

Factors Influencing Adherence to Non-Invasive Telemedicine in Heart Failure: A Systematic Review
 , ,
, ,  and
and
Abstract
1. Introduction
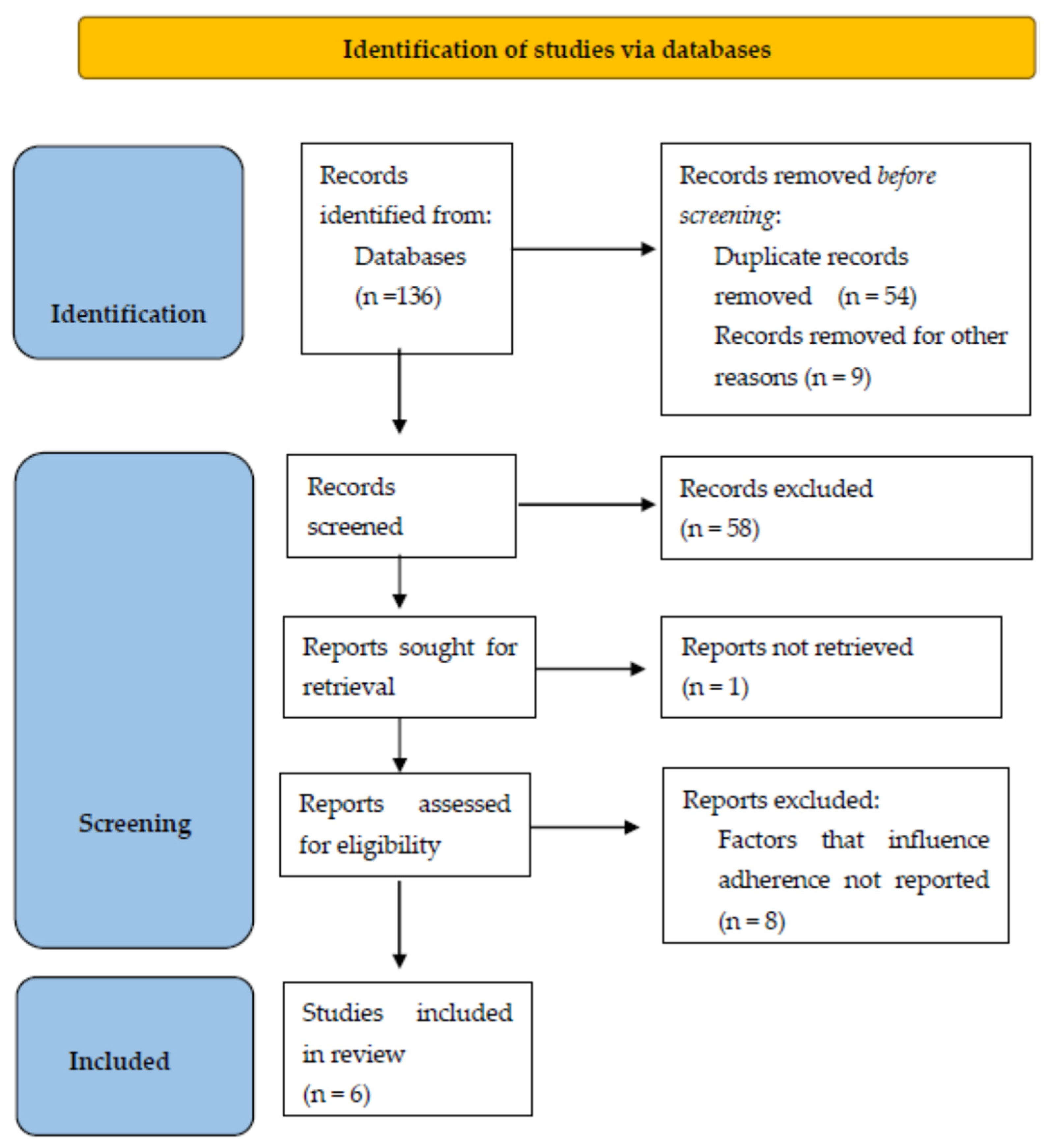
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
3. Results
3.1. Risk of Bias
3.2. Studies Characteristics
3.3. Adherence
3.4. Age
3.5. Sex
3.6. Race
3.7. Place of Residence
3.8. Follow-Up Period
3.9. Number of Recorded Parameters
4. Discussion
4.1. Standardizing Terminology
4.2. Improving Compliance
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics-2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [PubMed]
- Groenewegen, A.; Rutten, F.H.; Mosterd, A.; Hoes, A.W. Epidemiology of heart failure. Eur. J. Heart Fail. 2020, 22, 1342–1356. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. AHA statistical update: Heart disease and stroke statistics—2019 update. A report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESCGuidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA)of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar]
- Feltner, C.; Jones, C.D.; Cene, C.W.; Zheng, Z.J.; Sueta, C.A.; Coker-Schwimmer, E.J.; Arvanitis, M.; Lohr, K.N.; Middleton, J.C.; Jonas, D.E. Transitional care interventions to prevent readmissions for persons with heart failure: A systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 774–784. [Google Scholar] [CrossRef] [PubMed]
- Iellamo, F.; Sposato, B.; Volterrani, M. Telemonitoring for the Management of Patients with Heart Failure. Card. Fail. Rev. 2020, 6, e07. [Google Scholar] [CrossRef]
- Schmidt, S.; Schuchert, A.; Krieg, T.; Oeff, M. Home telemonitoring in patients with chronic heart failure: A chance to improve patient care? Dtsch. Arztebl. Int. 2010, 107, 131–138. [Google Scholar]
- Tedeschi, A.; Palazzini, M.; Trimarchi, G.; Conti, N.; Di Spigno, F.; Gentile, P.; D’Angelo, L.; Garascia, A.; Ammirati, E.; Morici, N.; et al. Heart Failure Management through Telehealth: Expanding Care and Connecting Hearts. J. Clin. Med. 2024, 13, 2592. [Google Scholar] [CrossRef]
- Jaarsma, T.; Hill, L.; Bayes-Genis, A.; La Rocca, H.B.; Castiello, T.; Čelutkienė, J.; Marques-Sule, E.; Plymen, C.M.; Piper, S.E.; Riegel, B.; et al. Self-care of heart failure patients: Practical management recommendations from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2021, 23, 157–174. [Google Scholar] [CrossRef]
- Di Lenarda, A.; Casolo, G.; Gulizia, M.M.; Aspromonte, N.; Scalvini, S.; Mortara, A.; Alunni, G.; Ricci, R.P.; Mantovan, R.; Russo, G.; et al. The future of telemedicine for the management of heart failure patients: A Consensus Document of the Italian Association of Hospital Cardiologists (A.N.M.C.O), the Italian Society of Cardiology (S.I.C.) and the Italian Society for Telemedicine and eHealth (Digital S.I.T.). Eur. Heart J. Suppl. 2017, 19, D113–D129. [Google Scholar] [PubMed]
