
Association of Depression and Anxiety with Cardiac Structural and Functional Characteristics in Heart Failure with Reduced and Mildly Reduced Ejection Fraction
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Cardiac and Lung Ultrasound
2.3. Six-Minute Walking Test and Ankle-Brachial Index Assessment
2.4. Mental Health Status and Quality of Life in Heart Failure
2.5. Laboratory Data
2.6. Statistical Analysis
3. Results
3.1. Study Group Characteristics
3.2. Correlations for GAD-7, PHQ-9, and MLHFQ
3.3. Multivariate Linear Regression Models for PHQ-9 and MLHFQ
4. Discussion
5. Conclusions
Author Contributions
Funding
Limitations
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, E876–E894. [Google Scholar] [CrossRef]
- Sbolli, M.; Fiuzat, M.; Cani, D.; O′Connor, C.M. Depression and heart failure: The lonely comorbidity. Eur. J. Heart Fail. 2020, 22, 2007–2017. [Google Scholar] [CrossRef]
- van Melle, J.P.; de Jonge, P.; Ormel, J.; Crijns, H.; van Veldhuisen, D.J.; Honig, A.; Schene, A.H.; van den Berg, M.P.; Investigators, M.-I. Relationship between left ventricular dysfunction and depression following myocardial infarction: Data from the MIND-IT. Eur. Heart J. 2005, 26, 2650–2656. [Google Scholar] [CrossRef]
- Bagherian-Sararoudi, R.; Gilani, B.; Bahrami Ehsan, H.; Sanei, H. Relationship between left ventricular ejection fraction and depression following myocardial infarction: An original article. ARYA Atheroscler. 2013, 9, 16–21. [Google Scholar]
- Bekfani, T.; Nisser, J.; Derlien, S.; Hamadanchi, A.; Frob, E.; Dannberg, G.; Lichtenauer, M.; Smolenski, U.C.; Lehmann, G.; Mobius-Winkler, S.; et al. Psychosocial factors, mental health, and coordination capacity in patients with heart failure with preserved ejection fraction compared with heart failure with reduced ejection fraction. Esc. Heart Fail. 2021, 8, 3268–3278. [Google Scholar] [CrossRef]
- Fino, P.; Sousa, R.M.; Carvalho, R.; Sousa, N.; Almeida, F.; Pereira, V.H. Cognitive performance is associated with worse prognosis in patients with heart failure with reduced ejection fraction. Esc. Heart Fail. 2020, 7, 3059–3066. [Google Scholar] [CrossRef]
- Zafar, M.U.; Paz-Yepes, M.; Shimbo, D.; Vilahur, G.; Burg, M.M.; Chaplin, W.; Fuster, V.; Davidson, K.W.; Badimon, J.J. Anxiety is a better predictor of platelet reactivity in coronary artery disease patients than depression. Eur. Heart J. 2010, 31, 1573–1582. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kramer, D.G.; Patel, A.R.; Maron, M.S.; Udelson, J.E. Left Ventricular Remodeling in Heart Failure Current Concepts in Clinical Significance and Assessment. JACC-Cardiovasc. Imaging 2011, 4, 98–108. [Google Scholar] [CrossRef]
