
Time Capsule Medicine: A Mixed-Methods Pilot Study on Immersive Simulation for Chronic Disease Education in Medical Students


Abstract
1. Introduction
- (1)
- To quantitatively evaluate the impact of an immersive, time-lapse simulation on medical students’ confidence, empathy, and understanding of chronic disease management, measured through pre- and post-simulation surveys.
- (2)
- To qualitatively explore students’ lived experiences of managing chronic illness over time, including their reflections on the continuity of care, emotional and functional challenges, and systemic barriers to effective patient-centred care.
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Variables and Data Sources/Measurement
2.4. Intervention Structure
2.4.1. Phase 1: Preparation
- An in-depth overview on chronic diseases, such as diabetes, osteoarthritis, and macular degeneration, and how these conditions evolve over decades;
- Discussion of age-related changes: physical frailty, impairment of vision, and decline of cognition;
- There are ethical considerations in the understanding and empathising of the journeys of the patients by insisting on continuity of care.
2.4.2. Phase 2: Immersive Simulation
- Year 0–5: Early-stage disease with minimal functional impact. Students simulated managing a new diagnosis and initiating medication.
- Year 6–10: moderate disease progression, introducing physical limitations, such as mobility challenges (e.g., using weighted clothing), and addressing intermittent symptoms and assistive device use.
- Year 11–15: Advanced stages with significant physical and emotional strain. This phase included simulations of vision impairments (e.g., blurred vision goggles) and the complexities of managing multiple medications.
- Year 16–20: Severe disease progression characterised by high dependency, cognitive impairments (e.g., memory challenges), and reliance on caregivers or structured medical routines.
- Managing complex medication schedules with visual or cognitive limitations;
- Navigating to medical appointments despite physical constraints;
- Balancing daily activities, like cooking or personal hygiene, alongside health-related challenges.
2.4.3. Phase 3: Review and Reflection
- “Describe the most significant challenge you faced during the simulation and, importantly, how it enhanced your insight into the management of long-term patient care.”
- “How did the simulated disease progression influence your concept of continuity of care?”
- “What changes would you recommend in the healthcare system to better support patients with chronic conditions over decades?”
2.5. Bias
2.6. Analysis Process
2.7. Ethical Considerations
3. Results
3.1. Participant Demographics
3.2. Impact on Students’ Knowledge and Confidence
3.3. Students’ Experience During the Simulation
3.4. Post-Simulation Reflections
3.5. Quantitative Outcomes
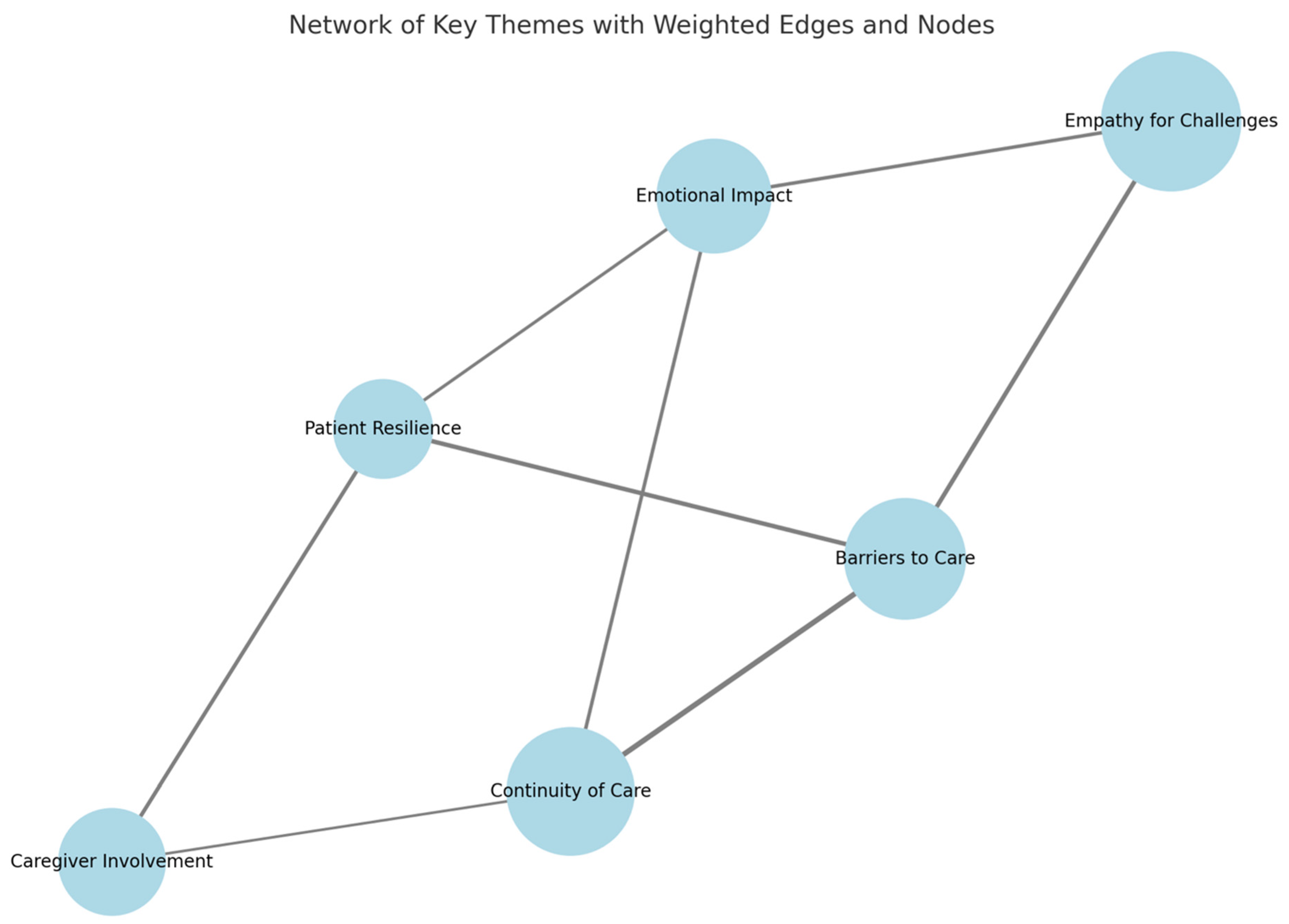
3.6. Qualitative Outcomes
- Empathy for Progressive Challenges: students most often shared a new sense of empathy related to the progressive loss of independence associated with such illnesses.
