
Ensemble Transfer Learning for Distinguishing Cognitively Normal and Mild Cognitive Impairment Patients Using MRI

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
- This paper presents a neural network framework with two ensemble methods, i.e., weighted averaging and simple averaging, on the OASIS-3 dataset for AD diagnosis.
- Fine tuning of eight different models such as VGG19, DenseNet201, EfficientNetV2S, MobileNet, ResNet152, InceptionV3, NASNetLarge, and Xception achieved a higher accuracy in comparison to the state of the art.
- This paper conducts a qualitative evaluation in the result variations of pre-trained models between cropping and without cropping of MRI images.
2. Related Works
3. Methodology
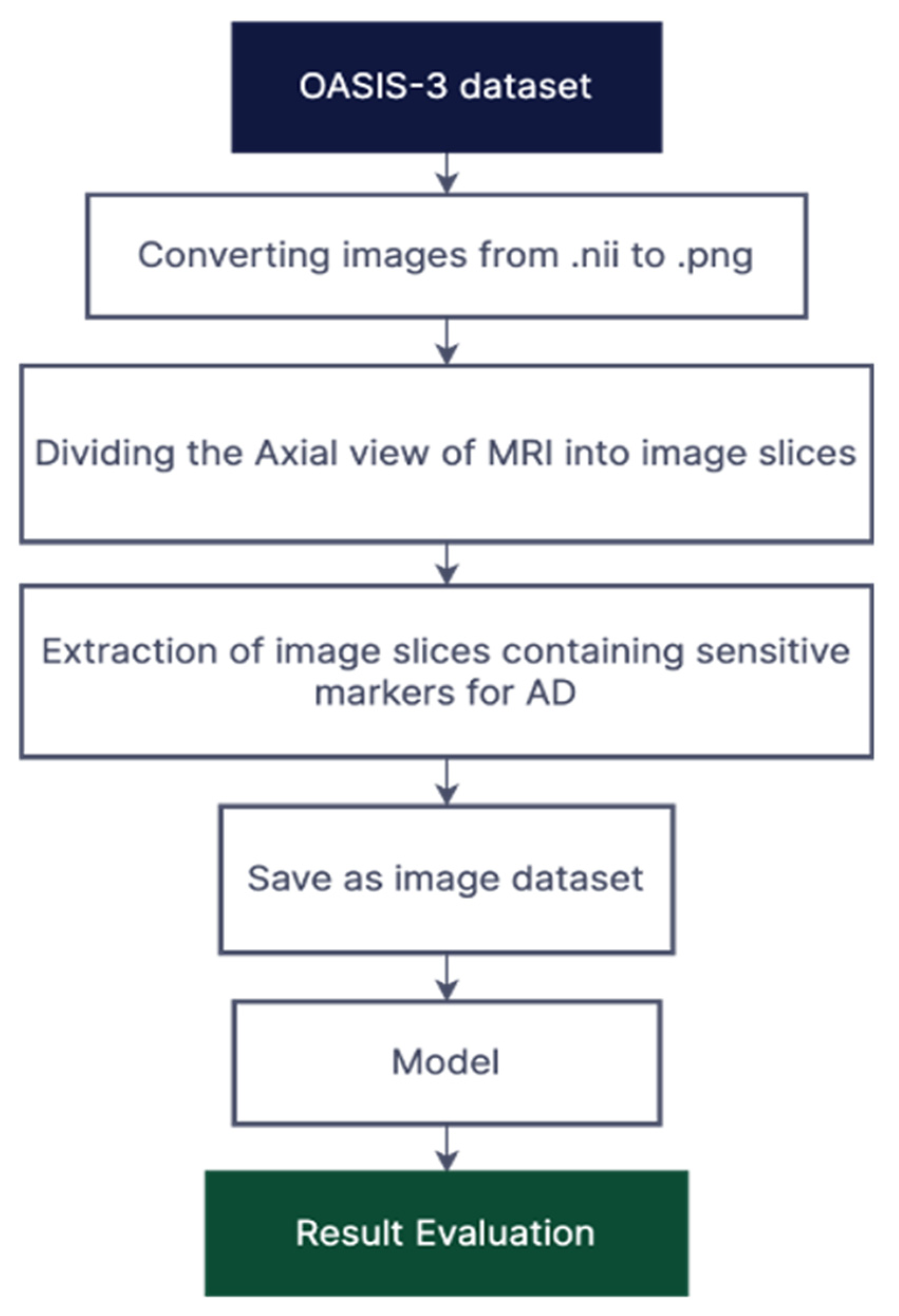
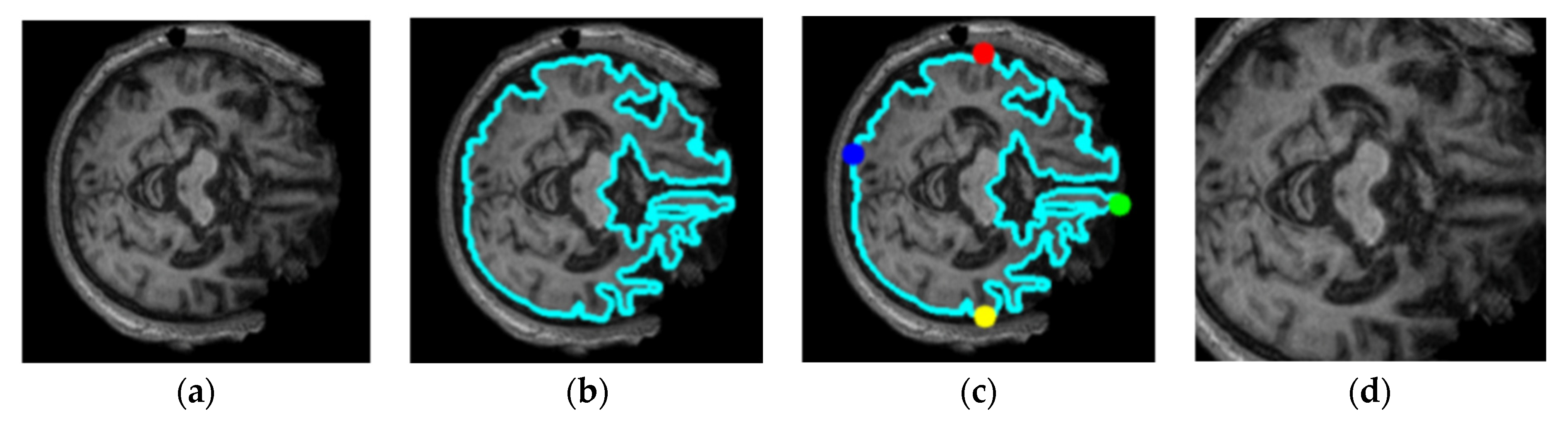
3.1. Dataset Pre-Processing
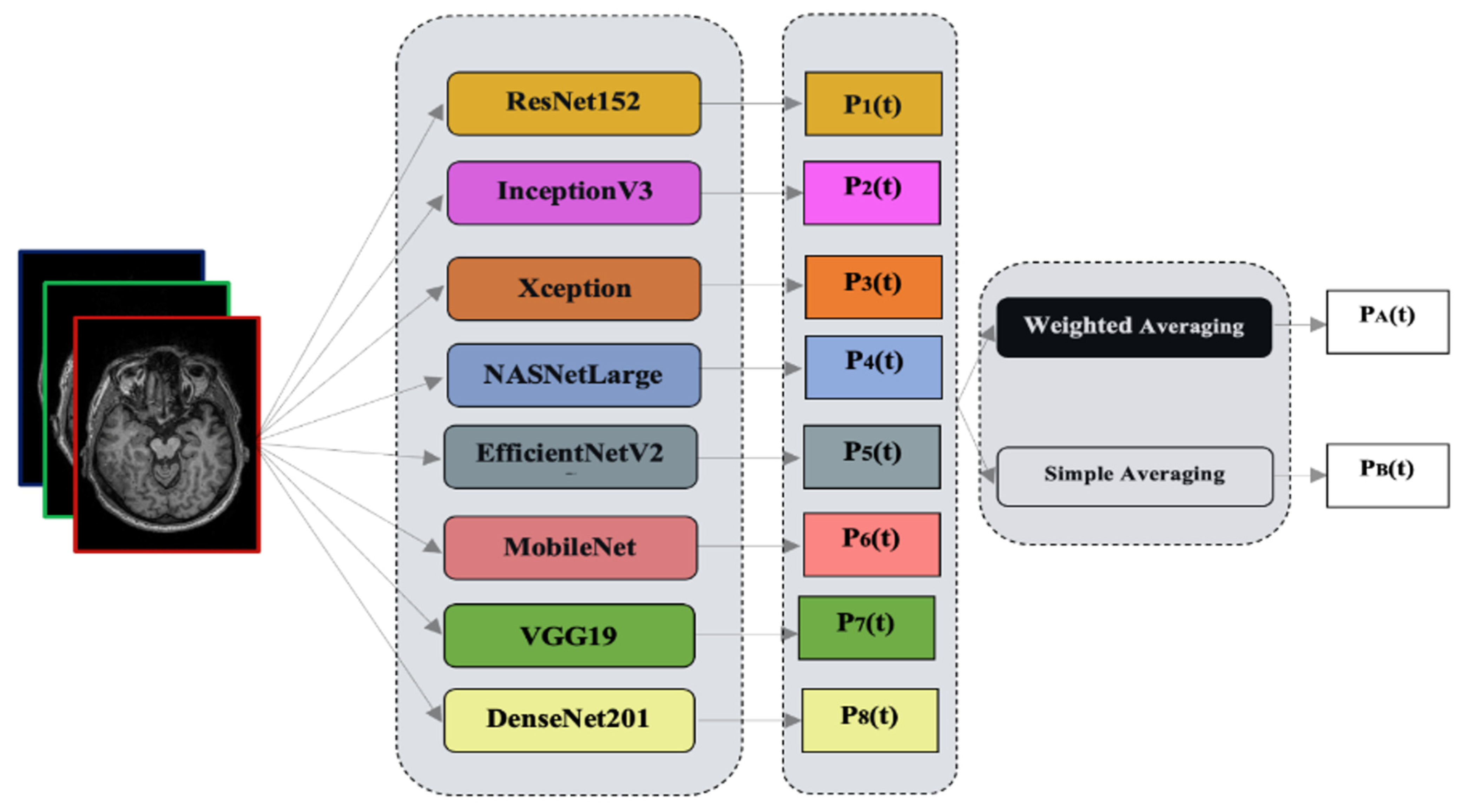
3.2. Ensemble Learning
4. Experimentation and Results
4.1. Evaluation Indicators
4.2. Model Selection
4.3. Model Ensembling Strategy
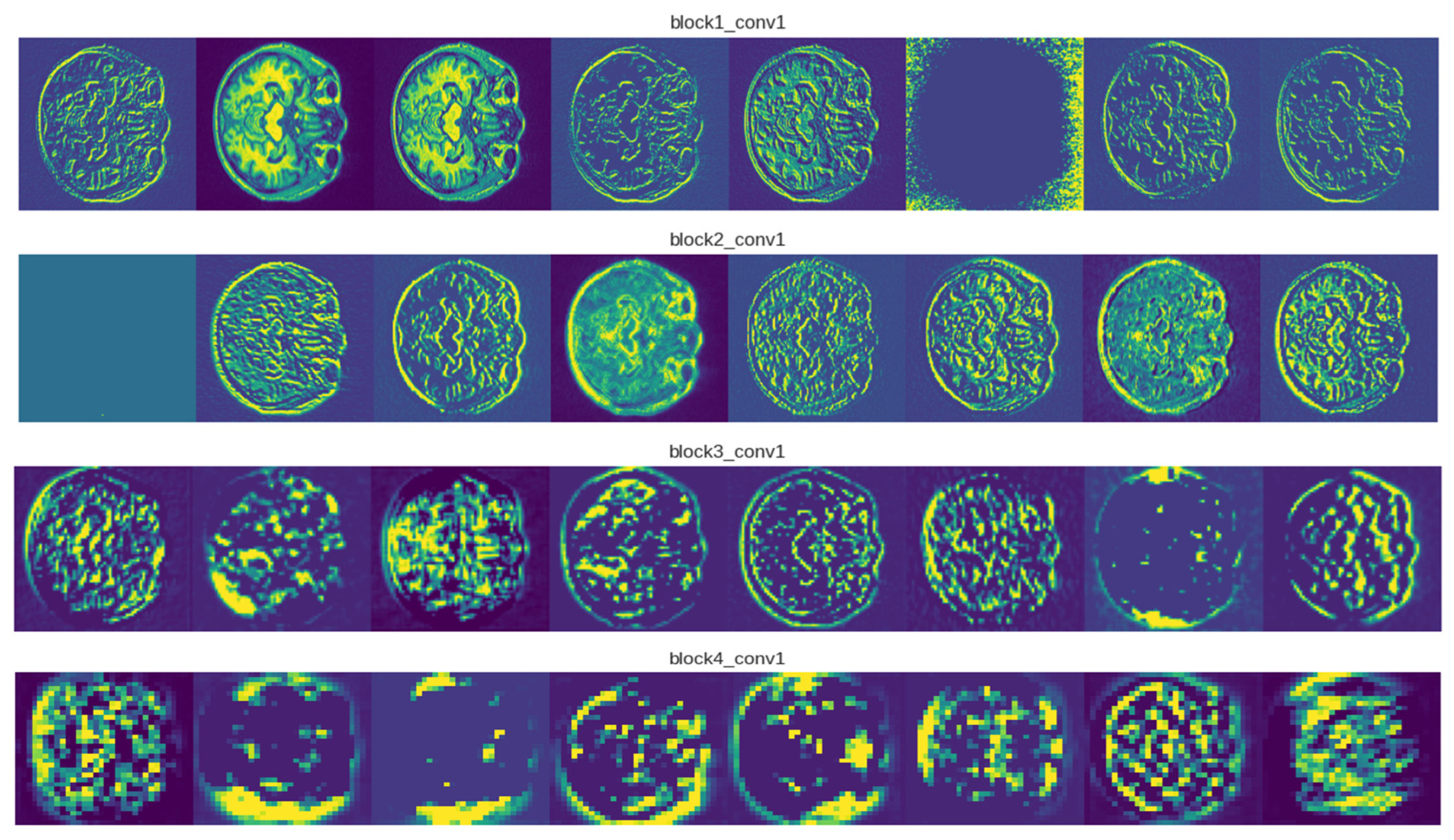
4.4. Visualizations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Alzheimer’s Association. 2022 Alzheimer’s Disease Facts and Figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef] [PubMed]
- Thushara, A. An Efficient Alzheimer’s Disease Prediction Based on MEPC-SSC Segmentation and Momentum Geo-Transient MLPs. Comput. Biol. Med. 2022, 151, 106247. [Google Scholar] [CrossRef] [PubMed]
- Thapa, S.; Singh, P.; Jain, D.K.; Bharill, N.; Gupta, A.; Prasad, M. Data-Driven Approach Based on Feature Selection Technique for Early Diagnosis of Alzheimer’s Disease. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar]
- Adhikari, S.; Thapa, S.; Naseem, U.; Singh, P.; Huo, H.; Bharathy, G.; Prasad, M. Exploiting Linguistic Information from Nepali Transcripts for Early Detection of Alzheimer’s Disease Using Natural Language Processing and Machine Learning Techniques. Int. J. Hum. Comput. Stud. 2022, 160, 102761. [Google Scholar] [CrossRef]
