Zika Virus and Arthritis/Arthralgia: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
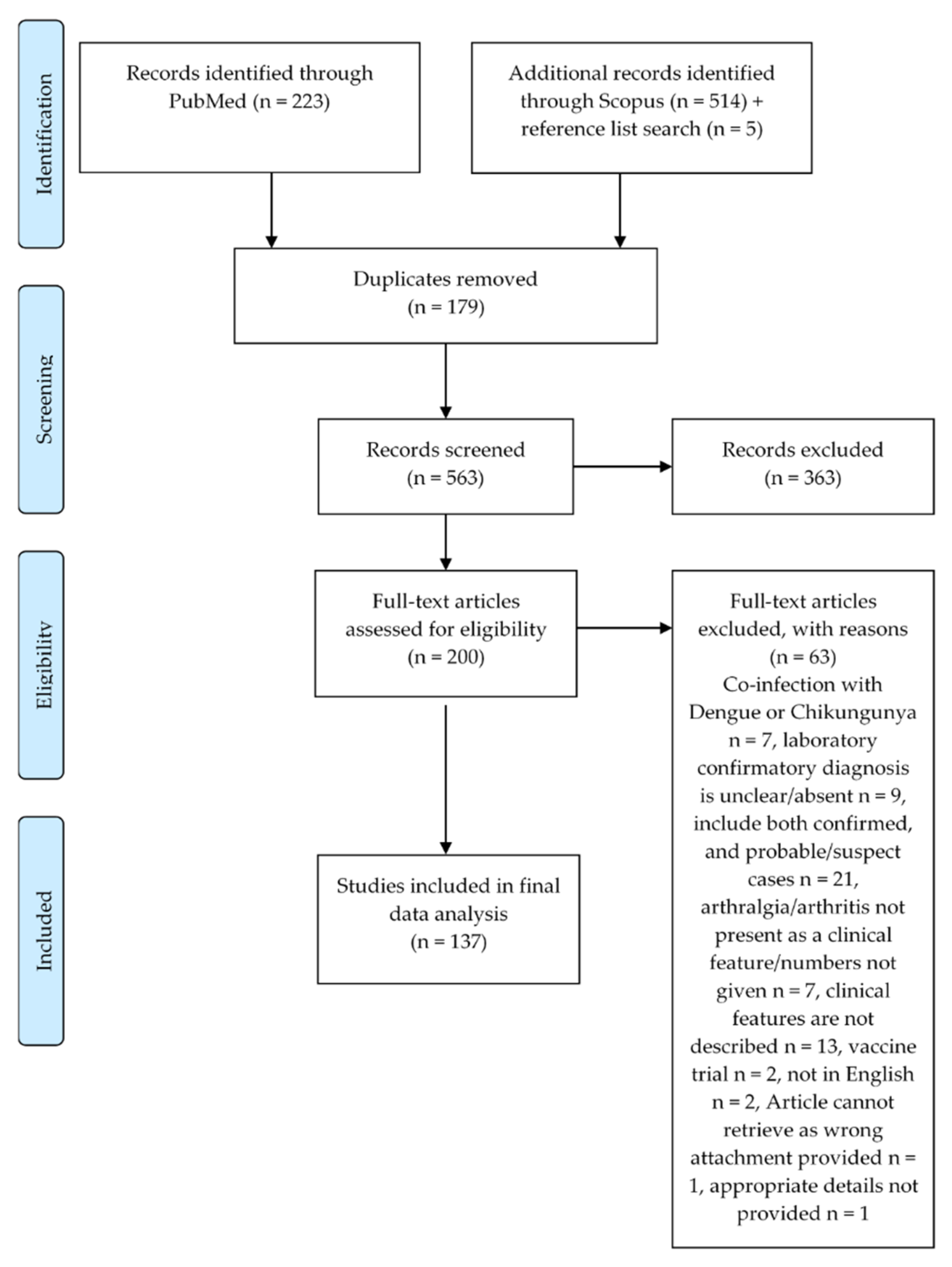
2.1. Search Strategy and Selection
2.2. Data Analysis
3. Results
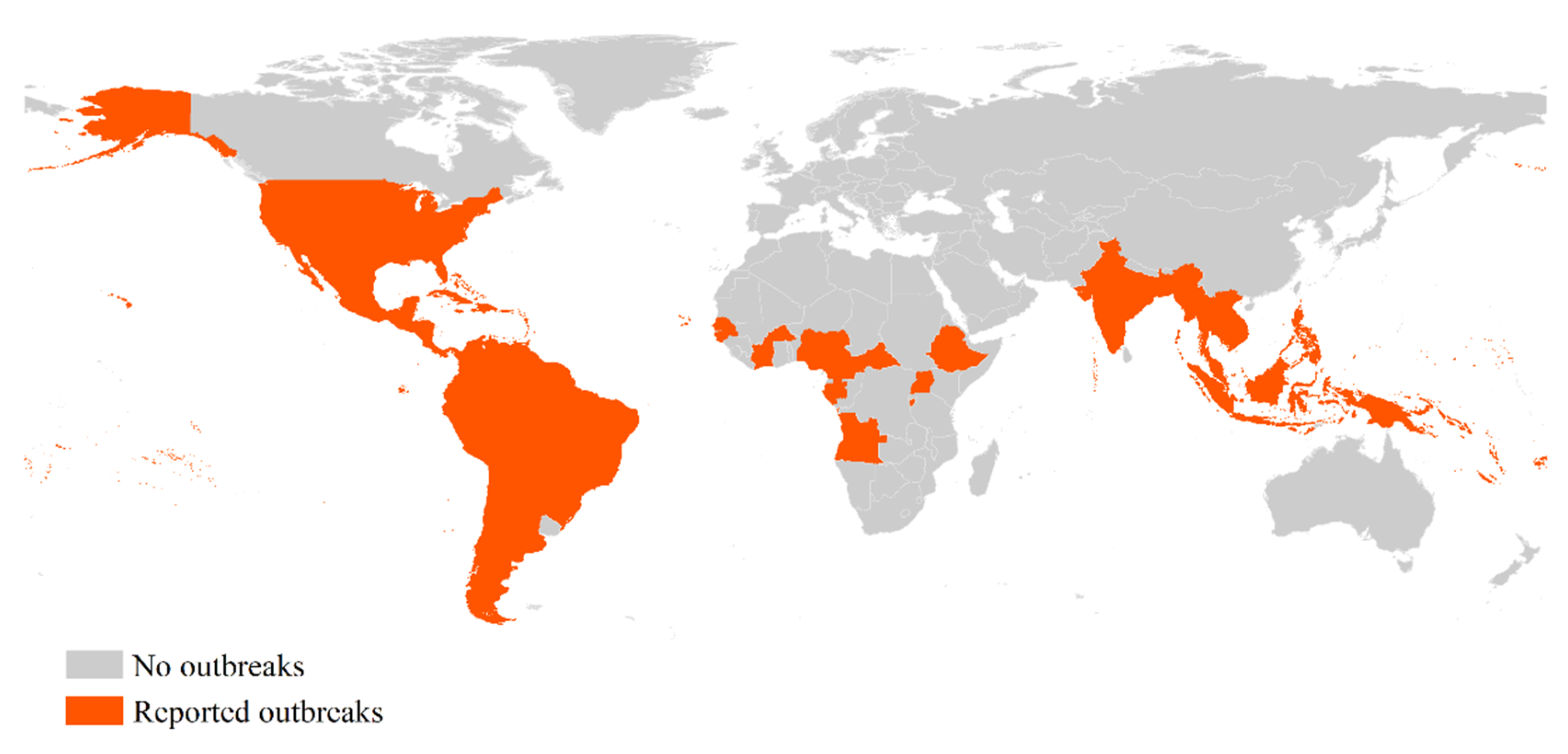
3.1. Regional Distribution of Records Reporting ZIKV with Joint Signs/Symptoms