- Barriers to Care: the major barriers to healthcare identified by the students were transportation, mobility restrictions, and declines in cognition.
- Continuity of Care: students continuously identified the need for continuity in care plans, which must be both evolving and patient-centred throughout the course of the patient’s disease.
- Psychological Effects that Patients Often Undergo: the simulation depicted, among other aspects, the psychological effects brought forth by chronic diseases, including feelings of isolation and frustration, which clinical settings usually fail to acknowledge.
4. Discussion
4.1. Key Results
4.2. Interpretations
4.3. Generalisability
4.4. Practical Applications and Scalability of Time Capsule Medicine Model
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Student Forms
Appendix A.1. Pre-Simulation Survey
- 1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree.
| Statement | 1 | 2 | 3 | 4 | 5 |
| |||||
| |||||
| |||||
| |||||
|
- What do you expect to learn about chronic disease management from this simulation?
- What do you think will be the most challenging aspect of managing long-term care for patients?
- How do you currently approach patients with chronic conditions in your clinical practice?
Appendix A.2. Post-Simulation Survey
- 1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree.
| Statement | 1 | 2 | 3 | 4 | 5 |
| |||||
| |||||
| |||||
| |||||
|
- What was the most valuable lesson you learned from this simulation?
- How has your understanding of patient-centred care for chronic conditions changed after this experience?
- What challenges did you face during the simulation, and how did you overcome them?
Appendix A.3. Reflective Journal Prompts
- 4.
- Describe your experience managing a patient in the early stage of chronic disease progression. How did the patient’s emotional and practical challenges influence your approach?
- 5.
- Reflect on the challenges you encountered during the moderate stage of the simulation. What strategies did you find most effective in addressing these challenges?
- 6.
- What insights did you gain about managing polypharmacy and functional impairments during the advanced stage?
- 7.
- Discuss the key lessons from the severe stage regarding caregiver dependency and cognitive decline. How will these experiences shape your future practice?
- 8.
- Overall, how has this simulation influenced your perspective on continuity of care and the long-term impacts of chronic diseases?
References
- Hacker, K. The Burden of Chronic Disease. Mayo Clin. Proc. Innov. Qual. Outcomes 2024, 8, 112–119. [Google Scholar] [CrossRef]
- Reynolds, R.; Dennis, S.; Hasan, I.; Slewa, J.; Chen, W.; Tian, D.; Bobba, S.; Zwar, N. A systematic review of chronic disease management interventions in primary care. BMC Fam. Pract. 2018, 19, 11. [Google Scholar] [CrossRef]
- General Medical Council. Outcomes for Graduates. Available online: https://www.gmc-uk.org/-/media/documents/outcomes-for-graduates-2020_pdf-84622587.pdf (accessed on 25 November 2024).
