
Clinically Relevant Properties of 3D Printable Materials for Intraoral Use in Orthodontics: A Critical Review of the Literature


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
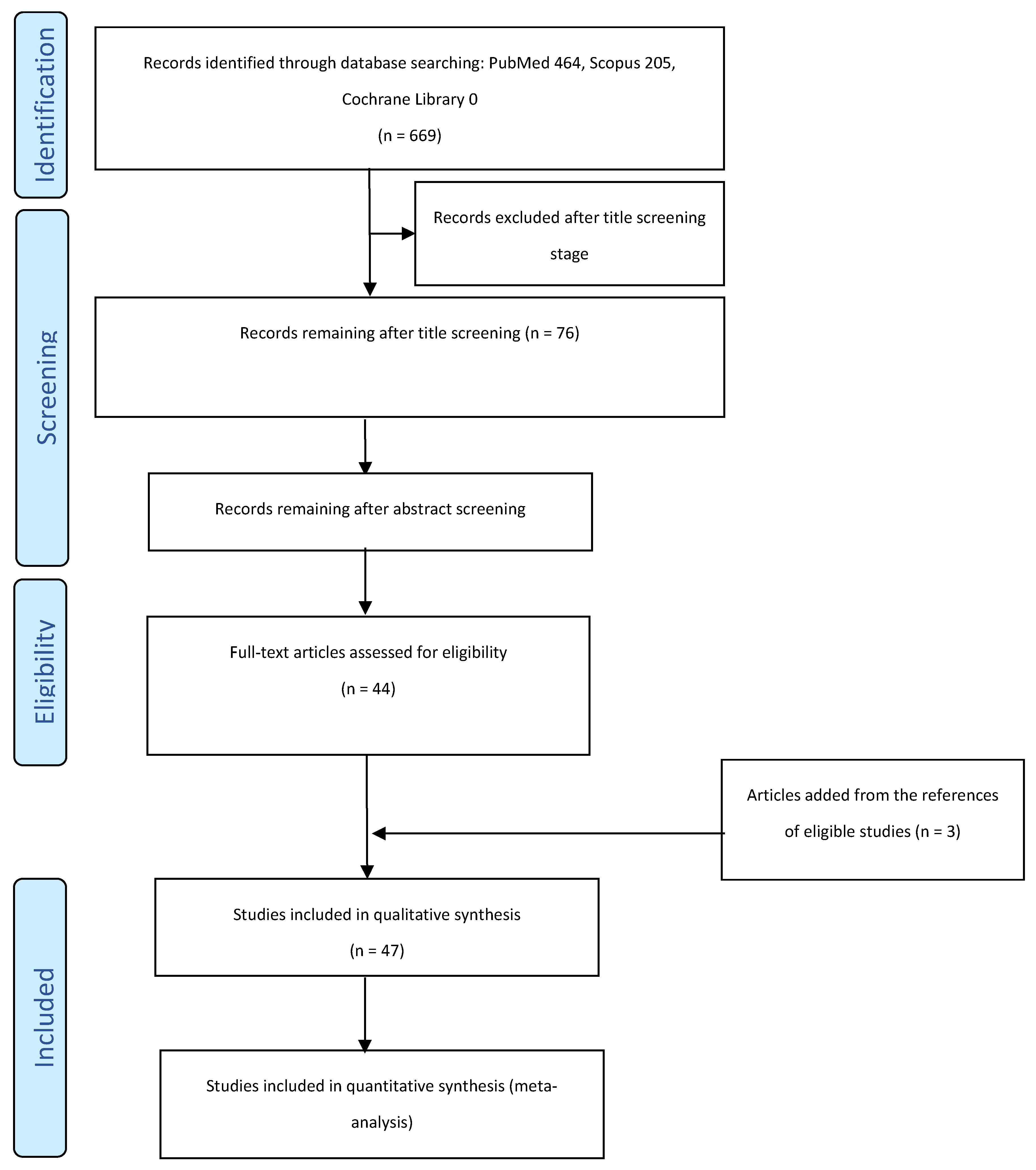
2.2. Information Sources and Research Strategies
2.3. Sources of Evidence Selection
3. Results
3.1. Case Reports and Proofs of Concept Clinical Cases
3.2. Mechanical and Geometric Properties
3.2.1. 3D-Printed Aligners and Retainers
3.2.2. 3D-Printed Fixed Retainers
3.2.3. 3D-Printed Orthodontic Brackets
3.2.4. 3D-Printed Springs
3.2.5. 3D-Printed Palatal Plates
3.2.6. 3D-Printed Metal Appliances
3.3. Biocompatibility
3.4. Aesthetic Properties
3.4.1. 3D-Printed Retainers
3.4.2. 3D-Printed Brackets
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leonardi, R.M. 3D Imaging Advancements and New Technologies in Clinical and Scientific Dental and Orthodontic Fields. J. Clin. Med. 2022, 11, 2200. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Maspero, C.; Tartaglia, G.M. 3D Printing of Clear Orthodontic Aligners: Where We Are and Where We Are Going. Materials 2020, 13, 5204. [Google Scholar] [CrossRef] [PubMed]
- Bachour, P.C.; Klabunde, R.; Grunheid, T. Transfer accuracy of 3D-printed trays for indirect bonding of orthodontic brackets. Angle Orthod. 2022, 92, 372–379. [Google Scholar] [CrossRef]
- Shannon, T.; Groth, C. Be your own manufacturer: 3D printing intraoral appliances. Semin. Orthod. 2021, 27, 184–188. [Google Scholar] [CrossRef]
- Franchi, L.; Vichi, A.; Marti, P.; Lampus, F.; Guercio, S.; Recupero, A.; Giuntini, V.; Goracci, C. 3D Printed Customized Facemask for Maxillary Protraction in the Early Treatment of a Class III Malocclusion: Proof-of-Concept Clinical Case. Materials 2022, 15, 3747. [Google Scholar] [CrossRef]
- Graf, S.; Tarraf, N.E.; Kravitz, N.D. Three-dimensional metal printed orthodontic laboratory appliances. Semin. Orthod. 2021, 27, 189–193. [Google Scholar] [CrossRef]
- Kim, M.; Li, J.; Kim, S.; Kim, W.; Kim, S.H.; Lee, S.M.; Park, Y.L.; Yang, S.; Kim, J.W. Individualized 3D-Printed Bone-Anchored Maxillary Protraction Device for Growth Modification in Skeletal Class III Malocclusion. J. Pers. Med. 2021, 11, 1087. [Google Scholar] [CrossRef]
- Panayi, N.; Eliades, T. In-office 3-dimensional-printing: Does the hype obscure the hazards for the operator? Am. J. Orthod. Dentofac. Orthop. 2022, 161, 757–759. [Google Scholar] [CrossRef]
- Zinelis, S.; Polychronis, G.; Papadopoulos, F.; Kokkinos, C.; Economou, A.; Panayi, N.; Papageorgiou, S.N.; Eliades, T. Mechanical and electrochemical characterization of 3D printed orthodontic metallic appliances after in vivo ageing. Dent. Mater. 2022, 38, 1721–1727. [Google Scholar] [CrossRef]
