Cross-Sectional and Longitudinal Association between Glycemic Status and Body Composition in Men: A Population-Based Study


Abstract

1. Introduction
2. Materials and Methods
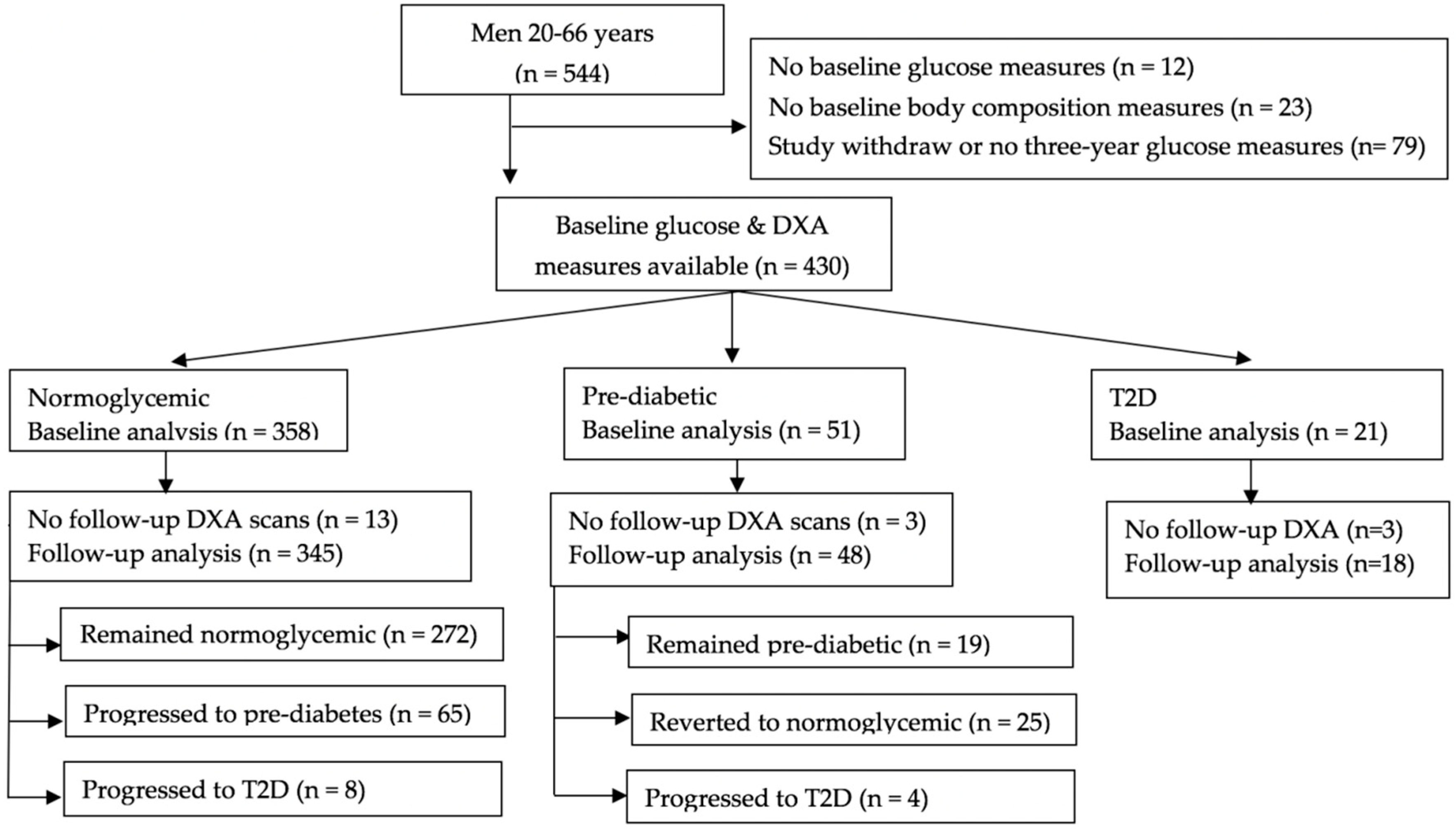
2.1. Study Population
2.2. Assessment of Covariates
2.2.1. Anthropometric Measures
2.2.2. Physical Activity Assessment
2.2.3. Dietary Assessment
2.3. Ascertainment of Glycemic Status
2.4. Body Composition Measurements
2.5. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Cross-Sectional Assessment of Baseline Body Composition in Men with Prediabetes or Type 2 Diabetes
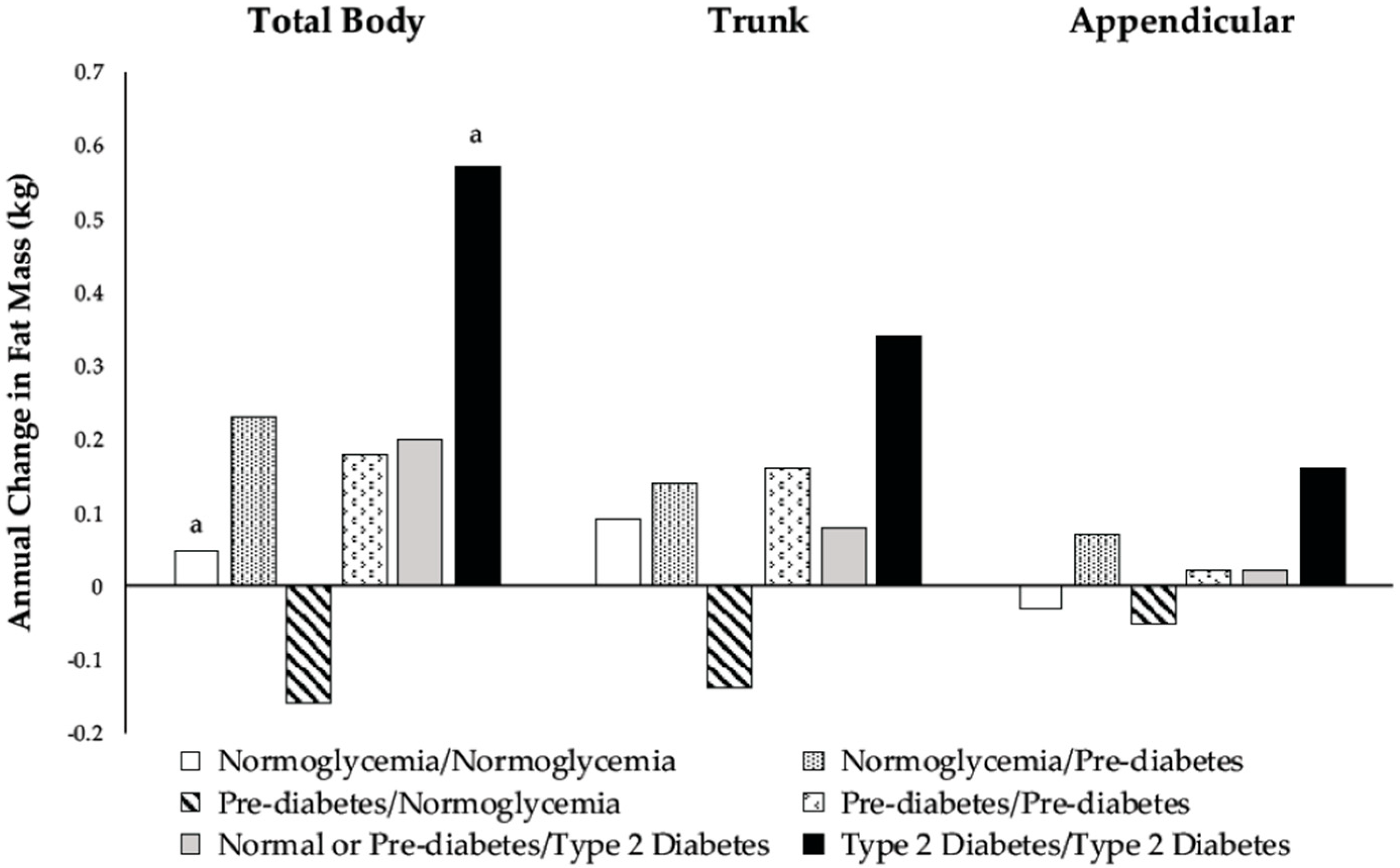
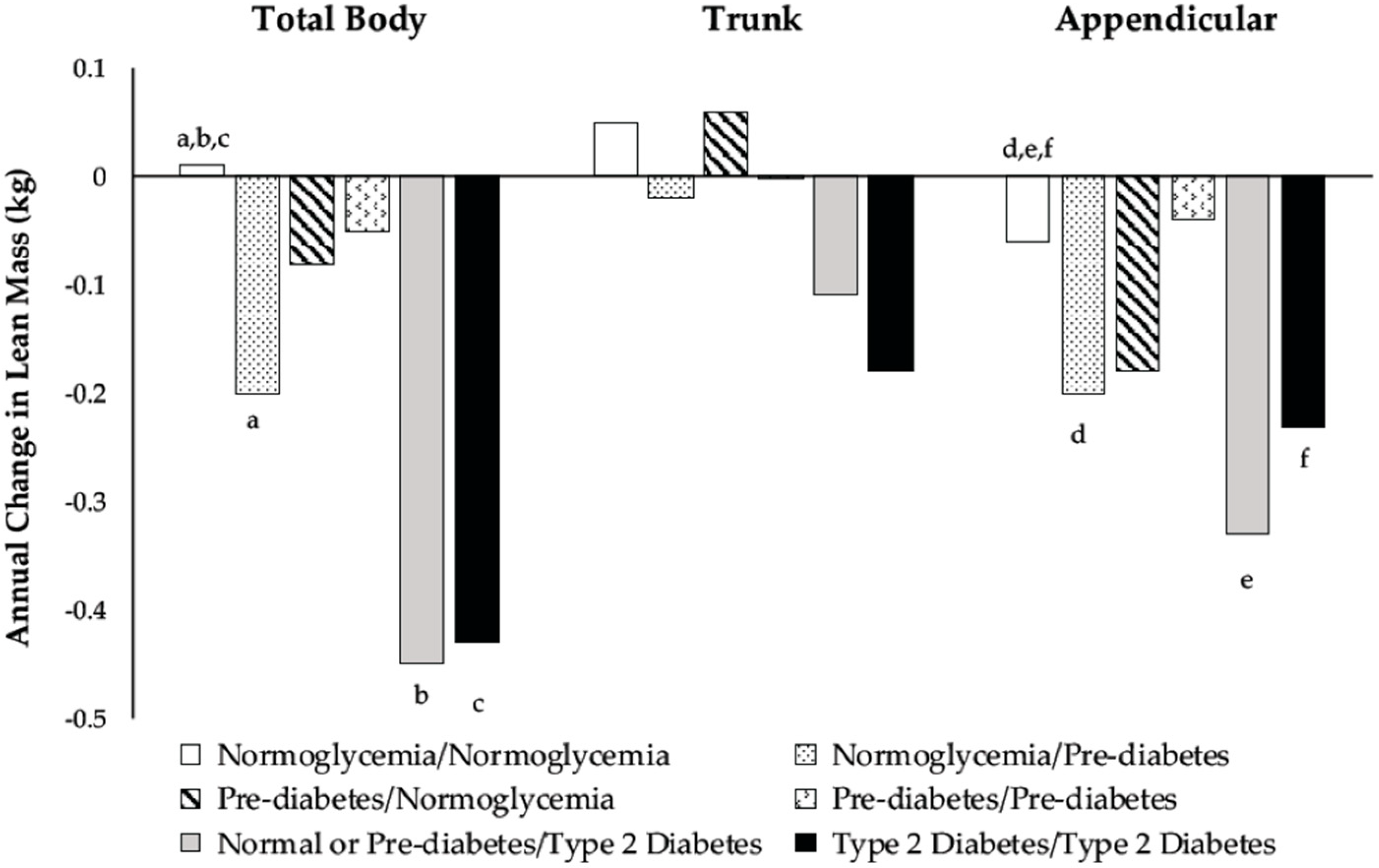
3.3. Association between Development of Prediabetes and Type 2 Diabetes and Changes in Body Composition
3.4. Changes in Body Composition among Prediabetic Men Depending on Reversion to Normoglycemia
3.5. Changes in Body Composition among Type 2 Diabetic Men
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cowie, C.C.; Rust, K.F.; Ford, E.S.; Eberhardt, M.S.; Byrd-Holt, D.D.; Li, C.; Williams, D.E.; Gregg, E.W.; Bainbridge, K.E.; Saydah, S.H. Full accounting of diabetes and pre-diabetes in the US population in 1988–1994 and 2005–2006. Diabetes Care 2009, 32, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and its Burden in the United States, 2014; US Department of Health and Human Services: Atlanta, GA, USA, 2014.
- Centers for Disease Control and Prevention. Prediabetes: Could It Be You? Available online: http://www.cdc.gov/diabetes/pubs/images/prediabetes-inforgraphic.jpg (accessed on 12 July 2017).
- O’Brien, M.J.; Whitaker, R.C.; Yu, D.; Ackermann, R.T. The comparative efficacy of lifestyle intervention and metformin by educational attainment in the Diabetes Prevention Program. Prev. Med. 2015, 77, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Steeves, J.A.; Murphy, R.A.; Crainiceanu, C.M.; Zipunnikov, V.; Van Domelen, D.R.; Harris, T.B. Daily