
Socio-Economic Predictors of Hiring Live-In Migrant Care Workers to Support Community Dwelling Older Adults with Long-Term Care Needs: Recent Evidence from a Central Italian Region



Abstract
1. Introduction
1.1. Long-Term and Informal Care in Italy
1.2. The Italian Migrant Care Worker Market
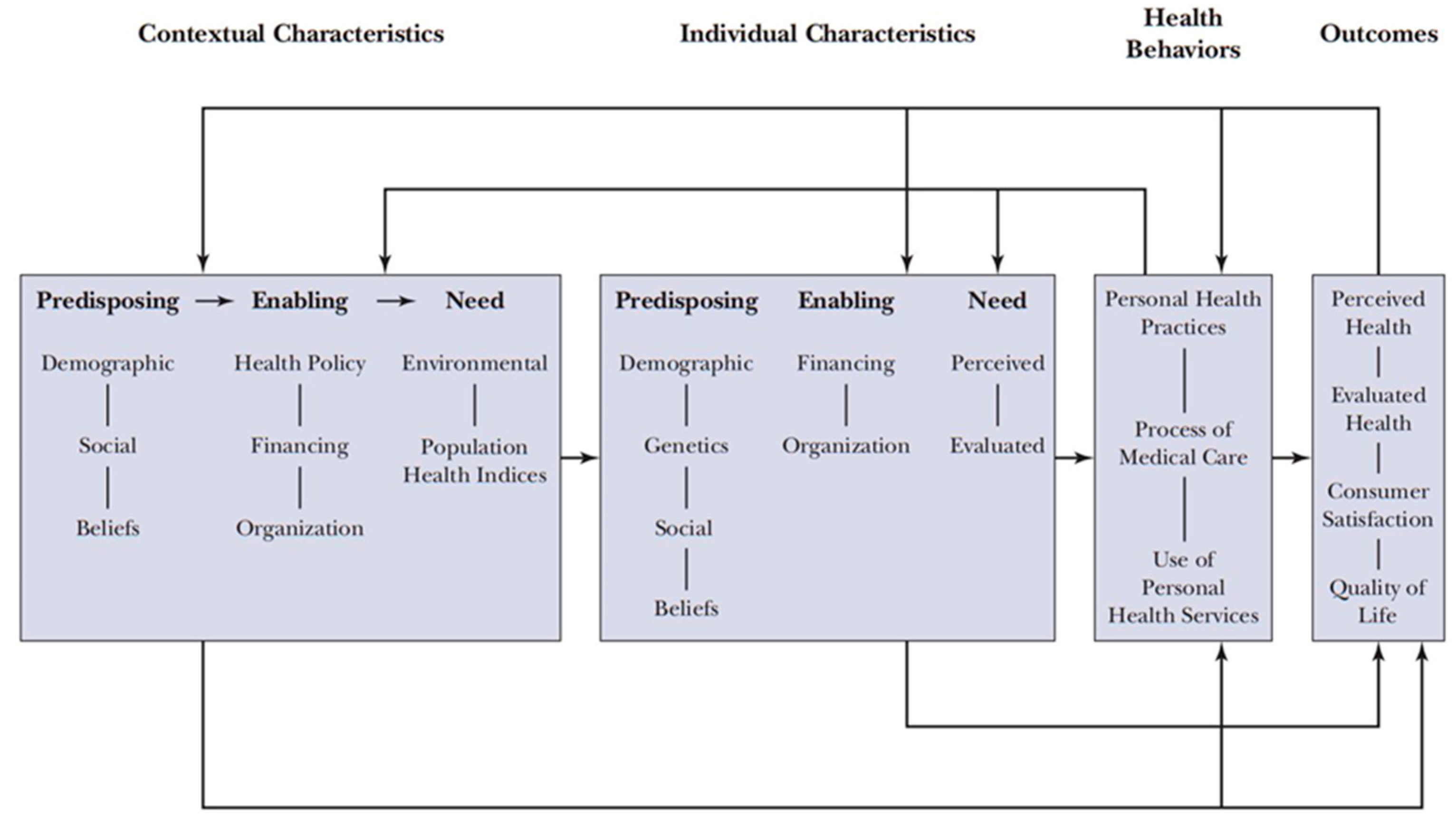
1.3. Behavioural Model of Health Service Use
1.4. Predictors of Hiring Paid Care Workers
1.5. Objectives and Aims
- To determine the predictors of hiring a live-in MCW among adults with LTC needs;
- to analyse the costs and any financial barriers associated with the hiring of live-in MCWs by people in need of care and their informal caregivers;
- to investigate the objective care burden, tasks provided, and perception of care provided by live-in MCWs.
