
The Use of Vacuum Devices as Adjuvant Therapy before and after Penile Curvature Surgery in Patients Affected by La Peyronie’s Disease: Results from a Comparative Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
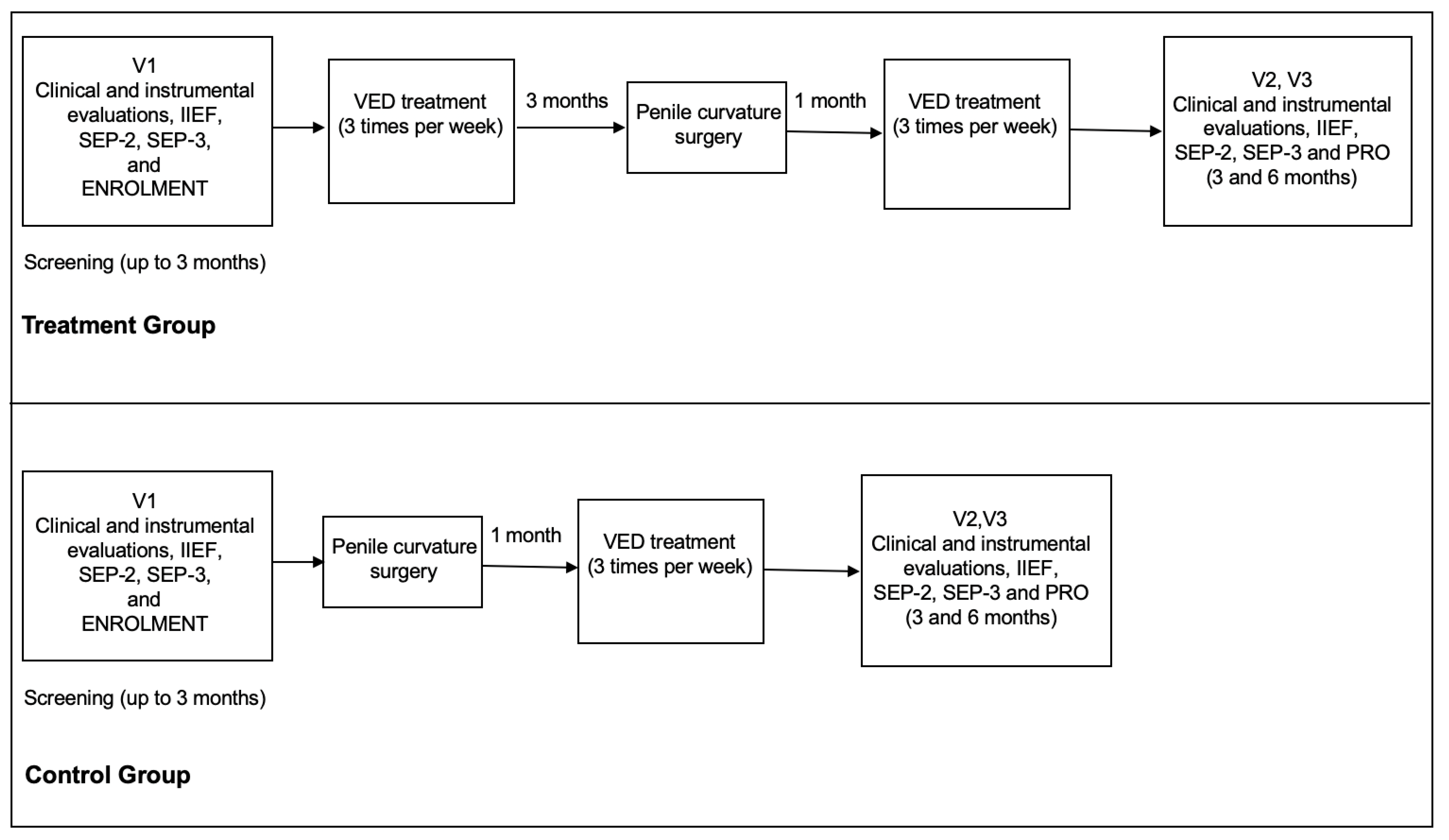
2.1. Study Design and Patient’s Population
2.2. Inclusion and Exclusion Criteria
2.3. Preoperative Assessment and VED Adjuvant Treatment
2.4. Surgical Treatment and Post-Operative Management
2.5. Outcome Measurements
2.6. Questionnaires
2.7. Statistical and Ethical Considerations
3. Results
3.1. Clinical Characteristics of the Study Participants at the Enrolment
3.2. Intra-Operative and Peri-Operative Findings
3.3. Follow-Up Results
4. Discussion
4.1. Main Findings
4.2. Results in the Context of Current Knowledge
4.3. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moisés da Silva, G.V.; Dávila, F.J.; Rosito, T.E.; Martins, F.E. Global Perspective on the Management of Peyronie’s Disease. Front. Reprod. Health 2022, 4, 863844. [Google Scholar] [CrossRef] [PubMed]
- Kadioglu, A.; Dincer, M.; Salabas, E.; Culha, M.G.; Akdere, H.; Cilesiz, N.C. A Population-Based Study of Peyronie’s Disease in Turkey: Prevalence and Related Comorbidities. Sex. Med. 2020, 8, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Stuntz, M.; Perlaky, A.; des Vignes, F.; Kyriakides, T.; Glass, D. The Prevalence of Peyronie’s Disease in the United States: A Population-Based Study. PLoS ONE 2016, 11, e0150157. [Google Scholar] [CrossRef] [PubMed]