- Tanveer, M.; Richhariya, B.; Khan, R.U.; Rashid, A.H.; Khanna, P.; Prasad, M.; Lin, C.T. Machine Learning Techniques for the Diagnosis of Alzheimer’s Disease. ACM Trans. Multimed. Comput. Commun. Appl. 2020, 16, 1–35. [Google Scholar] [CrossRef]
- Tremblay-Mercier, J.; Madjar, C.; Das, S.; Pichet Binette, A.; Dyke, S.O.M.; Étienne, P.; Lafaille-Magnan, M.-E.; Remz, J.; Bellec, P.; Louis Collins, D.; et al. Open Science Datasets from PREVENT-AD, a Longitudinal Cohort of Pre-Symptomatic Alzheimer’s Disease. NeuroImage Clin. 2021, 31, 102733. [Google Scholar] [CrossRef] [PubMed]
- Poulin, S.P.; Dautoff, R.; Morris, J.C.; Barrett, L.F.; Dickerson, B.C. Amygdala Atrophy Is Prominent in Early Alzheimer’s Disease and Relates to Symptom Severity. Psychiatry Res. Neuroimaging 2011, 194, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Westman, E.; Cavallin, L.; Muehlboeck, J.-S.; Zhang, Y.; Mecocci, P.; Vellas, B.; Tsolaki, M.; Kłoszewska, I.; Soininen, H.; Spenger, C.; et al. Sensitivity and Specificity of Medial Temporal Lobe Visual Ratings and Multivariate Regional MRI Classification in Alzheimer’s Disease. PLoS ONE 2011, 6, e22506. [Google Scholar] [CrossRef]
- Gupta, A.; Kumar, D.; Verma, H.; Tanveer, M.; Javier, A.P.; Lin, C.-T.; Prasad, M. Recognition of Multi-Cognitive Tasks from EEG Signals Using EMD Methods. Neural Comput. Appl. 2022. [Google Scholar] [CrossRef]
- Kiani, M.; Andreu-Perez, J.; Hagras, H.; Papageorgiou, E.I.; Prasad, M.; Lin, C.-T. Effective Brain Connectivity for FNIRS With Fuzzy Cognitive Maps in Neuroergonomics. IEEE Trans. Cogn. Dev. Syst. 2022, 14, 50–63. [Google Scholar] [CrossRef]
- Ding, W.; Lin, C.-T.; Prasad, M. Hierarchical Co-Evolutionary Clustering Tree-Based Rough Feature Game Equilibrium Selection and Its Application in Neonatal Cerebral Cortex MRI. Expert Syst. Appl. 2018, 101, 243–257. [Google Scholar] [CrossRef]
