1. Introduction
The continued increase in human lifespans is accelerating the aging of the population in most countries, and the number of people aged 65 and over worldwide is expected to double from 73 million in 2019 to 150 million by 2050 [
1].
In Korea, a society with a population aged 65 or older accounting for more than 14% of the total population, is called an aging society, and a society with more than 20% is called a super-aged society. As of 2020, 15.7% of the population is over the age of 65, meaning that the nation has become an aging society, and by 2025, the proportion of the elderly will exceed 20%, at which point it is expected to become a super-aged society [
2]. Therefore, continued increases in the proportion of the elderly population are leading to corresponding increases in the numbers of residential aged care facilities (RACF) and care hospitals. Elderly people living in these facilities generally have geriatric diseases as well as restricted mobility, and thus they cannot evacuate on their own in the event of a disaster such as a fire; this poses a serious safety risk.
In Korea, there were 27 casualties in the fire accident at the Indeok Nursing Home in Pohang in 2010 [
3], and the fire at the Jangseong Filial Love Sharing Nursing Hospital in 2014 caused 29 casualties [
4]. In 2018, there was a large fire disaster at Miryang Sejong Nursing Hospital that killed 39 people and injured 151 people [
5].
Table 1 presents fire accidents that have occurred in nursing facilities in different countries.
Residents of such facilities may suffer greater damage from fires than the general population due to geriatric diseases and limited mobility; it is therefore crucial that such facilities have efficient evacuation methods that are suitable for their residents, and it is also necessary to improve shelter equipment.
In a related study, Lee and Heo using fire and evacuation simulation to compare the required safety escape time (RSET) and the available safety escape time (ASET) in nursing hospitals to determine the safety of evacuation inducers in terms of legal standards [
16].
Kim et al. calculated the evacuation time by applying a fire simulation to elderly care hospitals, and they reported that the evacuation time could be reduced by establishing separate fire safety standards for day and night protection, which they determined using Simulex [
17].
Jeon et al. suggested a plan for reducing the evacuation time depending on the situation—such as whether the sprinkler or fire door is closed—using Pyrosim and Pathfinder for elderly medical welfare facilities [
18].
Rie et al. quantitatively compared ASET and RSET by providing an information transfer function between agents by using artistic simulation that enables bypass evacuation according to the risk and that also allows for the evacuation route and evacuation start time to be individually set for each evacuee [
19].
Mufeng Xiao et al. reported that the evacuation time could be reduced through evacuation guidance by applying the physical characteristics of library occupants as well as the movement speed that reflects these characteristics by using Pathfinder [
20].
Evacuation times in high-rise buildings were studied using Pathfinder by Boonngam and Patvichaichod. They reported that when the passenger elevator was used as a fire escape elevator, the efficiency of evacuation performance increased from 29.21% to 35.05% [
21].
In Hunt et al. an algorithm that considers both horizontal and vertical evacuation at the same time using Pathfinder and Exodus is presented [
22].
According to Anastasios et al., in the case of fire, the smoke reduces the maximum movement speed of the occupants and increases the minimum movement speed [
23].
Hospitals do not have common evacuation guidelines, even in various publications, reports, and conclusions, and lack adequate preparation. It has been suggested that nationality cooperation is necessary for the joint use of these evacuation plans and guidelines by trade unions and the international community [
24].
The optimum reduction in evacuation time to minimize damage to human life caused by fire is determined based on the characteristics of the residents and the evacuation routes. In Korea, the enforcement regulations of the Elderly Welfare Act stipulate that a ramp should be installed in all elderly care hospitals [
25]. However, the installation of such ramps is excluded from the mandatory requirements if the elevator installation conditions of the Domestic Elevator Facility Safety Management Act are satisfied.
Groups that are vulnerable during egress (e.g., residents of elderly nursing hospitals, nursing homes, etc.) need to be clearly presented with appropriate evacuation routes and methods to reduce evacuation time. In this study, through quantitative analysis of evacuation times by evacuation route (stair stairs, elevators, ramps, etc.), suitable evacuation routes are presented for facilities for vulnerable groups during egress. In addition, this analysis was performed using a coupling method using FDS and Pathfinder, which are simulations of fire and evacuation, to suggest ways to reduce evacuation time through the classification of patient groups.
2. Analysis of Predicting Fatality by Evacuation Method
The safety evaluation applied to this study reflected the reduction in evacuation time due to reduced visibility as well as increased temperature, CO, CO
2, and smoke caused by a fire in real-time evacuation sites.
