


Influences of Different CAD/CAM Ceramic Compositions and Thicknesses on the Mechanical Properties of Ceramic Restorations: An In Vitro Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
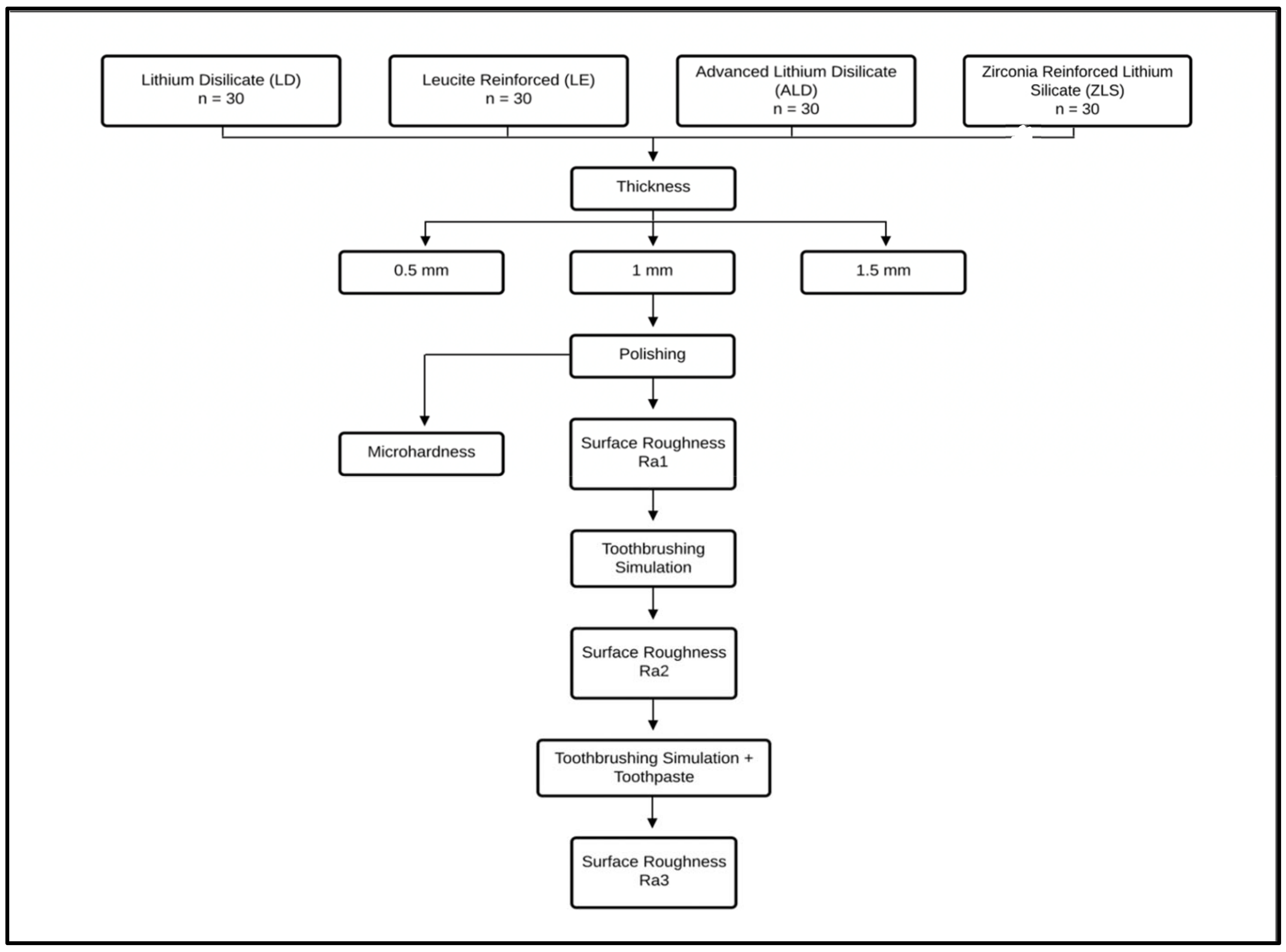
2.1. Sample Grouping
2.2. Specimens’ Preparation
2.3. Microhardness Measurements
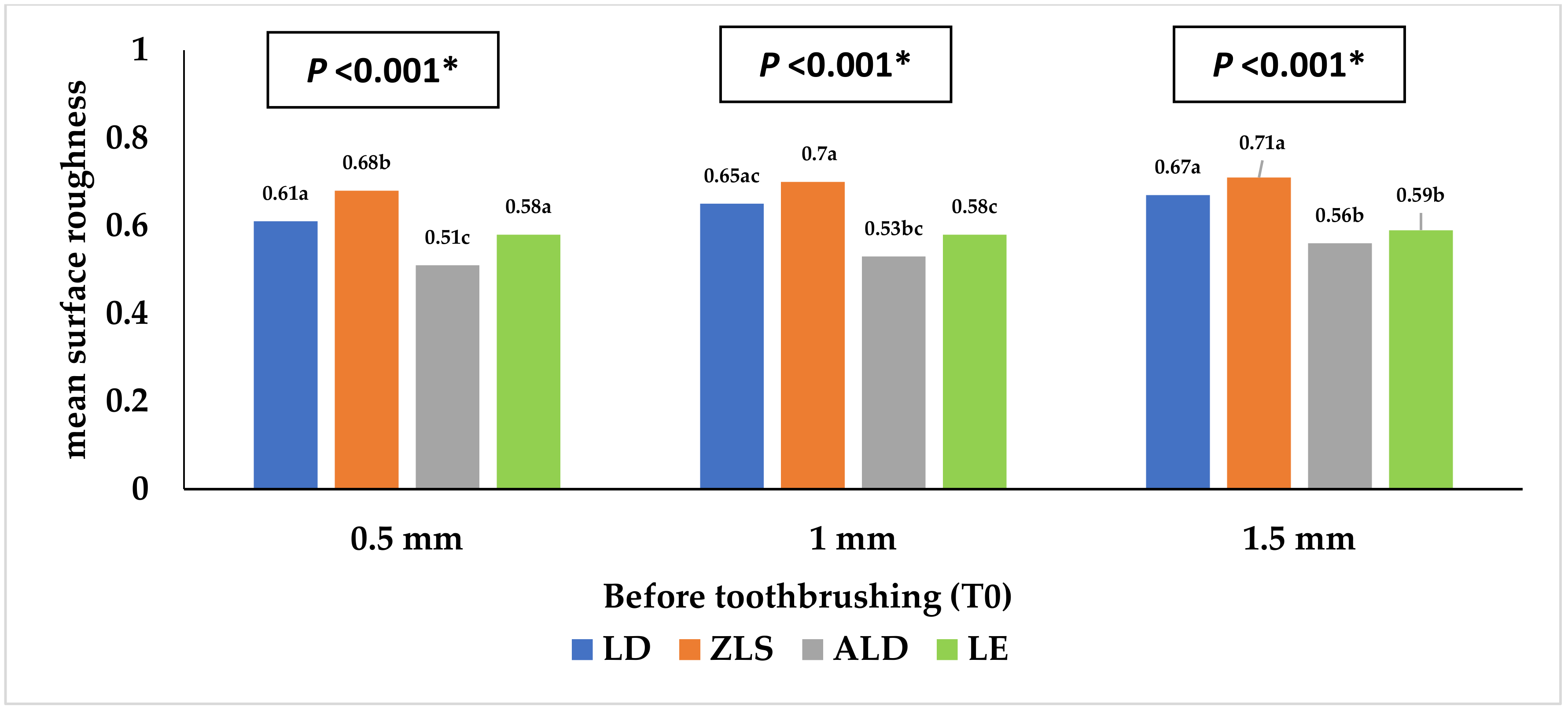
2.4. Surface Roughness Measurements (Ra)
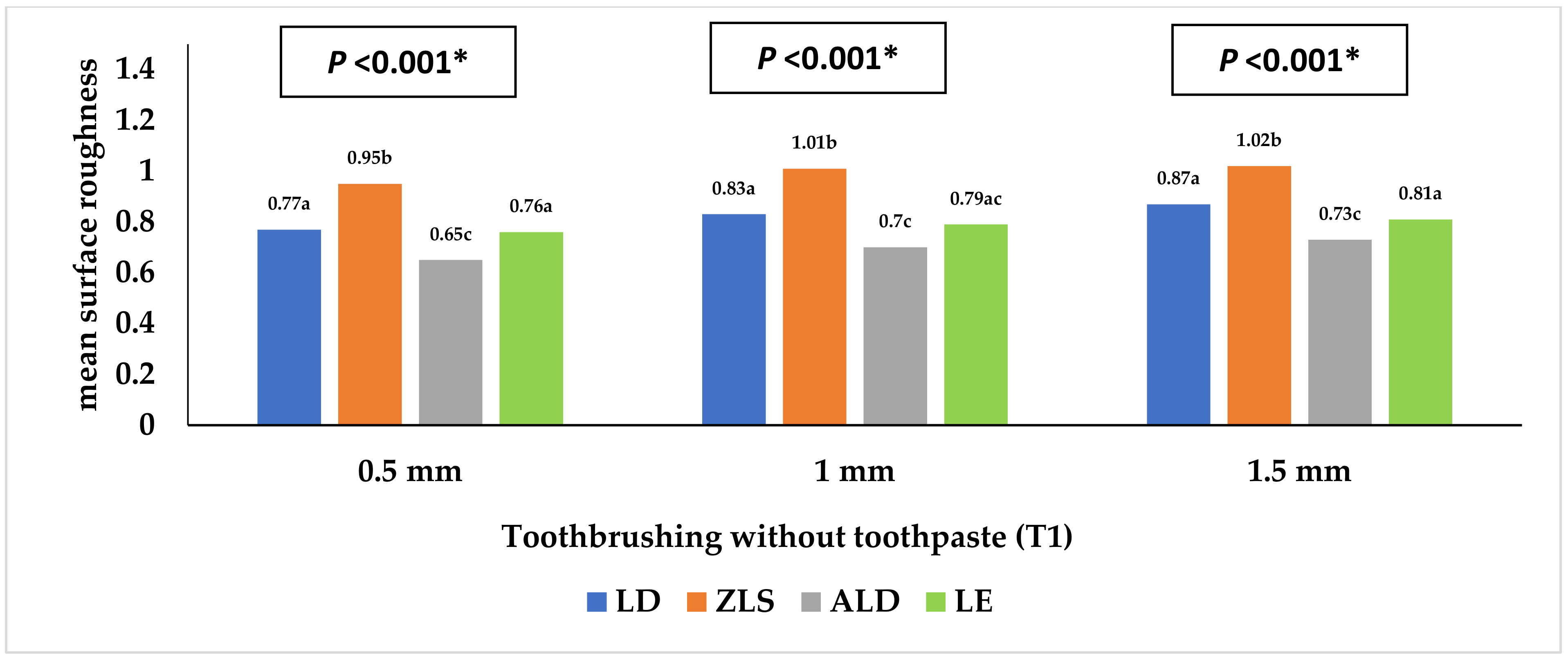
2.5. Toothbrushing Simulation Procedure
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.-H.; Choi, Y.-S.; Kang, K.-H.; Att, W. Effects of Thermal and Mechanical Cycling on the Mechanical Strength and Surface Properties of Dental CAD-CAM Restorative Materials. J. Prosthet. Dent. 2022, 128, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Ellakany, P.; Aly, N.M.; Al-Harbi, F. Accuracy of 3D Printed and Digital Casts Produced from Intraoral and Extraoral Scanners with Different Scanning Technologies: In Vitro Study. J. Prosthodont. 