

Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register–12-Month Follow-Up

 ,
,  , ,
, ,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
- (a)
- COVID-19 disease (confirmed by PCR or antigen tests in accordance with applicable regulations in the European Union);
- (b)
- Age ≥ 18 years;
- (c)
- Written consent to participate in the study.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mumtaz, A.; Sheikh, A.A.E.; Khan, A.M.; Khalid, S.N.; Khan, J.; Nasrullah, A.; Sagheer, S.; Sheikh, A.B. COVID-19 Vaccine and Long COVID: A Scoping Review. Life 2022, 12, 1066. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 10 March 2023).
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. EClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef] [PubMed]
- Raport Szczepień Przeciwko COVID-19. Available online: https://www.gov.pl/web/szczepimysie/raport-szczepien-przeciwko-COVID-19 (accessed on 10 March 2023).
- Watanabe, A.; Iwagami, M.; Yasuhara, J.; Takagi, H.; Kuno, T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 10 March 2023).
- COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 8 June 2023).
- Wisnivesky, J.P.; Govindarajulu, U.; Bagiella, E.; Goswami, R.; Kale, M.; Campbell, K.N.; Meliambro, K.; Chen, Z.; Aberg, J.A.; Lin, J.J. Association of Vaccination with the Persistence of Post-COVID Symptoms. J. Gen. Intern. Med. 2022, 37, 1748–1753. [Google Scholar] [CrossRef] [PubMed]
- Chudzik, M.; Babicki, M.; Kapusta, J.; Kaluzinska-Kolat, Z.; Kolat, D.; Jankowski, P.; Mastalerz-Migas, A. Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study. Viruses 2022, 14, 1755. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Liu, J.; Liu, M. Effect of COVID-19 Vaccines on Reducing the Risk of Long COVID in the Real World: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12422. [Google Scholar] [CrossRef]
- Post-COVID Conditions: Information for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html (accessed on 10 March 2023).
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyere, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, S.W.; Chang, H.H.; Kwon, K.T.; Hwang, S.; Bae, S. One Year Follow-Up of COVID-19 Related Symptoms and Patient Quality of Life: A Prospective Cohort Study. Yonsei Med. J. 2022, 63, 499–510. [Google Scholar] [CrossRef]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef]