- White, H.D.; Norris, R.M.; Brown, M.A.; Brandt, P.W.T.; Whitlock, R.M.L.; Wild, C.J. Left-Ventricular End-Systolic Volume as the Major Determinant of Survival after Recovery from Myocardial-Infarction. Circulation 1987, 76, 44–51. [Google Scholar] [CrossRef]
- Kramer, D.G.; Trikalinos, T.A.; Kent, D.M.; Antonopoulos, G.V.; Konstam, M.A.; Udelson, J.E. Quantitative Evaluation of Drug or Device Effects on Ventricular Remodeling as Predictors of Therapeutic Effects on Mortality in Patients With Heart Failure and Reduced Ejection Fraction A Meta-Analytic Approach. J. Am. Coll. Cardiol. 2010, 56, 392–406. [Google Scholar] [CrossRef]
- Selvaraj, S.; Fu, Z.X.; Jones, P.; Kwee, L.C.; Windsor, S.L.; Ilkayeva, O.; Newgard, C.B.; Margulies, K.B.; Husain, M.; Inzucchi, S.E.; et al. Metabolomic Profiling of the Effects of Dapagliflozin in Heart Failure with Reduced Ejection Fraction: DEFINE-HF. Circulation 2022, 146, 808–818. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Mayr, M.; Badimon, J. SGLT2 Inhibitors in Heart Failure: Targeted Metabolomics and Energetic Metabolism. Circulation 2022, 146, 819–821. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Vargas-Delgado, A.P.; Requena-Ibanez, J.A.; Garcia-Ropero, A.; Mancini, D.; Pinney, S.; Macaluso, F.; Sartori, S.; Roque, M.; Sabatel-Perez, F.; et al. Randomized Trial of Empagliflozin in Nondiabetic Patients with Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 243–255. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Requena-Ibanez, J.A.; Santos-Gallego, C.G.; Rodriguez-Cordero, A.; Vargas-Delgado, A.P.; Badimon, J.J. Empagliflozin improves quality of life in nondiabetic HFrEF patients. Sub-analysis of the EMPATROPISM trial. Diabetes Metab. Syndr.-Clin. Res. Rev. 2022, 16, 102417. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1-U170. [Google Scholar] [CrossRef]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsens, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L.; European Assoc Cardiovasc, I. Recommendations for the echocardiographic assessment of native valvular regurgitation: An executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2013, 14, 611–612. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Volpicelli, G.; Mussa, A.; Garofalo, G.; Cardinale, L.; Casoli, G.; Perotto, F.; Fava, C.; Frascisco, M. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am. J. Emerg. Med. 2006, 24, 689–696. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9-Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Bhatt, K.N.; Kalogeropoulos, A.P.; Dunbar, S.B.; Butler, J.; Georgiopoulou, V.V. Depression in heart failure: Can PHQ-9 help? Int. J. Cardiol. 2016, 221, 246–250. [Google Scholar] [CrossRef]
- Flint, K.M.; Fairclough, D.L.; Spertus, J.A.; Bekelman, D.B. Does heart failure-specific health status identify patients with bothersome symptoms, depression, anxiety, and/or poorer spiritual well-being? Eur. Heart J.-Qual. Care Clin. Outcomes 2019, 5, 233–241. [Google Scholar] [CrossRef]
- Rector, T.S.; Tschumperlin, L.K.; Kubo, S.H.; Bank, A.J.; Francis, G.S.; McDonald, K.M.; Cohn, J.N. Clinically Significant Improvements in the Living with Heart-Failure Questionnaire Score as Judged by Patients with Heart-Failure. Qual. Life Res. 1994, 3, 60–61. [Google Scholar]
- Behlouli, H.; Feldman, D.E.; Ducharme, A.; Frenette, M.; Giannetti, N.; Grondin, F.; Michel, C.; Sheppard, R.; Pilote, L. Identifying relative Cut-Off Scores with Neural Networks for Interpretation of the Minnesota Living with Heart Failure Questionnaire. In Proceedings of the Annual International Conference of the IEEE-Engineering-in-Medicine-and-Biology-Society, Minneapolis, MN, USA, 3–6 September 2009; p. 6242. [Google Scholar]
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in heart failure-A meta-analytic review of prevalence, intervention effects, and associations with clinical outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537. [Google Scholar] [CrossRef]
- Sokoreli, I.; Vries, J.J.G.; Pauws, S.C.; Steyerberg, E.W. Depression and anxiety as predictors of mortality among heart failure patients: Systematic review and meta-analysis. Heart Fail. Rev. 2016, 21, 49–63. [Google Scholar] [CrossRef]
- Regan, J.A.; Kitzman, D.W.; Leifer, E.S.; Kraus, W.E.; Fleg, J.L.; Forman, D.E.; Whellan, D.J.; Wojdyla, D.; Parikh, K.; O′onnor, C.M.; et al. Impact of Age on Comorbidities and Outcomes in Heart Failure with Reduced Election Fraction. JACC-Heart Fail. 2019, 7, 1056–1065. [Google Scholar] [CrossRef]