2. Materials and Methods
2.1. Research Design
2.2. Eligibility Criteria for Inclusion
2.3. Recruitment and Data Collection
2.4. Study Sample
2.5. Measures
2.6. Data Analysis
2.7. Ethics
3. Results
3.1. Characteristics of Those That Hired or Did Not Hire a Live-In MCW
3.1.1. Socio-Demographic Factors and Health Status
3.1.2. Support Services
3.2. Predictors of Hiring Live-In MCWs
3.3. Characteristics of Care Provided
3.4. Financial Aspects of Care Provision
4. Discussion
4.1. Links to the Existing Literature
4.2. Implications for Policy and Practice
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Prospects 2019: Highlights; United Nations, Department of Economic and Social Affairs: San Francisco, CA, USA, 2019; pp. 1–1238. [Google Scholar]
- Williams, F. Converging Variations in Migrant Care Work in Europe. J. Eur. Soc. Policy 2012, 22, 363–376. [Google Scholar] [CrossRef]
- King-Dejardin, A. The Social Construction of Migrant Care Work: At the Intersection of Care, Migration and Gender; International Labour Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Spasova, S.; Baeten, R.; Coster, S.; Ghailani, D.; Peña-Casas, R.; Vanhercke, B. Challenges in Long-Term Care in Europe: A Study of National Policies 2018; European Commission: Brussels, Balgium, 2018; ISBN 92-79-87174-9. [Google Scholar]
- Costa, G. Private assistants in the Italian care system: Facts and policies. Obs. Société Br. 2013, 14, 99–117. [Google Scholar] [CrossRef]
- Palumbo, L. Exploiting for care: Trafficking and abuse in domestic work in Italy. J. Immigr. Refugee Stud. 2017, 15, 171–186. [Google Scholar] [CrossRef]
- Papa, R.; Lamura, G. Caregivers’ Iceberg: Qualitative narratives of Italian caregivers’ roles and challenges. J. Gerontol. Geriatr. 2019, 67, 156–167. [Google Scholar]
- Meyer, P. Relations of care: The contexts for immigrant care workers in Northern Italy. Antropol. Work Rev. 2015, 36, 2–12. [Google Scholar] [CrossRef]
- Istat. Condizioni di Salute e Ricorso ai Servizi Sanitari in Italia e nell’Unione Europea—Indagine Ehis 2015. Available online: https://www.istat.it/it/archivio/204655 (accessed on 10 March 2021).
- Maggioli S.p.A. L’assistenza Agli Anziani Non Autosufficienti in Italia: 7° Rapporto 2020/2021; Maggioli S.p.A.: Santarcangelo di Romagna, Italy, 2021; pp. 1–241. [Google Scholar]
- Tur-Sinai, A.; Teti, A.; Rommel, A.; Hlebec, V.; Lamura, G. How many older informal caregivers are there in Europe? Comparison of estimates of their prevalence from three European surveys. Int. J. Environ. Res. Public Health 2020, 17, 9531. [Google Scholar] [CrossRef] [PubMed]
- Bom, J.; Bakx, P.; Schut, F.; van Doorslaer, E. Health effects of caring for and about parents and spouses. J. Econ. Aging 2019, 14, 100196. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Spouses, adult children, and children-in-law as caregivers of older adults: A meta-analytic comparison. Psychol. Aging 2011, 26, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Verbakel, E. How to understand informal caregiving patterns in Europe? The role of formal long-term care provisions and family care norms. Scand. J. Public Health 2018, 46, 436–447. [Google Scholar] [CrossRef]
- Kaschowitz, J.; Brandt, M. Health effects of informal caregiving across Europe: A longitudinal approach. Soc. Sci. Med. 2017, 173, 72–80. [Google Scholar] [CrossRef]
- Istat. Ospiti Dei Presidi Residenziali Socio-Assistenziali e Socio-Sanitari: Anziani per Genere e Livello Di Assistenza Sanitaria—Reg. Available online: http://dati.istat.it/Index.aspx?QueryId=21803 (accessed on 8 March 2021).
