Efficacy of Lactobacillus Administration in School-Age Children with Asthma: A Randomized, Placebo-Controlled Trial



Abstract
1. Introduction
2. Materials and Methods
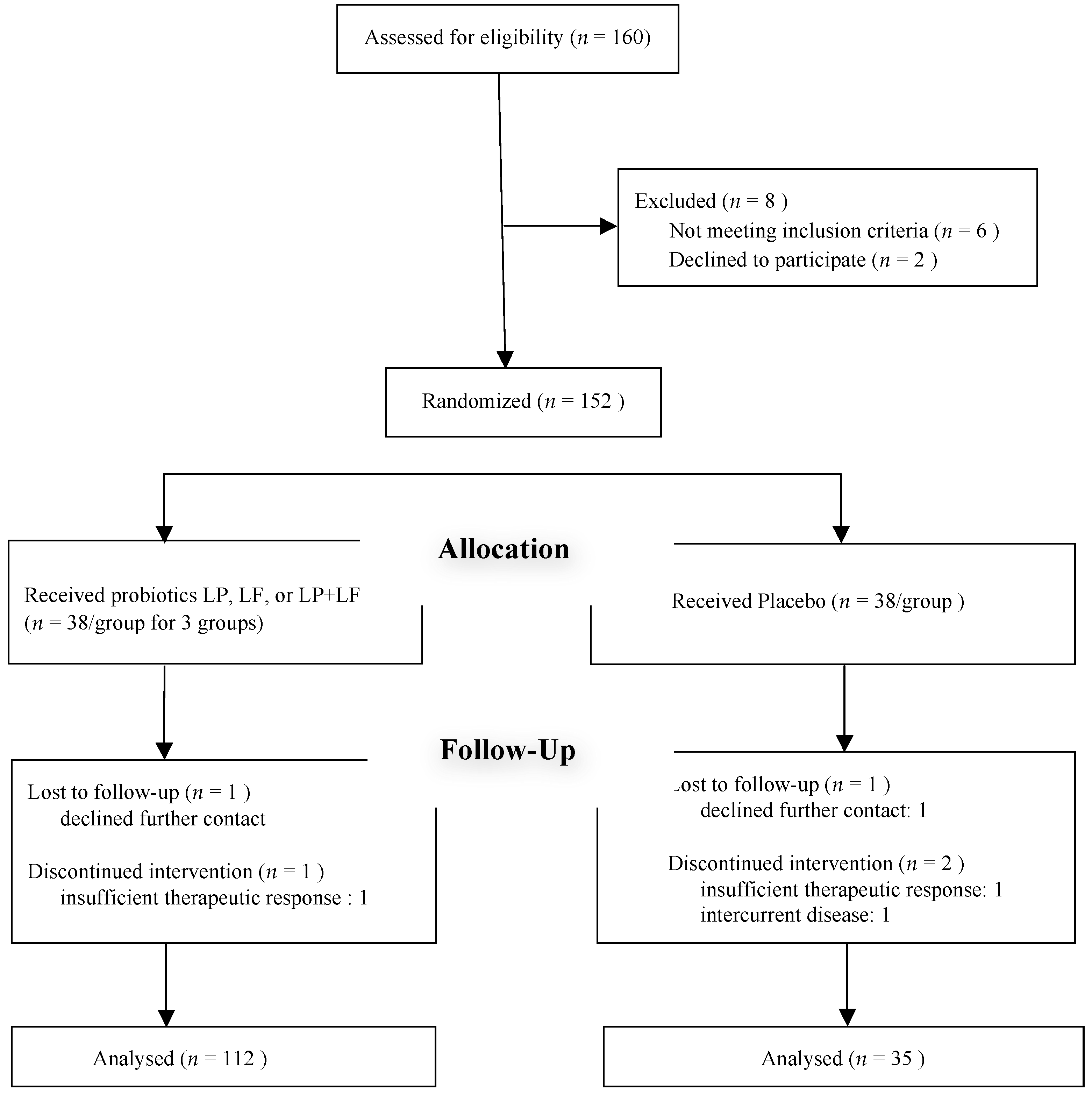
2.1. Participants
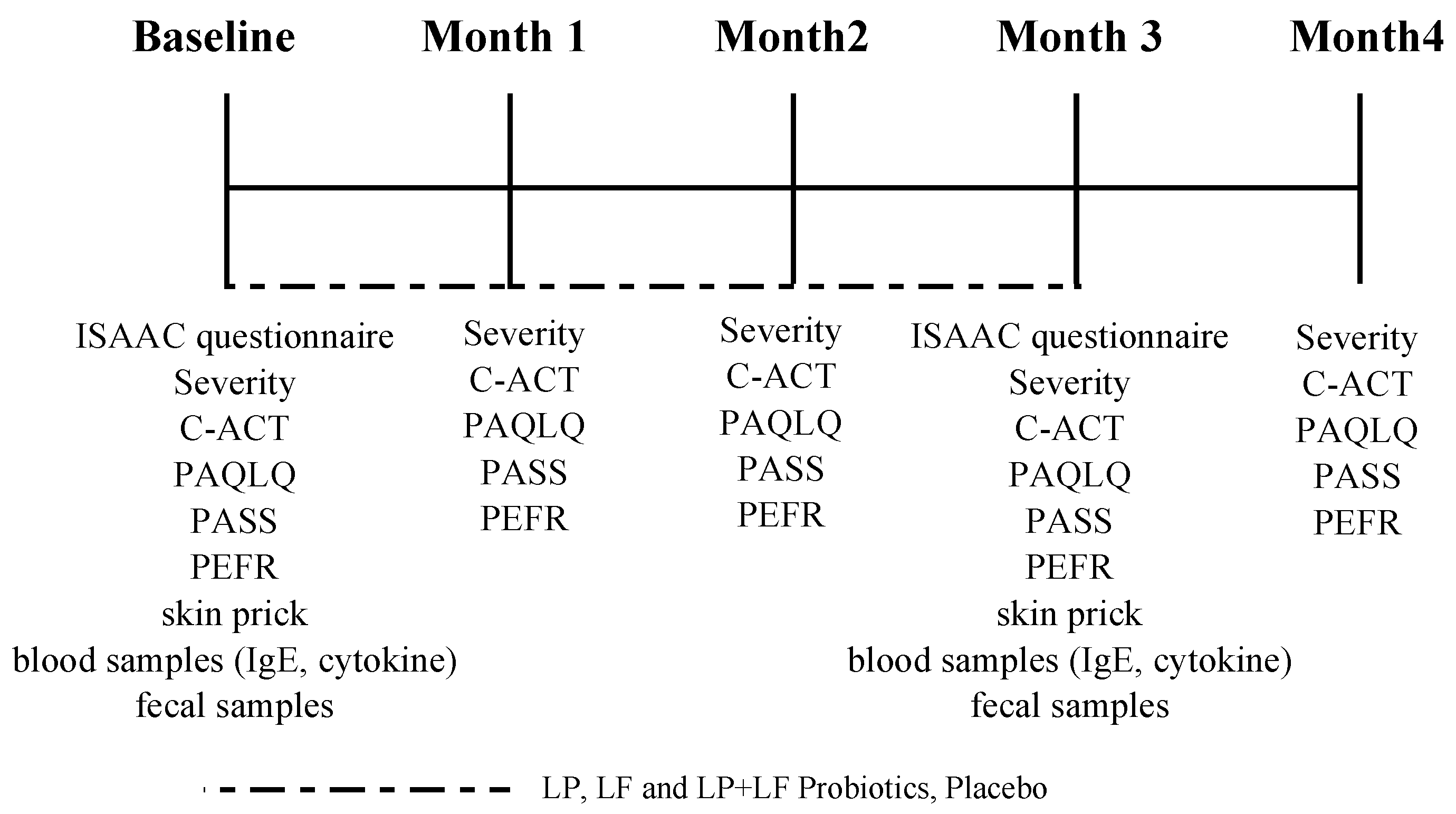
2.2. Protocol
2.3. Outcome Measures
2.4. Laboratory Methods
2.5. Sample Size Estimation
2.6. Statistical Analysis
3. Result
3.1. Baseline Characteristics of Participants
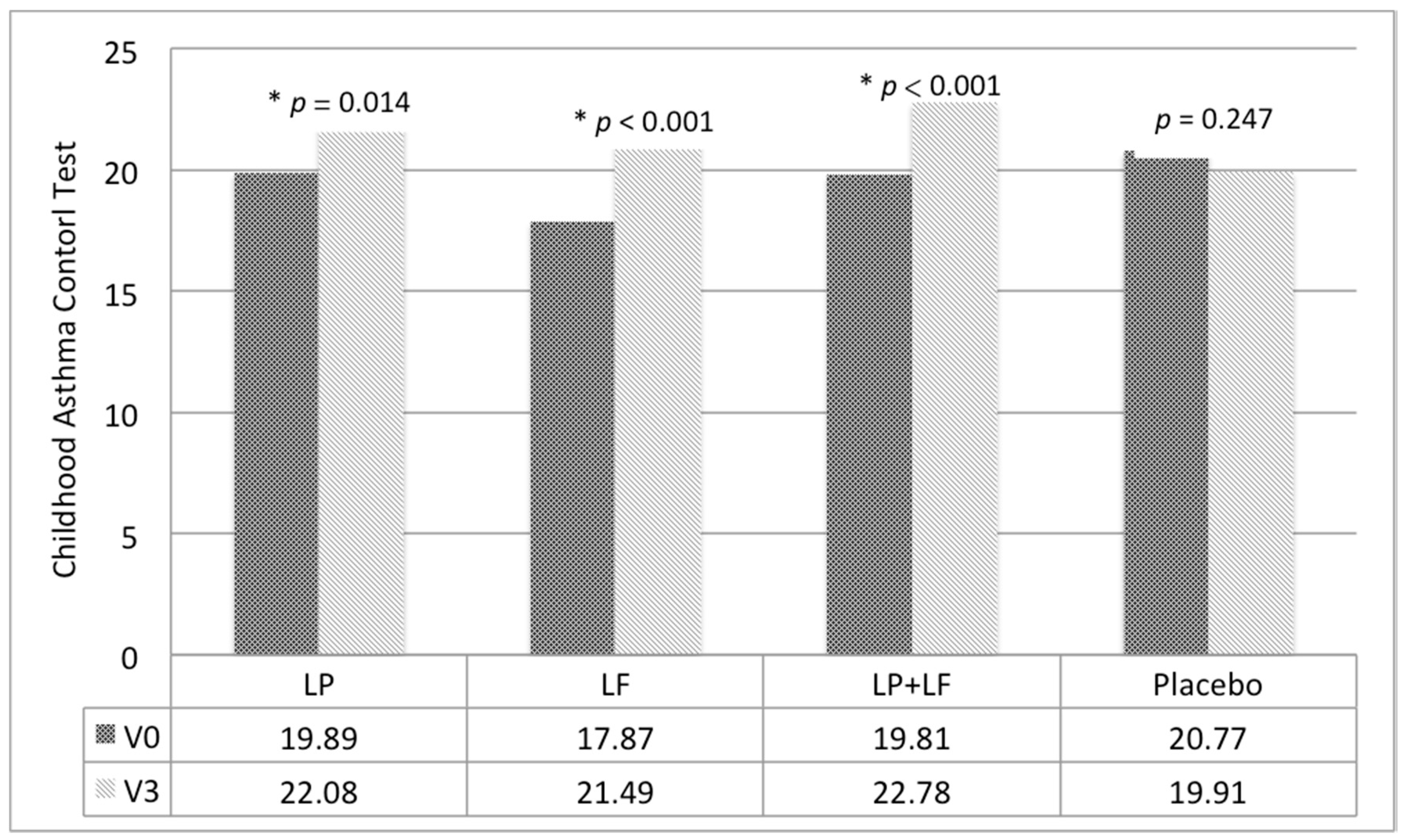
3.2. Effects of Probiotics on Severity of Asthma and Quality of Life
3.3. Effects of Probiotics on Sensitization and Immune Biomarker Levels
3.4. Fecal Microbial Composition, Rescue Medication Use and Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shifren, A.; Witt, C.; Christie, C.; Castro, M. Mechanisms