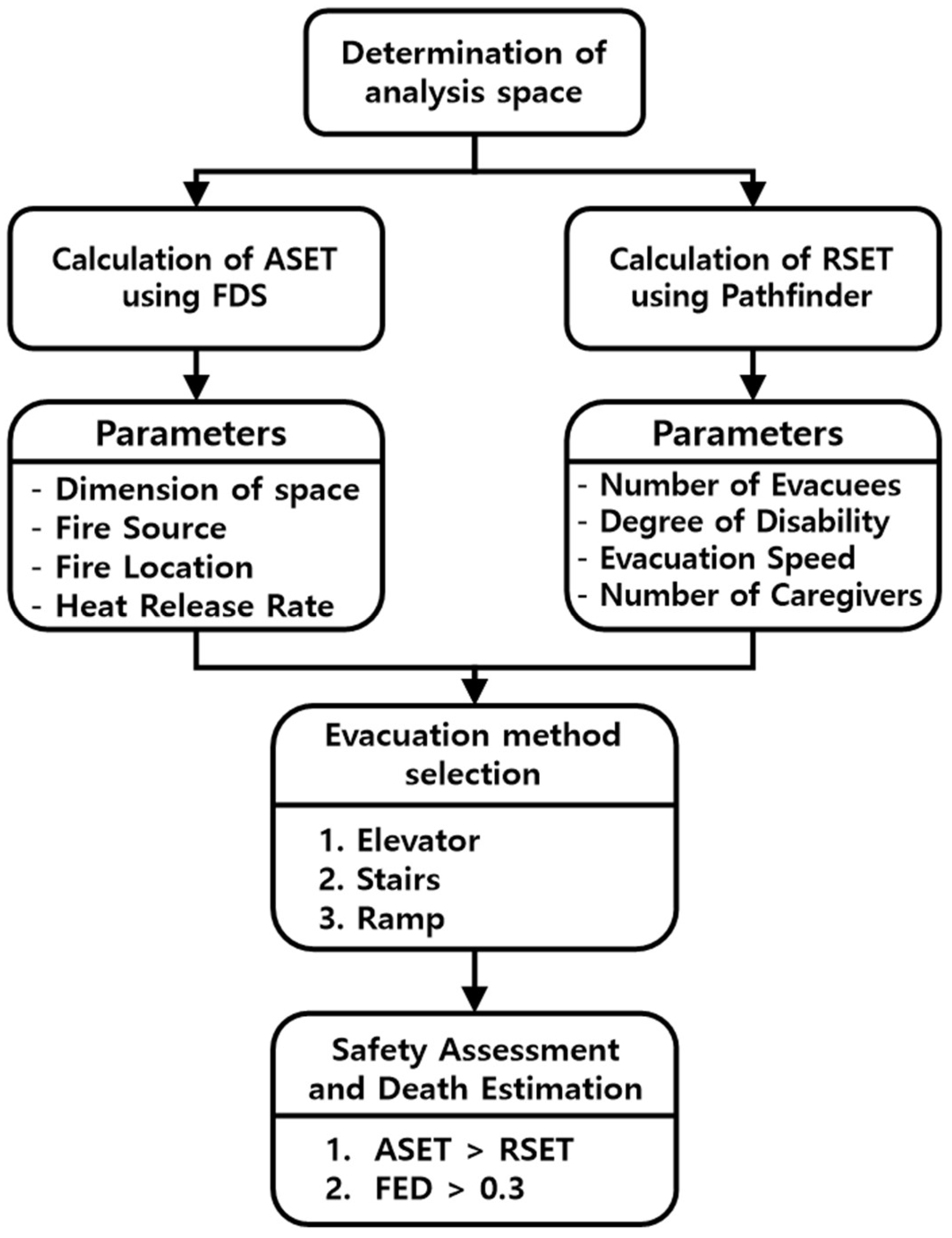
Figure 1 shows the flow chart of the study.
2.1. Evaluation of ASET and RSET
In this evaluation, the fire dynamics simulator (FDS) was used for ASET analysis, and the Pathfinder 2019 version [
26,
27] was used for RSET analysis. FDS is a computational fluid dynamics model of fire-driven fluid flow provided by the National Institute of Standards and Technology (NIST) of the US Department of Commerce and is a free open-source software. FDS is a computational fluid dynamics software for fire-driven fluid flows that numerically solves the form of Navier–Stokes equations suitable for low-velocity heat-driven flows and also solves smoke and heat transfer problems due to fire. Pathfinder is an agent-based software that uses 3D analysis to measure the route and time for a person in a room to evacuate to an exit. Therefore, this study used Pathfinder to perform an evacuation simulation, including congestion-based pedestrian movement characteristics.
Evacuation risk assessment was conducted by comparing the RSET time required to evacuate from a fire site with the ASET defined as the time it takes for fire effluents to reach the human body. Equation (1) shows the conditions for securing safety obtained by comparing ASET and RSET in this study.
Figure 2 shows the time conceptual diagram for ASET and RSET.
