
Roles of Economic Development Level and Other Human System Factors in COVID-19 Spread in the Early Stage of the Pandemic




Abstract
:1. Introduction
2. Data and Methods
2.1. COVID-19 Data and Processing
2.2. Cluster Analysis on COVID-19 Prevalence Trajectories
2.3. Logistic Model (3PL) for Trajectory Forecasting
2.4. Key Human System Factors for COVID-19 Infections
3. Results
3.1. Clustered Countries by COVID-19 Infections
3.2. The Near Future of Prevalence Rate
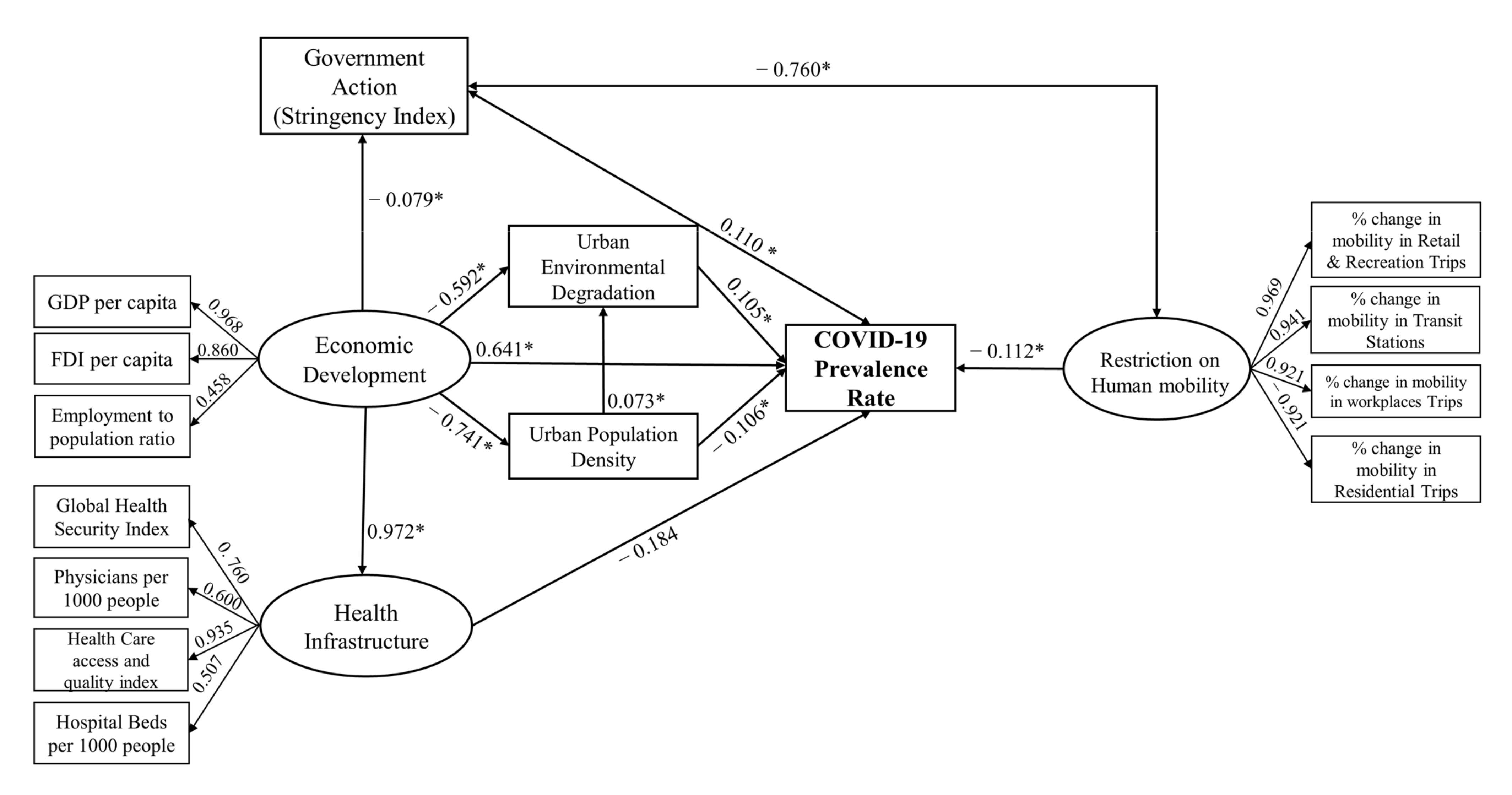
3.3. Human System Influences in the Spread of COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Code Availability
Guideline Statement
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Data | Unit | Availability | Data Source |
|---|---|---|---|
| COVID-19 Prevalence rate | per 105 | Weekly cases (1 February 2020–29 May 2021) | Dong et al. [52]; JHU CSSE [6] |
| Change in mobility in retail and recreation trips | % | Weekly data compared to baseline | Google [35] |
| Change in mobility in transit stations | % | Weekly data compared to baseline | Google [35] |
| Change in mobility in workplaces trips | % | Weekly data compared to baseline | Google [35] |
| Change in mobility in residential trips | % | Weekly data compared to baseline | Google [35] |
| Government response stringency index | NA | Weekly data of stringency index | OxCGRT [34] |
| GDP per capita | USD | Most recent year of each country | WB [27] |
| Foreign direct investment, net inflows | USD | Most recent year of each country | WB [27] |
| Total population | # | Most recent year of each country | WB [27] |
| Employment-to-population ratio | % | Most recent year of each country | WB [27] |
| Global Health Security Index | NA | Global Health Security Index (2019) | JHU CHS [53] |
| Physicians per 1000 people | # | Most recent year of each country | WB [27] |