- Monrouxe, L.V.; Bullock, A.; Gormley, G.; Kaufhold, K.; Kelly, N.; Roberts, C.E.; Mattick, K.; Rees, C. New graduate doctors’ preparedness for practice: A multistakeholder, multicentre narrative study. BMJ Open 2018, 8, e023146. [Google Scholar] [CrossRef]
- Benkel, I.; Arnby, M.; Molander, U. Living with a chronic disease: A quantitative study of the views of patients with a chronic disease on the change in their life situation. SAGE Open Med. 2020, 8, 2050312120910350. [Google Scholar] [CrossRef]
- Ljungholm, L.; Klinga, C.; Edin-Liljegren, A.; Ekstedt, M. What matters in care continuity on the chronic care trajectory for patients and family carers?—A conceptual model. J. Clin. Nurs. 2022, 31, 1327–1338. [Google Scholar] [CrossRef]
- Stoutenberg, M.; Lewis, L.K.; Jones, R.M.; Portacio, F.; Vidot, D.C.; Kornfeld, J. Assessing the current and desired levels of training and applied experiences in chronic disease prevention of students during medical school. BMC Med. Educ. 2023, 23, 54. [Google Scholar] [CrossRef]
- Novo-Veleiro, I.; Bengoa, R.; Pose-Reino, A. Teaching about chronicity in medical schools—A review of the current situation. Rev. Clín. Esp. (Engl. Ed.) 2023, 223, 100–113. [Google Scholar] [CrossRef]
- Lavanya, K.M.; Somu, L.K.; Mishra, S.K. Effectiveness of Scenario-based Roleplay as a Method of Teaching Soft Skills for Undergraduate Medical Students. Int. J. Appl. Basic Med. Res. 2024, 14, 78–84. [Google Scholar] [CrossRef]
- Del Moral, B.L.M.; VanPutte, C.L.; McCracken, B.A. The use of role-play in the learning of medical terminology for online and face-to-face courses. Adv. Physiol. Educ. 2024, 48, 578–587. [Google Scholar] [CrossRef]
- Xu, L.; Liu, W.; Jiang, X.; Li, Y. Impact of using peer role-playing on the clinical skills performance of pediatric trainees. BMC Med. Educ. 2023, 23, 654. [Google Scholar] [CrossRef]
- Nelson, E.E.C.; Spence, A.D.; Gormley, G.J. Stepping into the shoes of older people: A scoping review of simulating ageing experiences for healthcare professional students. Age Ageing 2023, 52, afad235. [Google Scholar] [CrossRef]
- Bharti, R.K. Contribution of Medical Education through Role Playing in Community Health Promotion: A Review. Iran. J. Public Health 2023, 52, 1121–1128. [Google Scholar] [CrossRef]
- Nagel, D.A.; Penner, J.L.; Halas, G.; Philip, M.T.; Cooke, C.A. Exploring experiential learning within interprofessional practice education initiatives for pre-licensure healthcare students: A scoping review. BMC Med. Educ. 2024, 24, 139. [Google Scholar] [CrossRef]
- Hense, H.; Harst, L.; Küster, D.; Walther, F.; Schmitt, J. Implementing longitudinal integrated curricula: Systematic review of barriers and facilitators. Med. Educ. 2021, 55, 558–573. [Google Scholar] [CrossRef]
- Puvanendran, R.; Vasanwala, F.F.; Kamei, R.K.; Hock, L.K.; Lie, D.A. What do medical students learn when they follow patients from hospital to community? A longitudinal qualitative study. Med. Educ. Online 2012, 17, 18899. [Google Scholar] [CrossRef]
- Howick, J.; Dudko, M.; Feng, S.N.; Ahmed, A.A.; Alluri, N.; Nockels, K.; Winter, R.; Holland, R. Why might medical student empathy change throughout medical school? a systematic review and thematic synthesis of qualitative studies. BMC Med. Educ. 2023, 23, 270. [Google Scholar] [CrossRef]
- Mullen, K.; Nicolson, M.; Cotton, P. Improving medical students’ attitudes towards the chronic sick: A role for social science research. BMC Med. Educ. 2010, 10, 84. [Google Scholar] [CrossRef]
- Forestier, B.; Anthoine, E.; Reguiai, Z.; Fohrer, C.; Blanchin, M. A systematic review of dimensions evaluating patient experience in chronic illness. Health Qual. Life Outcomes 2019, 17, 19. [Google Scholar] [CrossRef]
- Collins, C.; Doran, G.; Patton, P.; Fitzgerald, R.; Rochfort, A. Does education of primary care professionals promote patient self-management and improve outcomes in chronic disease? An updated systematic review. BJGP Open 2021, 5, BJGPO.2020.0186. [Google Scholar] [CrossRef]
- Chen, H.; Xuan, H.; Cai, J.; Liu, M.; Shi, L. The impact of empathy on medical students: An integrative review. BMC Med. Educ. 2024, 24, 455. [Google Scholar] [CrossRef]