- Lazli, L.; Boukadoum, M.; Mohamed, O.A. A Survey on Computer-Aided Diagnosis of Brain Disorders through MRI Based on Machine Learning and Data Mining Methodologies with an Emphasis on Alzheimer Disease Diagnosis and the Contribution of the Multimodal Fusion. Appl. Sci. 2020, 10, 1894. [Google Scholar] [CrossRef]
- Chen, Z.S.; Kulkarni, P.; Galatzer-Levy, I.R.; Bigio, B.; Nasca, C.; Zhang, Y. Modern Views of Machine Learning for Precision Psychiatry. Patterns 2022, 3, 100602. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, H.; Adeli, E.; Chen, X.; Liu, M.; Shen, D. Multiview Feature Learning With Multiatlas-Based Functional Connectivity Networks for MCI Diagnosis. IEEE Trans. Cybern. 2022, 52, 6822–6833. [Google Scholar] [CrossRef]
- Anh, N.; Prasad, M.; Srikanth, N.; Sundaram, S. Wave Forecasting Using Meta-Cognitive Interval Type-2 Fuzzy Inference System. Procedia Comput. Sci. 2018, 144, 33–41. [Google Scholar] [CrossRef]
- Za’in, C.; Pratama, M.; Prasad, M.; Puthal, D.; Lim, C.P.; Seera, M. Motor Fault Detection and Diagnosis Based on a Meta-Cognitive Random Vector Functional Link Network. In Fault Diagnosis of Hybrid Dynamic and Complex Systems; Springer International Publishing: Cham, Switzerland, 2018; pp. 15–44. [Google Scholar]
- Castellazzi, G.; Cuzzoni, M.G.; Cotta Ramusino, M.; Martinelli, D.; Denaro, F.; Ricciardi, A.; Vitali, P.; Anzalone, N.; Bernini, S.; Palesi, F.; et al. A Machine Learning Approach for the Differential Diagnosis of Alzheimer and Vascular Dementia Fed by MRI Selected Features. Front. Neuroinform. 2020, 14. [Google Scholar] [CrossRef] [PubMed]
- Battineni, G.; Chintalapudi, N.; Amenta, F.; Traini, E. A Comprehensive Machine-Learning Model Applied to Magnetic Resonance Imaging (MRI) to Predict Alzheimer’s Disease (AD) in Older Subjects. J. Clin. Med. 2020, 9, 2146. [Google Scholar] [CrossRef] [PubMed]
- Alickovic, E.; Subasi, A. Automatic Detection of Alzheimer Disease Based on Histogram and Random Forest; Springer: Berlin/Heidelberg, Germany, 2020; pp. 91–96. [Google Scholar]