patterns of physical activity by type 2 diabetes definition: Comparing diabetes, prediabetes, and participants with normal glucose levels in nhanes 2003–2006. Prev. Med. Rep. 2015, 2, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Rabijewski, M.; Papierska, L.; Piątkiewicz, P. The relationships between anabolic hormones and body composition in middle-aged and elderly men with prediabetes: A cross-sectional study. J. Diabetes Res. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Heshka, S.; Ruggiero, A.; Bray, G.A.; Foreyt, J.; Kahn, S.E.; Lewis, C.E.; Saad, M.; Schwartz, A.V. Altered body composition in type 2 diabetes mellitus. Int. J. Obes. (Lond.) 2008, 32, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Azuma, K.; Heilbronn, L.K.; Albu, J.B.; Smith, S.R.; Ravussin, E.; Kelley, D.E. Adipose tissue distribution in relation to insulin resistance in type 2 diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E435–E442. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Verdijk, L.B.; van der Hoeven, L.; Adam, J.J.; van Kranenburg, J.; Nilwik, R.; van Loon, L.J. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J. Am. Med. Dir. Assoc. 2013, 14, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Tra, Y.; Egan, J.; Ferrucci, L.; Brancati, F. Hyperglycemia is associated with relatively lower lean body mass in older adults. J. Nutr. Health Aging 2014, 18, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Boyko, E.J.; Strotmeyer, E.S.; Lewis, C.E.; Cawthon, P.M.; Hoffman, A.R.; Everson-Rose, S.A.; Barrett-Connor, E.; Orwoll, E.S. Association between insulin resistance and lean mass loss and fat mass gain in older men without diabetes mellitus. J. Am. Geriatr. Soc. 2011, 59, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Pownall, H.J.; Bray, G.A.; Wagenknecht, L.E.; Walkup, M.P.; Heshka, S.; Hubbard, V.S.; Hill, J.; Kahn, S.E.; Nathan, D.M.; Schwartz, A.V. Changes in body composition