- Pal, D.; Taywade, M.; Gopi, K. Experiential Learning: How Pedagogy is Changing in Medical Education. Curr. Med. Issues 2022, 20, 198–200. [Google Scholar] [CrossRef]
- Lazari, E.C.; Mylonas, C.C.; Thomopoulou, G.E.; Manou, E.; Nastos, C.; Kavantzas, N.; Pikoulis, E.; Lazaris, A.C. Experiential student study groups: Perspectives on medical education in the post-COVID-19 period. BMC Med. Educ. 2023, 23, 42. [Google Scholar] [CrossRef]
- Bierman, A.S.; Wang, J.; O’Malley, P.G.; Moss, D.K. Transforming care for people with multiple chronic conditions: Agency for Healthcare Research and Quality’s research agenda. Health Serv. Res. 2021, 56 (Suppl. S1), 973–979. [Google Scholar] [CrossRef]
- Driessen, E.; van Tartwijk, J.; Dornan, T. The self critical doctor: Helping students become more reflective. Bmj 2008, 336, 827–830. [Google Scholar] [CrossRef]
- Teuwen, C.; van der Burgt, S.; Kusurkar, R.; Schreurs, H.; Daelmans, H.; Peerdeman, S. How does interprofessional education influence students’ perceptions of collaboration in the clinical setting? A qualitative study. BMC Med. Educ. 2022, 22, 325. [Google Scholar] [CrossRef]
- Verbree, A.-R.; Isik, U.; Janssen, J.; Dilaver, G. Inclusion and diversity within medical education: A focus group study of students’ experiences. BMC Med. Educ. 2023, 23, 61. [Google Scholar] [CrossRef]
- Eggeling, M.; Bientzle, M.; Korger, S.; Kimmerle, J. The impact of patient narratives on medical students’ perceptions of shared decision making: A randomized controlled trial. Med. Educ. Online 2021, 26, 1886642. [Google Scholar] [CrossRef]
- Foo, K.M.; Sundram, M.; Legido-Quigley, H. Facilitators and barriers of managing patients with multiple chronic conditions in the community: A qualitative study. BMC Public Health 2020, 20, 273. [Google Scholar] [CrossRef]
- Schwarz, T.; Schmidt, A.E.; Bobek, J.; Ladurner, J. Barriers to accessing health care for people with chronic conditions: A qualitative interview study. BMC Health Serv. Res. 2022, 22, 1037. [Google Scholar] [CrossRef]
- Ocloo, J.; Goodrich, J.; Tanaka, H.; Birchall-Searle, J.; Dawson, D.; Farr, M. The importance of power, context and agency in improving patient experience through a patient and family centred care approach. Health Res. Policy Syst. 2020, 18, 10. [Google Scholar] [CrossRef]
- Witkowski, K.; Okhai, R.; Neely, S.R. Public perceptions of artificial intelligence in healthcare: Ethical concerns and opportunities for patient-centered care. BMC Med. Ethics 2024, 25, 74. [Google Scholar] [CrossRef] [PubMed]
- Arshad, M.; Sriram, S.; Khan, S.; Gollapalli, P.K.; Albadrani, M. Mediating role of physician’s empathy between physician’s communication and patient’s satisfaction. J. Fam. Med. Prim. Care 2024, 13, 1530–1534. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, A.; Hickey, Z.; Patel, N.; Newbigging, J.; Wolfrom, B. Training medical students and residents in the use of electronic health records: A systematic review of the literature. J. Am. Med. Inform. Assoc. 2020, 27, 175–180. [Google Scholar] [CrossRef]
- Balmer, D.F.; Varpio, L.; Bennett, D.; Teunissen, P.W. Longitudinal qualitative research in medical education: Time to conceptualise time. Med. Educ. 2021, 55, 1253–1260. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Key Activities | Objectives | Outcomes Measured |
|---|---|---|---|
| Phase 1: Preparation |
|
|
|
| Phase 2: Immersive Simulation |
|
|
|
| Phase 3: Reflection and Evaluation |
|
|
|
| Phase | Year Range | Key Activities | Simulated Challenges | Learning Objectives |
|---|---|---|---|---|
| Early Stage | 0–5 | Students simulated managing an initial diagnosis and initiating treatment plans. | Minimal functional impact; students focused on understanding disease basics and patient concerns. | Understand the patient’s emotional and practical challenges upon receiving a chronic diagnosis. |
| Moderate Stage | 6–10 | Role-playing involved navigating mobility challenges and intermittent symptoms while continuing treatment. | Weighted clothing to mimic frailty, scenarios for addressing adherence issues, and balancing daily tasks. | Build strategies for managing mid-stage disease progression and assisting patients with moderate limitations. |