| Hospital beds per 1000 people | # | Most recent year of each country | WB [27] |
| Healthcare Access and Quality Index | NA | Healthcare Access and Quality Index (2015) | Barber et al. [54] |
| Urban population density (per km2) | # | Population distribution layer (2015) | CIESIN [55] |
| Urban centers | km2 | Global human settlement layer (2015) | EC [56] |
| Urban air pollution | µgm−3 | annual average, weighted PM2.5 (2015) | Shaddick et al. [43] |
References
- Varkey, R.S.; Joy, J.; Sarmah, G.; Panda, P.K. Socioeconomic determinants of COVID-19 in Asian countries: An empirical analysis. J. Public Aff. 2020, 21, e2532. [Google Scholar] [CrossRef] [PubMed]
- Sá, F. Socioeconomic Determinants of Covid-19 Infections and Mortality: Evidence from England and Wales; SSRN: Rochester, NY, USA, 2020; Available online: https://ssrn.com/abstract=3612850 (accessed on 1 June 2021).
- Ehlert, A. The socio-economic determinants of COVID-19: A spatial analysis of German county level data. Soc. Econ. Plan. Sci. 2021, 78, 101083. [Google Scholar] [CrossRef] [PubMed]
- Stojkoski, V.; Utkovski, Z.; Jolakoski, P.; Tevdovski, D.; Kocarev, L. The Socio-Economic Determinants of the Coronavirus Disease (COVID-19) Pandemic; SSRN: Rochester, NY, USA, 2020; Available online: https://ssrn.com/abstract=3576037 (accessed on 1 June 2021).
- Hassan, M.M.; Kalam, M.; Shano, S.; Nayem, M.; Khan, R.; Rahman, M.; Islam, A. Assessment of epidemiological determinants of COVID-19 pandemic related to social and economic factors globally. J. Risk Financ. Manag. 2020, 13, 194. [Google Scholar] [CrossRef]
- Johns Hopkins University Center for Systems Science and Engineering (JHU CSSE). COVID-19 Data Repository by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. 2021. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 7 June 2021).
