
Leveraging Omeprazole PBPK/PD Modeling to Inform Drug–Drug Interactions and Specific Recommendations for Pediatric Labeling

 , , ,
, , ,  ,
,  and
and
Abstract

1. Introduction
2. Materials and Methods
2.1. Software
2.2. Clinical PK Data
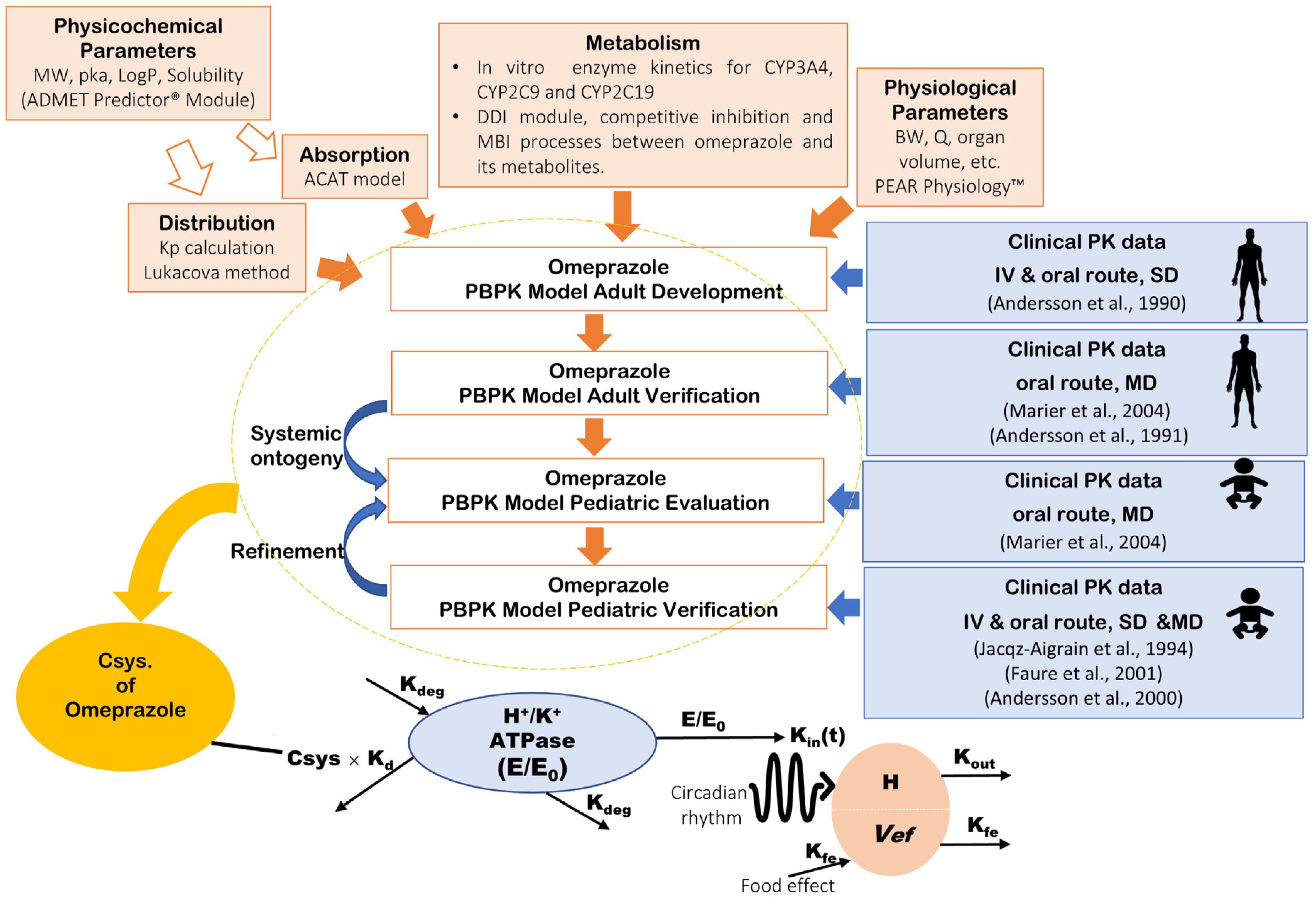
2.3. PBPK Model Development and Verification of Omeprazole in Adults
- Liver metabolism of omeprazole by CYP2C19 to form hydroxy–omeprazole and others such as 5′-O-desmethylomeprazole.
- Liver metabolism of omeprazole by CYP3A4 to form hydroxy–omeprazole, omeprazole sulphone and others such as 5′-O-desmethylomeprazole.
- Gut metabolism of omeprazole by CYP3A4 to form omeprazole sulphone.
- Liver metabolism of omeprazole by CYP2C9 to form hydroxy-omeprazole and others such as 5′-O-desmethylomeprazole.