over 8 years in a randomized trial of a lifestyle intervention: The Look Ahead Study. Obesity 2015, 23, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Pownall, H.J.; Schwartz, A.V.; Bray, G.A.; Berkowitz, R.I.; Lewis, C.E.; Boyko, E.J.; Jakicic, J.M.; Chen, H.; Heshka, S.; Gregg, E.W. Changes in regional body composition over 8 years in a randomized lifestyle trial: The Look Ahead Study. Obesity 2016, 24, 1899–1905. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.G.; Boyko, E.J.; Barrett-Connor, E.; Miljkovic, I.; Hoffman, A.R.; Everson-Rose, S.A.; Lewis, C.E.; Cawthon, P.M.; Strotmeyer, E.S.; Orwoll, E.S. Insulin sensitizers may attenuate lean mass loss in older men with diabetes. Diabetes Care 2011, 34, 2381–2386. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Lee, J.S.; Kuller, L.H.; Boudreau, R.; De Rekeneire, N.; Harris, T.B.; Kritchevsky, S.; Tylavsky, F.A.; Nevitt, M. Excessive loss of skeletal muscle mass in older adults with type 2 diabetes. Diabetes Care 2009, 32, 1993–1997. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Metter, E.J.; Egan, J.; Golden, S.H.; Ferrucci, L. Hyperglycemia predicts persistently lower muscle strength with aging. Diabetes Care 2015, 38, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Specker, B.; Binkley, T.; Fahrenwald, N. Rural versus nonrural differences in BMC, volumetric BMD, and bone size: A population-based cross-sectional study. Bone 2004, 35, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S.; Wing, A.L.; Hyde, R.T. Physical activity as an index of heart attack risk in college alumni. Am. J. Epidemiol. 1978, 108, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.; Parker, B.; Capizzi, J.; Thompson, P.; Clarkson, P.; Freedson, P.; Pescatello, L.S. Validity and reliability question 8 of the Paffenbarger physical activity questionnaire among healthy adults. J. Phys. Act. Health 2015, 12, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Samra, H.A.; Beare, T.; Specker, B. Pedometer readings and self-reported walking distances in a rural Hutterite population. J. Rural Health 2008, 24, 99–100. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and diagnosis of diabetes. Sec. 2. In standards of medical care in diabetes—2015. Diabetes Care 2015, 38, S8–S16. [Google Scholar]
- Kim, T.N.; Park, M.S.; Yang, S.J.; Yoo, H.J.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H. Prevalence and determinant factors of sarcopenia in patients with type 2 diabetes: The Korean Sarcopenic Obesity Study (KSOS). Diabetes Care 2010, 33, 1497–1499. [Google Scholar] [CrossRef] [PubMed]
- Julian, V.; Blondel, R.; Pereira, B.; Thivel, D.; Boirie, Y.; Duclos, M. Body composition is altered in pre-diabetic patients with impaired fasting glucose tolerance: Results from the NHANES survey. J. Clin. Med. Res. 2017, 9, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Heshka, S.; Albu, J.; Heymsfield, S.; Kuznia, P.; Harris, T.; Gallagher, D. Intermuscular adipose tissue rivals visceral adipose tissue in independent associations with cardiovascular risk. Int. J. Obes. (Lond.) 2007, 31, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Aguiari, P.; Leo, S.; Zavan, B.; Vindigni, V.; Rimessi, A.; Bianchi, K.; Franzin, C.; Cortivo, R.; Rossato, M.; Vettor, R. High glucose induces adipogenic differentiation of muscle-derived stem cells. Proc. Natl. Acad. Sci. USA 2008, 105, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-P.; Reid, M.B. Nf-κb mediates the protein loss induced by TNF-α in differentiated skeletal muscle myotubes. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R1165–R1170. [Google Scholar] [CrossRef] [PubMed]