- Lopes, I.; Sousa, F.; Moreira, E.; Cardoso, J. Smartphone-Based Remote Monitoring Solution for Heart Failure Patients. Stud. Health Technol. Inform. 2019, 261, 109–114. [Google Scholar]
- Koehler, J.; Stengel, A.; Hofmann, T.; Wegscheider, K.; Koehler, K.; Sehner, S.; Rose, M.; Deckwart, O.; Anker, S.D.; Koehler, F.; et al. Telemonitoring in patients with chronic heart failure and moderate depressed symptoms: Results of the Telemedical Interventional Monitoring in Heart Failure (TIM-HF) study. Eur. J. Heart Fail. 2021, 23, 186–194. [Google Scholar] [CrossRef]
- Neubeck, L.; Hansen, T.; Jaarsma, T.; Klompstra, L.; Gallagher, R. Delivering healthcare remotely to cardiovascular patients during COVID-19: A rapid review of the evidence. Eur. J. Cardiovasc. Nurs. 2020, 19, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, G.; Marlicz, W.; Koulaouzidis, A. Telemedicine in the Time of COVID-19: Better Late Than Never. Am. J. Gastroenterol. 2021, 116, 1088–1089. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, G.; Charisopoulou, D.; Wojakowski, W.; Koulaouzidis, A.; Marlicz, W.; Jadczyk, T. Telemedicine in cardiology in the time of coronavirus disease 2019: A friend that everybody needs. Pol. Arch. Intern. Med. 2020, 130, 559–561. [Google Scholar] [CrossRef]
- Planinc, I.; Milicic, D.; Cikes, M. Telemonitoring in Heart Failure Management. Card. Fail. Rev. 2020, 6, e06. [Google Scholar] [CrossRef]
- Marlicz, W.; Koulaouzidis, A.; Charisopoulou, D.; Jankowski, J.; Marlicz, M.; Skonieczna-Zydecka, K.; Krynicka, P.; Loniewski, I.; Samochowiec, J.; Rydzewska, G.; et al. Burnout in healthcare—the Emperor’s New Clothes. Prz. Gastroenterol. 2023, 18, 274–280. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. CHAMPION Trial Study Group. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomized controlled trial. Lancet 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Lindenfeld, J.; Abraham, W.T.; Maisel, A.; Zile, M.; Smart, F.; Costanzo, M.R.; Mehra, M.R.; Ducharme, A.; Sears, S.F.; Desai, A.S.; et al. Hemodynamic-GUIDEd management of Heart Failure (GUIDE-HF). Am. Heart J. 2019, 214, 18–27. [Google Scholar] [CrossRef]
- Angermann, C.E.; Assmus, B.; Anker, S.D.; Asselbergs, F.W.; Brachmann, J.; Brett, M.E.; Brugts, J.J.; Ertl, G.; Ginn, G.; Hilker, L.; et al. MEMS-HF Investigators. Pulmonary artery pressure-guided therapy in ambulatory patients with symptomatic heart failure: The CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur. J. Heart Fail. 2020, 22, 1891–1901. [Google Scholar] [CrossRef]
- Veenis, J.F.; Brugts, J.J. Remote monitoring of chronic heart failure patients: Invasive versus non-invasive tools for optimising patient management. Neth. Heart J. 2020, 28, 3–13. [Google Scholar] [CrossRef]
- Halawa, A.; Enezate, T.; Flaker, G. Device monitoring in heart failure management: Outcomes based on a systematic review and meta-analysis. Cardiovasc. Diagn. Ther. 2019, 9, 386–393. [Google Scholar] [CrossRef]
