Gluten-Containing Dietary Patterns



Abstract
1. Introduction
2. Materials and Methods
2.1. Study 1: Analysis of Healthy Dietary Recommendations Implemented as GF and GC Menus
2.2. Study 2: Literature Review and Meta-Analysis of Self-Reported Dietary Intakes among Individuals Consuming a GF Diet Versus a GC Diet
2.3. Statistical Analysis
3. Results
3.1. Study 1: Analysis of Healthy Dietary Recommendations Implemented as GF and GC Menus
3.2. Study 2: Literature Review and Meta-Analysis of Self-Reported Dietary Intake among Individuals Consuming a Gluten-Free Diet Versus a Gluten-Containing Diet
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Percentage of U.S. Adults Trying to Cut Down or Avoid Gluten in Their Diets Reaches New High in 2013, Reports NBD. Available online: https://www.npd.com/wps/portal/npd/us/news/press-releases/percentage-of-us-adults-trying-to-cut-down-or-avoid-gluten-in-their-diets-reaches-new-high-in-2013-reports-npd/ (accessed on 4 September 2018).
- Rubio-Tapia, A.; Ludvigsson, J.F.; Brantner, T.L.; Murray, J.A.; Everhart, J.E. The prevalence of celiac disease in the United States. Am. J. Gastroenterol. 2012, 107, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Sapone, A.; Bai, J.C.; Ciacci, C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; et al. Spectrum of gluten-related disorders: Consensus on new nomenclature and classification. BMC Med. 2012, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Marcason, W. Is there evidence to support the claim that a gluten-free diet should be used for weight loss? J. Am. Diet. Assoc. 2011, 111, 1786. [Google Scholar] [CrossRef] [PubMed]
- Gaesser, G.A.; Angadi, S.S. Navigating the gluten-free boom. J. Am. Acad. Physician. Assist. 2015, 28. [Google Scholar] [CrossRef] [PubMed]
- De Giorgio, R.; Volta, U.; Gibson, P.R. Sensitivity to wheat, gluten and FODMAPs in IBS: Facts or fiction? Gut 2016, 65, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.; Lasa, A.; Bustamante, M.A.; Churruca, I.; Simon, E. Nutritional differences between a gluten-free diet and a diet containing equivalent products with gluten. Plant Foods Hum. Nutr. 2014, 69, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.H.; Neal, B.; Trevena, H.; Crino, M.; Stuart-Smith, W.; Faulkner-Hogg, K.; Yu Louie, J.C.; Dunford, E. Are gluten-free foods healthier than non-gluten-free foods? An evaluation of supermarket products in Australia. Br. J. Nutr. 2015, 114, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Kulai, T.; Rashid, M. Assessment of Nutritional Adequacy of Packaged Gluten-free Food Products. Can. J. Diet. Pract. Res. 2014, 75, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Scientific report of the 2015 Dietary Guidelines Advisory Committee. Available online: https://health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 20 March 2015).
- Roberts, S.B.; Lucas, A. Measurement of urinary constituents and output using disposable diapers. Arch. Dis. Child. 1985, 60, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Della Valle, N.; Rosania, R.; Facciorusso, A.; Trotta, A.; Cantatore, F.P.; Falco, S.; Pignatiello, S.; Viggiani, M.T.; Amoruso, A.; et al. A comparison of the nutritional status between adult celiac patients on a long-term, strictly gluten-free diet and healthy subjects. Eur. J. Clin. Nutr. 2016, 70, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Dall’Asta, C.; Scarlato, A.P.; Galaverna, G.; Brighenti, F.; Pellegrini, N. Dietary exposure to fumonisins and evaluation of nutrient intake in a group of adult celiac patients on a gluten-free diet. Mol. Nutr. Food Res. 2012, 56, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Grehn, S.; Fridell, K.; Lilliecreutz, M.; Hallert, C. Dietary habits of Swedish adult coeliac patients treated by a gluten-free diet for 10 years. Näringsforskning 2001, 45, 178–182. [Google Scholar] [CrossRef]