- Sunbul, E.A.; Sunbul, M.; Yanartas, O.; Cengiz, F.; Bozbay, M.; Sari, I.; Gulec, H. Increased Neutrophil/Lymphocyte Ratio in Patients with Depression is Correlated with the Severity of Depression and Cardiovascular Risk Factors. Psychiatry Investig. 2016, 13, 121–126. [Google Scholar] [CrossRef]
- Lin, T.K.; Hsu, B.C.; Li, Y.D.; Chen, C.H.; Lin, J.W.; Chien, C.Y.; Weng, C.Y. Prognostic Value of Anxiety Between Heart Failure with Reduced Ejection Fraction and Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc. 2019, 8, e010739. [Google Scholar] [CrossRef]
- Ceriani, E.; Casazza, G.; Peta, J.; Torzillo, D.; Furlotti, S.; Cogliati, C. Residual congestion and long-term prognosis in acutely decompensated heart failure patients. Intern. Emerg. Med. 2020, 15, 719–724. [Google Scholar] [CrossRef]
- Cascino, T.M.; Kittleson, M.M.; Lala, A.; Stehlik, J.; Palardy, M.; Pamboukian, S.V.; Ewald, G.A.; Mountis, M.M.; Horstmanshof, D.A.; Robinson, S.W.; et al. Comorbid Conditions and Health-Related Quality of Life in Ambulatory Heart Failure Patients REVIVAL (Registry Evaluation of Vital Information for VADs in Ambulatory Life REVIVAL). Circ.-Heart Fail. 2020, 13, e006858. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Babyak, M.A.; O′Connor, C.; Keteyian, S.; Landzberg, J.; Howlett, J.; Kraus, W.; Gottlieb, S.; Blackburn, G.; Swank, A.; et al. Effects of Exercise Training on Depressive Symptoms in Patients With Chronic Heart Failure The HF-ACTION Randomized Trial. JAMA-J. Am. Med. Assoc. 2012, 308, 465–474. [Google Scholar] [CrossRef]
- Jeyanantham, K.; Kotecha, D.; Thanki, D.; Dekker, R.; Lane, D.A. Effects of cognitive behavioural therapy for depression in heart failure patients: A systematic review and meta-analysis. Heart Fail. Rev. 2017, 22, 731–741. [Google Scholar] [CrossRef]
- Angermann, C.E.; Gelbrich, G.; Stork, S.; Gunold, H.; Edelmann, F.; Wachter, R.; Schunkert, H.; Graf, T.; Kindermann, I.; Haass, M.; et al. Effect of Escitalopramon All-Cause Mortality and Hospitalization in Patients with Heart Failure and Depression The MOOD-HF Randomized Clinical Trial. JAMA-J. Am. Med. Assoc. 2016, 315, 2683–2693. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | HF with Impaired EF, n = 43 | HFrEF, n = 29 | HFmrEF, n = 14 | p-Value |
|---|---|---|---|---|
| Basic characteristics, comorbidities | ||||
| Inpatient/outpatient, no. (%) | 22 (51)/21 (49) | 20 (69)/9 (31) | 2 (14)/12 (84) | 0.004 |
| Male/female, no. (%) | 33 (76)/10 (24) | 22 (76)/7 (24) | 11 (78)/3 (22) | 0.895 |