3.2. Outbreaks of ZIKV with Joint Signs/Symptoms
3.3. Case Studies Reporting Confirmed ZIKV Cases with Joint Signs/Symptoms

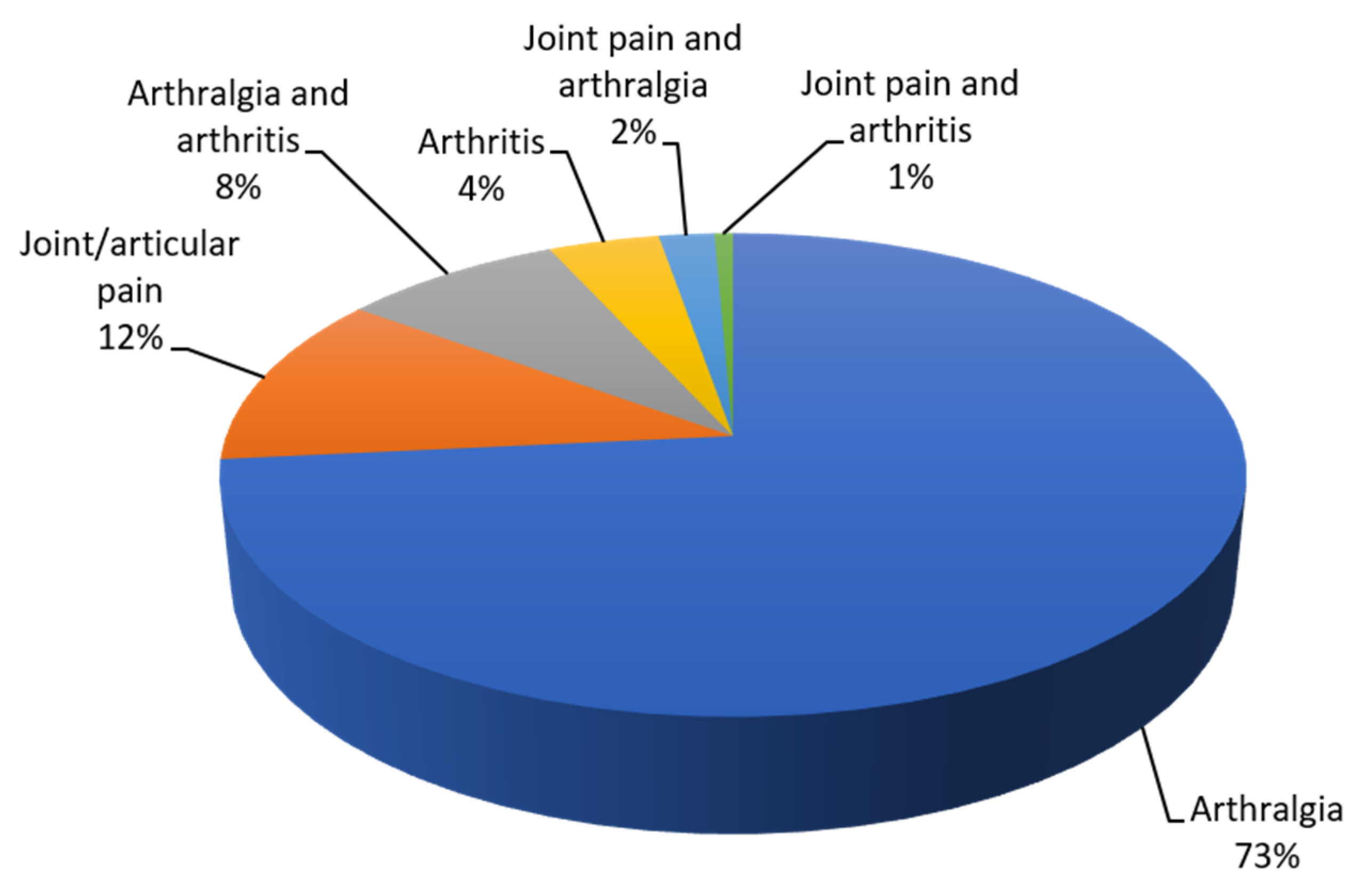
3.3.1. Arthralgia and Joint/Articular Pain
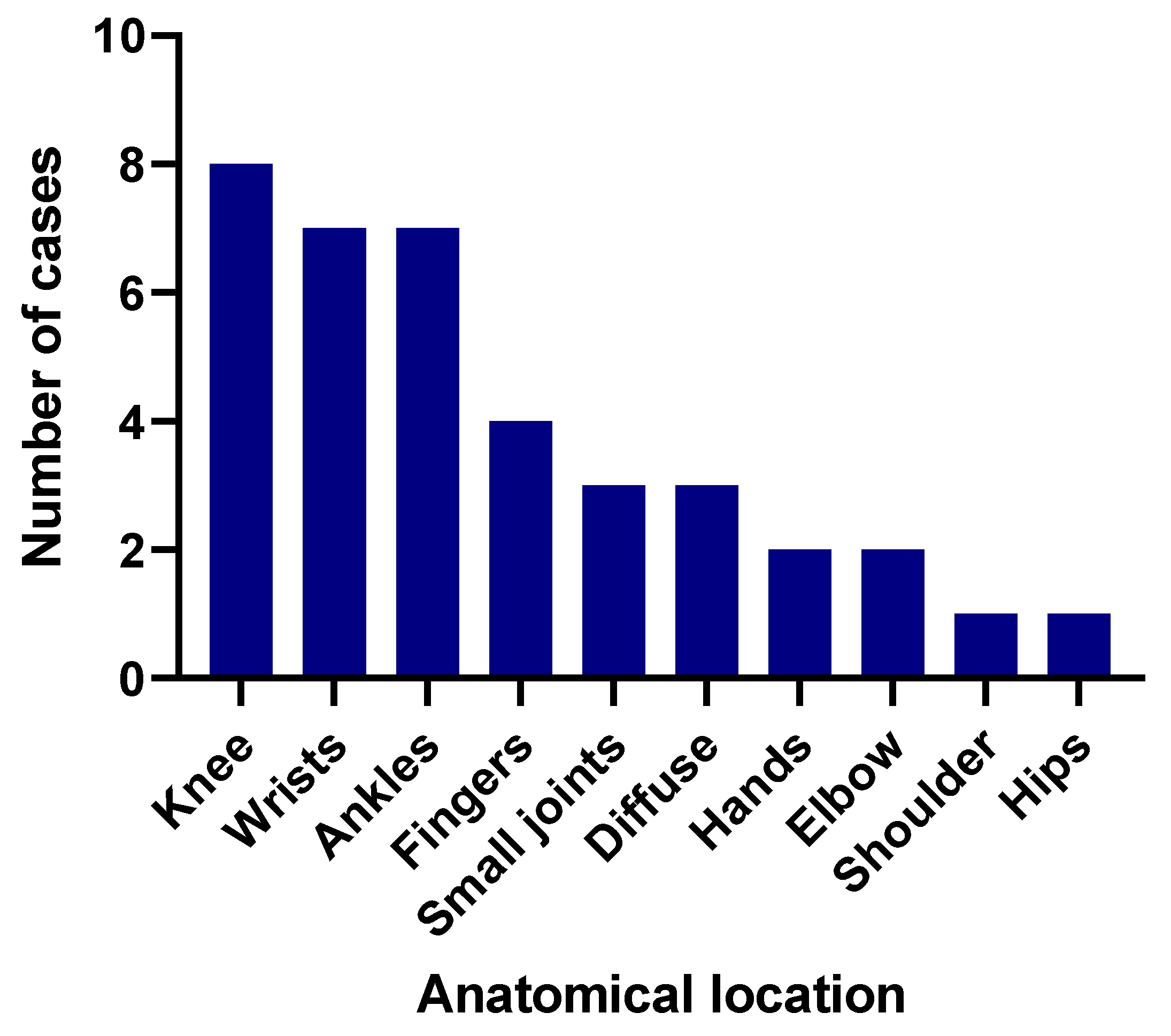
3.3.2. Arthritis
3.4. Population-Based Studies Reporting Confirmed ZIKV Cases with Joint Signs/Symptoms
3.4.1. Meta-Analysis for Pooled Prevalence of Joint Signs/Symptoms
3.4.2. Prevalence of Joint Signs/Symptoms during ZIKV Outbreaks Depends on the Geographic Location
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Weaver, S. C-102 Zika virus: History, evolution, transmission, emergence mechanisms, and activities of the GVN task force. Jaids J. Acquir. Immune Defic. Syndr. 2017, 74, 42. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Zika Virus [Internet]. National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Vector-Borne Diseases (DVBD). Available online: https://www.cdc.gov/zika/about/overview.html (accessed on 20 August 2020).