of remodeling in asthmatic airways. J. Allergy (Cairo) 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, H.Y.; Lee, S.Y.; Seo, J.H.; Lee, E.; Hong, S.J. Clinical efficacy and mechanism of probiotics in allergic diseases. Korean J. Pediatr. 2013, 56, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Schlundt, J. Report of a Joint FAO/WHO Expert Consultation on Evaluation of Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria; Food and Agriculture Organization of the United Nations: Córdoba, Argentina, 2001. [Google Scholar]
- Ta, V.; Laubach, S. Probiotic administration in early life, atopy, and asthma: A Meta-analysis of clinical trials. Pediatrics 2013, 132, e666–e676. [Google Scholar] [CrossRef] [PubMed]
- Stockert, K.; Schneider, B.; Porenta, G.; Rath, R.; Nissel, H.; Eichler, I. Laser acupuncture and probiotics in school age children with asthma: A randomized, placebo-controlled pilot study of therapy guided by principles of Traditional Chinese Medicine. Pedriatr. Allergy Immunol. 2007, 18, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Yang, Y.H.; Chuang, S.Y.; Huang, S.Y.; Pan, W.H. Reduced medication use and improved pulmonary function with supplements containing vegetable and fruit concentrate, fish oil and probiotics in asthmatic school children: A randomised controlled trial. Br. J. Nutr. 2013, 110, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Duotip-Test® II Package Insert. Available online: https://www.penallergytest.com/wp-content/uploads/Duo-Tip-2-Package-Insert.pdf (accessed on 16 September 2018).