- Kemppainen, T.; Kroger, H.; Janatuinen, E.; Arnala, I.; Kosma, V.M.; Pikkarainen, P.; Julkunen, R.; Jurvelin, J.; Alhava, E.; Uusitupa, M. Osteoporosis in adult patients with celiac disease. Bone 1999, 24, 249–255. [Google Scholar] [CrossRef]
- Kinsey, L.; Burden, S.T.; Bannerman, E. A dietary survey to determine if patients with coeliac disease are meeting current healthy eating guidelines and how their diet compares to that of the British general population. Eur. J. Clin. Nutr. 2008, 62, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Valente, F.X.; Campos Tdo, N.; Moraes, L.F.; Hermsdorff, H.H.; Cardoso Lde, M.; Pinheiro-Sant’Ana, H.M.; Gilberti, F.A.; Peluzio Mdo, C. B vitamins related to homocysteine metabolism in adults celiac disease patients: A cross-sectional study. Nutr. J. 2015, 14, 110. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Robins, G.G.; Burley, V.J.; Howdle, P.D. Evidence of high sugar intake, and low fibre and mineral intake, in the gluten-free diet. Liment. Pharmacol. Ther. 2010, 32, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Kautto, E.; Ryden, P.J.; Ivarsson, A.; Olsson, C.; Norstrom, F.; Hogberg, L.; Carlsson, A.; Hagfors, L.; Hornell, A. What happens to food choices when a gluten-free diet is required? A prospective longitudinal population-based study among Swedish adolescent with coeliac disease and their peers. J. Nutr. Sci. 2014, 3, e2. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Gibson, P.R. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J. Hum. Nutr. Diete. 2013, 26, 349–358. [Google Scholar] [CrossRef] [PubMed]
- McRorie, J.W., Jr. Evidence-Based Approach to Fiber Supplements and Clinically Meaningful Health Benefits, Part 1: What to Look for and How to Recommend an Effective Fiber Therapy. Nutr. Today 2015, 50, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Halfdanarson, T.R.; Litzow, M.R.; Murray, J.A. Hematologic manifestations of celiac disease. Blood 2007, 109, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.K. Dietary Salt Intake and Hypertension. Electrolyte Blood Press. 2014, 12, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Grant, C.; Grehn, S.; Granno, C.; Hulten, S.; Midhagen, G.; Strom, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar]
- Ciacci, C.; Cirillo, M.; Cavallaro, R.; Mazzacca, G. Long-term follow-up of celiac adults on gluten-free diet: Prevalence and correlates of intestinal damage. Digestion 2002, 66, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Bardella, M.T.; Fredella, C.; Prampolini, L.; Molteni, N.; Giunta, A.M.; Bianchi, P.A. Body composition and dietary intakes in adult celiac disease patients consuming a strict gluten-free diet. Am. J. Clin. Nutr. 2000, 72, 937–939. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Meal | Gluten Containing | Gluten Free |
|---|---|---|
| Breakfast | 1 whole wheat English muffin | 1 GF brown rice English muffin |
| 1 tbsp all-fruit preserves | 1 tbsp all-fruit preserves | |
| 1 hard-cooked egg | 1 hard-cooked egg | |
| Beverage: 1 cup water, coffee, or tea | Beverage: 1 cup water, coffee, or tea | |
| Lunch | White bean-vegetable soup: | White bean-vegetable soup: |
| 1 ¼ cup chunky vegetable soup with pasta | 1 ¼ cup GF vegetable noodle soup | |
| ½ cup white beans | ½ cup white beans | |