- Böcker, A.; Bruquetas Callejo, M.; Horn, V.; Schweppe, C. This Is Affordable! Money Matters in Live-in Migrant Care Worker Arrangements; Nijmegen Sociology of Law Working Papers Series; 2020/02; Radboud University Nijmegen: Nijmegen, The Netherlands, 2020; pp. 1–20. [Google Scholar]
- Cordini, M.; Ranci, C. Legitimising the care market: The social recognition of migrant care workers in Italy. J. Soc. Policy 2017, 46, 91–108. [Google Scholar] [CrossRef]
- Barbabella, F.; Chiatti, C.; Rimland, J.M.; Melchiorre, M.G.; Lamura, G.; Lattanzio, F. Socioeconomic predictors of the employment of migrant care workers by Italian families assisting older Alzheimer’s Disease patients: Evidence from the up-tech study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Casanova, G.; Tur-Sinai, A.; Lamura, G. Innovating long-term care provision in mediterranean welfare states: A comparison between Italy and Israel. J. Aging Soc. Policy 2019, 32, 55–82. [Google Scholar] [CrossRef] [PubMed]
- Rugolotto, S.; Larotonda, A.; van der Geest, S. How migrants keep Italian families Italian: Badanti and the private care of older people. Int. J. Migr. Health Soc. Care 2017, 13, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Baldassar, L.; Ferrero, L.; Portis, L. ‘More like a daughter than an employee’: The kinning process between migrant care workers, elderly care receivers and their extended families. Identities 2017, 24, 524–541. [Google Scholar] [CrossRef]
- Nicolescu, G. Keeping the elderly alive global: Entanglements and embodied practices in long-term care in southeast Italy. Anthropol. Aging 2019, 40, 77–93. [Google Scholar] [CrossRef]
- INPS. Osservatori Statistici e Altre Statistiche. Available online: https://www.inps.it/osservatoristatistici/12/o/350 (accessed on 31 December 2020).
- Governo Italiano. Lavoro Domestico: Accordo Sui Minimi Retributivi 2021. Available online: https://www.lavoro.gov.it/notizie/pagine/lavoro-domestico-accordo-sui-minimi-retributivi-2021.aspx/ (accessed on 10 March 2021).
- INPS. Il rapporto di lavoro. Available online: https://www.inps.it/nuovoportaleinps/default.aspx?itemdir=43287 (accessed on 10 March 2021).
- Scrinzi, F. Caring for the elderly in the family or in the nation? Gender, women and migrant care labour in the Lega Nord. West Eur. Politics 2017, 40, 869–886. [Google Scholar] [CrossRef]
- Fusco, S.; Corsonello, A.; Chiatti, C.; Fabbietti, P.; Salerno, G.; De Bonis, E.; Corica, F.; Lattanzio, F. Migrant care workers and rehospitalization among older patients discharged from acute care hospitals. Geriatr. Gerontol. Int. 2015, 15, 196–203. [Google Scholar] [CrossRef]
- Boccagni, P. Searching for well-being in care work migration: Constructions, practices and displacements among immigrant women in Italy. Soc. Politics 2016, 23, 284–306. [Google Scholar] [CrossRef]
- Miyazaki, R. Migrant care workers and care-migration policies: A comparison between Italy and Japan. Asia Eur. J. 2019, 17, 161–177. [Google Scholar] [CrossRef]
- Ministero dell’Interno. Emersione Dei Rapporti Di Lavoro 2020: Analisi Statistica Delle Domande—Dati Aggiornati Alle Ore 24:00 Del 15 Agosto 2020; Ministero dell’Interno: Roma, Italy, 2020. [Google Scholar]
- Salis, E. A Crucial testing ground: The governance of labour migration in the long-term care sector. Comp. Migr. Stud. 2014, 2, 519–545. [Google Scholar] [CrossRef]
- INPS. Indennità di Accompagnamento per Invalidi Civili. Available online: https://www.inps.it/nuovoportaleinps/default.aspx?itemdir=50194 (accessed on 31 December 2020).