- Wåhlin-Larsson, B.; Wilkinson, D.J.; Strandberg, E.; Hosford-Donovan, A.; Atherton, P.J.; Kadi, F. Mechanistic links underlying the impact of c-reactive protein on muscle mass in elderly. Cell Physiol. Biochem. 2017, 44, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Volpato, S. Muscle dysfunction in type 2 diabetes: A major threat to patient’s mobility and independence. Acta Diabetol. 2016, 53, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Piaggi, P.; Thearle, M.S.; Bogardus, C.; Krakoff, J. Fasting hyperglycemia predicts lower rates of weight gain by increased energy expenditure and fat oxidation rate. J. Clin. Endocrinol. Metab. 2015, 100, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Frayn, K.N. Visceral fat and insulin resistance—causative or correlative? Br. J. Nutr. 2000, 83, S71–S77. [Google Scholar] [CrossRef] [PubMed]
- Brøns, C.; Grunnet, L.G. Mechanisms in endocrinology: Skeletal muscle lipotoxicity in insulin resistance and type 2 diabetes: A causal mechanism or an innocent bystander? Eur. J. Endocrinol. 2017, 176, R67–R78. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Moshfegh, A.J. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: An observational validation study. J. Am. Diet. Assoc. 2004, 104, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Casagrande, S.; Geiss, L.; Cowie, C.C. Prevalence of and trends in diabetes among adults in the United States, 1988–2012. JAMA 2015, 314, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Rust, K.F.; Cowie, C.C. Diabetes based on 2-h plasma glucose among those classified as having prediabetes based on fasting plasma glucose or A1c. Diab. Vasc. Dis. Res. 2018, 15, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Cowie, C.C.; Rust, K.F.; Byrd-Holt, D.D.; Eberhardt, M.S.; Flegal, K.M.; Engelgau, M.M.; Saydah, S.H.; Williams, D.E.; Geiss, L.S.; Gregg, E.W. Prevalence of diabetes and impaired fasting glucose in adults in the US population. Diabetes Care 2006, 29, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Cowie, C.C.; Rust, K.F.; Byrd-Holt, D.D.; Gregg, E.W.; Ford, E.S.; Geiss, L.S.; Bainbridge, K.E.; Fradkin, J.E. Prevalence of diabetes and high risk for diabetes using A1c criteria in the US population in 1988–2006. Diabetes Care 2010, 33, 562–568. [Google Scholar] [CrossRef] [PubMed]