- Rather, I.A.; Lone, J.B.; Bajpai, V.K.; Paek, W.K.; Lim, J. Zika Virus: An Emerging Worldwide Threat. Front. Microbiol. 2017, 8, 1417. [Google Scholar] [CrossRef]
- Duffy, M.R.; Chen, T.-H.; Hancock, W.T.; Powers, A.M.; Kool, J.L.; Lanciotti, R.S.; Pretrick, M.; Marfel, M.; Holzbauer, S.M.; Dubray, C.; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N. Engl. J. Med. 2009, 360, 2536–2553. [Google Scholar] [CrossRef]
- Musso, D.; Gubler, D.J. Zika virus. Clin. Microbiol. Rev. 2016, 29, 487–524. [Google Scholar] [CrossRef]
- Aubry, M.; Teissier, A.; Huart, M.; Merceron, S.; Vanhomwegen, J.; Roche, C.; Vial, A.-L.; Teururai, S.; Sicard, S.; Paulous, S.; et al. Zika Virus Seroprevalence, French Polynesia, 2014–2015. Emerg. Infect. Dis. 2017, 23, 669–672. [Google Scholar] [CrossRef]
- Dasgupta, S.; Reagan-Steiner, S.; Goodenough, D.; Russell, K.; Tanner, M.; Lewis, L.; Petersen, E.E.; Powers, A.M.; Kniss, K.; Meaney-Delman, D. Patterns in Zika virus testing and infection, by report of symptoms and pregnancy status—United States, January 3–March 5, 2016. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 395–399. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fifth Meeting of the Emergency Committee under the International Health Regulations (2005) Regarding Microcephaly, other Neurological Disorders and Zika Virus 2016. Available online: https://www.who.int/en/news-room/detail/18-11-2016-fifth-meeting-of-the-emergency-committee-under-the-international-health-regulations-(2005)-regarding-microcephaly-other-neurological-disorders-and-zika-virus (accessed on 22 July 2020).
- World Health Organization. Countries and Territories with Current or Previous Zika Virus Transmission. 2019. Available online: https://www.who.int/emergencies/diseases/zika/countries-with-zika-and-vectors-table.pdf (accessed on 22 July 2020).
- ProMED-mail. PRO/AH/EDR> Zika virus (03): Americas, Asia research, observations. Int. Soc. Infect. Dis. 2020. Available online: https://outbreakwatch.blogspot.com/2018/02/proahedr-zika-virus-03-americas-asia.html (accessed on 20 August 2020).
- Flamand, C.; Fritzell, C.; Matheus, S.; Dueymes, M.; Carles, G.; Favre, A.; Enfissi, A.; Adde, A.; Demar, M.; Kazanji, M. The proportion of asymptomatic infections and spectrum of disease among pregnant women infected by Zika virus: Systematic monitoring in French Guiana, 2016. Euro Surveill. 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Zika Virus 2018 [updated 20 July 2018]. Available online: https://www.who.int/news-room/fact-sheets/detail/zika-virus (accessed on 5 August 2019).
- Ioos, S.; Mallet, H.P.; Goffart, I.L.; Gauthier, V.; Cardoso, T.; Herida, M. Current Zika virus epidemiology and recent epidemics. Médecine Mal. Infect. 2014, 44, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Zika Transmission [Internet]. National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Vector-Borne Diseases (DVBD). 2019. Available online: https://www.cdc.gov/zika/prevention/transmission-methods.html (accessed on 22 August 2020).
- Rosenthal, I.M. Arthritis and joint pain: IBD Resource Center, Crohn’s & Colitis Foundation. 2015 (06.08.2019). Available online: https://www.crohnscolitisfoundation.org/sites/default/files/legacy/assets/pdfs/emr/arthritiscomplications.pdf (accessed on 20 August 2020).
- Tiwari, V.; Bergman, M.J.; Viral Arthritis. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC; 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK531507/ (accessed on 2 July 2020).
- World Health Organization. Chikungunya [05.08.2019]. Available online: https://www.who.int/emergencies/diseases/chikungunya/en/ (accessed on 5 September 2019).
- Calabrese, L.H. Emerging viral infections and arthritis: The role of the rheumatologist. Nat. Clin. Pract. Rheumatol. 2007, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Zika Epidemiology Update- July 2019 [updated 02.07.2019]. Available online: https://www.who.int/emergencies/diseases/zika/zika-epidemiology-update-july-2019.pdf?ua=1 (accessed on 2 August 2019).