- Shyur, S.-D.; Jan, R.-L.; Webster, J.R.; Chang, P.; Lu, Y.J.; Wang, J.Y. Determination of multiple allergen-specific IgE by microfluidic immunoassay cartridge in clinical settings. Pediatr. Allergy Immunol. 2010, 21, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.C.; Chiu, T.H.; Ho, C.Y.; Lin, P.P.; Wu, T.Y. Effects of anti-hypertension and intestinal micro-flora of spontaneously hypertensive rats fed gammaaminobutyric acid-enriched Chingshey purple sweet potato fermented milk by lactic acid bacteria. Afr. J. Microbiol. Res. 2013, 7, 932–940. [Google Scholar]
- Chen, Y.S.; Jan, R.L.; Lin, Y.L.; Chen, H.H.; Wang, J.Y. Randomized placebo-controlled trial of lactobacillus on asthmatic children with allergic rhinitis. Pediatr. Pulmonol. 2010, 45, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Miraglia Del Giudice, M.; Maiello, N.; Decimo, F.; Fusco, N.; D’Agostino, B.; Sullo, N.; Capasso, M.; Salpietro, V.; Gitto, E.; Ciprandi, G.; et al. Airways allergic inflammation and L. reuterii treatment in asthmatic children. J. Biol. Regul. Homeost. Agents 2012, 26, S35–S40. [Google Scholar] [PubMed]
- Giovannini, M.; Agostoni, C.; Riva, E.; Salvini, F.; Ruscitto, A.; Zuccotti, G.V.; Radaelli, G. A randomized prospective double blind controlled trial on effects of long-term consumption of fermented milk containing lactobacillus casei in pre-school children with allergic asthma and/or rhinitis. Pediatr. Res. 2007, 62, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Miraglia Del Giudice, M.; Indolfi, C.; Capasso, M.; Maiello, N.; Decimo, F.; Ciprandi, G. Bifidobacterium mixture (B longum BB536, B infantis M-63, B breve M-16V) treatment in children with seasonal allergic rhinitis and intermittent asthma. Ital. J. Pediatr. 2017, 43. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.; Black, P.N.; Stanley, T.V.; Mitchell, E.; Fitzharris, P.; Tannock, G.W.; Purdie, G.; Crane, J. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2008, 122, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, D.; Wakabayashi, H.; Watanabe, H. A double blind trial of Lactobacillus paracasei strain KW3110 administration for immunomodulation in patients with pollen allergy. Allergol. Int. 2005, 54, 143–149. [Google Scholar] [CrossRef]
- Wang, X.; Hui, Y.; Zhao, L.; Hao, Y.; Guo, H.; Ren, F. Oral administration of lactobacillus paracasei l9 attenuates PM2.5-induced enhancement of airway hyperresponsiveness and allergic airway response in murine model of asthma. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Dunstan, J.A.; Hale, J.; Breckler, L.; Lehmann, H.; Weston, S. Clinical effects of probiotics are associated with increased interferon-gamma responses in very young children with atopic dermatitis. Clin. Exp. Allergy 2005, 35, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- El-Ghaish, S.; Rabesona, H.; Choiset, Y.; Sitohy, M.; Haertle, T.; Chobert, J.M. Proteolysis by Lactobacillus fermentum IFO3956 isolated from Egyptian milk products decreases immuno-reactivity of αS1-casein. J. Dairy Res. 2011, 78, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Mikelsaar, M.; Zilmer, M. Lactobacillus fermentum ME-3 an antimicrobial and antioxidative probiotic. Microb. Ecol. Health Dis. 2009, 21, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.S.; Trivedi, M.K.; Jha, A.; Lin, Y.F.; Dimaano, L.; Garcia-Romero, M.T. Synbiotics for prevention and treatment of atopic dermatitis: a meta-analysis of randomized clinical trials. JAMA Pediatr. 