- DECODE Study Group. Age-and sex-specific prevalences of diabetes and impaired glucose regulation in 13 European cohorts1. Diabetes Care 2003, 26, 61–69. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration. Effects of diabetes definition on global surveillance of diabetes prevalence and diagnosis: A pooled analysis of 96 population-based studies with 331 288 participants. Lancet Diabetes Endocrinol. 2015, 3, 624–637. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normoglycemic | Prediabetic | T2D | p-Value 1 | |
|---|---|---|---|---|
| Participants (n) | 358 | 51 | 21 | |
| Demographics | ||||
| Age (years) | 41.6 ± 0.6 a | 45.8 ± 1.7 | 53.0 ± 2.6 a | <0.001 |
| Population Group (%) | 0.001 | |||
| Hutterite (n = 161) | 73.3 | 18.0 | 8.7 | |
| NH Rural (n = 160) | 89.3 | 8.8 | 1.9 | |
| NH Non-rural (n = 109) | 89.0 | 7.3 | 3.7 | |
| Ever Married (%) | 81.3 | 92.2 | 95.2 | 0.06 |
| Anthropometrics | ||||
| Height (cm) | 177.9 ± 0.4 | 177.9 ± 0.9 | 174.3 ± 1.5 | 0.06 |
| Weight (kg) | 91.1 ± 0.8 a | 98.5 ± 2.1 a | 95.9 ± 3.3 | 0.003 |
| Lifestyle Variables | ||||
| Smokers (%) | 33.2 | 24.0 | 38.1 | 0.43 |
| BP Meds (%) | 8.7 | 23.5 | 47.6 | <0.001 |
| % Time in MVPA 2 | 21.8 ± 0.5 | 23.1 ± 1.4 | 19.3 ± 2.1 | 0.32 |
| Daily Macronutrient Intake 2 | ||||
| Total energy (kcal) | 2373 ± 33 | 2218 ± 87 | 2060 ± 135 | 0.03 3 |
| Carbohydrate (g) | 265 ± 5 ab | 224 ± 12 b | 202 ± 19 a | <0.001 |
| Fat (g) | 97 ± 2 | 98 ± 4 | 90 ± 7 | 0.55 |
| Protein (g) | 105 ± 2 | 102 ± 4 | 102 ± 7 | 0.80 |
| Baseline: | Normoglycemic | Prediabetic | Normoglycemic or Prediabetic | T2D | |||
|---|---|---|---|---|---|---|---|
| Follow-Up: | Normoglycemic | Prediabetic | Normoglycemic | Prediabetic | T2D | T2D | p-Value 1 |
| Participants (n) | 272 | 65 | 25 | 19 | 12 | 18 | |