| Advanced Stage | 11–15 | Students simulated managing complex medication regimens and significant physical impairments. | Blurred vision goggles, frequent doctor visits, and increasing reliance on assistive devices. | Recognise the cumulative challenges of polypharmacy, physical limitations, and emotional stress. |
| Severe Stage | 16–20 | Simulations emphasised dependency on caregivers and adapting care plans for cognitive decline. | Memory impairments, reliance on caregiver support, and structured medical routines. | Develop empathy and strategies for supporting patients with high dependency and reduced independence. |
| Characteristic | Value |
|---|---|
| Mean age (years) | 24.3 ± 1.2 |
| Gender | |
| Female | 53% (n = 16) |
| Male | 47% (n = 14) |
| Ethnicity | |
| White | 50% |
| Asian | 27% |
| Black | 13% |
| Other | 10% |
| Completed primary care rotation | 100% |
| Completed internal medicine rotation | 87% |
| Completed surgical rotation | 60% |
| Prior chronic disease management exposure | 40% |
| Prior palliative care exposure | 33% |
| Involved in long-term follow-up care | 60% |
| Attended communication skills workshops | 80% |
| Prior experience with chronic disease simulation | 37% |
| Metric | Pre-Simulation Score | Post-Simulation Score | Change |
|---|---|---|---|
| Confidence in managing long-term disease trajectories | 2.8 ± 0.9 | 4.3 ± 0.6 | +1.5 points |
| Understanding of age-related challenges (e.g., cognitive decline and mobility restrictions) | 3.1 ± 1.0 | 4.5 ± 0.5 | +1.4 points |
| Recognition of the importance of continuity of care | 3.2 ± 0.8 | 4.6 ± 0.4 | +1.4 points |
| Perceived ability to address non-clinical barriers (e.g., transportation and caregiver support) | 2.9 ± 0.7 | 4.1 ± 0.6 | +1.2 points |
| Empathy for patients with chronic illnesses | 3.0 ± 0.9 | 4.7 ± 0.5 | +1.7 points |
| Understanding of healthcare provider–patient dynamics | 3.3 ± 0.8 | 4.5 ± 0.5 | +1.2 points |
| Students who felt prepared to manage chronic conditions | 35% | 87% | +52% |
| Students who recognised age-related changes as critical in care planning | 42% | 92% | +50% |
| Phase | Metric | Pre-Simulation Score | Post-Simulation Score | Change |
|---|---|---|---|---|
| Early Stage | Confidence in initial disease management | 3.0 ± 0.8 | 4.2 ± 0.5 | +1.2 |
| Understanding of emotional challenges | 3.2 ± 0.7 | 4.3 ± 0.6 | +1.1 | |
| Moderate Stage | Confidence in managing mid-stage disease | 2.9 ± 0.6 | 4.4 ± 0.4 | +1.5 |
| Awareness of systemic barriers | 2.8 ± 0.8 | 4.3 ± 0.5 | +1.5 | |
| Advanced Stage | Empathy for progressive physical challenges | 3.0 ± 0.9 | 4.6 ± 0.5 | +1.6 |
| Confidence in polypharmacy management | 2.7 ± 0.8 | 4.2 ± 0.5 | +1.5 | |
| Severe Stage | Awareness of caregiver roles | 3.1 ± 0.7 | 4.5 ± 0.4 | +1.4 |
| Confidence in supporting high-dependency care | 2.9 ± 0.9 | 4.4 ± 0.5 | +1.5 |
| Theme | Description | Illustrative Student Quotes | Key Implications |
|---|---|---|---|
| Empathy for Progressive Challenges | Students developed a deeper understanding of the gradual, compounding difficulties faced by patients with chronic illnesses, including the loss of independence and emotional toll. | “I never realised how much something as small as blurry vision could disrupt someone’s daily life.” | Emphasises the need for holistic care that addresses not only physical symptoms but also emotional and logistical barriers. |
| Recognition of Barriers to Care | Participants identified systemic challenges, such as transportation difficulties, reliance on caregivers, and access to assistive devices, as significant barriers to effective care. | “It’s not just the disease—it’s how patients have to navigate everything around it that makes managing their health so hard.” | Highlights the importance of integrating support services and community resources into chronic disease management plans. |
| Emotional Impact on Patients | Students gained insight into the psychological toll of chronic diseases, including feelings of isolation, frustration, and dependency. | “Living with this condition for 20 years isn’t just about managing the disease—it’s about how it affects your entire identity.” | Suggests incorporating mental health support and counselling into routine care for patients with chronic conditions. |