2016, 170, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Szulińska, M.; Łoniewski, I.; van Hemert, S.; Sobieska, M.; Bogdański, P. Dose-dependent effects of multispecies probiotic supplementation on the lipopolysaccharide (LPS) level and cardiometabolic profile in obese postmenopausal women: A 12-week randomized clinical trial. Nutrients 2018, 10, 773. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Zhang, Y.; He, C.; Dai, J. Probiotics supplementation in children with asthma: A systematic review and meta-analysis. J. Paediatr. Child Health 2018, 54, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.O.; Ah, Y.M.; Yu, Y.M.; Choi, K.H.; Shin, W.G.; Lee, J.Y. Effects of probiotics for the treatment of atopic dermatitis: A meta-analysis of randomized controlled trials. Ann. Allergy Asthma Immunol. 2014, 113, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.J.; Wang, J.Y. Children with atopic dermatitis show clinical improvement after Lactobacillus exposure. Clin. Exp. Allergy 2015, 45, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Prakoeswa, C.R.; Herwanto, N.; Prameswari, R.; Astari, L.; Sawitri, S.; Hidayati, A.N.; Indramaya, D.M.; Kusumowidagdo, E.R.; Surono, I.S. Lactobacillus plantarum IS-10506 supplementation reduced SCORAD in children with atopic dermatitis. Benef. Microbes 2017, 8, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Oncham, S.; Udomsubpayakul, U.; Laisuan, W. Skin prick test reactivity to aeroallergens in adult allergy clinic in Thailand: A 12-year retrospective study. Asia Pac. Allergy 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Arshad, S.H.; Tariq, S.M.; Matthews, S.; Hakim, E. Sensitization to common allergens and its association with allergic disorders at age 4 years: A whole population birth cohort study. Pediatrics 2001, 108. [Google Scholar] [CrossRef]
- Vidal, C.; Lojo, S.; Juangorena, M.; Gonzalez-Quintela, A. Association between asthma and sensitization to allergens of Dermatophagoides pteronyssinus. J. Investig. Allergol. Clin. Immunol. 2016, 26, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Spacova, I.; Petrova, M.; Fremau, A.; Pollaris, L.; Vanoirbeek, J.; Ceuppens, J.L.; Seys, S.; Lebeer, S. Intranasal administration of probiotic Lactobacillus rhamnosus GG prevents birch pollen-induced allergic asthma in a murine model. Allergy 2018. [Google Scholar] [CrossRef] [PubMed]
- Spergel, J.M. From atopic dermatitis to asthma: The atopic march. Ann. Allergy Asthma Immunol. 2010, 105, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Novembre, E.; Cianferoni, A.; Lombardi, E.; Bernardini, R.; Pucci, N.; Vierucci, A. Natural history of “intrinsic” atopic dermatitis. Allergy 2001, 56, 452–453. [Google Scholar] [CrossRef] [PubMed]