- Ainayev, Y.; Zhanbyrbekuly, U.; Gaipov, A.; Suleiman, M.; Kadyrzhanuly, K.; Kissamedenov, N.; Zhaparov, U.; Akhmetov, D.; Khairli, G. Surgical Reconstruction of Penile Curvature due to Peyronie’s Disease by Plaque Incision and Buccal Mucosa Graft. J. Sex. Med. 2021, 18, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, U.; Ilg, M.M.; Cellek, S.; Albersen, M. Pathophysiology and Future Therapeutic Perspectives for Resolving Fibrosis in Peyronie’s Disease. Sex. Med. Rev. 2019, 7, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.; Gillman, M.; Tuckey, J.; La Bianca, S.; Love, C. A clinical pathway for the management of Peyronie’s disease: Integrating clinical guidelines from the International Society of Sexual Medicine, American Urological Association and European Urological Association. BJU Int. 2020, 126 (Suppl. S1), 12–17. [Google Scholar] [CrossRef] [PubMed]
- Broderick, G.A.; McGahan, J.P.; Stone, A.R.; White, R.D. The hemodynamics of vacuum constriction erections: Assessment by color Doppler ultrasound. J. Urol. 1992, 147, 57–61. [Google Scholar] [CrossRef] [PubMed]
- European Association of Urology Guidelines on Sexual and Reproductive Health. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Sexual-and-Reproductive-Health-2022_2022-03-29-084141_megw.pdf (accessed on 3 March 2023).