- Hunter, P.R.; Resebro, H.; Cameron, J.; Hunter, P.; Jagals, P.; Pond, K. Defining the Current Situation-Epidemiology. In Valuing Water, Valuing Livelihoods: Guidance on Social Cost-Benefit Analysis of Drinking-Water Interventions, with Special Reference to Small Water Supplies; World Health Organization/IWA Publishing: London, UK, 2011; pp. 75–100. [Google Scholar]
- Jain, A.K.; Dubes, R.C. Algorithms for Clustering Data; Prentice-Hall, Inc.: Hoboken, NJ, USA, 1988. [Google Scholar]
- Genolini, C.; Alacoque, X.; Sentenac, M.; Arnaud, C. Kml and kml3d: R packages to cluster longitudinal data. J. Stat. Softw. 2015, 65, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Genolini, C.; Falissard, B. KmL: A package to cluster longitudinal data. Comput. Methods Programs Biomed. 2011, 104, e112–e121. [Google Scholar] [CrossRef] [PubMed]
- Shim, Y.; Chung, J.; Choi, I.C. A comparison study of cluster validity indices using a nonhierarchical clustering algorithm. In Proceedings of the International Conference on Computational Intelligence for Modelling, Control and Automation and International Conference on Intelligent Agents, Web Technologies and Internet Commerce (CIMCA-IAWTIC’06), Vienna, Austria, 28–30 November 2005; pp. 199–204. [Google Scholar]
- Cramer, J.S. The early origins of the logit model. Stud. Hist. Philos. Biol. Biomed. Sci. 2004, 35, 613–626. [Google Scholar] [CrossRef]
- Ausloos, M. The Logistic Map and the Route to Chaos: From the Beginnings to Modern Applications; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Fan, Y.; Chen, J.; Shirkey, G.; John, R.; Wu, S.R.; Park, H.; Shao, C. Applications of structural equation modeling (SEM) in ecological studies: An updated review. Ecol. Process. 2016, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fan, P.; Ouyang, Z.; Nguyen, D.D.; Nguyen, T.T.H.; Park, H.; Chen, J. Urbanization, economic development, environmental and social changes in transitional economies: Vietnam after Doimoi. Landsc. Urban Plan. 2019, 187, 145–155. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Matthews, L.M.; Matthews, R.L.; Sarstedt, M. PLS-SEM or CB-SEM: Updated guidelines on which method to use. J. Multivar. Anal. 2017, 1, 107–123. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: New York, NY, USA, 2021. [Google Scholar]
- Mikhael, E.M.; Al-Jumaili, A.A. Can developing countries face novel coronavirus outbreak alone? The Iraqi situation. Public Health Pract. 2020, 1, 100004. [Google Scholar] [CrossRef]
- Szulczuk, K.; Cheema, M.A. COVID-19: The Impact of Socio-Economic Characteristics on the Fatality Rate; SSRN: Rochester, NY, USA, 2020; Available online: https://ssrn.com/abstract=3591551 (accessed on 1 June 2021).
- Caan, W. The spirit level. Why equality is better for everyone? J. Public Ment. Health 2011, 10, 250. [Google Scholar] [CrossRef]
- Adda, J. Economic activity and the spread of viral diseases: Evidence from high frequency data. Q. J. Econ. 2016, 131, 891–941. [Google Scholar] [CrossRef] [Green Version]
- Klepac, P.; Kucharski, A.J.; Conlan, A.J.; Kissler, S.; Tang, M.L.; Fry, H.; Gog, J.R. Contacts in context: Large-scale setting specific social mixing matrices from the BBC Pandemic project. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, S.; Nesson, E.; Robinson, J.J. The effects of employment on influenza rates. Econ. Hum. Biol. 2019, 34, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef]
- Zanakis, S.H.; Alvarez, C.; Li, V. Socio-economic determinants of HIV/AIDS pandemic and nations efficiencies. Eur. J. Oper. Res. 2007, 176, 1811–1838. [Google Scholar] [CrossRef]
- Patel, J.A.; Nielsen, F.B.H.; Badiani, A.A.; Assi, S.; Unadkat, V.A.; Patel, B.; Wardle, H. Poverty, inequality and COVID-19: The forgotten vulnerable. Public Health 2020, 183, 110–111. [Google Scholar] [CrossRef]
- World Bank (WB). World Development Indicator. 2021. Available online: https://databank.worldbank.org/home (accessed on 15 June 2021).
- Zhang, Y.; Zhang, A.; Wang, J. Exploring the roles of high-speed train, air and coach services in the spread of COVID-19 in China. Transp. Policy 2020, 94, 34–42. [Google Scholar] [CrossRef]
- Atalan, A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Ann. Med. Surg. 2020, 56, 38–42. [Google Scholar] [CrossRef]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, 037. [Google Scholar] [CrossRef] [Green Version]
- Bahinipati, C.S.; Sirohi, R.A.; Biswal, D.; Singh, M. COVID-19: Policy Interventions and Socio-Economic Impact in Andhra Pradesh; MPRA Paper No. 10050; Indian Institute of Technology Tirupati: Tirupati, India, 2020. [Google Scholar]
- Ray, D.; Subramanian, S. India’s lockdown: An interim report. Indian Econ. Rev. 2020, 55, 31–79. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Chen, X.; Shi, W. Impacts of social and economic factors on the transmission of coronavirus disease 2019 (COVID-19) in China. J. Popul. Econ. 2020, 33, 1127–1172. [Google Scholar] [CrossRef] [PubMed]
- University of Oxford, Covid-19 Government Response Tracker (OXCGRT). Covid-19 Government Response Tracker 2021. Available online: https://www.bsg.ox.ac.uk/research/research-projects/covid-19-government-response-tracker (accessed on 7 June 2021).