- INPS. Indennità di Accompagnamento—Ciechi Civili Assoluti. Available online: https://www.inps.it/nuovoportaleinps/default.aspx?itemdir=50081 (accessed on 31 December 2020).
- Nicolescu, G. From border fetishism to tactical socialism. East Cent. Eur. 2018, 45, 279–299. [Google Scholar] [CrossRef]
- Di Santo, P.; Ceruzzi, F. Migrant Care Workers in Italy. A Case Study; Interlinks Project: Delft, The Netherlands, 2010; Available online: http://interlinks.euro.centre.org/sites/default/files/WP5_MigrantCarers_FINAL.pdf (accessed on 7 May 2021).
- Andersen, R.M.; Davidson, P.L. Improving access to care in america: Individual and contextual indicators. In Changing the U.S. Health Care System: Key Issues in Health Services Policy and Management, 3rd ed.; Jossey-Bass: San Francisco, CA, USA, 2007; pp. 3–31. [Google Scholar]
- Rogero-García, J.; Rosenberg, M.W. Paid and unpaid support received by co-resident informal caregivers attending to community-dwelling older adults in Spain. Eur. J. Ageing 2011, 8. [Google Scholar] [CrossRef]
- Pego, M.A.; Nunes, C. Aging, Disability, and Informal Caregivers: A Cross-Sectional Study in Portugal. Front. Med. 2018, 4, 255. [Google Scholar] [CrossRef] [PubMed]
- Di Rosa, M.; Melchiorre, M.G.; Lucchetti, M.; Lamura, G. The impact of migrant work in the elder care sector: Recent trends and empirical evidence in Italy. Eur. J. Soc. Work 2012, 15, 9–27. [Google Scholar] [CrossRef]
- Di Rosa, M.; Barbabella, F.; Chiatti, C.; Melchiorre, M.G.; Lamura, G. Private employment of home care workers and use of health services by disabled older people in Italy. Euroreg. J. Socio-Econ. Anal. 2013, 1, 33–42. [Google Scholar]
- Van Hooren, F. When families need immigrants: The exceptional position of migrant domestic workers and care assistants in Italian immigration policy. Bull. Ital. Politics 2010, 2, 21–38. [Google Scholar]
- World Health Organization Delivering Quality Health Services: A Global Imperative; OECD Publishing: Paris, France, 2018; ISBN 92-64-30030-9.
- United Nations. Goal 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 25 April 2021).
- Addati, L.; Cattaneo, U.; Esquivel, V.; Valarino, I. Care Work and Care Jobs for the Future of Decent Work; International Labour Organization: Geneva, Switzerland, 2018. [Google Scholar]
- United Nations. Goal 4: Quality Education. Available online: https://www.globalgoals.org/4-quality-education (accessed on 25 April 2021).
- United Nations. Goal 5: Gender Equality. Available online: https://www.globalgoals.org/5-gender-equality (accessed on 25 April 2021).
- United Nations. Goal 8: Decent Work and Economic Growth. Available online: https://www.globalgoals.org/8-decent-work-and-economic-growth (accessed on 25 April 2021).
- Scrinzi, F. Beyond “Women’s Work”: Gender, ethnicity, and the management of paid care work in nonprofit domiciliary services in Italy. J. Immigr. Refug. Stud. 2018, 17, 441–456. [Google Scholar] [CrossRef]
- Bonatti, V.; Muniandy, P. Defiant aspirations: Migrant women’s struggles for stability and upward mobility in Naples and Kuala Lumpur. Migr. Stud. 2018, 8, 113–130. [Google Scholar] [CrossRef]
- Piccinini, F.; Gagliardi, C.; Lamura, G.; Fabbietti, P. L’assistenza Alle Persone Anziane Non Autosufficienti Nella Regione Marche: Il Punto Di Vista Degli Interessati e Delle Loro Famiglie; IRCCS INRCA: Ancona, Italy, 2020; pp. 1–54. [Google Scholar]
- Tuttitalia. Regione Marche. Available online: https://www.tuttitalia.it/marche/ (accessed on 28 April 2021).