- Alotaibi, S.; Hernandez-Montfort, J.; Ali, O.E.; El-Chilali, K.; Perez, B.A. Remote monitoring of implantable cardiac devices in heart failure patients: A systematic review and meta-analysis of randomized controlled trials. Heart Fail. Rev. 2020, 25, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Ahmed, S.; Grapsa, J. Apps and Online Platforms for Patients with Heart Failure. Card. Fail. Rev. 2020, 6, e14. [Google Scholar] [CrossRef] [PubMed]
- Silva-Cardoso, J.; Juanatey, J.R.G.; Comin-Colet, J.; Sousa, J.M.; Cavalheiro, A.; Moreira, E. The Future of Telemedicine in the Management of Heart Failure Patients. Card. Fail. Rev. 2021, 7, e11. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, G.; Barrett, D.; Mohee, K.; Clark, A.L. Telemonitoring in subjects with newly diagnosed heart failure with reduced ejection fraction: From clinical research to everyday practice. J. Telemed. Telecare 2019, 25, 167–171. [Google Scholar] [CrossRef]
- Stevenson, L.W.; Ross, H.J.; Rathman, L.D.; Boehmer, J.P. Remote Monitoring for Heart Failure Management at Home. J. Am. Coll. Cardiol. 2023, 81, 2272–2291. [Google Scholar] [CrossRef]
- Faragli, A.; Abawi, D.; Quinn, C.; Cvetkovic, M.; Schlabs, T.; Tahirovic, E.; Düngen, H.D.; Pieske, B.; Kelle, S.; Edelmann, F.; et al. The role of non-invasive devices for the telemonitoring of heart failure patients. Heart Fail. Rev. 2021, 26, 1063–1080. [Google Scholar] [CrossRef]
- Wańczura, P.; Aebisher, D.; Wiśniowski, M.; Kos, M.; Bukowski, H.; Hołownia-Voloskova, M.; Przybylski, A. Telemedical Intervention and Its Effect on Quality of Life in Chronic Heart Failure Patients: The Results from the Telemedicine and e-Health Solution Pilot Program. J. Clin. Med. 2024, 13, 2604. [Google Scholar] [CrossRef]
- Kinast, B.; Lutz, M.; Schreiweis, B. Telemonitoring of Real-World Health Data in Cardiology: A Systematic Review. Int. J. Environ. Res. Public. Health 2021, 18, 9070. [Google Scholar] [CrossRef] [PubMed]
- Iakovidis, D.K.; Douska, D.; Barba, E.; Koulaouzidis, G. Wavelet-based signal analysis for heart failure hospitalization prediction. Stud. Health Technol. Inform. 2016, 224, 21–26. [Google Scholar] [PubMed]
- Joshi, R.; Gyllensten, I.C. Changes in Daily Measures of Blood Pressure and Heart Rate Improve Weight-Based Detection of Heart Failure Deterioration in Patients on Telemonitoring. IEEE J. Biomed. Health Inform. 2019, 23, 1041–1048. [Google Scholar] [CrossRef]
- Henriques, J.; Carvalho, P.; Paredes, S.; Rocha, T.; Habetha, J.; Antunes, M.; Morais, J. Prediction of Heart Failure Decompensation Events by Trend Analysis of Telemonitoring Data. IEEE J. Biomed. Health Inform. 2015, 19, 1757–1769. [Google Scholar] [CrossRef]
- Koulaouzidis, G.; Iakovidis, D.K.; Clark, A.L. Telemonitoring predicts in advance heart failure admissions. Int. J. Cardiol. 2016, 216, 78–84. [Google Scholar] [CrossRef]