2.4. PBPK Model Development and Verification of Omeprazole in Pediatrics
2.5. Application of the PBPK Model to Explore the Impact of Age-Dependent Physiological Changes on Omeprazole Exposure and Response
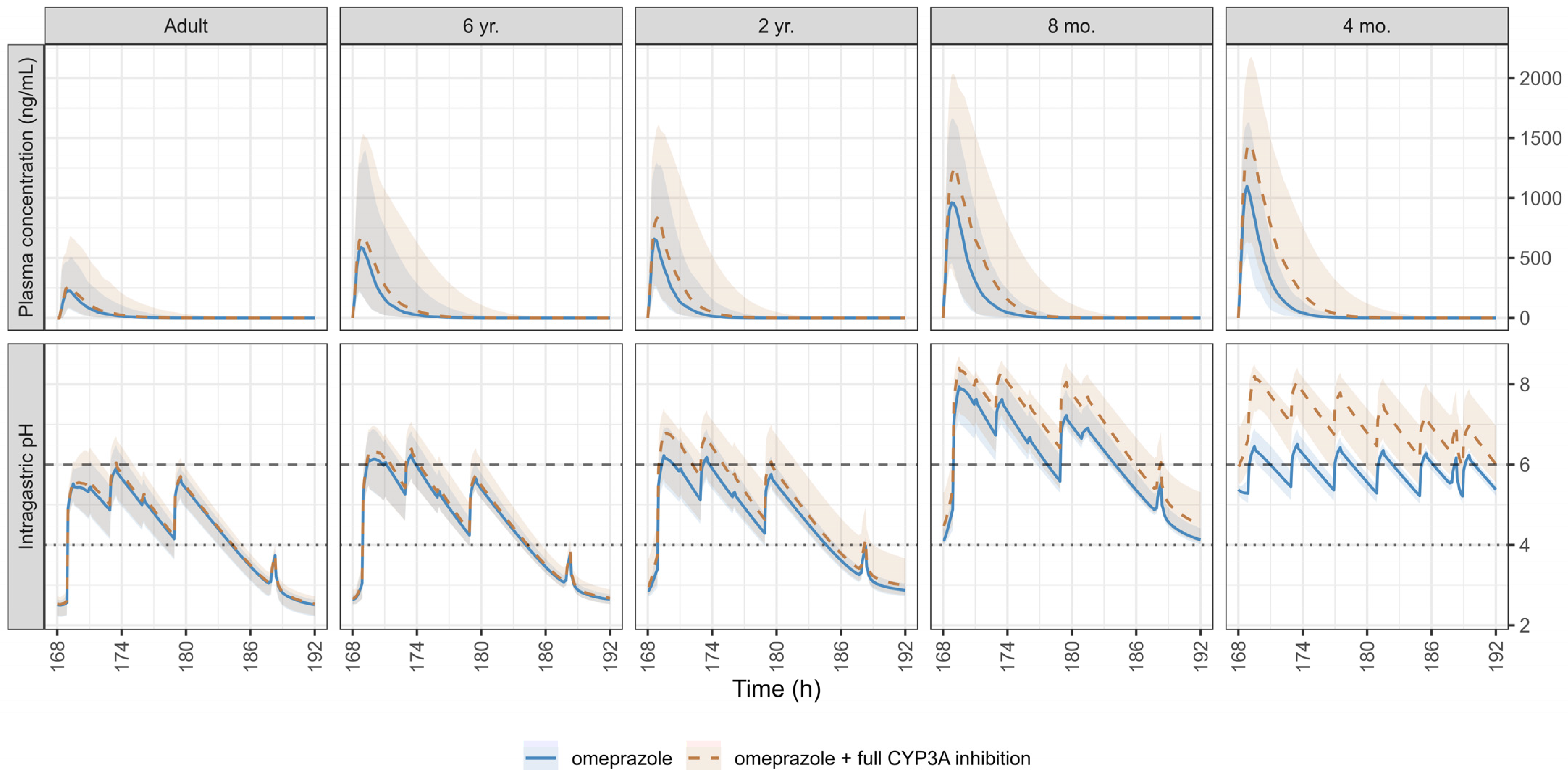
2.6. Application of the PBPK Model to Evaluate DDI on Omeprazole Exposure and Response
2.7. Statistical Analysis
3. Results
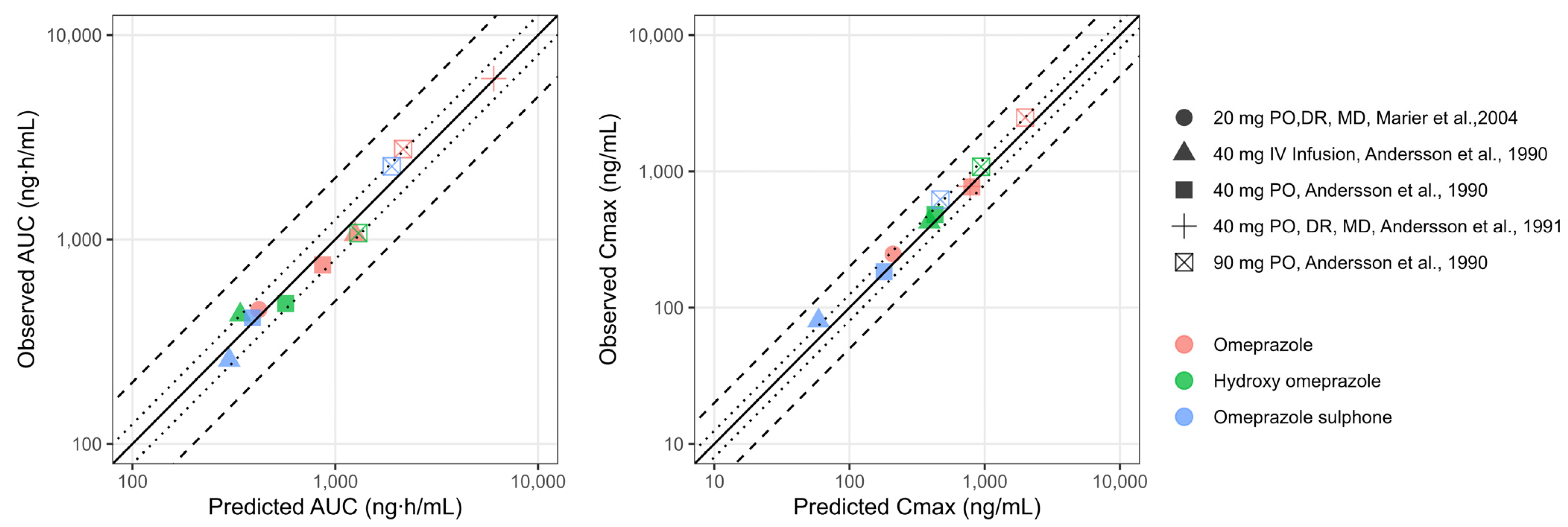
3.1. PBPK Model Development and Verification of Omeprazole and Its Metabolites in Adults
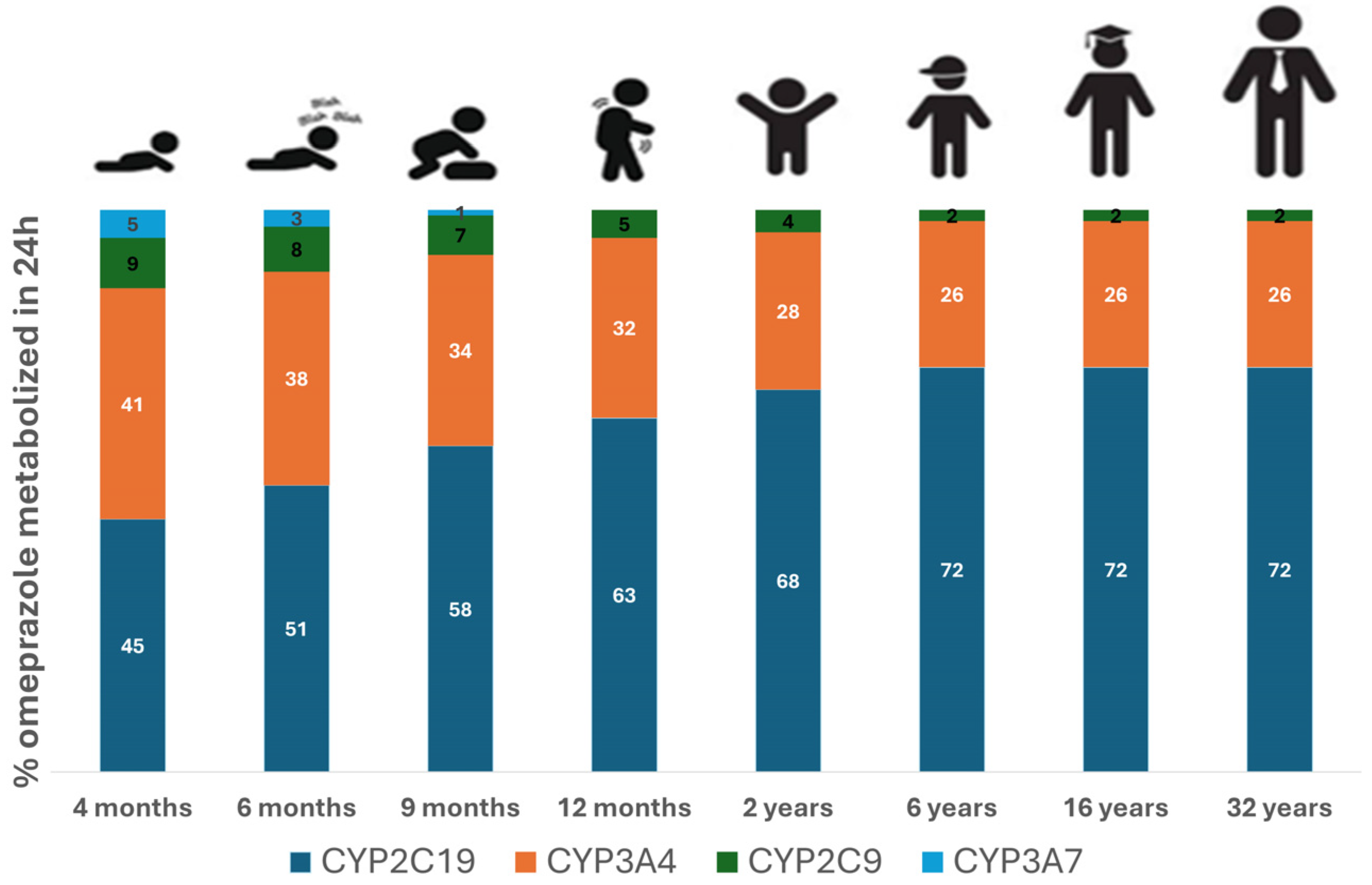
3.2. PBPK Model Extrapolation from Adults to Pediatrics
3.3. The Impact of Age-Dependent Physiological Changes on Omeprazole Exposure and Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lima, J.J.; Thomas, C.D.; Barbarino, J.; Desta, Z.; Van Driest, S.L.; El Rouby, N.; Johnson, J.A.; Cavallari, L.H.; Shakhnovich, V.; Thacker, D.L.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin. Pharmacol. Ther. 2021, 109, 1417–1423. [Google Scholar] [CrossRef]
- Boulton, K.H.A.; Dettmar, P.W. A Narrative Review of the Prevalence of Gastroesophageal Reflux Disease (GERD). Ann. Esophagus 2022, 5, 7. [Google Scholar] [CrossRef]
- Nirwan, J.S.; Hasan, S.S.; Babar, Z.-U.-D.; Conway, B.R.; Ghori, M.U. Global Prevalence and Risk Factors of Gastro-Oesophageal Reflux Disease (GORD): Systematic Review with Meta-Analysis. Sci. Rep. 2020, 10, 5814. [Google Scholar] [CrossRef] [PubMed]
- Cicala, M. Proton Pump Inhibitor Resistance, the Real Challenge in Gastro-Esophageal Reflux Disease. WJG 2013, 19, 6529. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.; Becher, A.; Jones, R. Systematic Review: Persistent Reflux Symptoms on Proton Pump Inhibitor Therapy in Primary Care and Community Studies. Aliment. Pharmacol. Ther. 2010, 32, 720–737. [Google Scholar] [CrossRef] [PubMed]
- Klinkenberg-knol, E.C.; Nelis, F.; Dent, J.; Snel, P.; Mitchell, B.; Prichard, P.; Lloyd, D.; Havu, N.; Frame, M.H.; Roma, J.; et al. Long-Term Omeprazole Treatment in Resistant Gastroesophageal Reflux Disease: Efficacy, Safety, and Influence on Gastric Mucosa. Gastroenterology 2000, 118, 661–669. [Google Scholar] [CrossRef]
- Andersson, T. Pharmacokinetics, Metabolism and Interactions of Acid Pump Inhibitors. Clin. Pharmacokinet. 1996, 31, 9–28. [Google Scholar] [CrossRef]