| Age, mean ± SD (min; max), years | 64 ± 10 (40; 86) | 64 ± 10 (40; 86) | 64 ± 10 (43; 78) | 0.859 |
| BMI, mean ± SD, kg/m2 | 28.51 ± 5.55 | 29.26 ± 5.76 | 26.95 ± 4.92 | 0.205 |
| Heart disease, median (IQR), years | 8 (5–15) | 9 (6–16) | 8 (3–11) | 0.174 |
| HF, median (IQR), years | 3 (1–8) | 4 (1–8) | 3 (1–8) | 0.846 |
| NYHA class I/II/III, no. (%) | 4 (9)/28 (65)/11 (26) | 1 (3)/19 (66)/9 (31) | 3 (22)/9 (64)/2 (14) | 0.131 |
| Smoking, no. (%) | 13 (30) | 10 (34) | 3 (22) | 0.493 |
| Hypertension, no. (%) | 24 (56) | 15 (51) | 9 (64) | 0.512 |
| Cardiomyopathy ischemic/non-ischemic, no. (%) | 15 (35)/28 (65) | 13 (45)/16 (55) | 2 (14)/12 (86) | 0.105 |
| Mitral valve regurgitation medium/severe, no. (%) | 11 (26) | 9 (31) | 2 (14) | 0.375 |
| Aortic stenosis medium/severe, no. (%) | 3 (7) | 1 (3) | 2 (14) | 0.566 |
| Tricuspid regurgitation medium/severe, no. (%) | 10 (24) | 7 (24) | 3 (22) | 0.895 |
| AF/AFL, no. (%) | 16 (37) | 11 (38) | 5 (36) | 0.916 |
| PVCs/NSVT, no. (%) | 20 (47) | 13 (45) | 7 (50) | 0.793 |
| ICD/CRT, no. (%) | 2 (5) | 1 (3) | 1 (3) | 0.851 |
| LBBB, no. (%) | 21 (49) | 16 (55) | 5 (36) | 0.307 |
| Type II DM, no. (%) | 8 (19) | 7 (24) | 1 (3) | 0.365 |
| Atherosclerosis 0/1/2/3 territories *, no. (%) | 23 (53)/9 (21)/11 (26)/0 (0) | 12 (41)/6 (21)/11 (38)/0 (0) | 11 (78)/3 (22)/0 (0)/0 (0) | 0.017 |
| Symptomatic PAD, no. (%) | 5 (12) | 4 (14) | 1 (3) | 0.728 |
| ABI, mean ± SD | 1.05 ± 0.24 | 1.03 ± 0.25 | 1.09 ± 0.19 | 0.492 |
| CAD, no. (%) | 8 (19) | 7 (24) | 1 (7) | 0.365 |
| COPD, no. (%) | 9 (21) | 6 (21) | 3 (22) | 0.979 |
| Iron deficiency, no. (%) | 11 (26) | 8 (28) | 3 (22) | 0.751 |
| Anemia, no. (%) | 4 (9) | 3 (10) | 1 (7) | 0.872 |
| Thyroid function 0/1/2 **, no. (%) | 38 (89)/4 (9)/1 (2) | 26 (90)/2 (7)/1 (3) | 12 (86)/2 (14)/0 (0) | 0.862 |
| Ultrasound parameters | ||||
| Lung US profile 0/1, no. (%) | 32 (74)/11 (26) | 19 (66)/10 (34) | 13 (93)/1 (7) | 0.144 |
| LAVI, median (IQR), mL/m2 | 42.51 (33.23–50.64) | 45.4 (39.4–55.09) | 31.99 (28.31–37.95) | 0.0008 |
| E/e’, median (IQR) | 9.8 (7.97–12.4) | 10.15 (8.4–12.8) | 8.85 (6.86–11.65) | 0.139 |
| LVEDVI, mean ± SD, mL/m2 | 94 ± 34 | 106 ± 32 | 67 ± 16 | <0.0001 |
| LVESVI, mean ± SD, mL/m2 | 62 ± 30 | 74 ± 28 | 36 ± 10 | <0.0001 |
| LVEF, mean ± SD, % | 35 ± 9 | 29 ± 6 | 46 ± 3 | <0.0001 |
| LVGLS, mean ± SD, % | −10.58 ± 3.52 | −8.81 ± 2.63 | −14.25 ± 1.91 | <0.0001 |