- Higgins, J.P.T.; Green, S.E. Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration. 2011. Available online: http://handbook.cochrane.org (accessed on 20 April 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- The Cochrane Collaboration. Review Manager (RevMan), 5.3 ed.; The Nordic Cochrane Centre: Copenhagen, Denmark; Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 20 July 2020).
- Moghadas, S.M.; Shoukat, A.; Espindola, A.L.; Pereira, R.S.; Abdirizak, F.; Laskowski, M.; Viboud, C.; Chowell, G. Asymptomatic transmission and the dynamics of Zika infection. Sci. Rep. 2017, 7, 5829. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Lal, S.K. Zika Virus: Transmission, Detection, Control, and Prevention. Front. Microbiol. 2017, 8, 110. [Google Scholar] [CrossRef] [PubMed]
- Petersen, L.R.; Jamieson, D.J.; Powers, A.M.; Honein, M.A. Zika virus. N. Engl. J. Med. 2016, 374, 1552–1563. [Google Scholar] [CrossRef] [PubMed]
- Brito, F.M.L.; de Brit, C.A.A.; Moreira, Á.J.P.; de Morais, M.M.Í.; Henriques-Souza, A.; Cordeiro, M.T.; de Azevedo Marques, E.T., Jr.; Pena, L.J. Guillain-Barré Syndrome, Acute Disseminated Encephalomyelitis and Encephalitis Associated with Zika Virus Infection in Brazil: Detection of Viral RNA and Isolation of Virus during Late Infection. Am. J. Trop. Med. Hyg. 2017, 97, 1405. [Google Scholar] [CrossRef] [PubMed]
- Rozé, B.; Najioullah, F.; Fergé, J.-L.; Dorléans, F.; Apetse, K.; Barnay, J.-L.; Daudens-Vaysse, E.; Brouste, Y.; Césaire, R.; Fagour, L. Guillain-Barré syndrome associated with Zika virus infection in Martinique in 2016: A prospective study. Clin. Infect. Dis. 2017, 65, 1462–1468. [Google Scholar] [CrossRef] [PubMed]
- Wikan, N.; Smith, D.R. Zika virus from a Southeast Asian perspective. Asian Pac. J. Trop. Med. 2017, 10, 1–5. [Google Scholar] [CrossRef]
- Borgherini, G.; Poubeau, P.; Jossaume, A.; Gouix, A.; Cotte, L.; Michault, A.; Arvin-Berod, C.; Paganin, F. Persistent arthralgia associated with Chikungunya Virus: A study of 88 adult patients on Reunion Island. Clin. Infect. Dis. 2008, 47, 469–475. [Google Scholar] [CrossRef]
- Simon, F.; Parola, P.; Grandadam, M.; Fourcade, S.; Oliver, M.; Brouqui, P.; Hance, P.; Kraemer, P.; Mohamed, A.A.; de Lamballerie, X. Chikungunya infection: An emerging rheumatism among travelers returned from Indian Ocean islands. Report of 47 cases. Medicine 2007, 86, 123–137. [Google Scholar] [CrossRef]
- Brighton, S.W.; Prozesky, O.W.; De La Harpe, A.L. Chikungunya virus infection-A retrospective study of 107 cases. S. Afr. Med. J. 1983, 68, 313–315. [Google Scholar]
- Jain, V.; Jyotsana; Chopra, A.; Mir, K.A.; Babu, C.; Kohli, S.; Kapur, P.; Manjavkar, S. Clinicobiochemical difference of patients presenting with Dengue and Chikungunya during post-monsoon season. J. Clinic. Diagn. Res. 2018, 12. [Google Scholar] [CrossRef]
- Perl, A. Mechanisms of viral pathogenesis in rheumatic disease. Ann. Rheum. Dis. 1999, 58, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Suhrbier, A. Rheumatic manifestations of chikungunya: Emerging concepts and interventions. Nat. Rev. Rheumatol. 2019, 15, 597–611. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.; Suhrbier, A. Paired serology for Ross River virus and Barmah Forest virus. Aust. J. Gen. Pract. 2019, 48, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Aggarwal, A. Joint involvement in Dengue fever. J. Gen. Pract. 2007, 19, 35–36. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included | Excluded | |
|---|---|---|