- Stiemsma, L.T.; Arrieta, M.C.; Dimitriu, P.A.; Cheng, J.; Thorson, L.; Lefebvre, D.L.; Azad, M.B.; Subbarao, P.; Mandhane, P.; Becker, A.; et al. Shifts in Lachnospira and Clostridium sp. in the 3-month stool microbiome are associated with preschool age asthma. Clin. Sci. 2016, 130, 2199–2207. [Google Scholar] [CrossRef] [PubMed]
- Hevia, A.; Milani, C.; López, P.; Donado, C.D.; Cuervo, A.; González, S.; Suarez, A.; Turroni, F.; Gueimonde, M.; Ventura, M.; et al. Allergic patients with long-term asthma display low levels of Bifidobacterium adolescentis. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Durack, J.; Kimes, N.E.; Lin, D.L.; Rauch, M.; McKean, M.; McCauley, K.; Panzer, A.R.; Mar, J.S.; Cabana, M.D.; Lynch, S.V. Delayed gut microbiota development in high-risk for asthma infants is temporarily modifiable by Lactobacillus supplementation. Nat. Commun. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F.; Bjorksten, B.; Engstrand, L.; Jenmalm, M.C. Low gut microbiota diversity in early infancy precedes asthma at school age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | LP (n = 38) | LF (n = 38) | LP + LF (n = 36) | Placebo Group (n = 35) |
|---|---|---|---|---|
| Male, N (%) | 22 (57.9) | 24 (63.2) | 19 (52.8) | 18 (51.4) |
| Age (years), Mean (SD) | 7.68 (2.21) | 7.37 (2.34) | 7.00 (1.79) | 7.86 (2.50) |
| Height (cm), Mean (SD) | 121.24 (18.49) | 117.81 (17.21) | 117.51 (15.89) | 122.23 (18.94) |
| Weight (Kg), Mean (SD) | 26.45 (10.08) | 25.14 (10.16) | 24.75 (10.29) | 26.30 (11.76) |
| IgE (kU/I), Mean (SD) | 611.26 (511.83) | 600.23 (739.18) | 748.22 (896.40) | 493.06 (773.52) |
| Combine with allergic rhinitis (AR), N (%) | 31 (81.6) | 31 (81.6) | 32 (88.9) | 28 (80.0) |
| Combine with atopic dermatitis (AD), N (%) | 15 (39.5) | 10 (26.3) | 11 (30.6) | 9 (25.7) |
| Allergic sensitization, N (%) | ||||
| Mite | 33 (86.8) | 32 (84.2) | 30 (83.3) | 29 (82.9) |
| Cockroach | 3 (7.9) | 2 (5.3) | 1 (2.8) | 0 (0) |
| Animal dander | 2 (5.3) | 2 (5.3) | 1 (2.8) | 1 (2.9) |
| Milk | 2 (5.3) | 3 (7.9) | 1 (2.8) | 0 (0) |
| Egg | 2 (5.3) | 2 (5.3) | 1 (2.8) | 1 (2.9) |
| Crab | 2 (5.3) | 3 (7.9) | 1 (2.8) | 0 (0) |
| Maternal history of atopic disease, N (%) | 21 (55.3) | 22 (57.9) | 12 (33.3) | 15 (42.9) |
| Paternal history of atopic disease, N (%) | 21 (55.3) | 21 (55.3) | 20 (55.6) | 17 (48.6) |
| Subscale | LP (n = 38) Mean (SD) | LF (n = 38) Mean (SD) | LP + LF (n = 36) Mean (SD) | Placebo (n = 35) Mean (SD) | p-Value 4 Groups |
|---|---|---|---|---|---|
| Severity | 2.16 (0.64) | 2.13 (0.62) | 2.28 (0.62) | 2.20 (0.58) | 0.757 |
| C-ACT | 19.89 (4.28) | 17.87 (5.54) | 19.81 (4.72) | 20.77 (4.75) | 0.074 |
| PAQLQ | 5.44 (1.17) | 5.40 (1.41) | 5.90 (0.85) | 5.58 (1.16) | 0.268 |
| PASS | 16.84 (5.27) | 16.29 (5.79) | 15.71 (4.85) | 15.60 (5.16) | 0.738 |
| IFN-γ (ng/uL) | 170.73 (188.44) | 150.75 (158.12) | 156.97 (167.18) | 145.28 (162.26) | 0.954 |
| IL-4 (ng/uL) | 36.05 (29.63) | 48.48 (85.06) | 61.10 (117.67) | 55.38 (86.94) | 0.773 |