- Agenzia Regionale Sanitaria. L’organizzazione Dei Servizi Sanitari e Sociali Territoriali Nella Regione Marche: Presentazione Del Rapporto 2018; Regione Marche: Ancona, Italy, 2018. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index: A simple index of independence useful in scoring improvement in the rehabilitation of the chronically Ill. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Fillenbaum, G.G. Screening the Elderly: A brief instrumental activities of daily living measure. J. Am. Geriatr. Soc. 1985, 33, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Galeoto, G.; Lauta, A.; Palumbo, A.; Castiglia, S.; Mollica, R.; Santilli, V.; Sacchetti, M. The barthel index: Italian translation, adaptation and validation. Int. J. Neurol. Neurother. 2015, 2, 2378–3001. [Google Scholar]
- Ando, S.; Higuchi, Y.; Kitagawa, T.; Murakami, T.; Todo, E.; Ueda, T. Instrumental activities of daily living and number of daily steps in frail older females. J. Phys. Ther. Sci. 2019, 31, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Gallo, E.; Scrinzi, F. Outsourcing elderly care to migrant workers: The impact of gender and class on the experience of male employers. Sociology 2016, 50, 366–382. [Google Scholar] [CrossRef]
- Boccagni, P. At home in home care? Contents and boundaries of the ‘domestic’ among immigrant live-in workers in Italy. Hous. Stud. 2018, 33, 813–831. [Google Scholar] [CrossRef]
- International Labour Organization. How to Facilitate the Recognition of Skills of Migrant Workers: Guide for Employment Services Providers, 2nd ed.; International Labour Organization: Geneva, Switzerland, 2020; ISBN 9789220323076. [Google Scholar]
- Da Roit, B.; Le Bihan, B. Similar and Yet So Different: Cash-for-Care in Six European Countries’ Long-Term Care Policies. Milbank Q. 2010, 88, 286–309. [Google Scholar] [CrossRef] [PubMed]
- Da Roit, B.; Van Bochove, M. Migrant Care Work Going Dutch? The Emergence of a Live in Migrant Care Market and the Restructuring of the Dutch Long-term Care System. Soc. Policy Adm. 2017, 51, 76–94. [Google Scholar] [CrossRef]
- Sowa-Kofta, A.; Rodrigues, R.; Lamura, G.; Sopadzhiyan, A.; Wittenberg, R.; Bauer, G.; Doetter, L.F.; Ilinca, S.; Marczak, J.; Piersinaru, A. Long-term care and migrant care work: Addressing workforce shortages while raising questions for European Countries. Eurohealth 2019, 25, 15–18. [Google Scholar]
- Bordogna, M.T. Regional health systems and non-conventional medicine: The situation in Italy. EPMA J. 2011, 2, 411–423. [Google Scholar] [CrossRef][Green Version]
- Rogalewski, A.; Florek, K. The Future of Live-in Care Work in Europe: Report on the EESC Country Visits to the United Kingdom, Germany, Italy and Poland Following up on the EESC Opinion on “The Rights of Live-in Care Workers”; European Economic and Social Committee: Brussels, Belgium, 2020. [Google Scholar]



{kind=link}
{kind=link}
| No MCW N = 88 | MCW N = 278 | Total a N = 366 | p-Value b | |
|---|---|---|---|---|
| Predisposing characteristics | ||||
| Gender: women | 64.0 | 64.8 | 64.2 | 0.899 |