- Lind, T.; Cederberg, C.; Ekenved, G.; Haglund, U.; Olbe, L. Effect of Omeprazole--a Gastric Proton Pump Inhibitor--on Pentagastrin Stimulated Acid Secretion in Man. Gut 1983, 24, 270–276. [Google Scholar] [CrossRef]
- Cederberg, C.; Andersson, T.; Skånberg, I. Omeprazole: Pharmacokinetics and Metabolism in Man. Scand. J. Gastroenterol. 1989, 24, 33–40. [Google Scholar] [CrossRef]
- El-Kimary, E.I.; Ragab, M.A.A. Recent Analytical Methodologies for the Determination of Omeprazole and/or Its Active Isomer Esomeprazole in Different Matrices: A Critical Review. Crit. Rev. Anal. Chem. 2022, 52, 106–130. [Google Scholar] [CrossRef]
- Shin, J.M.; Kim, N. Pharmacokinetics and Pharmacodynamics of the Proton Pump Inhibitors. J. Neurogastroenterol. Motil. 2013, 19, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.-Y.; Sun, L.-N.; Zhang, X.-H.; Li, Y.-Q.; Yu, L.; Yuan, Z.-Q.-Y.; Meng, L.; Zhang, H.-W.; Wang, Y.-Q. A Review of the Novel Application and Potential Adverse Effects of Proton Pump Inhibitors. Adv. Ther. 2017, 34, 1070–1086. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Gibson, C.M.; Cheng, S.; Ollier, C.; Nicolas, O.; Bergougnan, L.; Perrin, L.; Lacreta, F.P.; Hurbin, F.; Dubar, M. Differential Effects of Omeprazole and Pantoprazole on the Pharmacodynamics and Pharmacokinetics of Clopidogrel in Healthy Subjects: Randomized, Placebo-Controlled, Crossover Comparison Studies. Clin. Pharmacol. Ther. 2011, 89, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Shirasaka, Y.; Sager, J.E.; Lutz, J.D.; Davis, C.; Isoherranen, N. Inhibition of CYP2C19 and CYP3A4 by Omeprazole Metabolites and Their Contribution to Drug-Drug Interactionss. Drug Metab. Dispos. 2013, 41, 1414–1424. [Google Scholar] [CrossRef]
- Zvyaga, T.; Chang, S.Y.; Chen, C.; Yang, Z.; Vuppugalla, R.; Hurley, J.; Thorndike, D.; Wagner, A.; Chimalakonda, A.; Rodrigues, A.D. Evaluation of Six Proton Pump Inhibitors as Inhibitors of Various Human Cytochromes P450: Focus on Cytochrome P450 2C19. Drug Metab. Dispos. 2012, 40, 1698–1711. [Google Scholar] [CrossRef]
- Ko, J.-W.; Sukhova, N.; Thacker, D.; Chen, P.; Flockhart, D.A. Evaluation of Omeprazole and Lansoprazole as Inhibitors of Cytochrome P450 Isoforms. Drug Metab. Dispos. 1997, 25, 853–862. [Google Scholar]