- Nehme, M.; Braillard, O.; Salamun, J.; Jacquerioz, F.; Courvoisier, D.S.; Spechbach, H.; Guessous, I. Symptoms After COVID-19 Vaccination in Patients with Post-Acute Sequelae of SARS-CoV-2. J. Gen. Intern. Med. 2022, 37, 1585–1588. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef]
- Mizrahi, B.; Sudry, T.; Flaks-Manov, N.; Yehezkelli, Y.; Kalkstein, N.; Akiva, P.; Ekka-Zohar, A.; Ben David, S.S.; Lerner, U.; Bivas-Benita, M.; et al. Long covid outcomes at one year after mild SARS-CoV-2 infection: Nationwide cohort study. BMJ 2023, 380, e072529. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Stehlik, P.; Clark, J.; Alcorn, K.; Glasziou, P. Effect of COVID-19 vaccination on long covid: Systematic review. BMJ Med. 2023, 2, e000385. [Google Scholar] [CrossRef] [PubMed]
- Edwards, F.; Hamilton, F.W. Impact of COVID-19 vaccination on long covid. BMJ Med. 2023, 2, e000470. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Harrison, P.J. Six-month sequelae of post-vaccination SARS-CoV-2 infection: A retrospective cohort study of 10,024 breakthrough infections. Brain Behav. Immun. 2022, 103, 154–162. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of long covid symptoms after COVID-19 vaccination: Community based cohort study. BMJ 2022, 377, e069676. [Google Scholar] [CrossRef]
- Richard, S.A.; Pollett, S.D.; Fries, A.C.; Berjohn, C.M.; Maves, R.C.; Lalani, T.; Smith, A.G.; Mody, R.M.; Ganesan, A.; Colombo, R.E.; et al. Persistent COVID-19 Symptoms at 6 Months After Onset and the Role of Vaccination Before or After SARS-CoV-2 Infection. JAMA Netw. Open 2023, 6, e2251360. [Google Scholar] [CrossRef]
- Swarnakar, R.; Jenifa, S.; Wadhwa, S. Musculoskeletal complications in long COVID-19: A systematic review. World J. Virol. 2022, 11, 485–495. [Google Scholar] [CrossRef]
- Disser, N.P.; De Micheli, A.J.; Schonk, M.M.; Konnaris, M.A.; Piacentini, A.N.; Edon, D.L.; Toresdahl, B.G.; Rodeo, S.A.; Casey, E.K.; Mendias, C.L. Musculoskeletal Consequences of COVID-19. J. Bone Jt. Surg. Am. 2020, 102, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Tleyjeh, I.M.; Saddik, B.; AlSwaidan, N.; AlAnazi, A.; Ramakrishnan, R.K.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.; Halwani, R. Prevalence and prbedictors of Post-Acute COVID-19 Syndrome (PACS) after hospital discharge: A cohort study with 4 months median follow-up. PLoS ONE 2021, 16, e0260568. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.; Kobayashi, K.; Tanaka, M.; Asayama, K.; Yamamoto, E.; Nakagami, H.; Hoshide, S.; Kishi, T.; Matsumoto, C.; Mogi, M.; et al. COVID-19 pandemic and hypertension: An updated report from the Japanese Society of Hypertension project team on COVID-19. Hypertens. Res. 2023, 46, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Cohen, K.; Ren, S.; Heath, K.; Dasmarinas, M.C.; Jubilo, K.G.; Guo, Y.; Lipsitch, M.; Daugherty, S.E. Risk of persistent and new clinical sequelae among adults aged 65 years and older during the post-acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ 2022, 376, e068414. [Google Scholar] [CrossRef]
- Matsumoto, C.; Shibata, S.; Kishi, T.; Morimoto, S.; Mogi, M.; Yamamoto, K.; Kobayashi, K.; Tanaka, M.; Asayama, K.; Yamamoto, E.; et al. Long COVID and hypertension-related disorders: A report from the Japanese Society of Hypertension Project Team on COVID-19. Hypertens. Res. 2023, 46, 601–619. [Google Scholar] [CrossRef]

{kind=link}
| N (%) | |
|---|---|
| Vaccination status | |
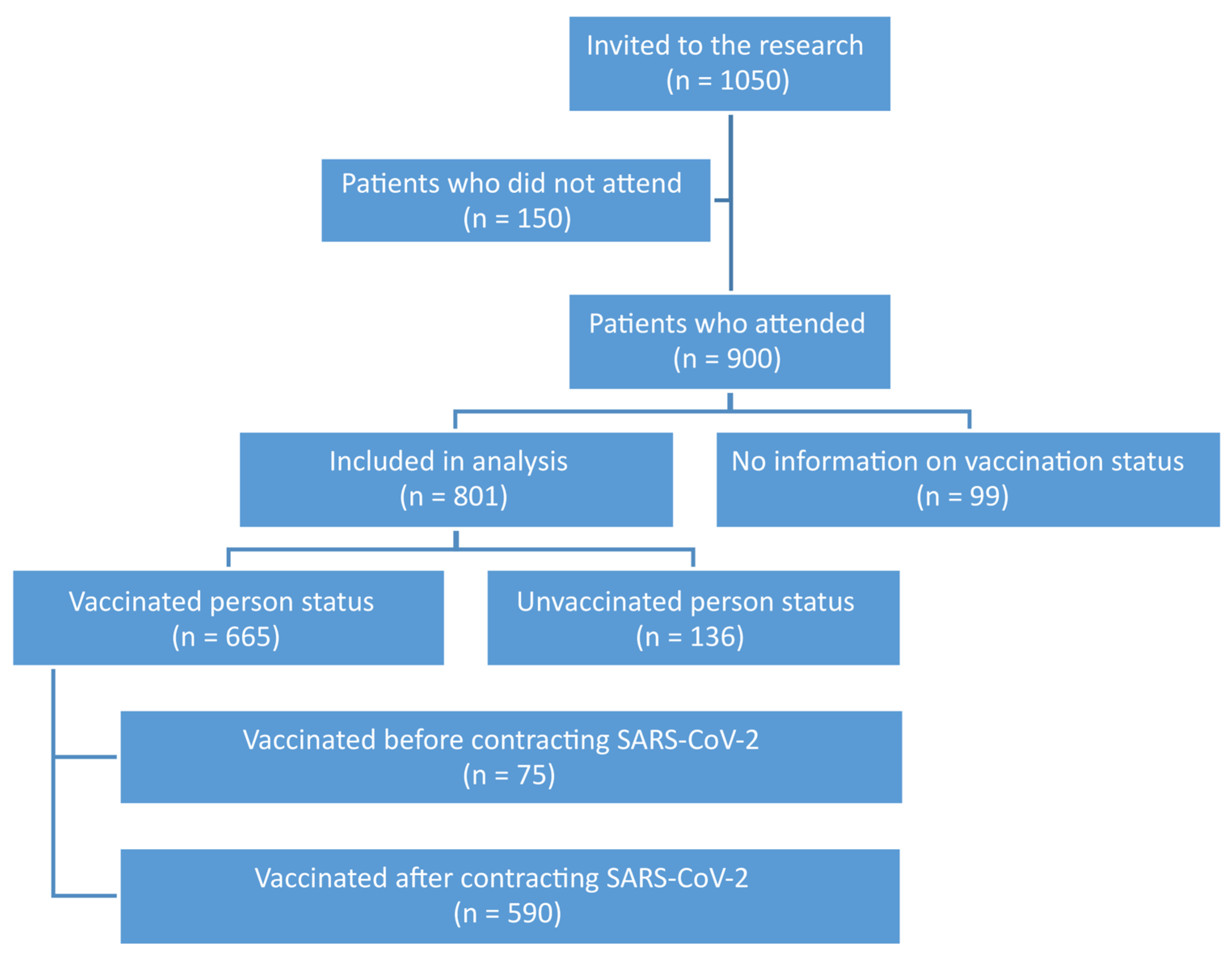
| Vaccinated | 665 (83.0) |
| Unvaccinated | 136 (17.0) |
| Date of vaccination against COVID-19 | |
| Before COVID-19 | 75 (9.4) |
| After COVID-19 | 590 (73.6) |
| Unvaccinated | 136 (17.0) |
| Variable | Whole Group [N (%)] | Vaccination Status [N (%)] | Vaccination Time [N (%)] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Vaccinated | Unvaccinated | p | Before COVID-19 | After COVID-19 | Unvaccinated | p | |||
| Age [M ± SD] | 53.5 ± 12.8 | 52.0 ± 13.7 | 53.9 ± 12.6 | 0.178 | 55.9 ± 14.1 | 52.0 ± 13.6 | 53.9 ± 12.6 | 0.176 | |
| Sex | Woman | 524 (65.4) | 437 (83.4) | 87 (16.6) | 0.696 | 59 (11.3) | 378 (72.1) | 87 (16.6) | 0.051 |
| Man | 277 (34.6) | 228 (82.3) | 49 (17.7) | 16 (5.8) | 212 (76.5) | 49 (17.7) | |||
| Chronic diseases | Hypertension | 354 (41.7) | 280 (83.8) | 54 (16.2) | 0.605 | 39 (11.6) | 241 (72.2) | 54 (16.2) | 0.161 |
| Hypercholesterolemia | 159 (19.9) | 131 (82.4) | 28 (17.6) | 0.812 | 115 (72.3) | 16 (10.1) | 28 (17.6) | 0.905 | |
| Diabetes | 81 (10.1) | 69 (85.2) | 12 (14.8) | 0.584 | 61 (75.3) | 8 (9.9) | 12 (14.8) | 0.858 | |
| Asthma | 87 (10.9) | 67 (77.0) | 20 (23.0) | 0.113 | 59 (67.8) | 8 (9.2) | 20 (23.0) | 0.282 | |
| COPD | 15 (1.9) | 12 (80.0) | 3 (20.0) | 0.753 | 11 (73.3) | 1 (6.7) | 3 (20.0) | 0.904 | |
| Thyroid diseases | 132 (16.5) | 111 (84.1) | 21 (15.9) | 0.720 | 97 (73.5) | 14 (10.6) | 21 (15.9) | 0.832 | |
| Whole Group [N (%)] | Vaccination Status | Size Effect | p | ||