| SVI, median (IQR), mL/m2 | 31.57 (25.23–40.1) | 27.55 (24.15–31.7) | 38.35 (35.47–45.51) | 0.004 |
| Laboratory variables | ||||
| WBC, mean ± SD, ×1000/mL | 7.43 ± 1.89 | 7.43 ± 2.03 | 7.45 ± 1.62 | 0.973 |
| Neu/lym, median (IQR) | 2.3 (1.89–3.08) | 2.47 (1.96–3.09) | 2.2 (2.08–2.87) | 0.496 |
| Hemoglobin, mean ± SD, g/dL | 14.9 ± 1.83 | 15.03 ± 2.08 | 14.62 ± 1.18 | 0.499 |
| Ferritin, mean ± SD, ng/dL | 185.91 ± 180.26 | 201.12 ± 208.85 | 154.41 ± 97.17 | 0.948 |
| Iron, mean ± SD, μg/dL | 85.95 ± 31.63 | 77.48 ± 28.44 | 103.5 ± 31.62 | 0.015 |
| Cholesterol, mean ± SD, mg/dL | 174.13 ± 47.59 | 175.1 ± 51.17 | 172.14 ± 40.88 | 0.851 |
| HDL-cholesterol, mean ± SD, mg/dL | 43.5 ± 12.6 | 41.98 ± 12.28 | 46.65 ± 13.13 | 0.260 |
| LDL-cholesterol, mean ± SD, mg/dL | 104.39 ± 35.68 | 105.08 ± 37.16 | 102.95 ± 33.69 | 0.857 |
| Triglycerides, median (IQR), mg/dL | 112 (81.5–139) | 112 (83–141) | 105 (79–136) | 0.543 |
| CRP, median (IQR), mg/Dl | 0.34 (0.13–0.71) | 0.35 (0.2–0.75) | 0.25 (0.08–0.38) | 0.233 |
| Fibrinogen, mean ± SD, mg/dL | 394.41 ± 134.16 | 413.55 ± 134.41 | 354.76 ± 129.35 | 0.181 |
| Albumin, median (IQR), g/L | 44.6 (41.65–46.95) | 44.2 (41.6–46) | 45.65 (43.25–47.85) | 0.182 |
| GFR, mean ± SD, mL/min/m2 | 75 ± 18 | 71 ± 17 | 82 ± 17 | 0.082 |
| NT-proBNP, median (IQR), pg/mL | 992.7 (524.4–1733.45) | 1113 (686.6–2664.9) | 602.55 (251.07–1211.37) | 0.015 |
| Treatment | ||||
| Loop diuretic, no. (%) | 33 (76) | 26 (90) | 7 (50) | 0.036 |
| MRA, no. (%) | 38 (89) | 25 (86) | 13 (93) | 0.728 |
| SGLT2i, no. (%) | 26 (60) | 19 (66) | 7 (50) | 0.416 |
| BB, no. (%) | 39 (91) | 27 (93) | 12 (86) | 0.699 |
| ACEI/ARB, no. (%) | 8 (19) | 5 (17) | 3 (22) | 0.832 |
| ARNI, no. (%) | 29 (67) | 19 (66) | 10 (71) | 0.762 |
| Statin and/or ezetimibe, no. (%) | 27 (63) | 19 (66) | 8 (57) | 0.665 |
| Characteristics | HF with Impaired EF, n = 43 | HFrEF, n = 29 | HFmrEF, n = 14 | p-Value |
|---|---|---|---|---|
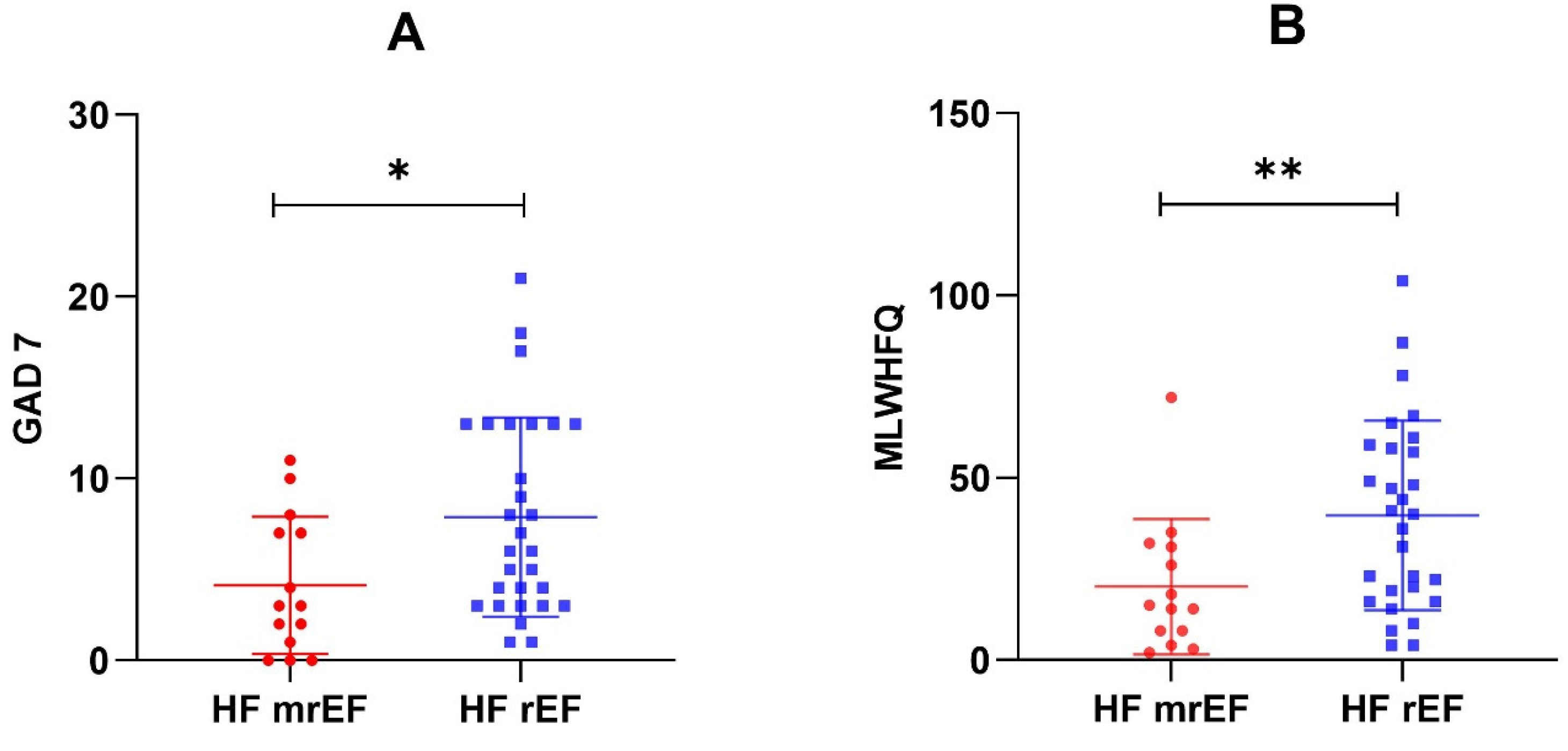
| GAD-7 score, mean ± SD | 7 ± 5 | 8 ± 5 | 4 ± 4 | 0.026 |
| PHQ-9 score, mean ± SD | 8 ± 5 | 9 ± 6 | 6 ± 4 | 0.061 |
| Problem severity 0/1/2/3 *, no. (%) | 10 (24)/31 (72)/1 (2)/1 (2) | 6 (21)/21 (73)/1 (3)/1 (3) | 4 (29)/10 (71)/0 (0)/0 (0) | 0.501 |
| MLHFQ score, mean ± SD | 33 ± 25 | 40 ± 26 | 20 ± 19 | 0.009 |
| Dyspnea, no. (%) | 38 (89) | 27 (93) | 11 (78) | 0.441 |
| Palpitations, no. (%) | 11 (26) | 7 (24) | 4 (29) | 0.823 |