2022, 31, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Zaniboni, J.F.; Silva, A.M.; Alencar, C.d.M.; Porto, T.S.; Jasinevicius, R.G.; Fortulan, C.A.; De Campos, E.A. Influence of Different Glaze Firing Protocols on the Mechanical Properties of CAD-CAM Ceramic Materials. J. Prosthet. Dent. 2022, 127, 925.e1–925.e8. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, R.D.; Uțu, I.-D.; Rusu, L.; Boloș, A.; Porojan, L. Fractographic and Microhardness Evaluation of All-Ceramic Hot-Pressed and CAD/CAM Restorations after Hydrothermal Aging. Materials 2022, 15, 3987. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.; Pjetursson, B.E. All-Ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPs)? A Systematic Review of the Survival and Complication Rates. Part I: Single Crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef]
- Rauch, A.; Reich, S.; Schierz, O. Chair-side generated posterior monolithic lithium disilicate crowns: Clinical survival after 6 years. Clin Oral Investig. 2017, 21, 2083–2089. [Google Scholar] [CrossRef]
- Sulaiman, T.A.; Delgado, A.J.; Donovan, T.E. Survival Rate of Lithium Disilicate Restorations at 4 Years: A Retrospective Study. J. Prosthet. Dent. 2015, 114, 364–366. [Google Scholar] [CrossRef]