- Haynie, A.S.; English, J.D.; Paravina, R.D.; Moon, A.; Hanigan, J.; Abu Al Tamn, M.A.; Kasper, F.K. Colour stability of 3D-printed resin orthodontic brackets. J. Orthod. 2021, 48, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.; Rao, D.; Panwar, S.; Pawar, B.A.; Ameen, S. 3D Printed Band and Loop Space Maintainer: A Digital Game Changer in Preventive Orthodontics. J. Clin. Pediatr. Dent. 2021, 45, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Pawar, B.A. Maintenance of space by innovative three-dimensional-printed band and loop space maintainer. J. Indian. Soc. Pedod. Prev. Dent. 2019, 37, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Xie, X.; Wang, F.; Chang, Q.; Wang, H.; Bai, Y. Maxillary protraction using customized mini-plates for anchorage in an adolescent girl with skeletal Class III malocclusion. Korean J. Orthod. 2020, 50, 346–355. [Google Scholar] [CrossRef]
- Graf, S.; Cornelis, M.A.; Hauber Gameiro, G.; Cattaneo, P.M. Computer-aided design and manufacture of hyrax devices: Can we really go digital? Am. J. Orthod. Dentofac. Orthop. 2017, 152, 870–874. [Google Scholar] [CrossRef]
- Graf, S.; Vasudavan, S.; Wilmes, B. CAD-CAM design and 3-dimensional printing of mini-implant retained orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 877–882. [Google Scholar] [CrossRef]
- Cozzani, M.; Antonini, S.; Lupini, D.; Decesari, D.; Anelli, F.; Doldo, T. A New Proposal: A Digital Flow for the Construction of a Haas-Inspired Rapid Maxillary Expander (HIRME). Materials 2020, 13, 2898. [Google Scholar] [CrossRef]
- van der Meer, W.J.; Vissink, A.; Ren, Y. Full 3-dimensional digital workflow for multicomponent dental appliances: A proof of concept. J. Am. Dent. Assoc. 2016, 147, 288–291. [Google Scholar] [CrossRef]
- Al Mortadi, N.; Jones, Q.; Eggbeer, D.; Lewis, J.; Williams, R.J. Fabrication of a resin appliance with alloy components using digital technology without an analog impression. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 862–867. [Google Scholar] [CrossRef]
- Nasef, A.A.; El-Beialy, A.R.; Mostafa, Y.A. Virtual techniques for designing and fabricating a retainer. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 394–398. [Google Scholar] [CrossRef]
- Fayyaz Ahamed, S.; Apros Kanna, A.S.; Vijaya Kumar, R.K. 3D-printed orthodontic auxiliaries. J. Clin. Orthod. 2015, 49, 337–341. [Google Scholar] [PubMed]
- Thurzo, A.; Kočiš, F.; Novák, B.; Czako, L.; Varga, I. Three-Dimensional Modeling and 3D Printing of Biocompatible Orthodontic Power-Arm Design with Clinical Application. Appl. Sci. 2021, 11, 9693. [Google Scholar] [CrossRef]
- Graf, S.; Tarraf, N.E.; Vasudavan, S. Direct printed removable appliances: A new approach for the Twin-block appliance. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 103–107. [Google Scholar] [CrossRef]
- Krey, K.F.; Darkazanly, N.; Kuhnert, R.; Ruge, S. 3D-printed orthodontic brackets—Proof of concept. Int. J. Comput. Dent. 2016, 19, 351–362. [Google Scholar] [PubMed]
- Bichu, Y.M.; Alwafi, A.; Liu, X.; Andrews, J.; Ludwig, B.; Bichu, A.Y.; Zou, B. Advances in orthodontic clear aligner materials. Bioact. Mater. 2023, 22, 384–403. [Google Scholar] [CrossRef]
- Naeem, O.A.; Bencharit, S.; Yang, I.H.; Stilianoudakis, S.C.; Carrico, C.; Tufekci, E. Comparison of 3-dimensional printing technologies on the precision, trueness, and accuracy of printed retainers. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 582–591. [Google Scholar] [CrossRef]