In this study, RSET means the amount of time that is required for occupants to evacuate a fire floor safely using (1) evacuation stairs, (2) elevators, and (3) ramps. Therefore, having a relatively lower RSET value means that the evacuation route is relatively less affected by fire effluents.
2.2. Evacuation Space Model
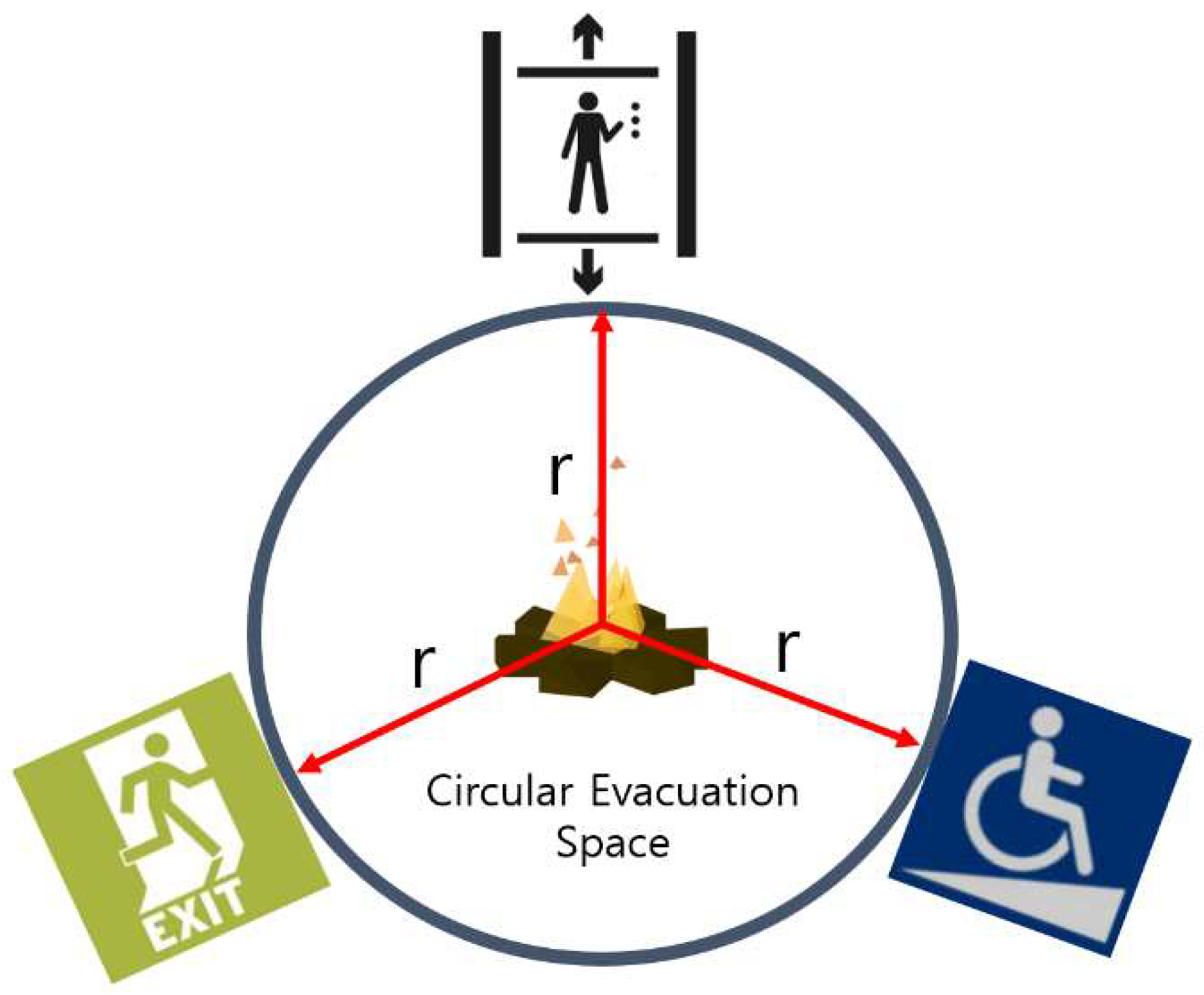
The target building for the fire hazard with evacuation analysis has different characteristics of usage, fire areas, evacuation methods, and locations of the evacuation route. In this study, circular space modeling was applied, as shown in
Figure 3, to simplify the problems of the various spaces and structures of these buildings.
The application of this simplified circular space model has the advantage of obtaining a uniform ASET value regardless of the arrangement of the evacuation route entrance located in the circular arc, as the evacuation route can be simplified regardless of the design structure.
Figure 4 shows the three-dimensional circular space modeling applied in this study [
28].