- Inglis, S.C.; Clark, R.A.; Dierckx, R.; Prieto-Merino, D.; Cleland, J.G. Structured telephone support or non-invasive telemonitoring for patients with heart failure. Cochrane Database Syst. Rev. 2015, 2015, CD007228. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Wu, T.H.; Wu, Y.C.; Han, C.C. Bluetooth-Based Healthcare Information and Medical Resource Management System. Sensors 2023, 23, 5389. [Google Scholar] [CrossRef]
- Brahmbhatt, D.H.; Cowie, M.R. Remote Management of Heart Failure: An Overview of Telemonitoring Technologies. Card. Fail. Rev. 2019, 5, 86–92. [Google Scholar] [CrossRef]
- Sousa, C.; Leite, S.; Lagido, R.; Ferreira, L.; Silva-Cardoso, J.; Maciel, M.J. Telemonitoring in heart failure: A state-of-the-art review. Rev. Port. Cardiol. 2014, 33, 229–239. [Google Scholar] [CrossRef]
- Fedson, S.; Bozkurt, B. Telehealth in Heart Failure. Heart Fail. Clin. 2022, 18, 213–221. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Deka, P.; Pozehl, B.; Williams, M.A.; Yates, B. Adherence to recommended exercise guidelines in patients with heart failure. Heart Fail. Rev. 2017, 22, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.; Keeling, P. Compliance with Telemonitoring in Heart Failure. Are Study Findings Representative of Reality? A Narrative Literature Review. Telemed. E-Health J. 2022, 28, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Prescher, S.; Winkler, S.; Riehle, L.; Hiddemann, M.; Moeller, V.; Collins, C.; Deckwart, O.; Spethmann, S. Patient reported experience and adherence to remote patient management in chronic heart failure patients: A posthoc analysis of the TIM-HF2 trial. Eur. J. Cardiovasc. Nurs. 2023, 22, 245–253. [Google Scholar] [CrossRef]
- Galinier, M.; Roubille, F.; Berdague, P.; Brierre, G.; Cantie, P.; Dary, P.; Ferradou, J.; Fondard, O.; Labarre, J.P.; Mansourati, J.; et al. Telemonitoring versus standard care in heart failure: A randomized multicentre trial. Eur. J. Heart Fail. 2020, 22, 985–994. [Google Scholar] [CrossRef]
- Haynes, S.C.; Tancredi, D.J.; Tong, K.; Hoch, J.S.; Ong, M.K.; Ganiats, T.G.; Evangelista, L.S.; Black, J.T.; Auerbach, A.; Romano, P.S.; et al. Association of adherence to weight telemonitoring with health care use and death: A secondary analysis of a randomized clinical trial. JAMA Netw. Open 2020, 3, e2010174. [Google Scholar] [CrossRef]
- Ding, H.; Jayasena, R.; Chen, S.H.; Maiorana, A.; Dowling, A.; Layland, J.; Good, N.; Karunanithi, M.; Edwards, I. The effects of telemonitoring on patient compliance with self-management recommendations and outcomes of the innovative telemonitoring enhanced care program for chronic heart failure: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e17559. [Google Scholar] [CrossRef]
- On behalf of the HOMES-HF study investigators; Kotooka, N.; Kittaka, M.; Nagashima, K.; Asaka, M.; Kinugasa, Y.; Nochioka, K.; Mizuno, A.; Nagatomo, D.; Mine, D.; et al. The first multicenter, randomized, controlled trial of home telemonitoring for Japanese patients with heart failure: Home telemonitoring study for patients with heart failure (HOMES-HF). Heart Vessel. 2018, 33, 866–876. [Google Scholar] [CrossRef]