- Bandyopadhyay, A.; Ghosh, S.; Bose, M.; Singh, A.; Othmani, A.; Santosh, K. Alzheimer’s Disease Detection Using Ensemble Learning and Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 2023; pp. 12–21. [Google Scholar]
- Wang, H.; Shen, Y.; Wang, S.; Xiao, T.; Deng, L.; Wang, X.; Zhao, X. Ensemble of 3D Densely Connected Convolutional Network for Diagnosis of Mild Cognitive Impairment and Alzheimer’s Disease. Neurocomputing 2019, 333, 145–156. [Google Scholar] [CrossRef]
- Ortiz, A.; Munilla, J.; Górriz, J.M.; Ramírez, J. Ensembles of Deep Learning Architectures for the Early Diagnosis of the Alzheimer’s Disease. Int. J. Neural Syst. 2016, 26, 1650025. [Google Scholar] [CrossRef]
- Tanveer, M.; Rashid, A.H.; Ganaie, M.A.; Reza, M.; Razzak, I.; Hua, K.-L. Classification of Alzheimer’s Disease Using Ensemble of Deep Neural Networks Trained Through Transfer Learning. IEEE J. Biomed. Health Inform. 2022, 26, 1453–1463. [Google Scholar] [CrossRef]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Rich Feature Hierarchies for Accurate Object Detection and Semantic Segmentation. arXiv 2013, arXiv:1311.2524. [Google Scholar]
- Yosinski, J.; Clune, J.; Bengio, Y.; Lipson, H. How Transferable Are Features in Deep Neural Networks? arXiv 2014, arXiv:1411.1792. [Google Scholar]
- Balaji, P.; Chaurasia, M.A.; Bilfaqih, S.M.; Muniasamy, A.; Alsid, L.E.G. Hybridized Deep Learning Approach for Detecting Alzheimer’s Disease. Biomedicines 2023, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- Pei, Z.; Wan, Z.; Zhang, Y.; Wang, M.; Leng, C.; Yang, Y.-H. Multi-Scale Attention-Based Pseudo-3D Convolution Neural Network for Alzheimer’s Disease Diagnosis Using Structural MRI. Pattern Recognit. 2022, 131, 108825. [Google Scholar] [CrossRef]