| Baseline Age (years) | 41.0 ± 0.7 ab | 42.6 ± 1.5 c | 43.9 ± 2.6 | 47.1 ± 2.3 | 51.9 ± 2.3 b | 53.0 ± 2.2 ac | <0.001 |
| Baseline Height (cm) | 177.9 ± 0.4 | 177.0 ± 0.8 | 179.4 ± 1.0 | 176.9 ± 2.0 | 175.3 ± 1.7 | 175.1 ± 1.7 | 0.17 |
| Weight (kg) | |||||||
| Baseline | 90.3 ± 0.9 ‡ | 92.5 ± 2.0 | 96.1 ± 3.3 | 98.8 ± 3.9 | 100.4 ± 4.1 | 96.0 ± 3.1 | 0.01 3 |
| Follow-Up | 91.5 ± 0.9 | 93.3 ± 2.0 | 95.2 ± 3.4 | 100.1 ± 4.3 | 98.3 ± 4.0 | 96.0 ± 3.3 | 0.08 |
| % Time MVPA 2 | |||||||
| Baseline | 21.0 ± 0.6 ‡ | 23.7 ± 1.2 | 22.6 ± 1.7 | 24.4 ± 2.3 | 26.2 ± 3.0 | 19.8 ± 2.1 | 0.11 |
| Follow-Up | 22.5 ± 0.6 | 22.1 ± 1.1 | 19.9 ± 1.6 | 21.9 ± 2.1 | 24.5 ± 2.5 | 22.8 ± 2.4 | 0.77 |
| Daily Intake 2 | |||||||
| Total Energy (kcal) | |||||||
| Baseline | 2344 ± 38 | 2435 ± 75 | 2284 ± 130 | 2140 ± 106 | 2248 ± 183 | 2067 ± 108 | 0.18 |
| Follow-Up | 2382 ± 38 a | 2386 ± 81 b | 2268 ± 102 | 2211 ± 95 | 2176 ± 189 | 1898 ± 132 ab | 0.02 |
| Carbohydrate (g) | |||||||
| Baseline | 263 ± 5 a | 268 ± 11 | 239 ± 17 | 208 ± 14 ‡ | 233 ± 21 | 204 ± 15 a | 0.003 |
| Follow-Up | 265 ± 5 a | 267 ± 13 b | 248 ± 16 | 232 ± 14 | 208 ± 19 | 186 ± 16 ab | 0.001 |
| Fat (g) | |||||||
| Baseline | 95 ± 2 | 102 ± 4 | 101 ± 7 | 94 ± 6 | 94 ± 10 | 91 ± 8 | 0.57 |
| Follow-Up | 101 ± 2 ‡ | 100 ± 3 | 95 ± 5 | 98 ± 6 | 99 ± 11 | 90 ± 8 | 0.75 |
| Protein (g) | |||||||
| Baseline | 103 ± 2 | 107 ± 4 | 105 ± 7 | 96 ± 5 | 101 ± 11 | 101 ± 6 | 0.79 |
| Follow-Up | 104 ± 2 | 106 ± 3 | 105 ± 5 | 98 ± 5 | 107 ± 11 | 93 ± 8 | 0.50 |
| Normoglycemic | Prediabetic | T2D | p-Value 1 | |
|---|---|---|---|---|
| Participants (n) | 358 | 51 | 21 | |
| Body Weight (kg) | ||||
| Unadjusted Model | 91.1 ± 0.8 a | 98.5 ± 2.1 a | 95.9 ± 3.3 | 0.003 |
| Basic Model 2 | 91.0 ± 0.8 a | 97.0 ± 3.2 a | 95.9 ± 3.2 | 0.01 |
| Fat Mass (kg) | ||||
| Total Body | ||||
| Unadjusted Model | 22.1 ± 0.5 ab | 26.4 ± 1.2 b | 26.7 ± 1.9 a | 0.001 |
| Full Model 3 | 22.6 ± 0.3 | 24.0 ± 0.9 | 23.3 ± 1.5 | 0.38 |