- Pekmezaris, R.; Nouryan, C.N.; Schwartz, R.; Castillo, S.; Makaryus, A.N.; Ahern, D.; Akerman, M.B.; Lesser, M.L.; Bauer, L.; Murray, L.; et al. A randomized controlled trial comparing telehealth self-management to standard outpatient management in underserved black and Hispanic patients living with heart failure. Telemed. J. E Health 2019, 25, 917–925. [Google Scholar] [CrossRef]
- NHFA CSANZ Heart Failure Guidelines Working Group; Atherton, J.J.; Sindone, A.; De Pasquale, C.G.; Driscoll, A.; MacDonald, P.S.; Hopper, I.; Kistler, P.M.; Briffa, T.; Wong, J.; et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Guidelines for the Prevention, Detection, and Management of Heart Failure in Australia 2018. Heart Lung Circ. 2018, 27, 1123–1208. [Google Scholar] [CrossRef] [PubMed]
- Şahin, E.; Yavuz Veizi, B.G.; Naharci, M.I. Telemedicine interventions for older adults: A systematic review. J. Telemed. Telecare 2024, 30, 305–319. [Google Scholar] [CrossRef] [PubMed]
- Magdalena, M.; Bujnowska-Fedak Grata-Borkowska, U. Use of telemedicine-based care for the aging and elderly: Promises and pitfalls. Smart Homecare Technol. TeleHealth 2015, 3, 91–105. [Google Scholar]
- Ware, P.; Dorai, M.; Ross, H.J.; Cafazzo, J.A.; Laporte, A.; Boodoo, C.; Seto, E. Patient Adherence to a Mobile Phone-Based Heart Failure Telemonitoring Program: A Longitudinal Mixed-Methods Study. JMIR Mhealth Uhealth 2019, 7, e13259. [Google Scholar] [CrossRef]
- Hay, K.; McDougal, L.; Percival, V.; Henry, S.; Klugman, J.; Wurie, H.; Raven, J.; Shabalala, F.; Fielding-Miller, R.; Dey, A.; et al. Gender Equality, Norms, and Health Steering Committee. Disrupting gender norms in health systems: Making the case for change. Lancet 2019, 393, 2535–2549. [Google Scholar] [CrossRef] [PubMed]
- Abd El Mawgod, M.M.; Alshutayli, A.A.; Alanazi, S.M.; Alqahtani, W.N.; Alqahtani, N.A.; Alamri, A.M.; Alshammari, N.Z. Awareness and Perception of Telemedicine Among the General Population in the Central, Northern, and Western Regions of Saudi Arabia. Cureus 2024, 16, e64895. [Google Scholar] [CrossRef]
- Muehlensiepen, F.; Hoffmann, M.J.; Nübel, J.; Ignatyev, Y.; Heinze, M.; Butter, C.; Haase-Fielitz, A. Acceptance of Telemedicine by Specialists and General Practitioners in Cardiology Care: Cross-Sectional Survey Study. JMIR Form. Res. 2024, 8, e49526. [Google Scholar] [CrossRef]
- Muehlensiepen, F.; Petit, P.; Knitza, J.; Welcker, M.; Vuillerme, N. Factors Associated with Telemedicine Use Among German General Practitioners and Rheumatologists: Secondary Analysis of Data from a Nationwide Survey. J. Med. Internet Res. 2022, 24, e40304. [Google Scholar] [CrossRef]