- Edelmann, A.; English, J.D.; Chen, S.J.; Kasper, F.K. Analysis of the thickness of 3-dimensional-printed orthodontic aligners. Am. J. Orthod. Dentofac. Orthop. 2020, 158, e91–e98. [Google Scholar] [CrossRef]
- Jindal, P.; Juneja, M.; Siena, F.L.; Bajaj, D.; Breedon, P. Mechanical and geometric properties of thermoformed and 3D printed clear dental aligners. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 694–701. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, H.; Kim, H.-J.; Chung, C.J.; Choi, Y.J.; Kim, S.-J.; Cha, J.-Y. Thermo-mechanical properties of 3D printed photocurable shape memory resin for clear aligners. Sci. Rep. 2022, 12, 6246. [Google Scholar] [CrossRef]
- McCarty, M.C.; Chen, S.J.; English, J.D.; Kasper, F. Effect of print orientation and duration of ultraviolet curing on the dimensional accuracy of a 3-dimensionally printed orthodontic clear aligner design. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 889–897. [Google Scholar] [CrossRef]
- Williams, A.; Bencharit, S.; Yang, I.H.; Stilianoudakis, S.C.; Carrico, C.K.; Tufekci, E. Effect of print angulation on the accuracy and precision of 3D-printed orthodontic retainers. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 133–139. [Google Scholar] [CrossRef]
- Boyer, R.A.; Kasper, F.K.; English, J.D.; Jacob, H.B. Effect of print orientation on the dimensional accuracy of orthodontic aligners printed 3-dimensionally. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 732–742.e1. [Google Scholar] [CrossRef]
- Cole, D.; Bencharit, S.; Carrico, C.K.; Arias, A.; Tufekci, E. Evaluation of fit for 3D-printed retainers compared with thermoform retainers. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 592–599. [Google Scholar] [CrossRef]
- Martorelli, M.; Gerbino, S.; Giudice, M.; Ausiello, P. A comparison between customized clear and removable orthodontic appliances manufactured using RP and CNC techniques. Dent. Mater. 2013, 29, e1–e10. [Google Scholar] [CrossRef]
- Koenig, N.; Choi, J.Y.; McCray, J.; Hayes, A.; Schneider, P.; Kim, K.B. Comparison of dimensional accuracy between direct-printed and thermoformed aligners. Korean J. Orthod. 2022, 52, 249–257. [Google Scholar] [CrossRef]
- Milovanovic, A.; Sedmak, A.; Golubovic, Z.; Mihajlovic, K.Z.; Zurkic, A.; Trajkovic, I.; Milosevic, M. The effect of time on mechanical properties of biocompatible photopolymer resins used for fabrication of clear dental aligners. J. Mech. Behav. Biomed. Mater. 2021, 119, 104494. [Google Scholar] [CrossRef] [PubMed]
- Jindal, P.; Worcester, F.; Siena, F.L.; Forbes, C.; Juneja, M.; Breedon, P. Mechanical behaviour of 3D printed vs thermoformed clear dental aligner materials under non-linear compressive loading using FEM. J. Mech. Behav. Biomed. Mater. 2020, 112, 104045. [Google Scholar] [CrossRef] [PubMed]