| Peripheral edema, no. (%) | 12 (28) | 11 (38) | 1 (7) | 0.100 |
| Exercise 1/2/3 **, no. (%) | 6 (14)/10 (23)/27 (63) | 6 (21)/8 (28)/15 (51) | 0 (0)/2 (14)/12 (86) | 0.049 |
| 6MWT, median (IQR), m | 405 (252–488) | 405 (250–452) | 445.5 (362.75–523.75) | 0.103 |
| Characteristics | GAD-7 Score | PHQ-9 Score | MLHFQ Score | |||
|---|---|---|---|---|---|---|
| Spearman’s R | p-Value | Spearman’s R | p-Value | Spearman’s R | p-Value | |
| Age | 0.083 | 0.594 | −0.144 | 0.356 | −0.087 | 0.576 |
| NYHA class | 0.306 | 0.045 | 0.411 | 0.006 | 0.444 | 0.002 |
| Peripheral edema | 0.310 | 0.042 | 0.302 | 0.048 | 0.405 | 0.006 |
| Dyspnea | 0.185 | 0.234 | 0.504 | 0.0005 | 0.435 | 0.003 |
| Exercise | −0.140 | 0.367 | −0.139 | 0.370 | −0.333 | 0.029 |
| 6MWT | −0.253 | 0.367 | −0.302 | 0.370 | −0.287 | 0.029 |
| Loop diuretics | 0.051 | 0.744 | 0.289 | 0.059 | 0.355 | 0.019 |
| Lung US profile | 0.131 | 0.400 | 0.194 | 0.212 | 0.244 | 0.113 |
| LVEDVI | 0.102 | 0.515 | 0.121 | 0.438 | 0.381 | 0.011 |
| LVESVI | 0.121 | 0.436 | 0.137 | 0.377 | 0.400 | 0.007 |
| LVEF | −0.215 | 0.166 | −0.259 | 0.093 | −0.467 | 0.001 |
| LVGLS | 0.201 | 0.194 | 0.281 | 0.067 | 0.487 | 0.0009 |
| SVI | −0.308 | 0.430 | −0.321 | 0.043 | −0.292 | 0.041 |
| LAVI | −0.253 | 0.100 | −0.302 | 0.048 | −0.287 | 0.061 |
| E/e’ | 0.111 | 0.478 | −0.001 | 0.992 | 0.164 | 0.290 |
| Neu/lym | −0.010 | 0.944 | 0.028 | 0.857 | −0.002 | 0.987 |
| CRP | −0.050 | 0.748 | 0.210 | 0.175 | 0.127 | 0.414 |
| Fibrinogen | −0.003 | 0.983 | 0.066 | 0.671 | 0.093 | 0.552 |
| Hemoglobin | −0.089 | 0.566 | 0.025 | 0.869 | 0.210 | 0.174 |
| Ferritin | −0.109 | 0.483 | −0.065 | 0.675 | −0.251 | 0.103 |
| Iron | −0.143 | 0.356 | −0.117 | 0.452 | −0.289 | 0.059 |
| Albumin | −0.0006 | 0.996 | −0.171 | 0.272 | −0.320 | 0.036 |
| GFR | −0.223 | 0.150 | −0.166 | 0.286 | −0.425 | 0.004 |
| NT-proBNP | 0.229 | 0.138 | 0.263 | 0.087 | 0.418 | 0.005 |
| Cholesterol | 0.286 | 0.062 | 0.129 | 0.407 | −0.004 | 0.975 |
| HDL-cholesterol | 0.102 | 0.512 | −0.005 | 0.970 | −0.027 | 0.862 |
| LDL-cholesterol | 0.201 | 0.195 | 0.015 | 0.920 | −0.140 | 0.370 |
| Triglycerides | 0.113 | 0.469 | 0.153 | 0.324 | 0.139 | 0.371 |
| (a) | |||||
| Model 1. Summary of regression | |||||
| Variables | B | SD of B | β | t | p-Value |
| Dyspnea | 5.633 | 2.446 | 0.345 | 2.303 | 0.027 |
| Peripheral edema | 2.295 | 1.930 | 0.197 | 1.189 | 0.242 |
