
Atypically Protracted Course of Liver Involvement in Kawasaki Disease. Case Report and Literature Review

 ,
,
Abstract
:1. Introduction
2. Case Report
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tremoulet, A.H.; Jain, S.; Chandrasekar, D.; Sun, X.; Sato, Y.; Burns, J.C. Evolution of Laboratory Values in Patients with Kawasaki Disease. Pediatr. Infect. Dis. J. 2011, 30, 1022–1026. [Google Scholar] [CrossRef] [Green Version]
- Eladawy, M.; Dominguez, S.R.; Anderson, M.S.; Glodé, M.P. Abnormal liver panel in acute Kawasaki disease. Pediatr. Infect. Dis. J. 2011, 30, 141–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Pahl, E. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association [published correction appears in Circulation. 2019, 140, e181–e184]. Circulation 2017, 135, e927–e999. [Google Scholar] [PubMed]
- Makino, N.; Nakamura, Y.; Yashiro, M.; Ae, R.; Tsuboi, S.; Aoyama, Y.; Yanagawa, H. Descriptive epidemiology of Kawasaki disease in Japan, 2011-2012: From the results of the 22nd nationwide survey. J. Epidemiol. 2015, 25, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasiak, A.; Smolewska, E. Retrospective study of the course, treatment and long-term follow-up of Kawasaki disease: A single-center experience from Poland. Rheumatol. Int. 2019, 39, 1069–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, M.; Oh, M.S.; Oh, S.C.; Kang, K.S. Distribution of Diseases Causing Liver Function Test Abnormality in Children and Natural Recovery Time of the Abnormal Liver Function. J. Korean Med. Sci. 2016, 31, 1784–1789. [Google Scholar] [CrossRef]
- Keeling, I.M.; Beran, E.; Dapunt, O.E. Kawasaki disease and hepatobiliary involvement: Report of two cases. Ital. J. Pediatr. 2016, 42, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, Y.; Fukaya, T.; Yamaura, Y.; Tsujiguchi, R.; Muratani, H.; Shimaya, M. Implications of hepatic dysfunction in Kawasaki disease: Time-related changes in aspartate aminotransferase, alanine aminotransferase, total bilirubin, and C-reactive protein levels. Pediatr. Investig. 