- Google. COVID-19 Community Mobility Reports 2020. Available online: https://www.google.com/covid19/mobility/ (accessed on 7 June 2021).
- Wong, D.W.; Li, Y. Spreading of COVID-19: Density matters. PLoS ONE 2020, 15, e0242398. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, S.; Sabouri, S.; Ewing, R. Does density aggravate the COVID-19 pandemic? Early findings and lessons for planners. J. Am. Plann. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Bhadra, A.; Mukherjee, A.; Sarkar, K. Impact of population density on Covid-19 infected and mortality rate in India. Model. Earth Syst. Environ. 2021, 7, 623–629. [Google Scholar] [CrossRef]
- Krefis, A.C.; Augustin, M.; Schlünzen, K.H.; Oßenbrügge, J.; Augustin, J. How does the urban environment affect health and well-being? A systematic review. Urban Sci. 2018, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Spencer, J.H.; Finucane, M.L.; Fox, J.M.; Saksena, S.; Sultana, N. Emerging infectious disease, the household built environment characteristics, and urban planning: Evidence on avian influenza in Vietnam. Landsc. Urban Plan. 2020, 193, 103681. [Google Scholar] [CrossRef]
- Isphording, I.E.; Pestel, N. Pandemic meets pollution: Poor air quality increases deaths by COVID-19. J. Environ. Econ. Manag. 2021, 108, 102448. [Google Scholar] [CrossRef]
- Dijkstra, L.; Florczyk, A.J.; Freire, S.; Kemper, T.; Melchiorri, M.; Pesaresi, M.; Schiavina, M. Applying the degree of urbanisation to the globe: A new harmonised definition reveals a different picture of global urbanisation. J. Urban Econ. 2021, 125, 103312. [Google Scholar] [CrossRef]
- Shaddick, G.; Thomas, M.L.; Mudu, P.; Ruggeri, G.; Gumy, S. Half the world’s population are exposed to increasing air pollution. NPJ Clim. Atmos. Sci. 2020, 3, 1–5. [Google Scholar] [CrossRef]
- Hailu, G. Economic thoughts on COVID-19 for Canadian food processors. Can. J. Agric. Econ. Can. D'agroeconomie 2020, 68, 163–169. [Google Scholar] [CrossRef]
- Belitski, M.; Guenther, C.; Kritikos, A.S.; Thurik, R. Economic effects of the COVID-19 pandemic on entrepreneurship and small businesses. Small Bus. Econ. 2021, 58, 1–17. [Google Scholar]
- Caraka, R.E.; Kurniawan, R.; Nasution, B.I.; Jamilatuzzahro, J.; Gio, P.U.; Basyuni, M.; Pardamean, B. Micro, small, and medium enterprises’ business vulnerability cluster in Indonesia: An analysis using optimized fuzzy geodemographic clustering. Sustainability 2021, 13, 7807. [Google Scholar] [CrossRef]
- Bonacini, L.; Gallo, G.; Scicchitano, S. Working from home and income inequality: Risks of a ‘new normal’ with COVID-19. J. Popul. Econ. 2021, 34, 303–360. [Google Scholar] [CrossRef]
- Tomé, E.; Gromova, E. Development of emergent knowledge strategies and new dynamic capabilities for business education in a time of crisis. Sustainability 2021, 13, 4518. [Google Scholar] [CrossRef]
- Susanto, A.P.; Findyartini, A.; Taher, A.; Susilaradeya, D.P.; Ariawan, I.; Dartanto, T.; Wiweko, B. COVID-19 in Indonesia: Challenges and Multidisciplinary Perspectives for a Safe and Productive New Normal. Acta Med. Indones. 2020, 52, 423–430. [Google Scholar]
- Sparrow, R.; Dartanto, T.; Hartwig, R. Indonesia under the new normal: Challenges and the way ahead. Bull. Indones. Econ. Stud. 2020, 56, 269–299. [Google Scholar] [CrossRef]
- Djalante, R.; Nurhidayah, L.; Van Minh, H.; Phuong NT, N.; Mahendradhata, Y.; Trias, A.; Lassa, J.; Miller, M.A. COVID-19 and ASEAN responses: Comparative policy analysis. Prog. Disaster Sci. 2020, 8, 100129. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Inf. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Johns Hopkins University, Center for Health Security (JHU CHS). Global Health Security Index 2019. Available online: www.ghsindex.org (accessed on 7 June 2021).