- Rybak, J.; Papagiannopoulos, D.; Levine, L. A retrospective comparative study of traction therapy vs. no traction following tunica albuginea plication or partial excision and grafting for Peyronie’s disease: Measured lengths and patient perceptions. J. Sex. Med. 2012, 9, 2396–2403. [Google Scholar] [CrossRef] [PubMed]
- Osmonov, D.; Ragheb, A.; Ward, S.; Blecher, G.; Falcone, M.; Soave, A.; Dahlem, R.; van Renterghem, K.; Christopher, N.; Hatzichristodoulou, G.; et al. ESSM Position Statement on Surgical Treatment of Peyronie’s Disease. Sex. Med. 2022, 10, 100459. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Liu, C.; Wang, R. Effect of Penile Traction and Vacuum Erectile Device for Peyronie’s Disease in an Animal Model. J. Sex. Med. 2017, 14, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.W.; Reardon, G.; Sandor, D.W.; Rosen, R.C.; Ferguson, D.M. Validation of stopwatch measurements of erection duration against responses to the sexual encounter profile and international index of erectile Function in patients treated with a phosphodiesterase type 5 inhibitor. J. Sex. Med. 2010, 7, 1147–1159. [Google Scholar] [CrossRef]
- Hellstrom, W.J.G.; Feldman, R.; Rosen, R.C.; Smith, T.; Kaufman, G.; Tursi, J. Bother and distress associated with peyronie’s disease: Validation of the Peyronie’s disease questionnaire. J. Urol. 2013, 190, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Neamatullah, I.; Douglass, M.M.; Lehman, L.W.; Reisner, A.; Villarroel, M.; Long, W.J.; Szolovits, P.; Moody, G.B.; Mark, R.G.; Clifford, G.D. Automated de-identification of free-text medical records. BMC Med. Inform. Decis. Mak. 2008, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Pascual, E.; Manfredi, C.; Torremadé, J.; Ibarra, F.P.; Geli, J.S.; Romero-Otero, J.; García-Baquero, R.; Poblador, A.F.; Barbará, M.R.; Campos-Juanatey, F.; et al. Multicenter Prospective Study of Grafting with Collagen Fleece TachoSil in Patients with Peyronie’s Disease. J. Sex. Med. 2020, 17, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Garaffa, G.; Trost, L.W.; Serefoglu, E.C.; Ralph, D.; Hellstrom, W.J. Understanding the course of Peyronie’s disease. Int. J. Clin. Pract. 2013, 67, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Avant, R.A.; Ziegelmann, M.; Nehra, A.; Alom, M.; Kohler, T.; Trost, L. Penile Traction Therapy and Vacuum Erection Devices in Peyronie’s Disease. Sex. Med. Rev. 2019, 7, 338–348. [Google Scholar] [CrossRef]
- Yuan, J.; Lin, H.; Li, P.; Zhang, R.; Luo, A.; Berardinelli, F.; Dai, Y.; Wang, R. Molecular mechanisms of vacuum therapy in penile rehabilitation: A novel animal study. Eur. Urol. 2010, 58, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Lue, T.F.; El-Sakka, A.I. Lengthening shortened penis caused by Peyronie’s disease using circular venous grafting and daily stretching with a vacuum erection device. J. Urol. 1999, 161, 1141–1144. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Treatment | Control | p | |
|---|---|---|---|
| No. of patients | 20 | 18 | |
| Age (years) | 1 | ||
| Median (IQR †) | 67 (57–74) | 66 (54–75) | |
| Marital status | 0.99 | ||
| Married | 18 (90) | 17 (94.4) | |
| Single | 2 (10) | 1 (5.6) | |
| Duration of disease-time from onset (months) | 0.89 | ||
| Median (IQR †) | 13 (12–22) | 14 (13–21) | |
| Penile curvature | 0.94 | ||
| Angle, degrees (IQR †) | 66 (60–80) | 64 (60–80) | |
| Direction, no. | |||
| dorsal | 13 (65) | 12 (66.6) | |