- Elshazly, T.M.; Keilig, L.; Alkabani, Y.; Ghoneima, A.; Abuzayda, M.; Talaat, W.; Talaat, S.; Bourauel, C.P. Potential Application of 4D Technology in Fabrication of Orthodontic Aligners. Front. Mater. 2022, 8, 794536. [Google Scholar] [CrossRef]
- Zinelis, S.; Panayi, N.; Polychronis, G.; Papageorgiou, S.N.; Eliades, T. Comparative analysis of mechanical properties of orthodontic aligners produced by different contemporary 3D printers. Orthod. Craniofac. Res. 2022, 25, 336–341. [Google Scholar] [CrossRef]
- Jindal, P.; Worcester, F.; Siena, F.L.; Forbes, C.; Juneja, M.; Breedon, P. Effects of post-curing conditions on mechanical properties of 3D printed clear dental aligners. Rapid Prototyp. J. 2020, 26, 1337–1344. [Google Scholar] [CrossRef]
- Xu, Y.; Xepapadeas, A.B.; Koos, B.; Geis-Gerstorfer, J.; Li, P.; Spintzyk, S. Effect of post-rinsing time on the mechanical strength and cytotoxicity of a 3D printed orthodontic splint material. Dent. Mater. 2021, 37, e314–e327. [Google Scholar] [CrossRef] [PubMed]
- Lambart, A.L.; Xepapadeas, A.B.; Koos, B.; Li, P.; Spintzyk, S. Rinsing postprocessing procedure of a 3D-printed orthodontic appliance material: Impact of alternative post-rinsing solutions on the roughness, flexural strength and cytotoxicity. Dent. Mater. 2022, 38, 1344–1353. [Google Scholar] [CrossRef]
- Can, E.; Panayi, N.; Polychronis, G.; Papageorgiou, S.N.; Zinelis, S.; Eliades, G.; Eliades, T. In-house 3D-printed aligners: Effect of in vivo ageing on mechanical properties. Eur. J. Orthod. 2022, 44, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Firlej, M.; Zaborowicz, K.; Zaborowicz, M.; Firlej, E.; Domagała, I.; Pieniak, D.; Igielska-Kalwat, J.; Dmowski, A.; Biedziak, B. Mechanical Properties of 3D Printed Orthodontic Retainers. Int. J. Environ. Res. Public Health 2022, 19, 5775. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Polychronis, G.; Panayi, N.; Zinelis, S.; Eliades, T. New aesthetic in-house 3D-printed brackets: Proof of concept and fundamental mechanical properties. Prog. Orthod. 2022, 23, 6. [Google Scholar] [CrossRef]
- Hodecker, L.; Bourauel, C.; Braumann, B.; Kruse, T.; Christ, H.; Scharf, S. Comparative in vitro analysis of the sliding resistance of a modern 3D-printed polymer bracket in combination with different archwire types. Clin. Oral. Investig. 2022, 26, 4049–4057. [Google Scholar] [CrossRef] [PubMed]
- Othman, A.; Hartman, S.; Strobele, D.; Arnold, J.; See, V. Preliminary feasibility torque mechanical evaluation for 3D printed orthodontic springs with different parameters: In vitro study. BMC Oral Health 2021, 21, 104. [Google Scholar] [CrossRef]
- Strobele, D.; Othman, A.; Alevizakos, V.; Turan, M.; von See, C. Mechanical evaluation for three-dimensional printed orthodontic springs with different heights-in vitro study. J. Clin. Exp. Dent. 2021, 13, e975–e979. [Google Scholar] [CrossRef]
- Aretxabaleta, M.; Xepapadeas, A.B.; Poets, C.F.; Koos, B.; Spintzyk, S. Fracture Load of an Orthodontic Appliance for Robin Sequence Treatment in a Digital Workflow. Materials 2021, 14, 344. [Google Scholar] [CrossRef]