2.3. Evacuation Condition
2.3.1. Fire Floor and Evacuation Route
Table 2 shows the fire floor width and radius set upon the Pathfinder and conditions for each evacuation method.
2.3.2. Total Number of Occupants
The area of the modeling space was set to be the same as the 15 open areas of the five-person room in the nursing hospital. The number of occupants was set as 114 persons according to the enforcement regulations of South Korea’s Elderly Welfare Act [
25].
The patient groups applied for the analysis consisted of (1) non-disabled people, (2) disabled people using canes, (3) disabled people using wheelchairs divided between the patients who used them alone and those who needed a caregiver in the same proportion, and (4) patients with disabilities who are bedridden. The number of moving caregivers for patients with disabilities was set at one caregiver for each patient using a wheelchair and two caregivers for each patient who is bedridden.
Table 3 shows the number of people per group and the evacuation delay time.
2.3.3. Body Dimensions and Sizes of Mattresses and Wheelchairs
The ages were set as 40 to 49 years old for caregivers and non-disabled people, and more than 60 years old for patients. The body dimensions were established by considering the average shoulder width, height, and standard deviation values in anthropometric data from South Korea [
29]. The size of the wheelchair was set according to the national standard certification integrated information system (KS P 6113) [
30], and the size of the mattress was set according to the value from the Ministry of Food and Drug Safety (2017-16) [
31].
Table 4 and
Table 5 show the applied dimensions for the wheelchair, mattress, and human bodies.
2.3.4. Evacuation Condition
The evacuation moving speed of the space members is an essential factor in calculating RSET, which is the time required to evacuate from the fire floor to the ground floor.
Table 6 shows the moving speed for each patient classification [
32,
33]. The stair-descending speed was set to 0.5 times the corresponding moving speed on flat ground for each group of patients [
34].
Horizontal evacuation from the fire floor is performed by having assistants help move patients using wheelchairs and patients who are bedridden to the evacuation stairs or the entrance to the evacuation elevator. The movement of the patient on the evacuation stairs—which is a vertical evacuation—is performed by separating the patient from the wheelchair or mattress and then having the patient descend the stairs with the aid of a caregiver or two caregivers.
Table 7 shows the evacuation patterns of each group for each evacuation route in the simulation.
2.4. Results of RSET
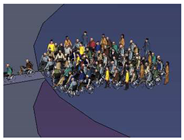
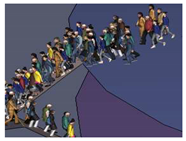
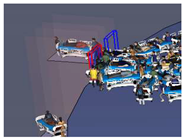
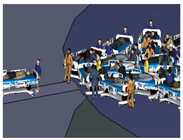
Table 8 shows the bottleneck according to the group evacuation route at the fire floor. The patient transfer of groups of patients using wheelchairs as well as patients who were bedridden under elevator and ramp conditions was identified as the cause of serious bottlenecks at the entrances of evacuation routes. From the 3D evacuation image, it can be seen that, for the stair evacuation of the group made up of patients using wheelchairs and patients who were bedridden, the bottleneck at the entrance of the evacuation route could be reduced by separating the patient from their means of transportation and having them continue on foot with the aid of a caregiver or two caregivers.
Figure 5 shows the number of evacuees on the fire floor according to each group’s evacuation route and evacuation time.
In the case of evacuation using stairs (
Figure 5a), the group of patients who were bedridden and the group of patients who used wheelchairs showed faster evacuation characteristics than the group of patients who used canes. This is the result of the fastest evacuation when the caregiver helped. Evacuation using the elevator condition (
Figure 5b) showed that the group of patients using canes showed faster evacuation characteristics than the group of patients who were bedridden and the group of patients using wheelchairs. This result shows that the number of elevator users increased because the means of mobility assistance (wheelchair, bed, etc.) were not included.
Figure 6 shows the RSET by following each evacuation group.
100% of patients without disabilities;
100% of patients with disabilities who used canes;
100% of patients with disabilities who used wheelchairs;
100% of patients with disabilities who were bedridden;
Equal proportions of all patients, i.e., 25% of each of (1) through (4).
The ramp evacuation method showed the shortest RSET—thus appearing as the shortest and most effective evacuation method—under all conditions except for the group of patients who were bedridden (3).
The group of patients with disabilities who used canes (2), moving by their own force, showed the maximum RSET value under the evacuation condition using stairs, and this was found to be the most inefficient evacuation method.
In the group of patients with disabilities who used wheelchairs (3), one caregiver was applied per patient; evacuation using stairs was thus found to be more efficient than that using the elevator.
In the case of the group of patients who were bedridden (4), the condition of stair evacuation was found to have the lowest RSET value with a relatively short evacuation route, as two moving caregivers were deployed per patient.
Under the condition of equal proportions of patients from each group (5), elevator evacuation was found to be the most inefficient method.