| 6 saltine crackers | 6 GF table crackers | |
| ½ cup celery sticks | ½ cup celery sticks | |
| Beverage: 1 cup fat-free milk | Beverage: 1 cup fat-free milk | |
| Dinner | Rigatoni with meat sauce: | Rigatoni with meat sauce: |
| 1 cup rigatoni pasta (2 oz dry) | 1 cup GF fusilli (2 oz dry) | |
| 2 ounces cooked ground beef | 2 ounces cooked ground beef | |
| (95% lean) | (95% lean) | |
| 2 tsp corn/canola oil (to cook beef) | 2 tsp corn/canola oil (to cook beef) | |
| ½ cup tomato sauce | ½ cup tomato sauce | |
| 3 tbsp grated parmesan cheese Spinach salad: | 3 tbsp grated parmesan cheese Spinach salad: | |
| 1 cup raw spinach leaves | 1 cup raw spinach leaves | |
| ½ cup tangerine sections | ½ cup tangerine sections | |
| ½ ounce chopped walnuts | ½ ounce chopped walnuts | |
| 4 tsp oil and vinegar dressing | 4 tsp oil and vinegar dressing | |
| Beverage: 1 cup water, coffee, or tea | Beverage: 1 cup water, coffee, or tea | |
| Snacks | 1 cup nonfat fruit yogurt | 1 cup nonfat fruit yogurt |
| Nutrient | Gluten Free (Mean ± SD a) | Gluten Containing (Mean ± SD a) | p Value b |
|---|---|---|---|
| Energy (calories) | 1979 ± 211 | 1991 ± 209 | 0.31 |
| Total Carbohydrates (g) | 275 ± 53 | 265 ± 66 | 0.23 |
| Total Protein (g) | 88 ± 14 | 96 ± 11 | 0.002 |
| Total Fat (g) | 64 ± 15 | 62 ± 16 | 0.06 |
| Saturated Fat (g) | 23 ± 10 | 22 ± 10 | 0.18 |
| Fiber (g) | 30 ± 6 | 31 ± 7 | 0.84 |
| Vitamin A (IU) | 14117 ± 12285 | 14085 ± 12292 | 0.88 |
| Vitamin C (mg) | 148 ± 80 | 147 ± 79 | 0.33 |
| Vitamin E (IU) | 6 ± 2 | 7 ± 3 | 0.02 |
| Folate (μg) | 259 ± 81 | 340 ± 114 | 0.02 |
| Calcium (mg) | 1578 ± 275 | 1639 ± 265 | 0.08 |
| Magnesium (mg) | 350 ± 69 | 409 ± 68 | 0.004 |
| Potassium (mg) | 4009 ± 700 | 4228 ± 785 | 0.01 |
| Sodium (mg) | 2124 ± 597 | 2494 ± 765 | 0.03 |
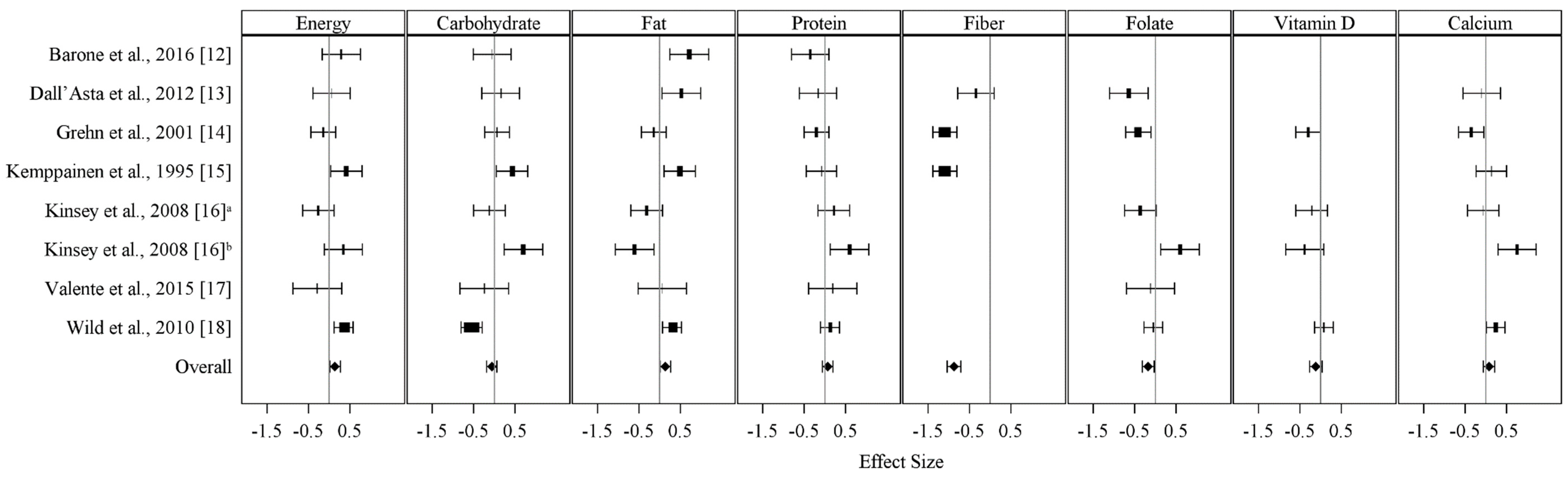
| Nutrient | Number of Studies | Mean Effect Size (95% CI) a | p Value b | p Value c |
|---|---|---|---|---|
| Energy (calories) | 7 | 0.14 (0.02, 0.27) | 0.03 | 0.24 |
| Total Carbohydrates | 7 | −0.06 (−0.19, 0.06) | 0.33 | 0.79 |
| Total Protein | 7 | 0.07 (−0.06, 0.19) | 0.29 | - |
| Total Fat | 7 | 0.14 (0.01, 0.26) | 0.03 | 0.44 |
| Fiber | 3 | −0.88 (−1.04, −0.71) | <0.001 | <0.001 |
| Folate | 5 | −0.17 (−0.31, −0.03) | 0.02 | 0.06 |
| Calcium | 5 | 0.08 (−0.06, 0.21) | 0.26 | 0.60 |
| Vitamin D | 3 | 0.12 (−0.27, 0.03) | 0.13 | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taetzsch, A.; Das, S.K.; Brown, C.; Krauss, A.; Silver, R.E.; Roberts, S.B. Are Gluten-Free Diets More Nutritious? An Evaluation of Self-Selected and Recommended Gluten-Free and Gluten-Containing Dietary Patterns. Nutrients 2018, 10, 1881. https://doi.org/10.3390/nu10121881
Taetzsch A, Das SK, Brown C, Krauss A, Silver RE, Roberts SB. Are Gluten-Free Diets More Nutritious? An Evaluation of Self-Selected and Recommended Gluten-Free and Gluten-Containing Dietary Patterns. Nutrients. 2018; 10(12):1881. https://doi.org/10.3390/nu10121881
Chicago/Turabian StyleTaetzsch, Amy, Sai Krupa Das, Carrie Brown, Amy Krauss, Rachel E. Silver, and Susan B. Roberts. 2018. "Are Gluten-Free Diets More Nutritious? An Evaluation of Self-Selected and Recommended Gluten-Free and Gluten-Containing Dietary Patterns" Nutrients 10, no. 12: 1881. https://doi.org/10.3390/nu10121881
APA StyleTaetzsch, A., Das, S. K., Brown, C., Krauss, A., Silver, R. E., & Roberts, S. B. (2018). Are Gluten-Free Diets More Nutritious? An Evaluation of Self-Selected and Recommended Gluten-Free and Gluten-Containing Dietary Patterns. Nutrients, 10(12), 1881. https://doi.org/10.3390/nu10121881