- U.S. Food and Drug Administration. Drug Development and Drug Interactions: Table of Substrates, Inhibitors, and Inducers; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2023; Available online: https://www.fda.gov/drugs/drug-interactions-labeling/drug-development-and-drug-interactions-table-substrates-inhibitors-and-inducers#table2-1 (accessed on 8 January 2025).
- Losurdo, G.; Caccavo, N.L.B.; Indellicati, G.; Celiberto, F.; Ierardi, E.; Barone, M.; Di Leo, A. Effect of Long-Term Proton Pump Inhibitor Use on Blood Vitamins and Minerals: A Primary Care Setting Study. J. Clin. Med. 2023, 12, 2910. [Google Scholar] [CrossRef]
- Lassalle, M.; Zureik, M.; Dray-Spira, R. Proton Pump Inhibitor Use and Risk of Serious Infections in Young Children. JAMA Pediatr. 2023, 177, 1028–1038. [Google Scholar] [CrossRef]
- Wagner, C.; Zhao, P.; Pan, Y.; Hsu, V.; Grillo, J.; Huang, S.; Sinha, V. Application of Physiologically Based Pharmacokinetic (PBPK) Modeling to Support Dose Selection: Report of an FDA Public Workshop on PBPK. CPT Pharmacom Syst. Pharma 2015, 4, 226–230. [Google Scholar] [CrossRef]
- Shin, J.M.; Sachs, G. Long-Lasting Inhibitors of the Gastric H,K-ATPase. Expert Rev. Clin. Pharmacol. 2009, 2, 461–468. [Google Scholar] [CrossRef]
- Shebley, M.; Sandhu, P.; Emami Riedmaier, A.; Jamei, M.; Narayanan, R.; Patel, A.; Peters, S.A.; Reddy, V.P.; Zheng, M.; De Zwart, L.; et al. Physiologically Based Pharmacokinetic Model Qualification and Reporting Procedures for Regulatory Submissions: A Consortium Perspective. Clin. Pharma Ther. 2018, 104, 88–110. [Google Scholar] [CrossRef] [PubMed]
- GastroPlus® PBPK & PBBM Modeling and Simulation. Available online: https://www.simulations-plus.com/software/gastroplus/ (accessed on 17 July 2024).
- Rackauckas, C.; Ma, Y.; Noack, A.; Dixit, V.; Mogensen, P.K.; Elrod, C.; Tarek, M.; Byrne, S.; Maddhashiya, S.; Calderón, J.B.S.; et al. Accelerated Predictive Healthcare Analytics with Pumas, A High Performance Pharmaceutical Modeling and Simulation Platform. BioRxiv, 2020; Preprint. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. In R Foundation for Statistical Computing; R Core Team R: Vienna, Austria, 2023. [Google Scholar]
- R Studio Team. RStudio: Integrated Development for R; R Studio Team: Boston, MA, USA, 2020; Available online: https://cir.nii.ac.jp/crid/1370004240607707919 (accessed on 5 February 2025).