- Liu, M.; Cheng, D.; Wang, K.; Wang, Y. Multi-Modality Cascaded Convolutional Neural Networks for Alzheimer’s Disease Diagnosis. Neuroinformatics 2018, 16, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Abdou, M.A. Literature Review: Efficient Deep Neural Networks Techniques for Medical Image Analysis. Neural Comput. Appl. 2022, 34, 5791–5812. [Google Scholar] [CrossRef]
- Zhang, T.; Shi, M. Multi-Modal Neuroimaging Feature Fusion for Diagnosis of Alzheimer’s Disease. J. Neurosci. Methods 2020, 341, 108795. [Google Scholar] [CrossRef]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R.; Misra, S. Explainable Deep-Learning-Based Diagnosis of Alzheimer’s Disease Using Multimodal Input Fusion of PET and MRI Images. J. Med. Biol. Eng. 2023, 43, 291–302. [Google Scholar] [CrossRef]
- Yu, W.; Lei, B.; Ng, M.K.; Cheung, A.C.; Shen, Y.; Wang, S. Tensorizing GAN With High-Order Pooling for Alzheimer’s Disease Assessment. IEEE Trans. Neural Netw. Learn. Syst. 2022, 33, 4945–4959. [Google Scholar] [CrossRef]
- Shi, J.; Zheng, X.; Li, Y.; Zhang, Q.; Ying, S. Multimodal Neuroimaging Feature Learning With Multimodal Stacked Deep Polynomial Networks for Diagnosis of Alzheimer’s Disease. IEEE J. Biomed. Health Inform. 2018, 22, 173–183. [Google Scholar] [CrossRef]
- Zhang, X.; Yao, L.; Wang, X.; Monaghan, J.; McAlpine, D.; Zhang, Y. A Survey on Deep Learning-Based Non-Invasive Brain Signals: Recent Advances and New Frontiers. J. Neural Eng. 2021, 18, 031002. [Google Scholar] [CrossRef]
- Suk, H.-I.; Lee, S.-W.; Shen, D. Deep Ensemble Learning of Sparse Regression Models for Brain Disease Diagnosis. Med. Image Anal. 2017, 37, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Van Halm-Lutterodt, N.; Tang, H.; Mecum, A.; Mesregah, M.K.; Ma, Y.; Li, H.; Zhang, F.; Wu, Z.; Yao, E.; et al. Automated MRI-Based Deep Learning Model for Detection of Alzheimer’s Disease Process. Int. J. Neural Syst. 2020, 30, 2050032. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, H.; Shen, Y.; Wang, X. Automatic Recognition of Mild Cognitive Impairment and Alzheimers Disease Using Ensemble Based 3D Densely Connected Convolutional Networks. In Proceedings of the 2018 17th IEEE International Conference on Machine Learning and Applications (ICMLA), Orlando, FL, USA, 17–20 December 2018; pp. 517–523. [Google Scholar]