- Aretxabaleta, M.; Unkovskiy, A.; Koos, B.; Spintzyk, S.; Xepapadeas, A.B. Accuracy Evaluation of Additively and Subtractively Fabricated Palatal Plate Orthodontic Appliances for Newborns and Infants-An In Vitro Study. Materials 2021, 14, 4103. [Google Scholar] [CrossRef]
- Thurzo, A.; Sufliarsky, B.; Urbanova, W.; Cverha, M.; Strunga, M.; Varga, I. Pierre Robin Sequence and 3D Printed Personalized Composite Appliances in Interdisciplinary Approach. Polymers 2022, 14, 3858. [Google Scholar] [CrossRef]
- Ahamed, S.F.; Kumar, S.M.; Kumar, R.K.V.; Kanna, A.S.A.; Dharshini, K.I. Cytotoxic evaluation of directly 3D printed aligners and Invisalign. Eur. J. Mol. Clin. Med. 2020, 7, 1129–1140. [Google Scholar]
- Formlabs. EU Declaration of Conformity. Available online: https://formlabs.com/media/upload/Declaration_of_Conformity_Dental_LT_Clear_DoC-FLOC-2017-01-UK.pdf. (accessed on 3 October 2022).
- Pratsinis, H.; Papageorgiou, S.N.; Panayi, N.; Iliadi, A.; Eliades, T.; Kletsas, D. Cytotoxicity and estrogenicity of a novel 3-dimensional printed orthodontic aligner. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e116–e122. [Google Scholar] [CrossRef] [PubMed]
- Willi, A.; Patcas, R.; Zervou, S.K.; Panayi, N.; Schatzle, M.; Eliades, G.; Hiskia, A.; Eliades, T. Leaching from a 3D-printed aligner resin. Eur. J. Orthod. 2022, cjac056. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H.; Kato, R.; Kakami, C.; Okamoto, H.; Mamada, K.; Maki, K. Development of Biocompatible Resins for 3D Printing of Direct Aligners. J. Photopolym. Sci. Technol. 2019, 32, 209–216. [Google Scholar] [CrossRef]
- Warnecki, M.; Sarul, M.; Kozakiewicz, M.; Zięty, A.; Babiarczuk, B.; Kawala, B.; Jurczyszyn, K. Surface Evaluation of Aligners after Immersion in Coca-Cola and Orange Juice. Materials 2022, 13, 6341. [Google Scholar] [CrossRef]
- Lombardo, L.; Martines, E.; Mazzanti, V.; Arreghini, A.; Mollica, F.; Siciliani, G. Stress relaxation properties of four orthodontic aligner materials: A 24-hour in vitro study. Angle Orthod. 2017, 87, 11–18. [Google Scholar] [CrossRef]
- Panayi, N.C. Consider material properties when selecting a resin for 3-dimensionally printed aligners. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 706. [Google Scholar] [CrossRef]
- Rajabi, M.; McConnell, M.; Cabral, J.; Ali, M.A. Chitosan hydrogels in 3D printing for biomedical applications. Carbohydr. Polym. 2021, 260, 117768. [Google Scholar] [CrossRef]
- Graf, S.; Berger, M.; Rohr, N. Influence of printing procedure and printing axis of dental alloys on dimensional accuracy, surface roughness, and porosity. APOS Trends Orthod. 2022, 12, 149–156. [Google Scholar] [CrossRef]
- Graf, S.; Tarraf, N.E. Advantages and disadvantages of the three-dimensional metal printed orthodontic appliances. J. World Fed. Orthod. 2022, 11, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Coleman, G. Cementation and removal of 3D-printed expanders. J. Clin. Orthod. 2021, 55, 571–573. [Google Scholar] [PubMed]