- Andersson, T.; Cederberg, C.; Reggtrdh, C.-G.; Skgtnberg, I. European Doumal of (Pharmacokinetics of Various Single Intravenous and Oral Doses of Omeprazole. Eur. J. Clin. Pharmacol. 1990, 39, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Marier, J.-F.; Dubuc, M.-C.; Drouin, E.; Alvarez, F.; Ducharme, M.P.; Brazier, J.-L. Pharmacokinetics of Omeprazole in Healthy Adults and in Children with Gastroesophageal Reflux Disease. Ther. Drug Monit. 2004, 26, 3–8. [Google Scholar] [CrossRef]
- Andersson, T.; Cederberg, C.; Heggelund, A.; Lundborg, P. The Pharmacokinetics of Single and Repeated Once-Daily Doses of 10, 20 and 40mg Omeprazole as Enteric-Coated Granules. Drug Investig. 1991, 3, 45–52. [Google Scholar] [CrossRef]
- Jacqz-Aigrain, E.; Andre, J.; Bellaich, M.; Faure, C.; Navarro, J.; Rohrlich, P.; Baudouin, V. Pharmacokinetics of Intravenous Omeprazole in Children. Eur. J. Clin. Pharmacol. 1994, 47, 181–185. [Google Scholar] [CrossRef]
- Faure, C.; Michaud, L.; Shaghaghi, E.K.; Popon, M.; Turck, D.; Navarro, J.; Jacqz-Aigrain, E. Intravenous Omeprazole in Children: Pharmacokinetics and Effect on 24-Hour Intragastric pH. J. Pediatr. Gastroenterol. Nutr. 2001, 33. [Google Scholar]
- Andersson, T.; Hassall, E.; Ch, M.B.B.; Shepherd, R.; Radke, M.; Marcon, M.; Dalväg, A.; Martin, S.; Behrens, R.; Koletzko, S.; et al. Pharmacokinetics of Orally Administered Omeprazole in Children. Am. J. Gastroenterol. 2000, 95, 3101–3106. [Google Scholar] [CrossRef]
- Lukacova, V.; Parrott, N.; Lave, T.; Fraczkiewicz, G.; Bolger, M. General Approach to Calculation of Tissue:Plasma Partition Coefficients for Physiologically Based Pharmacokinetic (PBPK) Modeling. In Proceedings of the Simulations Plus, Atlanta, GA, USA, 17 November 2008. [Google Scholar]
- Abelo, A.A.; Andersson, T.B.; Bredberg, U.; Skånberg, I.; Weidolf, L. Stereoselective Metabolism by Human Liver Cyp Enzymes of a Substituted Benzimidazole. Drug Metab. Dispos. 1999, 28, 58–64. [Google Scholar] [CrossRef]
- Andersson, T.; Hassan-Alin, M.; Hasselgren, G.; Röhss, K.; Weidolf, L. Pharmacokinetic Studies with Esomeprazole, the (S)-Isomer of Omeprazole. Clin. Pharmacokinet. 2001, 40, 411–426. [Google Scholar] [CrossRef]
- Abelo, A.A.; Andersson, T.B.; Antonsson, M.; Naudot, A.K.; Skånberg, I.; Weidolf, L. Stereoselective Metabolism of Omeprazole by Human Cytochrome P450 Enzymes. Drug Metab. Dispos. 1994, 28, 966–972. [Google Scholar] [CrossRef]
- Andersson, T.; Miners, J.; Veronese, M.; Birkett, D. Identification of Human Liver Cytochrome P450 Isoforms Mediating Secondary Omeprazole Metabolism. Br. J. Clin. Pharma 1994, 37, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.C.; Yang, C.Q.; Cho, H.K.; Suh, O.K.; Shin, W.G. Influence of Fluconazole on the Pharmacokinetics of Omeprazole in Healthy Volunteers. Biopharm. Drug Disp. 2002, 23, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.A.; Ring, B.J.; Cantrell, V.E.; Jones, D.R.; Eckstein, J.; Ruterbories, K.; Hamman, M.A.; Hall, S.D.; Wrighton, S.A. Comparative Metabolic Capabilities of CYP3A4, CYP3A5, and CYP3A7. Drug Metab. Dispos. 2002, 30, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, D.; Sonnier, M.; Moncion, A.; Cheron, G.; Cresteil, T. Expression of CYP3A in the Human Liver — Evidence That the Shift between CYP3A7 and CYP3A4 Occurs Immediately After Birth. Eur. J. Biochem. 1997, 247, 625–634. [Google Scholar] [CrossRef]
- Kovar, L.; Schräpel, C.; Selzer, D.; Kohl, Y.; Bals, R.; Schwab, M.; Lehr, T. Physiologically-Based Pharmacokinetic (PBPK) Modeling of Buprenorphine in Adults, Children and Preterm Neonates. Pharmaceutics 2020, 12, 578. [Google Scholar] [CrossRef]
- Du Bois, D.; Du Bois, E.F. A Formula to Estimate the Approximate Surface Area If Height and Weight Be Known. 1916. Nutrition 1989, 5, 303–311, discussion 312–313. [Google Scholar]
- Pacifici, G.M. Clinical Pharmacology of Omeprazole in Infants and Children. J. Drug Des. Res. 2022, 9, 1090. [Google Scholar] [CrossRef]
- Liu, D.; Yang, H.; Jiang, J.; Nagy, P.; Shen, K.; Qian, J.; Hu, P. Pharmacokinetic and Pharmacodynamic Modeling Analysis of Intravenous Esomeprazole in Healthy Volunteers: Esomeprazole in Healthy Volunteers. J. Clin. Pharmacol. 2016, 56, 816–826. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; Food and Drug Administration; Center for Drug Evaluation and Research (CDER); Center for Biologics Evaluation and Research (CBER). M12 Drug Interaction Studies: Guidance for Industry; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2024; Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/m12-drug-interaction-studies (accessed on 5 January 2025).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 4594, Omeprazole; National Center for Biotechnology Information: Bethesda, MD, USA, 2004; Available online: https://pubchem.ncbi.nlm.nih.gov/source/hsdb/3575 (accessed on 5 January 2025).