- Hughes, H.A.; Granger, B.B. Racial disparities and the use of technology for self-management in blacks with heart failure: A literature review. Curr. Heart Fail. Rep. 2014, 11, 281–289. [Google Scholar] [CrossRef]
- Franek, J. Self-management support interventions for persons with chronic disease: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2013, 13, 1–60. [Google Scholar]
- Gorst, S.L.; Armitage, C.J.; Brownsell, S.; Hawley, M.S. Home telehealth uptake and continued use among heart failure and chronic obstructive pulmonary disease patients: A systematic review. Ann. Behav. Med. 2014, 48, 323–336. [Google Scholar] [CrossRef] [PubMed]
- Goorts, K.; Dizon, J.; Milanese, S. The effectiveness of implementation strategies for promoting evidence informed interventions in allied healthcare: A systematic review. BMC Health Serv. Res. 2021, 21, 241. [Google Scholar] [CrossRef] [PubMed]
- Edgman-Levitan, S.; Schoenbaum, S.C. Patient-centered care: Achieving higher quality by designing care through the patient’s eyes. Isr. J. Health Policy Res. 2021, 10, 21. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | D1 | D2 | D3 | D4 | D5 | Overall |
|---|---|---|---|---|---|---|
| TIM-HF2 [45] |  |  |  |  |  |  |
| OSICAT [46] |  |  |  |  |  |  |
| BEAT-HF [47] |  |  |  |  |  |  |
| ITEC-CHF [48] |  |  |  |  |  |  |
| HOMES-HF [49] |  |  |  |  |  |  |
| Pekmezaris et al. [50] |  |  |  |  |  |  |
 low risk;
low risk;  some concerns.
some concerns.| Study | Study Type | Country/Centers | Duration | Sample Size | Age (Years) | Males (%) | Ethnicity (%) | HF Categories |
|---|---|---|---|---|---|---|---|---|
| TIM-HF2 [45] | Prospective, RCT (1:1) | Germany; 200 | 12 months | 1571 (796 TM, 775 UC) | 70 ± 10 | 70 | n/a | HFpEF 25% HFmEF 30% HFrEF 45% |
| OSICAT [46] | Prospective, RCT (1:1) | France; 13 | 18 months | 990 (507 TM, 483 UC) | 69.9 ± 12.4 | 72.3 | n/a | HFpEF 21.7% HFmEF 19.8% HFrEF 58.5% |
| BEAT-HF [47] | Prospective, RCT (1:1) | USA; 6 | 6 months | 1437 (722 TM, 715 UC) | 70.9 ± 14.1 | 53.8 | White 50.7 Black 23.2 Hispanic 13.2 | EF (mean) 42.7 |
| ITEC-CHF [48] | Prospective, RCT (1:1) | Australia; 2 | 6 months | 184 (91 TM, 93 UC) | 70.1 ± 12.3 | 76.6 | n/a | HFrEF 100% |
| HOMES-HF [49] | Prospective, RCT (1:1) | Japan; 27 | 12 months | 181 (90 TM, 91 UC) | 67.1 ± 12.8 | 57 | Japanese 100 | EF (mean ± SD) 40.5 ± 11.4 |
| Pekmezaris et al. [50] | Prospective, RCT (1:1) | USA; 1 | 90 days | 104 (46 TM, 58 UC) | 59.9 ± 15.1 | 59 | Black 69 Hispanic 31 | HFpEF 29% HFmEF 10% HFrEF 61% |
| Study | Inclusion Criteria | Data Transmitted | Intervention | Adherence |
|---|---|---|---|---|
| TIM-HF2 [45] | LVEF ≤ 45%, or if >45% treated with oral diuretics; NYHA II or III; inpatient for HF within 12 last months | Weight, BP, ECG, and self-rated health status | Physician-led medical support for 24/7 | The ratio between the number of days with measurements performed and the number of days with measurements possible |