| Report type | Abstracts and full-length articles, conference proceedings, case reports, letters, brief reports, short communications, correspondence and editorials with novel data. English abstracts of full papers published in other languages were too included. | Opinions, letters, editorials and correspondence without new data; similar data or findings published under different titles or in different formats; review articles, book chapters, animal research or perspectives without new data. |
| Study design | Any randomised or non-randomised design. | Modelled data, review data. |
| Results Place and time of occurrence | Symptomatic ZIKV incidence in any human population during any time interval. | |
| Type of the occurrence | Imported cases, sporadic cases, case series or disease clusters; outbreaks and epidemics case reports. | |
| Person (number of cases, age and sex) of affected people | Only laboratory-confirmed human cases. | Laboratory-confirmed cases of co-infection of ZIKV with other diseases/infections (e.g. Dengue and Chikungunya) Missing or unclear laboratory-based method; suspected/probable ZIKV cases. |
| Meta-analysis | Articles describing epidemiological features of ZIKV outbreaks. Comparison of prevalence of arthralgia and arthritis in the studies that gave information about both manifestations separately in the same study. | Purposes other than epidemiological evaluation of ZIKV or restricted to defined population. |
| PubMed Search | Scopus Search |
|---|---|
| Search: ((((((arthralgia) OR (“joint pain”)) OR (rheumatology)) OR (“joint swelling”)) OR (“inflammatory joint pain”)) OR (arthritis)) AND (zika) Sort by: Most Recent (((((((“arthralgia”[MeSH Terms] OR “arthralgia”[All Fields]) OR “arthralgias”[All Fields]) OR “joint pain”[All Fields]) OR ((“rheumatology”[MeSH Terms] OR “rheumatology”[All Fields]) OR “rheumatology s”[All Fields])) OR “joint swelling”[All Fields]) OR “inflammatory joint pain”[All Fields]) OR (((“arthritis”[MeSH Terms] OR “arthritis”[All Fields]) OR “arthritides”[All Fields]) OR “polyarthritides”[All Fields])) AND ((((((“zika virus”[MeSH Terms] OR (“zika”[All Fields] AND “virus”[All Fields])) OR “zika virus”[All Fields]) OR “zika”[All Fields]) OR “zika virus infection”[MeSH Terms]) OR ((“zika”[All Fields] AND “virus”[All Fields]) AND “infection”[All Fields])) OR “zika virus infection”[All Fields]) Translations arthralgia: “arthralgia”[MeSH Terms] OR “arthralgia”[All Fields] OR “arthralgias”[All Fields] rheumatology: “rheumatology”[MeSH Terms] OR “rheumatology”[All Fields] OR “rheumatology’s”[All Fields] arthritis: “arthritis”[MeSH Terms] OR “arthritis”[All Fields] OR “arthritides”[All Fields] OR “polyarthritides”[All Fields] zika: “zika virus”[MeSH Terms] OR (“zika”[All Fields] AND “virus”[All Fields]) OR “zika virus”[All Fields] OR “zika”[All Fields] OR “zika virus infection”[MeSH Terms] OR (“zika”[All Fields] AND “virus”[All Fields] AND “infection”[All Fields]) OR “zika virus infection”[All Fields] | TITLE-ABS-KEY (arthralgia OR arthritis OR “joint pain” OR rheumatology OR “joint swelling” OR “inflammatory joint pain” AND zika) |
| Region | Number of Articles | Countries Reporting Confirmed ZIKV Cases with Joint Symptoms |
|---|---|---|
| African Region | 1 | Ghana |
| Region of the Americas | 96 | Brazil, Canada, Colombia, Cuba, Dominican Republic, French Guiana, Honduras, Martinique, Mexico, Nicaragua, Panama, Peru, Puerto Rico, Suriname, Trinidad and Tobago, United States, Venezuela |
| European Region | 27 | Belgium, Croatia, France, Germany, Italy, Netherlands, Norway, Portugal, Russia, Spain, Switzerland, Turkey, United Kingdom |