- Yang, R.; Schulman, S.G.; Zavala, P.J. Acid–Base Chemistry of Omeprazole in Aqueous Solutions. Anal. Chim. Acta 2003, 481, 155–164. [Google Scholar] [CrossRef]
- Singh, R.; Saraf, S. Spectrophotometric Estimation of Omeprazole in Pharmaceutical Dosage Form. Res. J. Pharm. and Tech. 2003, 1, 276–277. [Google Scholar]
- Handin, N. Proteomics Informed Investigation of Human Hepatocytes and Liver Tissue. In Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Pharmacy; Acta Universitatis Upsaliensis: Uppsala, Sweden, 2021; Volume 298, ISBN 978-91-513-1247-7. [Google Scholar]
- Regårdh, C.-G.; Gabrielsson, M.; Hoffman, K.-J.; Löfberg, I.; Skånberg, I. Pharmacokinetics and Metabolism of Omeprazole in Animals and Man—An Overview. Scand. J. Gastroenterol. 1985, 20, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Regårdh, C.G.; Andersson, T.; Lagerström, P.O.; Lundborg, P.; Skånberg, I. The Pharmacokinetics of Omeprazole in Humans—A Study of Single Intravenous and Oral Doses. Ther. Drug Monit. 1990, 12, 163–172. [Google Scholar] [CrossRef]
- Yang, R.; Lin, Y.; Chen, K.; Huang, J.; Yang, S.; Yao, A.; Yang, X.; Lei, D.; Xiao, J.; Yang, G.; et al. Establishing Virtual Bioequivalence and Clinically Relevant Specifications for Omeprazole Enteric-Coated Capsules by Incorporating Dissolution Data in PBPK Modeling. AAPS J. 2024, 26, 82. [Google Scholar] [CrossRef]
- Segregur, D.; Mann, J.; Moir, A.; Karlsson, E.M.; Dressman, J. Prediction of Plasma Profiles of a Weakly Basic Drug after Administration of Omeprazole Using PBPK Modeling. Eur. J. Pharm. Sci. 2021, 158, 105656. [Google Scholar] [CrossRef] [PubMed]
- De Wildt, S.N.; Kearns, G.L.; Leeder, J.S.; Van Den Anker, J.N. Cytochrome P450 3A Ontogeny and Drug Disposition. Clin. Pharmacokinet. (Drug Dispos.) 1999, 37, 485–505. [Google Scholar] [CrossRef]
- Kearns, G.L.; Andersson, T.; James, L.P.; Gaedigk, A.; Kraynak, R.A.; Abdel-Rahman, S.M.; Ramabadran, K.; Van Den Anker, J.N. Pediatric Pharmacology Research Unit Network Omeprazole Disposition in Children Following Single-Dose Administration. J. Clin. Pharma 2003, 43, 840–848. [Google Scholar] [CrossRef]
- Leeder, J.S.; Kearns, G.L. Pharmacogenetics in Pediatrics. Pediatr. Clin. North. Am. 1997, 44, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Dean, L.; Kane, M. Omeprazole Therapy and CYP2C19 Genotype; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kattman, B.L., Malheiro, J.A., Eds.; Medical Genetics Summaries [Internet]. National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Shirai, N.; Furuta, T.; Moriyama, Y.; Okochi, H.; Kobayashi, K.; Takashima, M.; Xiao, F.; Kosuge, K.; Nakagawa, K.; Hanai, H.; et al. Effects of CYP2C19 Genotypic Differences in the Metabolism of Omeprazole and Rabeprazole on Intragastric pH. Aliment. Pharmacol. Ther. 2001, 15, 1929–1937. [Google Scholar] [CrossRef]
- Boyle, J.T. Acid Secretion From Birth to Adulthood. J. Pediatr. Gastroenterol. Nutr. 2003, 37, S12–S16. [Google Scholar] [CrossRef]
- Pippa, L.F.; Vozmediano, V.; Mitrov-Winkelmolen, L.; Touw, D.; Soliman, A.; Cristofoletti, R.; Salgado Junior, W.; de Moraes, N.V. Impact of Obesity and Roux-En-Y Gastric Bypass on the Pharmacokinetics of (R)- and (S)-Omeprazole and Intragastric pH. CPT: Pharmacomet. Syst. Pharmacol. 2024, 13, 1528–1541. [Google Scholar] [CrossRef]
- Kirchheiner, J.; Glatt, S.; Fuhr, U.; Klotz, U.; Meineke, I.; Seufferlein, T.; Brockmöller, J. Relative Potency of Proton-Pump Inhibitors—Comparison of Effects on Intragastric pH. Eur. J. Clin. Pharmacol. 2009, 65, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Jonathan Bishop, Ã.; Furman, M.; Mike Thomson à Sheffield Children, Ã. Omeprazole for Gastroesophageal Reflux Disease in the First 2 Years of Life: A Dose-Finding Study with Dual-Channel pH Monitoring. J. Pediatr. Gastroenterol. Nutr. 2007, 45, 50–55. [Google Scholar] [CrossRef]
- Gan, J.; Bornhorst, G.M.; Henrick, B.M.; German, J.B. Protein Digestion of Baby Foods: Study Approaches and Implications for Infant Health. Mol. Nutr. Food Res. 2018, 62, 1700231. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Gossman, W. Omeprazole. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK539786/ (accessed on 5 January 2025).