| LAVI | −0.008 | 0.006 | −0.192 | −1.240 | 0.223 |
| LVGLS | 0.122 | 0.281 | 0.081 | 0.432 | 0.668 |
| SVI | 0.012 | 0.076 | 0.024 | 0.157 | 0.876 |
| (b) | |||||
| Model 2. Summary of regression | |||||
| Variables | B | SD of B | β | t | p-Value |
| Dyspnea | 24.042 | 11.339 | 0.308 | 2.120 | 0.041 |
| LAVI | −0.053 | 0.032 | −0.273 | −1.664 | 0.104 |
| LVEDVI | 0.590 | 0.523 | 0.781 | 1.128 | 0.267 |
| LVESVI | −0.549 | 0.706 | −0.652 | −0.778 | 0.442 |
| LVEF | −0.624 | 0.897 | −0.225 | −0.695 | 0.491 |
| Model 3. Summary of regression | |||||
| Variables | B | SD of B | β | t | p-Value |
| Dyspnea | 23.290 | 11.335 | 0.298 | 2.055 | 0.047 |
| Peripheral edema | 14.346 | 9.377 | 0.257 | 1.530 | 0.135 |
| Exercise | −9.366 | 5.354 | −0.272 | −1.749 | 0.089 |
| LVESVI | 0.192 | 0.201 | 0.227 | 0.953 | 0.347 |
| LVEF | 0.221 | 0.810 | 0.080 | 0.273 | 0.787 |
| Albumin | −0.147 | 0.984 | −0.023 | −0.149 | 0.882 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabo, T.M.; Nagy, E.E.; Kirchmaier, Á.; Heidenhoffer, E.; Gábor-Kelemen, H.-L.; Frăsineanu, M.; Frigy, A. Association of Depression and Anxiety with Cardiac Structural and Functional Characteristics in Heart Failure with Reduced and Mildly Reduced Ejection Fraction. Clin. Pract. 2023, 13, 398-409. https://doi.org/10.3390/clinpract13020036
Szabo TM, Nagy EE, Kirchmaier Á, Heidenhoffer E, Gábor-Kelemen H-L, Frăsineanu M, Frigy A. Association of Depression and Anxiety with Cardiac Structural and Functional Characteristics in Heart Failure with Reduced and Mildly Reduced Ejection Fraction. Clinics and Practice. 2023; 13(2):398-409. https://doi.org/10.3390/clinpract13020036
Chicago/Turabian StyleSzabo, Timea Magdolna, Előd Ernő Nagy, Ádám Kirchmaier, Erhard Heidenhoffer, Hunor-László Gábor-Kelemen, Marius Frăsineanu, and Attila Frigy. 2023. "Association of Depression and Anxiety with Cardiac Structural and Functional Characteristics in Heart Failure with Reduced and Mildly Reduced Ejection Fraction" Clinics and Practice 13, no. 2: 398-409. https://doi.org/10.3390/clinpract13020036
APA StyleSzabo, T. M., Nagy, E. E., Kirchmaier, Á., Heidenhoffer, E., Gábor-Kelemen, H.-L., Frăsineanu, M., & Frigy, A. (2023). Association of Depression and Anxiety with Cardiac Structural and Functional Characteristics in Heart Failure with Reduced and Mildly Reduced Ejection Fraction. Clinics and Practice, 13(2), 398-409. https://doi.org/10.3390/clinpract13020036