- Jain, R.; Jain, N.; Aggarwal, A.; Hemanth, D.J. Convolutional Neural Network Based Alzheimer’s Disease Classification from Magnetic Resonance Brain Images. Cogn. Syst. Res. 2019, 57, 147–159. [Google Scholar] [CrossRef]
- Zhu, W.; Sun, L.; Huang, J.; Han, L.; Zhang, D. Dual Attention Multi-Instance Deep Learning for Alzheimer’s Disease Diagnosis With Structural MRI. IEEE Trans. Med. Imaging 2021, 40, 2354–2366. [Google Scholar] [CrossRef]
- Chen, Y.; Shi, B.; Wang, Z.; Zhang, P.; Smith, C.D.; Liu, J. Hippocampus Segmentation through Multi-View Ensemble ConvNets. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 192–196. [Google Scholar]
- Ataloglou, D.; Dimou, A.; Zarpalas, D.; Daras, P. Fast and Precise Hippocampus Segmentation Through Deep Convolutional Neural Network Ensembles and Transfer Learning. Neuroinformatics 2019, 17, 563–582. [Google Scholar] [CrossRef]
- Zhang, D.; Shen, D. Semi-Supervised Multimodal Classification of Alzheimer’s Disease. In Proceedings of the 2011 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Chicago, IL, USA, 30 March–2 April 2011; pp. 1628–1631. [Google Scholar]
- Liu, S.; Liu, S.; Cai, W.; Che, H.; Pujol, S.; Kikinis, R.; Feng, D.; Fulham, M.J. ADNI Multimodal Neuroimaging Feature Learning for Multiclass Diagnosis of Alzheimer’s Disease. IEEE Trans. Biomed. Eng. 2015, 62, 1132–1140. [Google Scholar] [CrossRef]
- Liu, C.; Huang, F.; Qiu, A. Monte Carlo Ensemble Neural Network for the Diagnosis of Alzheimer’s Disease. Neural Netw. 2023, 159, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, X.; Wang, P.; Xia, Y.; Ye, Q. Multi-Source Transfer Learning via Ensemble Approach for Initial Diagnosis of Alzheimer’s Disease. IEEE J. Transl. Eng. Health Med. 2020, 8, 1–10. [Google Scholar] [CrossRef]