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef]
- Rouaz-El Hajoui, K.; Chiclana-Rodríguez, B.; Nardi-Ricart, A.; Suñé-Pou, M.; Mercadé-Frutos, D.; María Suñé-Negre, J.; Pérez-Lozano, P.; García-Montoya, E. Formulation of Omeprazole in the Pediatric Population: A Review. J. Pharm. Sci. Drug Discov. 2023, 2, 1–13. [Google Scholar]
- Katashima, M.; Yamamoto, K.; Tokuma, Y.; Hata, T.; Sawada, Y.; Iga, T. Comparative Pharmacokinetic/Pharmacodynamic Analysis of Proton Pump Inhibitors Omeprazole, Lansoprazole and Pantoprazole, in Humans. Eur. J. Drug Metab. Pharmacokinet. 1998, 23, 19–26. [Google Scholar] [CrossRef]
- Kaye, J.L. Review of Paediatric Gastrointestinal Physiology Data Relevant to Oral Drug Delivery. Int. J. Clin. Pharm. 2011, 33, 20–24. [Google Scholar] [CrossRef]
- Rødbro, P.; Krasilnikoff, P.A.; Christiansen, P.M. Parietal Cell Secretory Function in Early Childhood. Scand. J. Gastroenterol. 1967, 2, 209–213. [Google Scholar] [CrossRef]
- Wills, L.; Paterson, D. A Study of Gastric Acidity in Infants. Arch. Dis. Child. 1926, 1, 232–244. [Google Scholar] [CrossRef]
- Bartelink, I.H.; Rademaker, C.M.A.; Schobben, A.F.A.M.; Van Den Anker, J.N. Guidelines on Paediatric Dosing on the Basis of Developmental Physiology and Pharmacokinetic Considerations. Clin. Pharmacokinet. 2006, 45, 1077–1097. [Google Scholar] [CrossRef]
- Energy In: Recommended Food & Drink Amounts for Children. Available online: https://www.healthychildren.org/English/healthy-living/nutrition/Pages/Energy-In-Recommended-Food-Drink-Amounts-for-Children.aspx (accessed on 1 February 2024).
- Amount and Schedule of Baby Formula Feedings. Available online: https://www.healthychildren.org/English/ages-stages/baby/formula-feeding/Pages/amount-and-schedule-of-formula-feedings.aspx (accessed on 1 February 2024).
- Sample Menu for A Two-Year-Old. Available online: https://www.healthychildren.org/English/ages-stages/toddler/nutrition/Pages/Sample-One-Day-Menu-for-a-Two-Year-Old.aspx (accessed on 1 February 2024).
- Sample Menu for A Baby 8 to 12 Months Old. Available online: https://www.healthychildren.org/English/ages-stages/baby/feeding-nutrition/Pages/sample-one-day-menu-for-an-8-to-12-month-old.aspx (accessed on 1 February 2024).
- Online Food Calculator. Food Weight to Volume Conversions. Available online: https://www.aqua-calc.com/calculate/food-weight-to-volume (accessed on 1 February 2024).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Reference) | Number Sex | Dosage Regimen | Route | Age [Years] Mean ± SD (Range) | Body Weight [kg] Mean ± SD (Range) | |
|---|---|---|---|---|---|---|
| Healthy adult PBPK model development | [27] | 10 M | 40 mg single dose 40 mg and 90 mg single dose | IV PO | (19–27) | (70–86) |
| Healthy adult PBPK model verification | [28] | 18M | 20 mg delayed-release capsules multiple doses | PO | 36.8 ± 5.6 (26–45) | 71.0 ± 7.6 (58.5–84.4) |
| [29] | 12M | 40 mg delayed-release granules multiple doses | PO | (23–29) | (67–86) | |
| Pediatric extrapolation of the PBPK model | [28] | 6M/6F | 10 to 20 mg delayed-release capsules multiple doses | PO | 6.1 ± 4.4 (0.5–13) | 24.2 ± 16.5 (6.0–64.2) |
| Pediatric PBPK model verification | [30] | 5 * | 60 to 80 mg/1.73 m2 loading dose followed by 40 mg * 1.73 m2 at 12 h intervals, | Slow bolus or over 15 min IV infusion | ||
| [31] | 6M/3F | 20 to 40 mg/1.73 m2 once daily | IV infusion (1 h) | (0.4–2.3) | ||
| [32] | 25 | the “healing dose” of omeprazole in each child was that which controlled pathological acid reflux | PO | (1–16) | (10.7–68) |
| Parameter | Value | Reference |
|---|---|---|
| Molecular weight | 345.4 g/mol | [42,46] |
| logP | 2.23 | [46] |
| Diffusion coefficient | 0.71 × 10−5 cm2/s | ADMET Predictor v.9.5 |
| pKa | 14.7 (Acid) 7.1 (Base) | [47] |
| Reference solubility | 0.0823 mg/mL at pH = 7.4 | [48] |
| Solubility Factor | 125.54 | ADMET Predictor v.9.5 |
| FaSSIF solubility | 0.27 mg/mL at pH = 6.5 | [49] |
| FeSSIF solubility | 0.22 mg/mL at pH = 5.0 | [49] |
| Human effective permeability (Peff) | 12 × 10−4 cm/s | Fitted |
| Particle radius | 25 μm | GastroPlus v.9.8 default |
| Precipitate radius | 1 μm | GastroPlus v.9.8 default |
| Drug particle density | 1.2 g/mL | GastroPlus v.9.8 default |