| OSICAT [46] | Inpatient for HF within 12 months ago | Weight and eight symptom questions | Structured telephone support and nurse-led collaborative care | The ratio of the number of days with body weight measurement divided by the effective days * |
| BEAT-HF [47] | Older adults being inpatients for HF during recruitment | Weight | Structured telephone support | Count of adherence days from 0 (no transmission) to 7 (daily transmission) in event-free weeks |
| ITEC-CHF [48] | EF ≤ 40% | Weight | Structured telephone support and nurse-led collaborative care | Monitoring days per/180 days × 7 days/week |
| HOMES-HF [49] | NYHA II–III; admission for HF within 30 days of enrolment | BP, HR, weight, and body composition | Nurse-led collaborative care | Monitoring days/ days that measurements should be performed in a month × 100% |
| Pekmezaris et al. [50] | NYHA I–III | BP, oxygen saturation rate, weight, and HR. | Structured telephone support and nurse-led collaborative care | Low: <10 uploads over 90 days High: ≥ 10 uploads over 90 days |
| ADHERENCE | |||||
|---|---|---|---|---|---|
| 3 Months | 6 Months | 9 Months | 12 Months | 18 Months | |
| TIM-HF2 [45] | >85% | >85% | >85% | >85% | |
| OSICAT [46] | 50.4 ± 31.4 | 74 ± 35.3 | 69.8 ± 36 | 68.8 ± 36.8 | 65.7 ± 37.6 |
| BEAT-HF [47] | 69% | 53.3% | - | - | - |
| ITEC-CHF [48] | - | 97% with ≥4 uploads/ week | - | - | - |
| HOMES-HF [49] | 96.2% | 90.4% | 88.5% | 90.9% | - |
| Pekmezaris et al. [50] | 50% with <10 uploads | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koulaouzidis, G.; Tsigkriki, L.; Grammenos, O.; Iliopoulou, S.; Kalaitzoglou, M.; Theodorou, P.; Bostanitis, I.; Skonieczna-Żydecka, K.; Charisopoulou, D. Factors Influencing Adherence to Non-Invasive Telemedicine in Heart Failure: A Systematic Review. Clin. Pract. 2025, 15, 79. https://doi.org/10.3390/clinpract15040079
Koulaouzidis G, Tsigkriki L, Grammenos O, Iliopoulou S, Kalaitzoglou M, Theodorou P, Bostanitis I, Skonieczna-Żydecka K, Charisopoulou D. Factors Influencing Adherence to Non-Invasive Telemedicine in Heart Failure: A Systematic Review. Clinics and Practice. 2025; 15(4):79. https://doi.org/10.3390/clinpract15040079
Chicago/Turabian StyleKoulaouzidis, George, Lamprini Tsigkriki, Orestis Grammenos, Sotiria Iliopoulou, Maria Kalaitzoglou, Panagiotis Theodorou, Ioannis Bostanitis, Karolina Skonieczna-Żydecka, and Dafni Charisopoulou. 2025. "Factors Influencing Adherence to Non-Invasive Telemedicine in Heart Failure: A Systematic Review" Clinics and Practice 15, no. 4: 79. https://doi.org/10.3390/clinpract15040079
APA StyleKoulaouzidis, G., Tsigkriki, L., Grammenos, O., Iliopoulou, S., Kalaitzoglou, M., Theodorou, P., Bostanitis, I., Skonieczna-Żydecka, K., & Charisopoulou, D. (2025). Factors Influencing Adherence to Non-Invasive Telemedicine in Heart Failure: A Systematic Review. Clinics and Practice, 15(4), 79. https://doi.org/10.3390/clinpract15040079