- Barber, R.M.; Fullman, N.; Sorensen, R.J.; Bollyky, T.; McKee, M.; Nolte, E.; Davey, G. Healthcare access and quality index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the Global Burden of Disease Study 2015. Lancet 2017, 390, 231–266. [Google Scholar] [CrossRef] [Green Version]
- Center for International Earth Science Information Network (CIESIN). Center for International Earth Science Information Network 2021. Available online: http://www.ciesin.org/ (accessed on 15 June 2021).
- European Commission. Global Human Settlement Layer (GHSL) 2021. Available online: https://ghsl.jrc.ec.europa.eu/CFS.php (accessed on 15 June 2021).
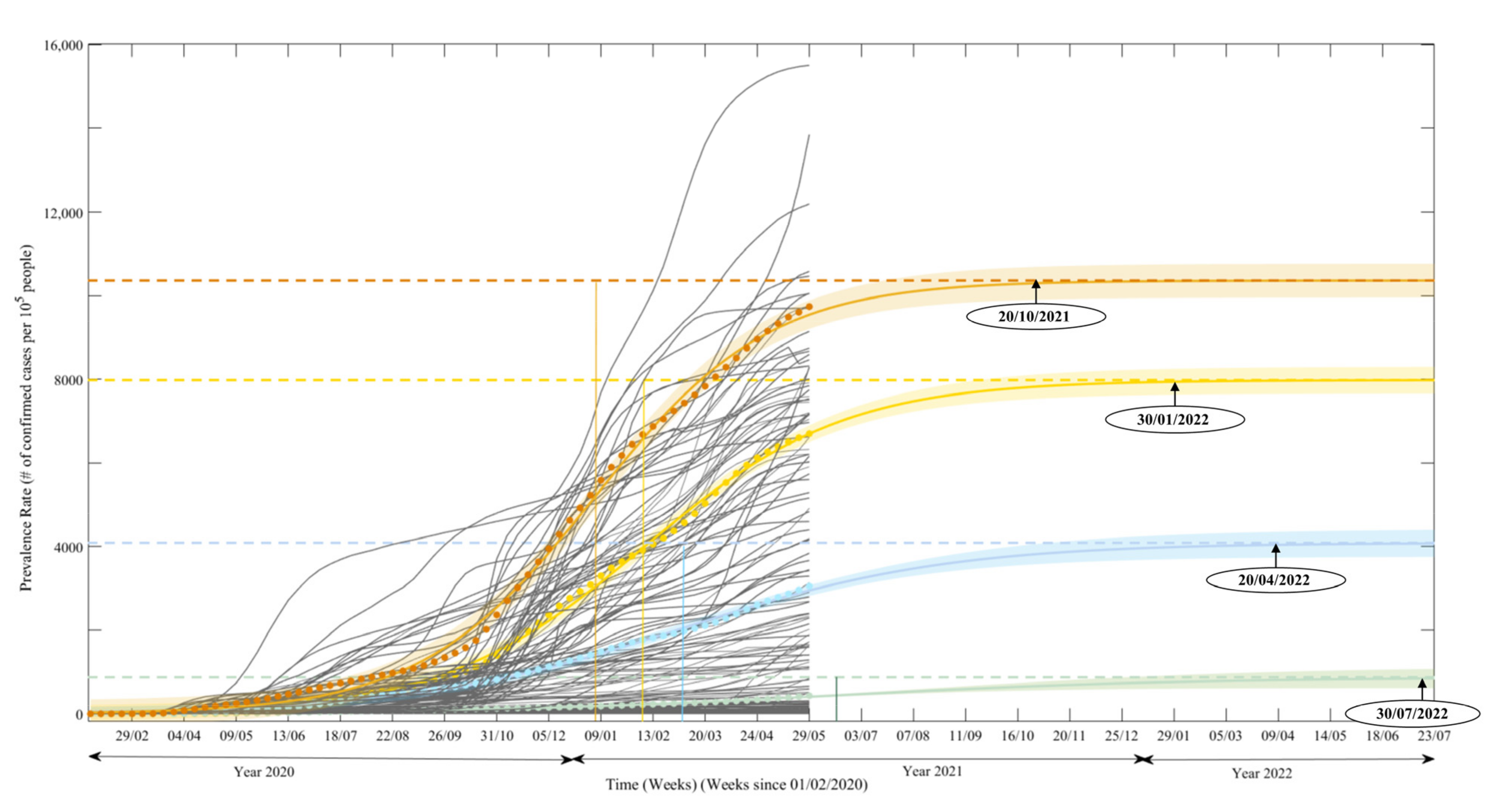

| Parameter | Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 |
|---|---|---|---|---|
| Growth rate | 0.058 (0.052, 0.064) | 0.077 (0.073,0.082) | 0.104 (0.1,0.108) | 0.119 (0.114, 0.124) |
| Inflection point | 72.15 (63.12, 81.19) | 57.82 (55.67, 59.96) | 54.13 (53.34, 54.93) | 49.4 (48.81, 49.99) |
| Asymptote | 872 (612.1, 1132) | 4090 (3782, 4398) | 7980 (7716, 8243) | 10,360.284 (10,110.73, 10,609.77) |
| Normalized RMSE | 0.029 | 0.013 | 0.019 | 0.016 |
| Country Names | |
|---|---|
| Cluster I (76) | |
| Africa (39) | Algeria, Angola, Benin, Burkina Faso, Burundi, Cameroon, Chad, Congo, Cote d’Ivoire, Democratic Rep. of Congo, Egypt, Equatorial Guinea, Eritrea, Ethiopia, Gabon, Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, Liberia, Madagascar, Malawi, Mali, Mauritania, Mauritius, Mozambique, Niger, Nigeria, Rwanda, Senegal, Sierra Leone, South Sudan, Sudan, Tanzania, Togo, Uganda, Zambia, Zimbabwe |
| Asia (25) | Afghanistan, Bangladesh, Cambodia, China, Hong Kong, India, Indonesia, Japan, Laos, Malaysia, Mongolia, Myanmar, Nepal, Pakistan, Philippines, Singapore, South Korea, Sri Lanka, Syria, Tajikistan, Thailand, Timor Este, Uzbekistan, Vietnam, Yemen |
| Central America (7) | Cuba, El Salvador, Guatemala, Haiti, Jamaica, Nicaragua, Trinidad and Tobago |
| Oceania (3) | Australia, New Zealand, Papua New Guinea |
| Europe (1) | Finland |
| South America (1) | Venezuela |