2019, 3, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Rohani, P.; Imanzadeh, F.; Sayyari, A.; Aghdam, M.K.; Shiari, R. Persistent elevation of aspartate aminotransferase in a child after incomplete Kawasaki disease: A case report and literature review. BMC Pediatr. 2020, 20, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.-M.; Du, Z.-D.; Fu, P.-P. Clinical features of recurrent Kawasaki disease and its risk factors. Eur. J. Nucl. Med. Mol. Imaging 2013, 172, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Yin, W.; Wang, R.; Sun, D.; He, X.; Ding, Y. The prognostic role of abnormal liver function in IVIG unresponsiveness in Kawasaki disease: A meta-analysis. Inflamm. Res. 2015, 65, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.Y.; Kim, J.Y.; Choi, E.Y.; Choi, J.Y.; Yang, H.R. Hepatobiliary risk factors for clinical outcome of Kawasaki disease in children. BMC Pediatr. 2014, 14, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; Ikeda, K.; Hamaoka, K. Aetiological Significance of Infectious Stimuli in Kawasaki Disease. Front. Pediatr. 2019, 7, 244. [Google Scholar] [CrossRef] [PubMed]
- Rosencrantz, R.A.; Huang, T.; Sonke, P.Y.; Tewari, D.; Chander, P.N. Autoimmune sclerosing cholangitis: An atypical association with Kawasaki disease. Hepatology 2016, 64, 2253–2256. [Google Scholar] [CrossRef] [PubMed]
- Vajro, P.; Maddaluno, S.; Veropalumbo, C. Persistent hypertransaminasemia in asymptomatic children: A stepwise approach. World J. Gastroenterol. 2013, 19, 2740–2751. [Google Scholar] [CrossRef] [PubMed]
- Colantonio, D.A.; Kyriakopoulou, L.; Chan, M.K.; Daly, C.H.; Brinc, D.; Venner, A.A.; Pasic, M.D.; Armbruster, D.; Adeli, K. Closing the Gaps in Pediatric Laboratory Reference Intervals: A CALIPER Database of 40 Biochemical Markers in a Healthy and Multiethnic Population of Children. Clin. Chem. 2012, 58, 854–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aithal, G.P.; Day, C.P. Nonsteroidal Anti-Inflammatory Drug–Induced Hepatotoxicity. Clin. Liver Dis. 2007, 11, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Mammadov, G.; Liu, H.H.; Chen, W.X.; Fan, G.Z.; Li, R.X.; Liu, F.F.; Samadli, S.; Wang, J.J.; Wu, Y.F.; Luo, H.H.; et