| Age | 63.56 (11.92) | 62.18 (9.04) | 63.23 (11.30) | 0.319 |
| Relationship status | 0.509 | |||
| Married | 67.3 | 75.0 | 69.1 | |
| Separated | 5.4 | 5.7 | 5.5 | |
| Widowed | 10.4 | 6.8 | 9.6 | |
| Other | 16.9 | 12.5 | 15.8 | |
| Education | <0.001 | |||
| No title | 1.8 | 0.0 | 1.4 | |
| Primary | 17.3 | 6.8 | 14.8 | |
| Middle school | 29.9 | 19.3 | 27.3 | |
| High school | 42.1 | 48.9 | 43.7 | |
| Above high school | 9.0 | 25.0 | 12.8 | |
| Relationship to the person in need of care | 0.001 | |||
| Husband/Wife | 25.9 | 4.5 | 20.8 | |
| Son/Daughter | 60.4 | 72.7 | 63.4 | |
| Other | 13.7 | 22.7 | 15.9 | |
| Enabling factors | ||||
| Distance to person in need of care | 0.001 | |||
| Live in the same apartment | 67.6 | 17.0 | 55.5 | |
| Live in same apartment building | 11.2 | 17.0 | 12.6 | |
| Walking distance | 11.5 | 33.0 | 16.7 | |
| Need to travel by car, bus, or train | 9.8 | 32.9 | 15.0 | |
| Currently working c: yes | 30.4 | 35.6 | 31.7 | 0.364 |
| No MCW N = 88 | MCW N = 278 | Total a N = 366 | p-Value b | |
|---|---|---|---|---|
| Predisposing characteristics | ||||
| Gender: women | 69.8 | 79.5 | 72.1 | 0.075 |
| Age | 85.37 (6.13) | 88.32 (6.44) | 86.08 (6.32) | <0.001 |
| Relationship status | 0.039 | |||
| Married | 39.6 | 22.7 | 35.5 | |
| Widowed | 55.8 | 70.5 | 59.3 | |
| Other | 4.7 | 6.8 | 5.2 | |
| Education level c | 0.143 | |||
| No title | 13.1 | 13.8 | 13.3 | |
| Primary | 64.7 | 64.4 | 64.6 | |
| Middle school | 13.5 | 8.0 | 12.2 | |
| High school | 5.5 | 11.5 | 6.9 | |
| Above high school | 3.3 | 2.2 | 3.0 | |
| Enabling factors | ||||
| Individual level | ||||
| Work pension d: yes | 71.1 | 63.6 | 69.3 | 0.185 |
| Social pension: yes | 10.8 | 19.3 | 12.8 | 0.037 |
| Disability pension: yes | 16.5 | 15.9 | 16.4 | 0.888 |
| Cash-for-care allowance (IdA): yes | 78.8 | 90.9 | 81.7 | 0.010 |
| Survivor’s pension d: yes | 46.6 | 61.4 | 50.1 | 0.016 |
| Annuities or income from rent/interest/dividends: yes | 5.0 | 11.4 | 6.6 | 0.037 |
| Income c | 0.030 | |||
| Less than 500 EUR/month | 1.8 | 1.1 | 1.6 | |
| 500–1000 EUR/month | 27.7 | 14.9 | 24.6 | |
| 1000–1500 EUR/month | 51.3 | 56.3 | 52.5 | |
| 1500–2000 EUR/month | 15.3 | 14.9 | 15.2 | |
| More than 2000 EUR/month | 4.0 | 12.6 | 6.1 | |
| Contextual level | ||||
| Household income e | 0.561 | |||
| Less than 1000 EUR/month | 5.3 | 2.4 | 4.7 | |
| 1000–1500 EUR/month | 24.0 | 32.9 | 26.2 | |
| 1500–2000 EUR/month | 24.0 | 24.4 | 24.1 | |
| 2000–2500 EUR/month | 22.5 | 17.1 | 21.2 | |
| 2500–3000 EUR/month | 14.9 | 14.6 | 14.8 | |
| More than 3000 EUR/month | 9.2 | 8.5 | 9.0 | |
| Needs characteristics | ||||
| ADL | 43.00 (25.53) | 34.94 (21.34) | 41.07 (23.25) | 0.004 |
| OR | 95% CI | p-Value | ||
|---|---|---|---|---|
| Person in need of care | ||||
| Predisposing characteristics | ||||
| Age (1 year increase) | 1.077 | 1.034 | 1.122 | <0.001 |
| Enabling characteristics | ||||
| Receiving social pension (ref: no) | 2.258 | 1.121 | 4.549 | 0.037 |
| Needs characteristics | ||||
| ADL (1 point increase) | 0.982 | 0.971 | 0.994 | 0.005 |
| Informal caregiver | ||||