| TNF-α (ng/uL) | 292.95 (425.14) | 324.71 (512.82) | 231.88 (187.97) | 207.51 (340.37) | 0.690 |
| IgE (kU/I) | 611.26 (511.83) | 600.23 (739.18) | 748.22 (896.40) | 493.06 (773.52) | 0.547 |
| Fecal cell count Log10 (CFU/g) | |||||
| Lactobacillus | 8.07 (0.87) | 7.90 (0.95) | 7.49 (1.15) | 7.71 (0.92) | 0.101 |
| Bifidobacterium | 8.81 (0.91) | 8.74 (0.85) | 8.75 (1.12) | 8.90 (0.72) | 0.872 |
| Clostridium | 7.19 (0.78) | 6.63 (1.09) | 6.84 (1.18) | 6.79 (1.11) | 0.133 |
| Measure | LP Group (n = 38) | LF Group (n = 38) | LP + LF Group (n = 36) | |||
|---|---|---|---|---|---|---|
| β (95% CI) | P Value | β (95% CI) | P Value | β (95% CI) | P Value | |
| Severity | −0.34 (−0.63, −0.04) | 0.024 * | −0.30 (−-0.59, −0.02) | 0.038 * | −0.43 (−0.74, −0.12) | 0.007 * |
| C-ACT | 3.13 (−0.95, 5.31) | 0.005 * | 4.54 (2.44, 6.65) | < 0.001 * | 3.83 (1.78, 5.89) | < 0.001 * |
| PAQLQ | −0.32 (−0.86, 0.23) | 0.256 | −0.30 (−0.89, 0.28) | 0.310 | −0.43 (−0.96, 0.09) | 0.104 |
| PASS | −1.39 (−4.09, 1.30) | 0.311 | −1.14 (−3.79, 1.51) | 0.400 | −0.48 (−3.17, 2.20) | 0.725 |
| PEFR | 8.77 (−11.74, 29.27) | 0.402 | 28.83 (−3.55, 61.21) | 0.081 | 33.81 (8.62, 59.00) | 0.009 * |
| Subscale | Examination | LP (n = 38) Mean (SD) | LF (n = 38) Mean (SD) | LP + LF (n = 36) Mean (SD) | Placebo Group(n = 35) Mean (SD) | p-Value 4 Groups |
|---|---|---|---|---|---|---|
| IgE | Baseline | 611.26 (511.83) | 600.23 (739.18) | 748.22 (896.40) | 493.06 (773.52) | 0.547 |
| (kU/I) | month 3 | 482.42 (371.68) | 496.40 (622.51) | 377.29 (268.51) * | 577.81 (705.94) | 0.448 |
| IFN-γ | Baseline | 170.73 (188.44) | 150.75 (158.12) | 156.97 (167.18) | 145.28 (162.26) | 0.954 |
| (ng/uL) | month 3 | 158.01 (164.61) | 182.75 (373.50) | 221.41 (426.21) | 166.21 (197.61) | 0.886 |
| IL-4 | Baseline | 36.05 (29.63) | 48.4 (85.06) | 61.10 (117.67) | 55.38 (86.94) | 0.773 |
| (ng/uL) | month 3 | 51.16 (85.33) | 49.58 (67.82) | 55.09 (109.40) | 104.13 (215.39) | 0.366 |
| TNF-α | Baseline | 292.95 (425.14) | 324.71 (512.82) | 231.88 (187.97) | 207.51 (340.37) | 0.690 |
| (ng/uL) | month 3 | 315.23 (625.85) | 777.92 (1731.71) | 584.30 (959.98) | 550.48 (1059.83) | 0.514 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-F.; Chie, W.-C.; Wang, I.-J. Efficacy of Lactobacillus Administration in School-Age Children with Asthma: A Randomized, Placebo-Controlled Trial. Nutrients 2018, 10, 1678. https://doi.org/10.3390/nu10111678
Huang C-F, Chie W-C, Wang I-J. Efficacy of Lactobacillus Administration in School-Age Children with Asthma: A Randomized, Placebo-Controlled Trial. Nutrients. 2018; 10(11):1678. https://doi.org/10.3390/nu10111678
Chicago/Turabian StyleHuang, Chian-Feng, Wei-Chu Chie, and I-Jen Wang. 2018. "Efficacy of Lactobacillus Administration in School-Age Children with Asthma: A Randomized, Placebo-Controlled Trial" Nutrients 10, no. 11: 1678. https://doi.org/10.3390/nu10111678
APA StyleHuang, C.-F., Chie, W.-C., & Wang, I.-J. (2018). Efficacy of Lactobacillus Administration in School-Age Children with Asthma: A Randomized, Placebo-Controlled Trial. Nutrients, 10(11), 1678. https://doi.org/10.3390/nu10111678