al. Hepatic dysfunction secondary to Kawasaki disease: Characteristics, etiology and predictive role in coronary artery abnormalities. Clin. Exp. Med. 2020, 20, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, A.; De Jacobis, I.T.; Rigante, D.; Rimini, A.; Malorni, W.; Corsello, G.; Bossi, G.; Buonuomo, S.; Cardinale, F.; Cortis, E.; et al. Kawasaki disease: Guidelines of the Italian Society of Pediatrics, part I—definition, epidemiology, etiopathogenesis, clinical expression and management of the acute phase. Ital. J. Pediatr. 2018, 44, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesi, A.; De Jacobis, I.T.; Rigante, D.; Rimini, A.; Malorni, W.; Corsello, G.; Villani, A. Kawasaki disease: Guidelines of Italian Society of Pediatrics, part II—treatment of resistant forms and cardiovascular complications, follow-up, lifestyle and prevention of cardiovascular risks. Ital. J. Pediatr. 2018, 44, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundel, R. Kawasaki Disease: Initial Treatment and Prognosis. 2020. Available online: https://www.uptodate.com/contents/kawasaki-disease-initial-treatment-and-prognosis. (accessed on 30 June 2021).

{kind=link}
| Author | Case Report/Case Series | Transaminases Values at Diagnosis | Recovery Time from Onset | Treatment with Acetylsalicylic Acid | ||
|---|---|---|---|---|---|---|
| N; Gender; Age | AST IU/L | ALT IU/L | AST IU/L | ALT IU/L | ||
| Jang 2016 [6] | 63 patients 2.3 ± 1.7 years | >50 | >50 | 7 days (median); range 2–99 days | NR | |
| Keeling 2016 [7] | 1 F 12 years | 17 | 42 | 4 months | 4 months | 500 mg three times a day during 10-days hospitalization and continued after discharge |
| Tomita 2019 [8] | 199/381 patients (52.2%) 97 F–102 M 27.2 ± 22.5 months | NR | (I) ALT ≥ 40 on admission | AST, peaked on days 1–3 and tended to exhibit recovery on the 4th day of illness | ALT began to normalize on the 6th day of illness | 37/199 patients (18.6%) received aspirin at doses of 10–30 mg/kg/day |