3. Risk Assessment
3.1. Fire Scenario
The spatial structure was applied to the ASET analysis in the same way as it was applied to the RSET analysis model.
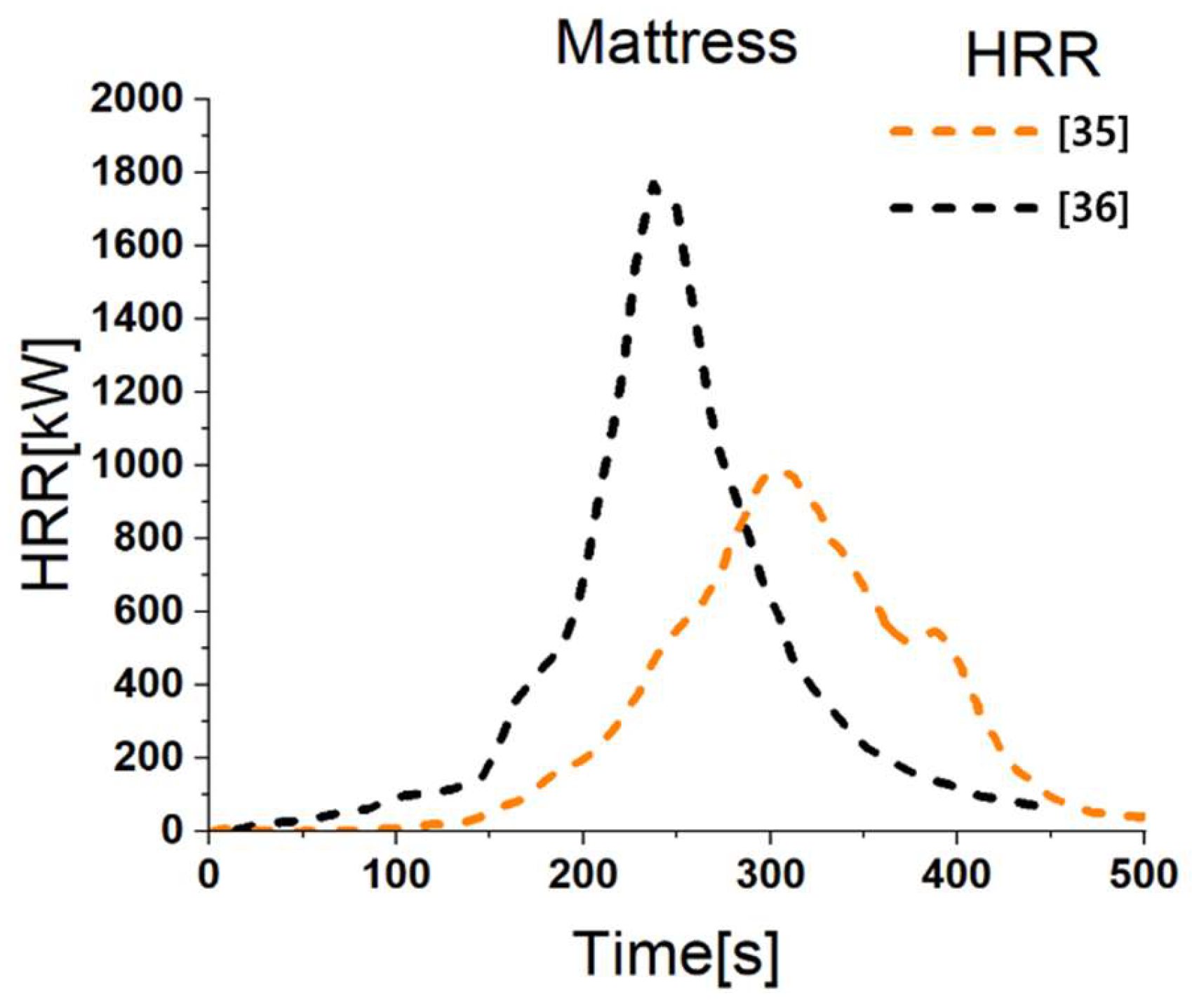
Table 9 presents the input variables applied to the FDS fire scenario to analyze the spatial distribution of fire effluents generated during a fire. A mattress was selected as the fire source, and the number of fire sources was sequentially extended from a minimum of one to a maximum of five.
Figure 7 shows the two types of heat release rate diagrams applied to the analysis [
34,
35].
3.2. Criteria for Fire Casualties
For the applied criteria for fire casualties, the fractional effective dose (FED) (ISO 2007) value, which is a probabilistic quantitative analysis method used to estimate the health effects of toxic gas on the evacuees, was used along with the domestic evacuation evaluation standard. FED is the time integral of the effects of excessive carbon monoxide and carbon dioxide inhalation, as well as oxygen depletion. The domestic standard is the individual item standard for the human limit concentration of fire effluent, and the detailed standard values are listed in
Table 10 [
37].