- LaMontagne, P.J.; Benzinger, T.L.S.; Morris, J.C.; Keefe, S.; Hornbeck, R.; Xiong, C.; Grant, E.; Hassenstab, J.; Moulder, K.; Vlassenko, A.G.; et al. OASIS-3: Longitudinal Neuroimaging, Clinical, and Cognitive Dataset for Normal Aging and Alzheimer Disease. medRxiv 2019. [Google Scholar] [CrossRef]
- Ganaie, M.A.; Hu, M.; Malik, A.K.; Tanveer, M.; Suganthan, P.N. Ensemble Deep Learning: A Review. Eng. Appl. Artif. Intell. 2022, 115, 105151. [Google Scholar] [CrossRef]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. MobileNets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. arXiv 2016, arXiv:1608.06993. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. arXiv 2015, arXiv:1512.03385. [Google Scholar]
- Tan, M.; Le, Q.V. EfficientNetV2: Smaller Models and Faster Training. arXiv 2021, arXiv:2104.00298. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. arXiv 2015, arXiv:1512.00567. [Google Scholar]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning Transferable Architectures for Scalable Image Recognition. arXiv 2017, arXiv:1707.07012. [Google Scholar]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. arXiv 2016, arXiv:1610.02357. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | Accuracy | Specificity | Sensitivity | AUC |
|---|---|---|---|---|
| MobileNet [48] | 0.922 | 0.927 | 0.913 | 0.920 |
| VGG19 [49] | 0.977 | 0.949 | 0.961 | 0.958 |
| DenseNet201 [50] | 0.961 | 0.965 | 0.958 | 0.962 |
| ResNet152 [51] | 0.946 | 0.942 | 0.911 | 0.937 |
| EfficientNetV2S [52] | 0.952 | 0.966 | 0.943 | 0.959 |
| InceptionV3 [53] | 0.936 | 0.939 | 0.923 | 0.932 |
| NASNetLarge [54] | 0.912 | 0.927 | 0.913 | 0.920 |
| Xception [55] | 0.931 | 0.929 | 0.901 | 0.918 |
| Models | Accuracy | Specificity | Sensitivity | AUC |
|---|---|---|---|---|
| MobileNet [48] | 0.915 | 0.892 | 0.867 | 0.899 |
| VGG19 [49] | 0.982 | 0.973 | 0.993 | 0.986 |