| 52/381patients (13.6%) 16 F–36 M 20.9 ± 25.6 months | NR | (II) ALT ≥ 40 at some point after admission | AST, peaked on 11th day and tended to exhibit recovery on 15th–17th day of illness | ALT decreased on 15th–17th days of illness | 10/52 patients (19.2%) received aspirin at doses of 10–30 mg/kg/day | |
| Rohani 2020 [9] | 1 M 16 months | 351 | 40 | Persistent elevation after 9 months (Macro-AST) | 2 weeks | 35 mg/kg/day divided q6h for 48 h from diagnosis and reduced after 36 h to 3 mg/kg once daily until 6 wk after illness onset |
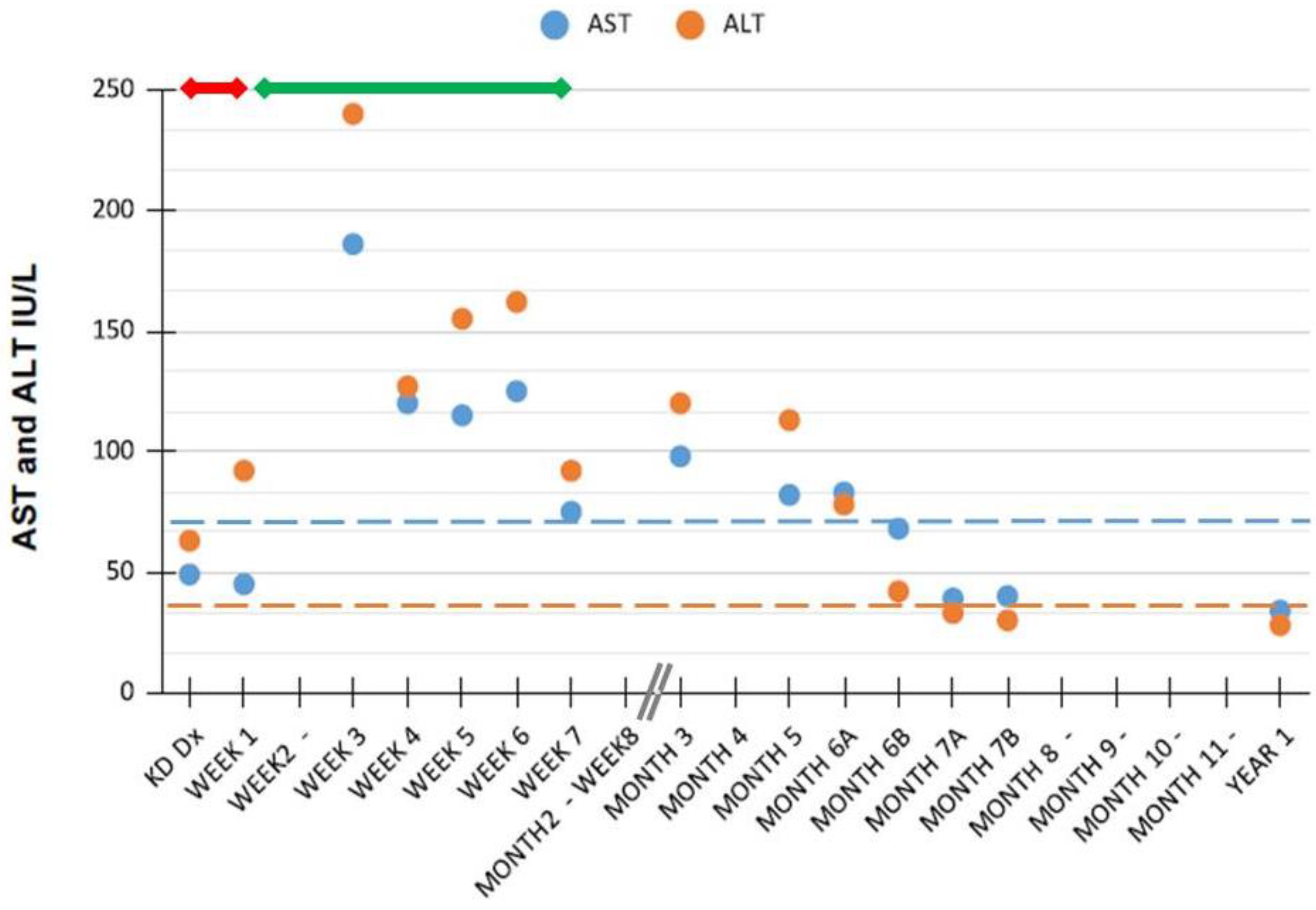
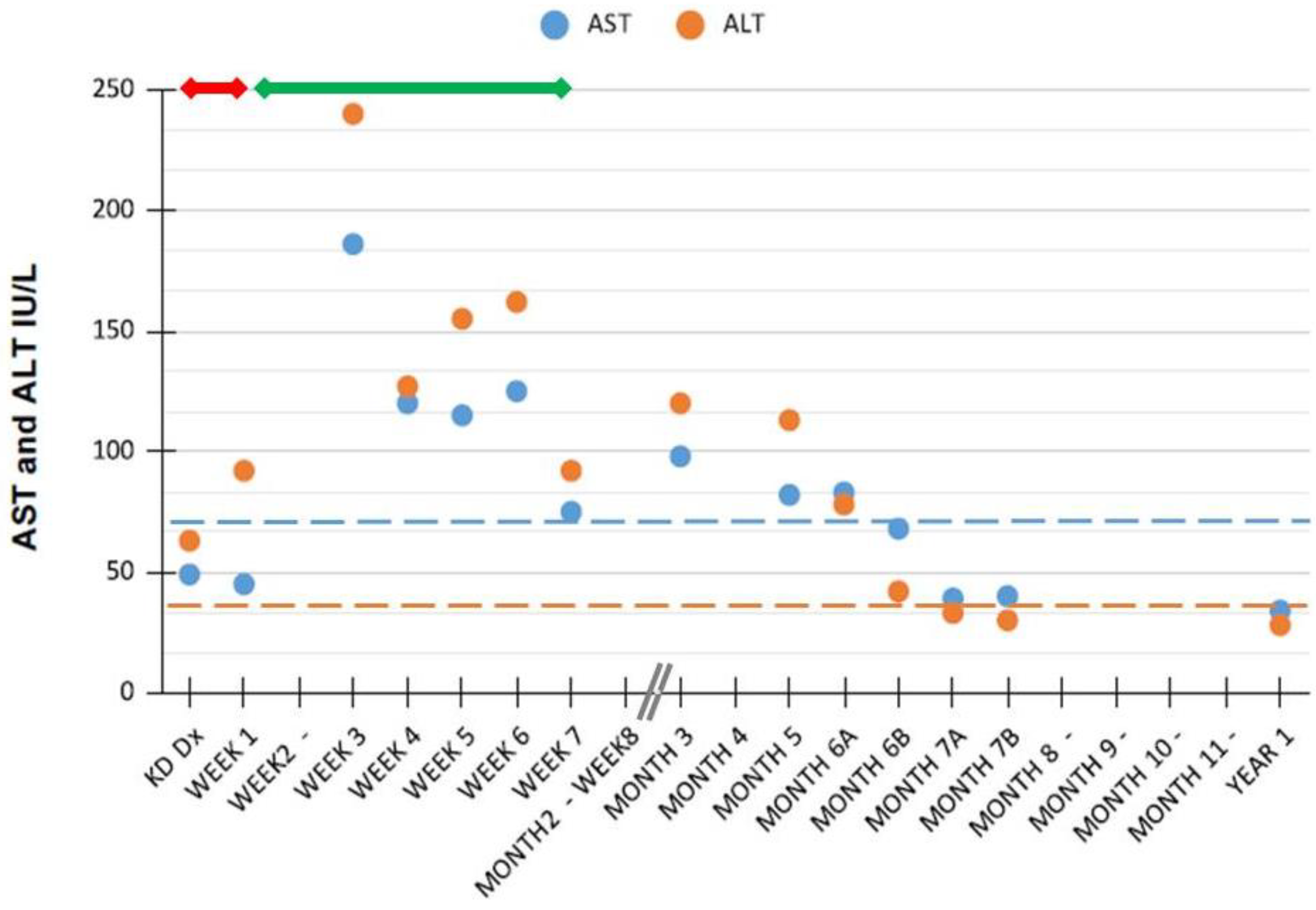
| Present Case | 1M 4 months | 50 (at Dx) | 60 (at Dx) | AST peaked at week 3 (186 IU/L); tended to normalize at 6th-7th month | ALT peaked at week 3 (240 IU/L); tended to normalize at 6th–7th month | 80 mg/kg/day × 5 days then 3 mg/kg/day × total 8 weeks |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paglia, P.; Nazzaro, L.; De Anseris, A.G.E.; Lettieri, M.; Colantuono, R.; Rocco, M.C.; Siano, M.A.; Biffaro, N.; VAJRO, P. Atypically Protracted Course of Liver Involvement in Kawasaki Disease. Case Report and Literature Review. Pediatr. Rep. 2021, 13, 357-362. https://doi.org/10.3390/pediatric13030044
Paglia P, Nazzaro L, De Anseris AGE, Lettieri M, Colantuono R, Rocco MC, Siano MA, Biffaro N, VAJRO P. Atypically Protracted Course of Liver Involvement in Kawasaki Disease. Case Report and Literature Review. Pediatric Reports. 2021; 13(3):357-362. https://doi.org/10.3390/pediatric13030044
Chicago/Turabian StylePaglia, Pamela, Lucia Nazzaro, Anna Giulia Elena De Anseris, Milena Lettieri, Rossella Colantuono, Maria Chiara Rocco, Maria Anna Siano, Nicola Biffaro, and Pietro VAJRO. 2021. "Atypically Protracted Course of Liver Involvement in Kawasaki Disease. Case Report and Literature Review" Pediatric Reports 13, no. 3: 357-362. https://doi.org/10.3390/pediatric13030044
APA StylePaglia, P., Nazzaro, L., De Anseris, A. G. E., Lettieri, M., Colantuono, R., Rocco, M. C., Siano, M. A., Biffaro, N., & VAJRO, P. (2021). Atypically Protracted Course of Liver Involvement in Kawasaki Disease. Case Report and Literature Review. Pediatric Reports, 13(3), 357-362. https://doi.org/10.3390/pediatric13030044