As the fatality condition applied in this analysis, the lowest threshold value of FED 0.3 was applied for the most sensitive population group, the elderly, young people, or those with compromised immune systems. The reason why FED was set to 0.3 is that it has been reported that evacuees are incapacitated from the FED value of 0.3 because of the decrease in oxygen due to the inhalation of carbon monoxide and carbon dioxide and insufficient oxygen caused by fire. Therefore, in this study, the point at which this value appeared was judged as the occurrence of casualties. By comparing ASET, which is the time affected by fire effluents in the evacuation route, and the RSET required to move to a safe place, it is possible to quantitatively evaluate the number of deaths among evacuees.
3.3. Spatial Distribution of FED, Visibility, and Temperature
Identifying the spatial distribution of risk assessment items for the entire space of evacuation layer is a very effective method for real-time risk assessment according to evacuee location.
Table 11 shows the FED distribution at 1.8 m above the floor according to the combustion of one to five mattresses up to 300 s at 100 s intervals for the two types of low and high heat release rates (hereafter HRR).
In the figure, the area marked in red indicates spatial regions that exceed the safety reference values.
Table 12 shows the visibility distribution at 1.8 m above the floor according to the one to five mattress fires at 100 s intervals for two types of low and high HRR.
Table 13 shows the temperature distribution at 1.8 m above the floor according to the one to five mattress fires up to 300 s at 100 s intervals for the two types of low and high HRR.
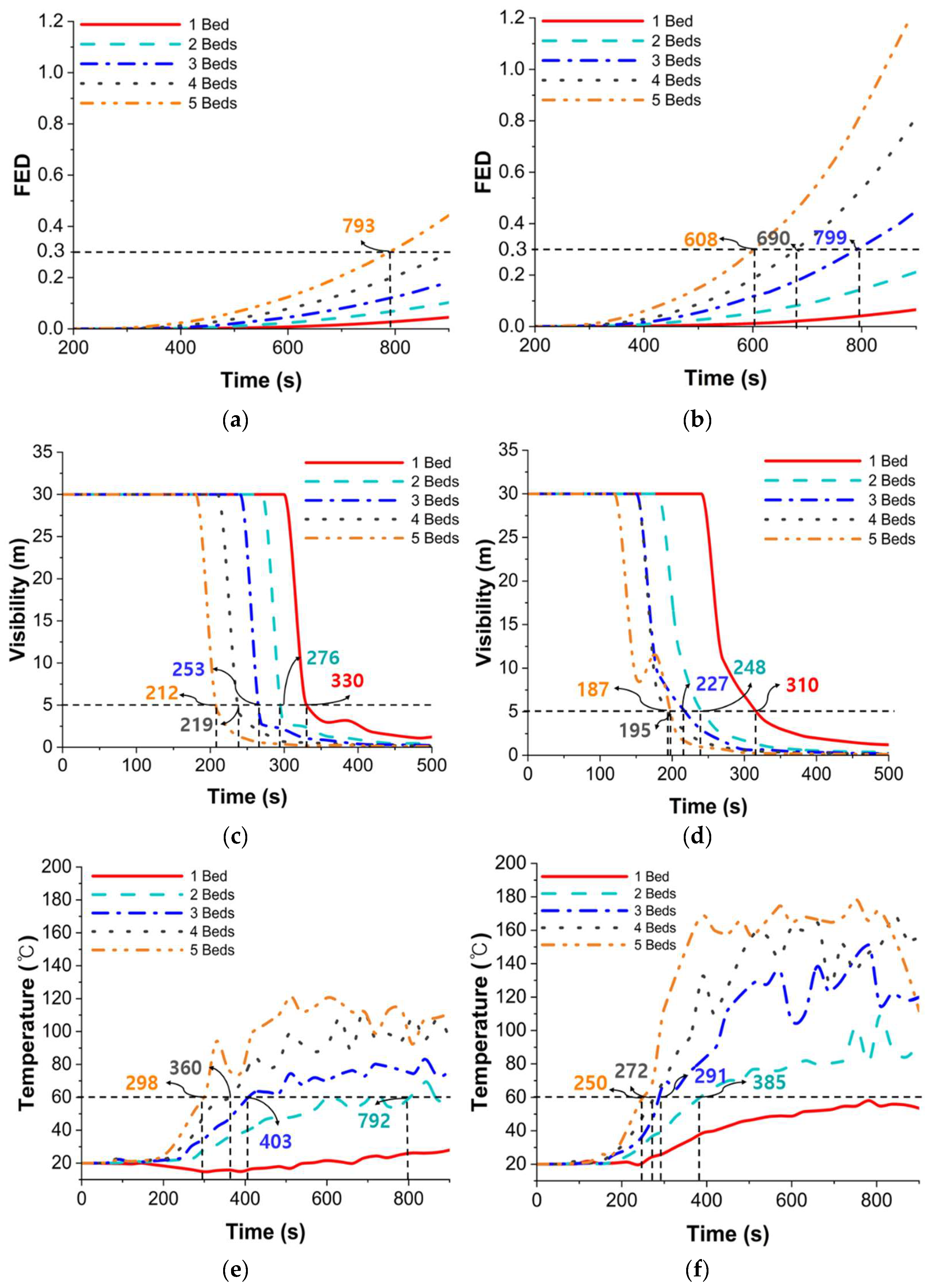
Figure 8 is a graph showing the real-time values according to the evacuation time based on the exit height of 1.8 m and in relation to the six evaluation items of the safety standards (FED, temperature, visibility, CO, O
2, and CO
2) for life shown in
Table 10.