| Predisposing characteristics | ||||
| Level of formal education (ref: below high school diploma) | 3.880 | 1.982 | 7.595 | <0.001 |
| Total a | |
|---|---|
| Number of months being provided care by an MCW (n = 84) | 35.43 (40.65) |
| The MCW had received skills training specific to caring for older adults or someone with a disability (n = 88) | |
| Yes | 6.8 |
| No | 68.2 |
| Do not know | 25.0 |
| Person in need of care’s views on the care provided by MCWs (n = 88) | |
| Positive | 89.8 |
| Positive and negative | 3.4 |
| Neutral | 5.7 |
| Negative | 1.1 |
| Hours of care provided per week (n = 85) | 75.22 (48.16) |
| Worked above 54 h per week b: yes (n = 85) | 37.5 |
| Care tasks provided/hours per week | |
| Personal care and hygiene (n = 80) | 33.59 (42.47) |
| Home mobility (n = 71) | 24.45 (30.91) |
| Supervision (n = 72) | 53.08 (54.29) |
| Domestic work including cooking (n = 68) | 28.12 (30.00) |
| Mobility outside the home (including transportation; n = 39) | 22.86 (36.48) |
| No MCW | MCW | Total a | |
|---|---|---|---|
| Did the person in need of care have or would have had difficulties in the past year in affording the costs of hiring a live-in MCW? | n = 272 | n = 87 | n = 359 |
| yes | 49.3 | 57.5 | 51.3 |
| Did the informal caregiver have or would have had problems in the last year relating to the additional expenses resulting from the hiring of a live-in MCW? | n = 276 | n = 87 | n = 363 |
| No additional expenses | 66.3 | 28.7 | 57.30 |
| Never | 11.6 | 4.6 | 9.9 |
| Sometimes | 6.5 | 10.3 | 7.4 |
| Often | 9.8 | 28.7 | 14.3 |
| A lot | 5.8 | 27.6 | 11.0 |
| The cost spent per month on hiring an MCW in EUR (n = 81) | N/A | 1167.46 (247.90) | 1167.46 (247.90) |
| The MCW received on or above the minimum wage for those caring for an older adult with long-term care needs b: yes (n = 81) | N/A | 76.1 | 76.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fisher, O.; Fabbietti, P.; Lamura, G. Socio-Economic Predictors of Hiring Live-In Migrant Care Workers to Support Community Dwelling Older Adults with Long-Term Care Needs: Recent Evidence from a Central Italian Region. Sustainability 2021, 13, 5349. https://doi.org/10.3390/su13105349
Fisher O, Fabbietti P, Lamura G. Socio-Economic Predictors of Hiring Live-In Migrant Care Workers to Support Community Dwelling Older Adults with Long-Term Care Needs: Recent Evidence from a Central Italian Region. Sustainability. 2021; 13(10):5349. https://doi.org/10.3390/su13105349
Chicago/Turabian StyleFisher, Oliver, Paolo Fabbietti, and Giovanni Lamura. 2021. "Socio-Economic Predictors of Hiring Live-In Migrant Care Workers to Support Community Dwelling Older Adults with Long-Term Care Needs: Recent Evidence from a Central Italian Region" Sustainability 13, no. 10: 5349. https://doi.org/10.3390/su13105349
APA StyleFisher, O., Fabbietti, P., & Lamura, G. (2021). Socio-Economic Predictors of Hiring Live-In Migrant Care Workers to Support Community Dwelling Older Adults with Long-Term Care Needs: Recent Evidence from a Central Italian Region. Sustainability, 13(10), 5349. https://doi.org/10.3390/su13105349