| lateral | 4 (20) | 5 (27.7) | |
| ventral | 3 (15) | 1 (5.7) | |
| Penile deformity | 0.77 | ||
| Hourglass | 3 (15) | 2 (11.1) | |
| Penile length (mm) | 0.83 | ||
| Median (IQR †) | 113 (110–140) | 115 (110–140) | |
| Plaque size (mm) | 0.94 | ||
| Median (IQR†) | 21 (15–31) | 22 (16–35) | |
| IIEF-15 * | 0.82 | ||
| Median (IQR †) | 24 (22–24) | 22 (22–24) | |
| PDQ ° | 0.75 | ||
| Median (IQR †) | 28 (19–35) | 28 (18–34) | |
| PDQ-Penile Pain | 13 (1–23) | 13 (1–23) | |
| PDQ-Symptom Bother | 10 (5–16) | 9 (4–16) | |
| PDQ-Psychological and Physical Symptoms | 3 (0–20) | 4 (0–20) | |
| SEP-2 § | 0.65 | ||
| Yes | 11 (55) | 9 (50) | |
| SEP-3 § | 0.84 | ||
| Yes | 10 (50) | 9 (50) |
| Treatment | Control | p | |
|---|---|---|---|
| Operative time (min) | 0.98 | ||
| Median (IQR †) | 105 (84–132) | 103 (84–128) | |
| Complete curvature correction | 0.57 | ||
| No. | 19 (95) | 17 (94.4) | |
| Penile length (mm) | 0.41 | ||
| Median (IQR †) | 116 (112–140) | 114 (110–140) | |
| Complications | 0.95 | ||
| Hematoma | 3 (15) | 3 (16.6) | |
| Oedema | 9 (45) | 8 (40) |
| Treatment | Control | p | |
|---|---|---|---|
| VED ° use (regular) | 1 | ||
| No. | 20 (100) | 18 (100) | |
| Patient Reported Outcomes | 0.02 | ||
| Overall satisfaction | 19 (95) | 14 (77.7) | |
| Penile sensitivity | 0.03 | ||
| Normal | 14 (70) | 11 (61.1) | |
| IIEF-15 * pre- | 0.82 | ||
| Median (IQR) | 24 (22–24) | 22 (22–24) | |
| IIEF-15 * post- | 0.02 | ||
| Median (IQR) | 26 (22–24) | 24 (22–24) | |
| p = 0.03 | |||
| SEP-2 § pre- | 0.65 | ||
| Yes | 11 (55) | 9 (50) | |
| SEP-2 § post- | <0.001 | ||
| Yes | 17 (85) | 12 (66.6) | |
| p < 0.001 | |||
| SEP-3 § pre- | 0.84 | ||
| Yes | 11 (55) | 9 (50) | |
| SEP-3 § post- | <0.001 | ||
| Yes | 17 (85) | 13 (72.2) | |
| p < 0.001 | |||
| PDQ ° overall—pre- | 0.75 | ||
| Median (IQR) | 28 (19–35) | 28 (18–34) | |
| PDQ ° overall—post- | 0.03 | ||
| Median (IQR) | 12 (8–20) | 17 (16–28) | |
| p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, T.; Capece, M.; Ceruti, C.; Tiscione, D.; Puglisi, M.; Verze, P.; Gontero, P.; Palmieri, A. The Use of Vacuum Devices as Adjuvant Therapy before and after Penile Curvature Surgery in Patients Affected by La Peyronie’s Disease: Results from a Comparative Study. Clin. Pract. 2023, 13, 1244-1252. https://doi.org/10.3390/clinpract13050112
Cai T, Capece M, Ceruti C, Tiscione D, Puglisi M, Verze P, Gontero P, Palmieri A. The Use of Vacuum Devices as Adjuvant Therapy before and after Penile Curvature Surgery in Patients Affected by La Peyronie’s Disease: Results from a Comparative Study. Clinics and Practice. 2023; 13(5):1244-1252. https://doi.org/10.3390/clinpract13050112
Chicago/Turabian StyleCai, Tommaso, Marco Capece, Carlo Ceruti, Daniele Tiscione, Marco Puglisi, Paolo Verze, Paolo Gontero, and Alessandro Palmieri. 2023. "The Use of Vacuum Devices as Adjuvant Therapy before and after Penile Curvature Surgery in Patients Affected by La Peyronie’s Disease: Results from a Comparative Study" Clinics and Practice 13, no. 5: 1244-1252. https://doi.org/10.3390/clinpract13050112
APA StyleCai, T., Capece, M., Ceruti, C., Tiscione, D., Puglisi, M., Verze, P., Gontero, P., & Palmieri, A. (2023). The Use of Vacuum Devices as Adjuvant Therapy before and after Penile Curvature Surgery in Patients Affected by La Peyronie’s Disease: Results from a Comparative Study. Clinics and Practice, 13(5), 1244-1252. https://doi.org/10.3390/clinpract13050112