| Cluster II (27) | |
| Africa (7) | Tunisia, South Africa, Libya, Botswana, Namibia, Eswatini, Morocco |
| Asia (7) | Oman, Iran, Azerbaijan, Iraq, Kazakhstan, Kyrgyzstan, Saudi Arabia |
| Europe (5) | Germany, Belarus, Greece, Russia, Norway |
| South America (4) | Uruguay, Paraguay, Bolivia, Ecuador |
| Central America (3) | Dominican Republic, Honduras, Mexico |
| North America (1) | Canada |
| Cluster III (29) | |
| Europe (17) | Estonia, Hungary, Poland, North Macedonia, Austria, Slovakia, Latvia, Italy, United Kingdom, Moldova, Bosnia and Herzegovina, Bulgaria, Romania, Ireland, Ukraine, Denmark, Albania |
| Asia (6) | Lebanon, Jordan, Kuwait, Turkey, Palestine, United Arab Emirates |
| South America (5) | Argentina, Brazil, Chile, Colombia, Peru |
| Central America (1) | Costa Rica |
| Cluster IV (19) | |
| Europe (12) | Czechia, Slovenia, Sweden, Serbia, Lithuania, Netherlands, Belgium, Croatia, France, Portugal, Switzerland, Spain |
| Middle East Asia (5) | Bahrain, Israel, Georgia, Qatar, Armenia |
| North America (1) | United States |
| South America (1) | Panama |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, P.; Chen, J.; Sarker, T. Roles of Economic Development Level and Other Human System Factors in COVID-19 Spread in the Early Stage of the Pandemic. Sustainability 2022, 14, 2342. https://doi.org/10.3390/su14042342
Fan P, Chen J, Sarker T. Roles of Economic Development Level and Other Human System Factors in COVID-19 Spread in the Early Stage of the Pandemic. Sustainability. 2022; 14(4):2342. https://doi.org/10.3390/su14042342
Chicago/Turabian StyleFan, Peilei, Jiquan Chen, and Tanni Sarker. 2022. "Roles of Economic Development Level and Other Human System Factors in COVID-19 Spread in the Early Stage of the Pandemic" Sustainability 14, no. 4: 2342. https://doi.org/10.3390/su14042342
APA StyleFan, P., Chen, J., & Sarker, T. (2022). Roles of Economic Development Level and Other Human System Factors in COVID-19 Spread in the Early Stage of the Pandemic. Sustainability, 14(4), 2342. https://doi.org/10.3390/su14042342