| Eastern Mediterranean Region | 0 | |
| Western Pacific Region | 5 | French Polynesia, Micronesia, New Caledonia, New Zealand |
| South-East Asia Region | 8 | Indonesia, Japan, Korea, Singapore, Viet Nam Thailand |
| Authors | Sign/Symptom | Reporter | Duration (Days) | Number of Cases | Joint(s) Affected | Country of Report | Age (Years) | Sex | Comorbidities | Diagnosed by | Source |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bachiller-Luque et al., 2016 | Arthralgia and synovitis | Clinician | 5 | 1 | Fingers, right knee, ankle and elbow | Spain | 49 | Male | Irritable bowel syndrome, hypertension, dyslipidemia | RT-PCR | Imported |
| Penot et al., 2017 | Arthritis, joints pain and swelling | Clinician | >10 (all cases) | 3 | Case 2—ankles and phalanges. Case 3—bilateral and symmetrical wrists, ankles and phalanges. Case 4—bilateral knees | France | 36, 30, 39 | All are female | Patient 3- Previously healthy Patient 4- hypothyroidism and non-treated rheumatoid polyarthritis | RT-PCR | Imported |
| Fabrizius et al., 2016 | Effusion with tenderness to palpation | Clinician | 1 | Finger joints | United States | 44 | Male | Previously healthy | RT-PCR | Imported | |
| Kulkarni et al., 2016 | Mild synovitis | Clinician | 1 | Metacarpophalangeal and proximal interphalangeal joints bilaterally | United States | 42 | Female | Previously healthy | IgM and Zika virus PRNT | Imported | |
| Rozé et al., 2016 | Peripheral arthritis | Clinician | 1 | Peripheral arthritis | Martinique | Late 70s | Not given | RT-PCR | Local | ||
| Nicastri et al., 2016 | Bilateral wrists swelling | Clinician | 1 | Bilateral wrists | Italy | 74 | Male | RT-PCR, serology, neutralisation | Imported | ||
| Zammarchi et al., 2015 | Arthralgia and ankle oedema | Patient | 2 | Ankle | Italy | Early30s | Male & Female | RT-PCR/ IgG/IgM | Imported | ||
| Harrower et al., 2016 | Arthralgia and ankle oedema | Patient | 1 | Ankle | New Zealand | 51 | Male | RT-PCR | Imported | ||
| Arsuaga et al., 2016 | Arthritis | Patient | 7, 8 | 2 | Ankles and wrists | Spain | 53, 51 | Male & Female | RT-PCR | Imported | |
| Cavalcanti et al., 2017 | Articular edema | Patient | 1 | Fingers and toes | Brazil | 42 | Female | RT-PCR | Local | ||
| Vinhaes et al., 2017 | Oedema in wrists | Patient | 2 | 1 | Wrists | Brazil | 23 | Male | IgM, PRNT | Local | |
| Zonneveld et al., 2016 | Arthritis | Patient | 1 | Not given | Suriname | 61 | Male | Hypertension | RT-PCR | Local | |
| Díaz-Quiñonez et al., 2016 | Arthritis | Patient | 1 | Not given | Mexico | 26 | Male | RT-PCR | Imported |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wimalasiri-Yapa, B.M.C.R.; Yapa, H.E.; Huang, X.; Hafner, L.M.; Kenna, T.J.; Frentiu, F.D. Zika Virus and Arthritis/Arthralgia: A Systematic Review and Meta-Analysis. Viruses 2020, 12, 1137. https://doi.org/10.3390/v12101137
Wimalasiri-Yapa BMCR, Yapa HE, Huang X, Hafner LM, Kenna TJ, Frentiu FD. Zika Virus and Arthritis/Arthralgia: A Systematic Review and Meta-Analysis. Viruses. 2020; 12(10):1137. https://doi.org/10.3390/v12101137
Chicago/Turabian StyleWimalasiri-Yapa, B.M.C.R., Harith E. Yapa, Xiaodong Huang, Louise M. Hafner, Tony J. Kenna, and Francesca D. Frentiu. 2020. "Zika Virus and Arthritis/Arthralgia: A Systematic Review and Meta-Analysis" Viruses 12, no. 10: 1137. https://doi.org/10.3390/v12101137
APA StyleWimalasiri-Yapa, B. M. C. R., Yapa, H. E., Huang, X., Hafner, L. M., Kenna, T. J., & Frentiu, F. D. (2020). Zika Virus and Arthritis/Arthralgia: A Systematic Review and Meta-Analysis. Viruses, 12(10), 1137. https://doi.org/10.3390/v12101137