Among the six evaluation items, visibility was found to be the fastest approaches to the criteria of life safety under both the low HRR and the high HRR conditions. This is followed by the effects that temperature and FED had on evacuees. It was also confirmed that the ASET value decreased with an increasing number of fire sources (mattresses).
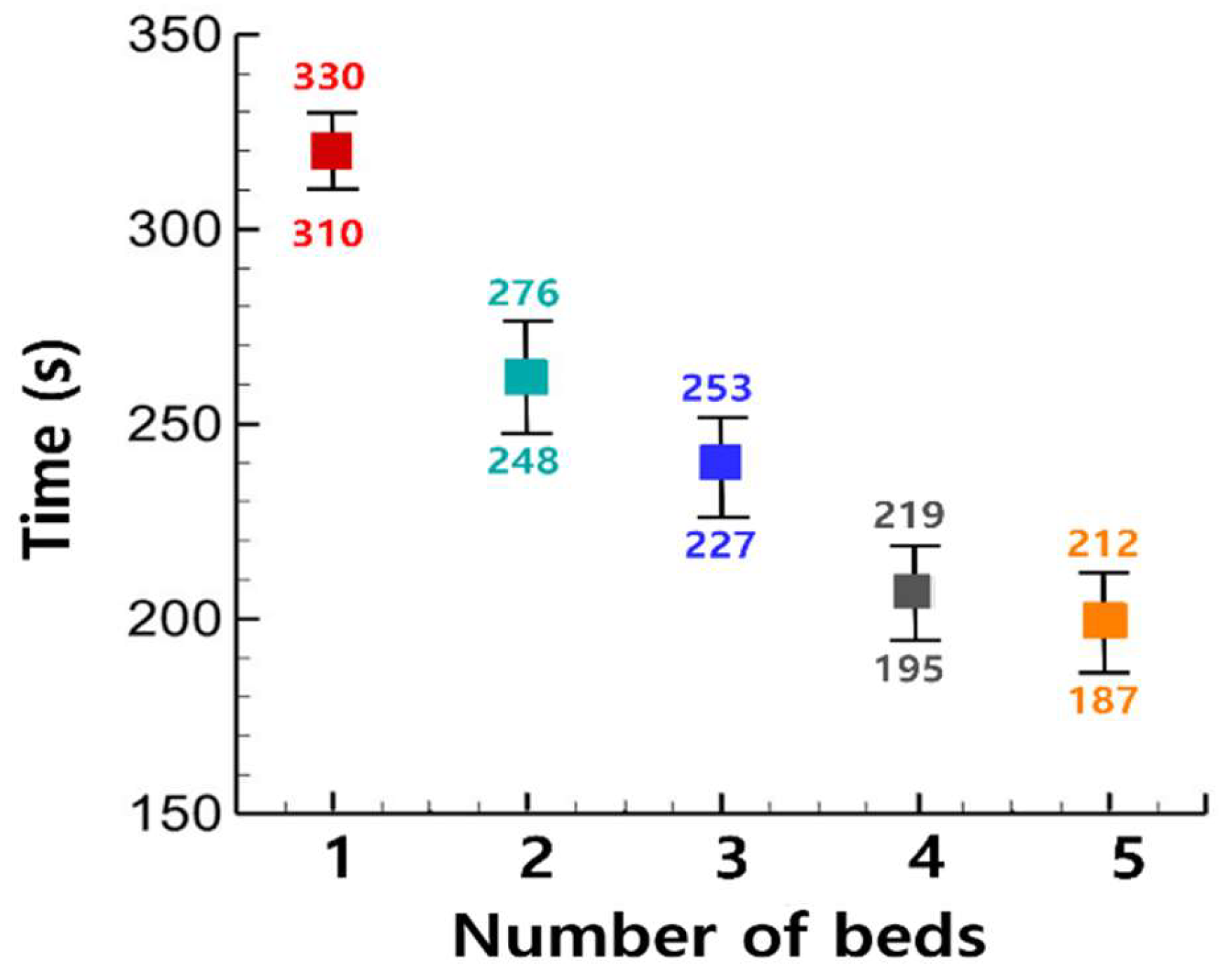
Figure 9 shows the ASET in combustion conditions from one mattress to a maximum of five mattresses based on visibility as a determinant of life safety criteria. This is because, among the six items in
Table 10, the decrease in visibility due to smoke affects evacuation first. ASET decreased about 17% when increasing from one to two mattress fires under low HRR conditions, and it decreased by 4% when increasing from four to five mattress fires.