| Mean precipitation time | 900 s | GastroPlus v.9.8 default |
| Blood–plasma concentration ratio (Rbp) | 0.6 | [50] |
| Fraction unbound in plasma (Fup)% | 4.9852% | [50] |
| Formation of 5-O-desmethyl metabolite | ||
| CYP2C19 Km,u (PBPK) | 0.811 mg/L | [34] |
| CYP2C19 Vmax (PBPK) | 5.115 × 10−4 mg/s/mg enzyme | Initially informed from in vitro [34] then fitted |
| CYP2C9 Km,u (PBPK) | 73.92 mg/L | [34] |
| CYP2C9 Vmax (PBPK) | 7.97 × 10−5 mg/s/mg enzyme | [34] |
| CYP3A4 Km,u (PBPK) | 181 mg/L | [34] |
| CYP3A4 Vmax (PBPK) | 3.637 × 10−3 mg/s/mg enzyme | Initially informed from in vitro [34] then fitted |
| CYP3A7 Km,u (PBPK) | 923.1 mg/L | Calculated from Km for CYP3A4 [41] |
| CYP3A7 Vmax (PBPK) | 9.09 × 10−4 mg/s/mg enzyme | Calculated from Vmax for CYP3A4 [41] |
| Formation of Hydroxy metabolite | ||
| CYP2C19 Km,u (PBPK) | 1.657 mg/L | [32] |
| CYP2C19 Vmax (PBPK) | 3.67 × 10−3 mg/s/mg enzyme | Initially informed from in vitro [32] then fitted |
| CYP2C9 Km,u (PBPK) | 141.3 mg/L | [32] |
| CYP2C9 Vmax (PBPK) | 1.803 × 10−3 mg/s/mg enzyme | Initially informed from in vitro [32] then fitted |
| CYP3A4 Km,u (PBPK) | 117.4 mg/L | [32] |
| CYP3A4 Vmax (PBPK) | 8.39 × 10−4 mg/s/mg enzyme | [32] |
| CYP3A7 Km,u (PBPK) | 598.23 mg/L | Calculated from Km for CYP3A4 [41] |
| CYP3A7 Vmax (PBPK) | 2.10 × 10−4 mg/s/mg enzyme | Calculated from Vmax for CYP3A4 [41] |
| Formation of Sulphone metabolite | ||
| CYP3A4 Km,u (PBPK) | 28.57 mg/L | [34] |
| CYP3A4 Vmax (PBPK) | 1.5 × 10−3 mg/s/mg enzyme | Initially informed from in vitro [34] then fitted |
| CYP3A4 Km,u (Gut) | 28.57 mg/L | [34] |
| CYP3A4 Vmax (Gut) | 0.921 mg/s/mg enzyme | Initially informed from in vitro [34] then fitted |
| CYP3A7 Km,u (PBPK) | 145.7 mg/L | Calculated from Km for CYP3A4 [41] |
| CYP3A7 Vmax (PBPK) | 3.75 × 10−4 mg/s/mg enzyme | Calculated from Vmax for CYP3A4 [41] |
| CYP450 target | Inhibitor | Parameters | References | ||
|---|---|---|---|---|---|
| IC50 | KI | Kinact | |||
| CYP2C19 | Omeprazole | 8.4 µM | 1.1 µM | 0.048 min−1 | [14,15] |
| Hydroxy omeprazole | 39 µM | [14] | |||
| Omeprazole sulphone | 5.1 µM | 5.7 µM | 0.015 min−1 | [14] | |
| CYP3A4 | Omeprazole | 40 µM | 52 µM | 0.029 min−1 | [14] |
| Hydroxy omeprazole | 21 µM | [14] | |||
| Omeprazole sulphone | 8 µM | [14] | |||
| Subject | Age (Years) | Dose (mg) | Body Weight (kg) a | Observed AUC0–12 (µg∙h/mL) | Predicted AUC0–12 (µg∙h/mL) Without CYP3A7, n = 1 Subject | Predicted AUC0–12 (µg∙h/mL) with CYP3A7, n = 1 Subject | Predicted AUC0–12 (µg∙h/mL) with CYP3A7 (Min–Max), n = 25 Subjects |
|---|---|---|---|---|---|---|---|
| 1 | 0.3 | 6 | 4.8 | 6.42 | 16 | 10.55 | (1.14–11.11) |
| 2 | 0.7 | 8 | 7.0 | 2.56 | 4.4 | 3.05 | (0.41–7.53) |
| 3 | 0.8 | 9 | 9.7 | 1.48 | 3.13 | 2.36 | (0.57–12.1) |
| 4 | 1.6 | 9 | 7.0 | 5.24 | 5.1 | 5.03 | (0.84–16.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soliman, A.; Rodriguez-Vera, L.; Alarcia-Lacalle, A.; Pippa, L.F.; Subhani, S.; Lukacova, V.; Duconge, J.; de Moraes, N.V.; Vozmediano, V. Leveraging Omeprazole PBPK/PD Modeling to Inform Drug–Drug Interactions and Specific Recommendations for Pediatric Labeling. Pharmaceutics 2025, 17, 373. https://doi.org/10.3390/pharmaceutics17030373
Soliman A, Rodriguez-Vera L, Alarcia-Lacalle A, Pippa LF, Subhani S, Lukacova V, Duconge J, de Moraes NV, Vozmediano V. Leveraging Omeprazole PBPK/PD Modeling to Inform Drug–Drug Interactions and Specific Recommendations for Pediatric Labeling. Pharmaceutics. 2025; 17(3):373. https://doi.org/10.3390/pharmaceutics17030373
Chicago/Turabian StyleSoliman, Amira, Leyanis Rodriguez-Vera, Ana Alarcia-Lacalle, Leandro F. Pippa, Saima Subhani, Viera Lukacova, Jorge Duconge, Natalia V. de Moraes, and Valvanera Vozmediano. 2025. "Leveraging Omeprazole PBPK/PD Modeling to Inform Drug–Drug Interactions and Specific Recommendations for Pediatric Labeling" Pharmaceutics 17, no. 3: 373. https://doi.org/10.3390/pharmaceutics17030373
APA StyleSoliman, A., Rodriguez-Vera, L., Alarcia-Lacalle, A., Pippa, L. F., Subhani, S., Lukacova, V., Duconge, J., de Moraes, N. V., & Vozmediano, V. (2025). Leveraging Omeprazole PBPK/PD Modeling to Inform Drug–Drug Interactions and Specific Recommendations for Pediatric Labeling. Pharmaceutics, 17(3), 373. https://doi.org/10.3390/pharmaceutics17030373