| Importance of Continuity of Care | The simulation reinforced the value of sustained, adaptable care over decades to meet the evolving needs of patients. | “This made me realise that our role isn’t just to treat the disease—it’s to be there for the patient as their life changes.” | Encourages medical education to place greater emphasis on longitudinal care and patient-centred approaches. |
| Challenges in Balancing Priorities | Students found it difficult to address all aspects of a patient’s care, particularly when physical, cognitive, and emotional needs conflicted or compounded each other. | “It was overwhelming to think about balancing their medications, appointments, and mental health at the same time.” | Stresses the need for multidisciplinary care teams to address the multifaceted needs of patients with chronic illnesses. |
| Realisation of Patient Resilience | Students were impressed by the resilience and adaptability of patients despite significant challenges, fostering a greater appreciation for patient experiences. | “Even with all the difficulties, patients still find ways to get through their day—it’s inspiring and humbling.” | Suggests incorporating patient narratives and testimonials into medical training to complement simulations and foster respect for patient resilience. |
| Proposals for Care Improvements | Participants suggested actionable strategies, such as expanding home-based care, improving transportation support, and enhancing caregiver involvement in healthcare planning. | “We need to think beyond the clinic—patients need systems that make their lives easier, not more complicated.” | Encourages the development of innovative, patient-centred healthcare policies and interventions that address non-clinical barriers. |
| Resource Level | Category | Adaptation Strategies |
|---|---|---|
| Low resource | Physical constraints | Use weighted backpacks, gloves, and blurred vision sheets instead of costly simulation tools. |
| Role-playing and storytelling | Conduct small-group role-playing or use narrative-based storytelling to simulate disease progression. | |
| Curriculum integration | Embed within primary care, geriatrics, or internal medicine rotations to avoid extra infrastructure costs. | |
| Moderate resource | Hybrid and digital models | Implement online workshops, virtual patient case studies, and telemedicine role-play exercises. |
| Community-based learning | Partner with community health programmes, caregiver networks, and home-care services for real-world insights. | |
| High resource | Advanced simulations | Utilise full-scale simulation labs with ageing suits, VR, or AI-driven patient cases to enhance realism. |
| Interdisciplinary collaboration | Include input from social workers, occupational therapists, and caregivers in the learning process. | |
| Patient narrative alternatives | Use recorded testimonials, patient-led discussions, or mentorship programmes with long-term care providers. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conte, A.; Jerjes, W. Time Capsule Medicine: A Mixed-Methods Pilot Study on Immersive Simulation for Chronic Disease Education in Medical Students. Clin. Pract. 2025, 15, 78. https://doi.org/10.3390/clinpract15040078
Conte A, Jerjes W. Time Capsule Medicine: A Mixed-Methods Pilot Study on Immersive Simulation for Chronic Disease Education in Medical Students. Clinics and Practice. 2025; 15(4):78. https://doi.org/10.3390/clinpract15040078
Chicago/Turabian StyleConte, Andreas, and Waseem Jerjes. 2025. "Time Capsule Medicine: A Mixed-Methods Pilot Study on Immersive Simulation for Chronic Disease Education in Medical Students" Clinics and Practice 15, no. 4: 78. https://doi.org/10.3390/clinpract15040078
APA StyleConte, A., & Jerjes, W. (2025). Time Capsule Medicine: A Mixed-Methods Pilot Study on Immersive Simulation for Chronic Disease Education in Medical Students. Clinics and Practice, 15(4), 78. https://doi.org/10.3390/clinpract15040078