|---|---|---|---|---|---|
| Vaccinated | Unvaccinated | ||||
| At least one symptom | 526 (65.7) | 435 (65.4) | 91 (66.9) | 0.011 | 0.737 |
| Fatigue | 291 (36.3) | 240 (36.1) | 51 (37.5) | 0.011 | 0.755 |
| Worse tolerance for exercise | 300 (37.5) | 248 (37.3) | 52 (38.2) | 0.007 | 0.836 |
| Taste and olfactory dysfunction | 62 (7.7) | 50 (7.5) | 12 (8.8) | 0.018 | 0.603 |
| Hair loss | 174 (21.7) | 139 (20.9) | 35 (25.7) | 0.044 | 0.212 |
| Skin lesions | 40 (5.0) | 32 (4.8) | 8 (5.9) | 0.018 | 0.602 |
| Excessive sweating | 134 (16.7) | 111 (16.7) | 23 (16.9) | 0.002 | 0.950 |
| Headache | 156 (19.5) | 116 (17.4) | 40 (29.4) | 0.113 | 0.001 |
| Memory and concentration problems | 291 (36.3) | 239 (35.9) | 52 (38.2) | 0.018 | 0.612 |
| Arthralgia | 50 (6.2) | 36 (5.4) | 14 (10.3) | 0.075 | 0.032 |
| Myalgia | 144 (18.0) | 121 (18.2) | 23 (16.9) | 0.012 | 0.722 |
| Palpitations | 187 (23.3) | 157 (23.6) | 30 (22.1) | 0.013 | 0.696 |
| Peripheral edema | 70 (8.7) | 55 (8.3) | 15 (11.0) | 0.036 | 0.299 |
| Newly diagnosed arterial hypertension | 102 (12.7) | 77 (11.6) | 25 (18.4) | 0.077 | 0.030 |
| Fainting/unconsciousness | 16 (2.0) | 16 (2.4) | 0 (0.0) | 0.065 | 0.136 |
| Dyspnea | 113 (14.1) | 92 (13.8) | 21 (15.4) | 0.017 | 0.623 |
| Cough | 85 (10.6) | 72 (10.8) | 13 (9.6) | 0.015 | 0.661 |
| Chest pain | 119 (14.9) | 100 (15.0) | 19 (14.0) | 0.012 | 0.749 |
| New chronic disease within 12 months from COVID-19 ending (N = 794) | 119 (14.9) | 101 (15.3) | 18 (13.3) | 0.021 | 0.555 |
| Hospitalization due to chronic disease (n = 798) | 85 (10.6) | 73 (11.0) | 12 (8.8) | 0.027 | 0.448 |
| Vaccination Status | Size Effect | p | |||
|---|---|---|---|---|---|
| Before COVID-19 | After COVID-19 | Unvaccinated | |||
| At least one symptom | 47 (62.7) | 388 (65.8) | 91 (66.9) | 0.022 | 0.821 |
| Fatigue | 29 (38.7) | 211 (35.8) | 51 (37.5) | 0.021 | 0.843 |
| Worse tolerance for exercise | 28 (37.3) | 220 (37.3) | 52 (38.2) | 0.007 | 0.973 |
| Taste and olfactory dysfunction | 5 (6.7) | 45 (7.6) | 12 (8.8) | 0.210 | 0.847 |
| Hair loss | 19 (25.3) | 120 (20.3) | 35 (25.7) | 0.056 | 0.282 |
| Skin lesions | 5 (6.7) | 27 (4.6) | 8 (5.9) | 0.033 | 0.642 |
| Excessive sweating | 12 (16.0) | 99 (16.8) | 23 (16.9) | 0.006 | 0.983 |
| Headache | 20 (26.7) | 96 (16.3) | 40 (29.4) | 0.137 | <0.001 |
| Memory and concentration problems | 26 (34.7) | 213 (36.1) | 52 (38.2) | 0.020 | 0.853 |
| Arthralgia | 17 (22.7) | 19 (3.2) | 14 (10.3) | 0.244 | <0.001 |