| DenseNet201 [50] | 0.974 | 0.967 | 0.975 | 0.969 |
| ResNet152 [51] | 0.966 | 0.957 | 0.968 | 0.959 |
| EfficientNetV2S [52] | 0.975 | 0.988 | 0.969 | 0.973 |
| InceptionV3 [53] | 0.952 | 0.947 | 0.962 | 0.942 |
| NASNetLarge [54] | 0.926 | 0.899 | 0.901 | 0.911 |
| Xception [55] | 0.959 | 0.944 | 0.966 | 0.954 |
| Ensemble Method | Models | Accuracy | Specificity | Sensitivity | AUC |
|---|---|---|---|---|---|
| Simple Average | M1 + M2 + M3 | 0.971 | 0.960 | 0.973 | 0.966 |
| M1 + M2 | 0.969 | 0.958 | 0.983 | 0.979 | |
| M1 + M3 | 0.977 | 0.989 | 0.969 | 0.977 | |
| M2 + M3 | 0.989 | 0.967 | 0.978 | 0.968 | |
| Weighted Average | M1 + M2 + M3 | 0.941 | 0.942 | 0.922 | 0.936 |
| M1 + M2 | 0.976 | 0.961 | 0.984 | 0.978 | |
| M1 + M3 | 0.969 | 0.964 | 0.936 | 0.952 | |
| M2 + M3 | 0.981 | 0.970 | 0.925 | 0.947 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grover, P.; Chaturvedi, K.; Zi, X.; Saxena, A.; Prakash, S.; Jan, T.; Prasad, M. Ensemble Transfer Learning for Distinguishing Cognitively Normal and Mild Cognitive Impairment Patients Using MRI. Algorithms 2023, 16, 377. https://doi.org/10.3390/a16080377
Grover P, Chaturvedi K, Zi X, Saxena A, Prakash S, Jan T, Prasad M. Ensemble Transfer Learning for Distinguishing Cognitively Normal and Mild Cognitive Impairment Patients Using MRI. Algorithms. 2023; 16(8):377. https://doi.org/10.3390/a16080377
Chicago/Turabian StyleGrover, Pratham, Kunal Chaturvedi, Xing Zi, Amit Saxena, Shiv Prakash, Tony Jan, and Mukesh Prasad. 2023. "Ensemble Transfer Learning for Distinguishing Cognitively Normal and Mild Cognitive Impairment Patients Using MRI" Algorithms 16, no. 8: 377. https://doi.org/10.3390/a16080377
APA StyleGrover, P., Chaturvedi, K., Zi, X., Saxena, A., Prakash, S., Jan, T., & Prasad, M. (2023). Ensemble Transfer Learning for Distinguishing Cognitively Normal and Mild Cognitive Impairment Patients Using MRI. Algorithms, 16(8), 377. https://doi.org/10.3390/a16080377