- Küffer, M.; Drescher, D.; Becker, K. Application of the Digital Workflow in Orofacial Orthopedics and Orthodontics: Printed Appliances with Skeletal Anchorage. Appl. Sci. 2022, 12, 3820. [Google Scholar] [CrossRef]


{kind=link}
| MEDLINE/PubMed |
|---|
| orthodontics AND (3D printing OR additive manufacturing OR rapid prototyping) |
| (“orthodontal”[All Fields] OR “orthodontic”[All Fields] OR “orthodontical”[All Fields] OR “orthodontically”[All Fields] OR “orthodontics”[MeSH Terms] OR “orthodontics”[All Fields]) AND (“printing, three dimensional”[MeSH Terms] OR (“printing”[All Fields] AND “three dimensional”[All Fields]) OR “three-dimensional printing”[All Fields] OR (“3d”[All Fields] AND “printing”[All Fields]) OR “3d printing”[All Fields] OR ((“rapid”[All Fields] OR “rapidities”[All Fields] OR “rapidity”[All Fields] OR “rapidness”[All Fields]) AND (“prototypal”[All Fields] OR “prototype”[All Fields] OR “prototype s”[All Fields] OR “prototyped”[All Fields] OR “prototypes”[All Fields] OR “prototypic”[All Fields] OR “prototypical”[All Fields] OR “prototypicality”[All Fields] OR “prototypically”[All Fields] OR “prototyping”[All Fields])) OR (“addit manuf”[Journal] OR (“additive”[All Fields] AND “manufacturing”[All Fields]) OR “additive manufacturing”[All Fields])) |
| 464 items |
| Scopus |
| orthodontics AND (3d printing) OR (additive manufacturing) OR (rapid prototyping) |
| ( TITLE-ABS-KEY ( orthodontics ) AND TITLE-ABS-KEY ( 3d AND printing ) OR TITLE-ABS-KEY ( additive AND manufacturing ) OR TITLE-ABS-KEY ( rapid AND prototyping ) ) |
| 205 documents |
| Cochrane Library |
| orthodontics AND 3d printing OR additive manufacturing OR rapid prototyping |
| orthodontics AND (3D printing OR additive manufacturing OR rapid prototyping) in Title Abstract Keyword |
| 0 Cochrane reviews |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goracci, C.; Juloski, J.; D’Amico, C.; Balestra, D.; Volpe, A.; Juloski, J.; Vichi, A. Clinically Relevant Properties of 3D Printable Materials for Intraoral Use in Orthodontics: A Critical Review of the Literature. Materials 2023, 16, 2166. https://doi.org/10.3390/ma16062166
Goracci C, Juloski J, D’Amico C, Balestra D, Volpe A, Juloski J, Vichi A. Clinically Relevant Properties of 3D Printable Materials for Intraoral Use in Orthodontics: A Critical Review of the Literature. Materials. 2023; 16(6):2166. https://doi.org/10.3390/ma16062166
Chicago/Turabian StyleGoracci, Cecilia, Jovana Juloski, Claudio D’Amico, Dario Balestra, Alessandra Volpe, Jelena Juloski, and Alessandro Vichi. 2023. "Clinically Relevant Properties of 3D Printable Materials for Intraoral Use in Orthodontics: A Critical Review of the Literature" Materials 16, no. 6: 2166. https://doi.org/10.3390/ma16062166
APA StyleGoracci, C., Juloski, J., D’Amico, C., Balestra, D., Volpe, A., Juloski, J., & Vichi, A. (2023). Clinically Relevant Properties of 3D Printable Materials for Intraoral Use in Orthodontics: A Critical Review of the Literature. Materials, 16(6), 2166. https://doi.org/10.3390/ma16062166