| Myalgia | 16 (21.3) | 105 (17.8) | 23 (16.9) | 0.029 | 0.707 |
| Palpitations | 13 (17.3) | 144 (24.4) | 30 (22.1) | 0.051 | 0.365 |
| Peripheral edema | 7 (9.3) | 48 (8.1) | 15 (11.0) | 0.038 | 0.549 |
| Newly diagnosed arterial hypertension | 10 (13.3) | 67 (11.4) | 25 (18.4) | 0.785 | 0.084 |
| Fainting/unconsciousness | 2 (2.7) | 14 (2.4) | 0 (0.0) | 0.0648 | 0.189 |
| Dyspnea | 12 (16.0) | 80 (13.6) | 21 (15.4) | 0.026 | 0.752 |
| Cough | 5 (6.7) | 67 (11.4) | 13 (9.6) | 0.046 | 0.421 |
| Chest pain | 9 (12.0) | 91 (15.4) | 19 (14.0) | 0.029 | 0.698 |
| New chronic disease within 12 months from COVID-19 ending (n = 794) | 7 (9.5) | 66 (11.2) | 12 (14.1) | 0.031 | 0.673 |
| Hospitalization due to chronic disease (n = 798) | 5 (6.8) | 96 (16.4) | 18 (13.3) | 0.081 | 0.076 |
| Vaccination | Vaccination before COVID-19 | Vaccination after COVID-19 | Unvaccinated |
|---|---|---|---|
| Headache | |||
| Vaccination before COVID-19 | – | 0.032 | <0.001 |
| Vaccination after COVID-19 | 0.032 | – | <0.001 |
| Unvaccinated | <0.001 | <0.001 | – |
| Arthralgy | |||
| Vaccination before COVID-19 | – | <0.001 | 0.031 |
| Vaccination after COVID-19 | <0.001 | – | <0.001 |
| Unvaccinated | 0.031 | <0.001 | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babicki, M.; Kapusta, J.; Pieniawska-Śmiech, K.; Kałuzińska-Kołat, Ż.; Kołat, D.; Mastalerz-Migas, A.; Jankowski, P.; Chudzik, M. Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register–12-Month Follow-Up. Viruses 2023, 15, 1370. https://doi.org/10.3390/v15061370
Babicki M, Kapusta J, Pieniawska-Śmiech K, Kałuzińska-Kołat Ż, Kołat D, Mastalerz-Migas A, Jankowski P, Chudzik M. Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register–12-Month Follow-Up. Viruses. 2023; 15(6):1370. https://doi.org/10.3390/v15061370
Chicago/Turabian StyleBabicki, Mateusz, Joanna Kapusta, Karolina Pieniawska-Śmiech, Żaneta Kałuzińska-Kołat, Damian Kołat, Agnieszka Mastalerz-Migas, Piotr Jankowski, and Michał Chudzik. 2023. "Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register–12-Month Follow-Up" Viruses 15, no. 6: 1370. https://doi.org/10.3390/v15061370
APA StyleBabicki, M., Kapusta, J., Pieniawska-Śmiech, K., Kałuzińska-Kołat, Ż., Kołat, D., Mastalerz-Migas, A., Jankowski, P., & Chudzik, M. (2023). Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register–12-Month Follow-Up. Viruses, 15(6), 1370. https://doi.org/10.3390/v15061370