| Trunk | ||||
| Unadjusted Model | 11.4 ± 0.3 ab | 14.2 ± 0.8 b | 15.1 ± 1.2 a | <0.001 |
| Full Model 3 | 11.8 ± 0.2 | 12.6 ± 0.5 | 11.8 ± 0.9 | 0.38 |
| Appendicular | ||||
| Unadjusted Model | 9.6 ± 0.2 a | 11.1 ± 0.5 a | 10.4 ± 0.8 | 0.01 |
| Full Model 3 | 9.7 ± 0.2 | 10.3 ± 0.4 | 10.1 ± 0.7 | 0.66 |
| Lean Mass (kg) | ||||
| Total Body | ||||
| Unadjusted Model | 67.0 ± 0.4 | 69.9 ± 1.2 | 66.8 ± 1.8 | 0.07 |
| Full Model 4 | 67.1 ± 0.3 | 67.9 ± 0.8 | 67.9 ± 1.2 | 0.56 |
| Trunk | ||||
| Unadjusted Model | 32.7 ± 0.2 a | 34.5 ± 0.6 a | 34.1 ± 0.9 | 0.01 |
| Full Model 4 | 32.7 ± 0.1 | 33.1 ± 0.4 | 33.8 ± 0.6 | 0.24 |
| Appendicular | ||||
| Unadjusted Model | 30.5 ± 0.2 | 31.6 ± 0.6 a | 28.9 ± 0.9 a | 0.04 |
| Full Model 4 | 30.5 ± 0.2 | 31.0 ± 0.4 | 30.3 ± 0.7 | 0.44 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almusaylim, K.; Minett, M.; Binkley, T.L.; Beare, T.M.; Specker, B. Cross-Sectional and Longitudinal Association between Glycemic Status and Body Composition in Men: A Population-Based Study. Nutrients 2018, 10, 1878. https://doi.org/10.3390/nu10121878
Almusaylim K, Minett M, Binkley TL, Beare TM, Specker B. Cross-Sectional and Longitudinal Association between Glycemic Status and Body Composition in Men: A Population-Based Study. Nutrients. 2018; 10(12):1878. https://doi.org/10.3390/nu10121878
Chicago/Turabian StyleAlmusaylim, Khaleal, Maggie Minett, Teresa L. Binkley, Tianna M. Beare, and Bonny Specker. 2018. "Cross-Sectional and Longitudinal Association between Glycemic Status and Body Composition in Men: A Population-Based Study" Nutrients 10, no. 12: 1878. https://doi.org/10.3390/nu10121878
APA StyleAlmusaylim, K., Minett, M., Binkley, T. L., Beare, T. M., & Specker, B. (2018). Cross-Sectional and Longitudinal Association between Glycemic Status and Body Composition in Men: A Population-Based Study. Nutrients, 10(12), 1878. https://doi.org/10.3390/nu10121878