Under the high HRR condition, ASET showed a decrease of about 20% when increasing from one to two mattress fires and a reduction of about 5% when increasing from four to five mattress fires.
In both low and High HRR, the most significant decrease in ASET was observed when increasing from one to two mattress fires, and a minor decrease was observed when increasing from four to five mattress fires. It was also found that the higher the HRR that could be obtained, the smaller the decrease in ASET.
5. Discussion
The results showed that the ramp escape route was the fastest evacuation route for all groups except for the group of patients who were bedridden. However, for the group of patients using wheelchairs, it was unsafe to have more than three mattress fires, while it was unsafe for the group of patients who were bedridden to have more than one mattress fire.
According to
Table 14,
Table 15 and
Table 16, there was a difference in the number of fatalities according to the selection of an escape route and a moving pattern for each group of patients with disabilities. Particularly in the case of the elevator-only evacuation route, the group of patients who were bedridden was found to have the highest number of fatalities due to the occurrence of a bottleneck caused by moving with a mattress.
In the case of the stair evacuation route, it was found that the number of fatalities could be reduced by moving the patients who were bedridden on foot with the aid of two assistants while leaving the mattress behind.
For the group of patients who used canes, compared to evacuation using the stairs alone, the conversion to the ramp-only evacuation route led to a reduction in fatalities in the range from a minimum of 86.3% to a maximum of 100%.
For the group of patients who were bedridden, compared to evacuation using the elevator alone, the conversion to the ramp-only evacuation route led to a reduction in fatalities in the range from a minimum of 78.8% to a maximum of 85.2%.
6. Conclusions
In this study, a simulation-based risk analysis was performed in order to conduct ASET and RSET assessments for nursing hospital patients on a circular building floor space used to equalize the distance to the entrance of each escape route. The following conclusions may be drawn from the results of the simulation regarding the safety of evacuation-vulnerable populations:
- (1)
In a circular space with an area of 2274 m2, the highest-risk factor in the occurrence of at least one to five mattress fires was a decrease in visibility due to smoke. It was confirmed that the ASET had a value between 187 s for low HRR and 212 s for high HRR. This underscores the importance of smoke emission or smoke control performance evaluations based on predictions of the smoke generation of combustibles present in elderly care facilities.
- (2)
The results of the fire simulation confirmed that visibility, temperature, and FED have the most significant effects on ASET, in descending order. It was also confirmed that when the size of the fire was set to 992 kW and 1778.9 kW per bed, the ASET value decreased as the number of mattress fires increased.
- (3)
For the group of patients using wheelchairs, 100% safety can be ensured by evacuating through the ramp under the condition of a fire with fewer than three fire sources (mattresses) and a low HRR.
- (4)
It was confirmed that 100% safety was ensured when evacuating through the ramp for the group of patients with disabilities who used canes.
- (5)
Elevator evacuation was identified as the most high-risk evacuation method, as it could cause more than 40 fatalities, even in a one-mattress fire with low heat release; this is attributed to the lack of space caused by the movement of beds and wheelchairs.
- (6)
In the group with equal proportions of all patients, 100% safety was secured by evacuating through stairs and ramps under the low-HRR one-mattress-fire condition.
- (7)
It was confirmed that the ramp-only evacuation could reduce casualties by a minimum of one person and a maximum of 48 people compared to the stairs-only evacuation, and by a minimum of 25 people and a maximum of 60 people compared to the elevator-only evacuation. This result clarifies that the ramp is an evacuation route that can secure the safety of the vulnerable.
- (8)
Therefore, it is necessary to install ramps in buildings for the vulnerable, such as elderly nursing hospitals and nursing homes, and that evacuation during disaster response training be conducted using ramps.
Based on the results of this study, to implement a specific performance-based design, it is essential to model the evaluation with an actual building and verify it through the optimal installation location for each evacuation route. In addition, if evacuation environment variables such as fire-extinguishing facilities (e.g., sprinklers and smoke exhaust facilities) are reflected, more detailed verification of lamp efficiency is possible.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}