- Pekkan, G.; Özcan, M.; Subaşı, M.G. Clinical factors affecting the translucency of monolithic Y-TZP ceramics. Odontology 2020, 108, 526–531. [Google Scholar] [CrossRef]
- Al-Haj Husain, N.; Dürr, T.; Özcan, M.; Brägger, U.; Joda, T. Mechanical Stability of Dental CAD-CAM Restoration Materials Made of Monolithic Zirconia, Lithium Disilicate, and Lithium Disilicate–Strengthened Aluminosilicate Glass-Ceramic with and without Fatigue Conditions. J. Prosthet. Dent. 2022, 128, 73–78. [Google Scholar] [CrossRef]
- Jurado, C.A.; Mourad, F.; Trevino, D.A.C.; Gouveia, D.N.; Hyer, J.; Elgreatly, A.; Mahrous, A.M.; Garcia-Godoy, F.; Tsujimoto, A. Comparison of Full and Partial Coverage Crowns with CAD/CAM Leucite Reinforced Ceramic Blocks on Fracture Resistance and Fractographic Analysis. Dent. Mater. J. 2022, 41, 2021–2253. [Google Scholar] [CrossRef]
- Skorulska, A.; Piszko, P.; Rybak, Z.; Szymonowicz, M.; Dobrzyński, M. Review on Polymer, Ceramic and Composite Materials for CAD/CAM Indirect Restorations in Dentistry—Application, Mechanical Characteristics and Comparison. Materials 2021, 14, 1592. [Google Scholar] [CrossRef]
- Ellakany, P.; Madi, M.; Aly, N.M.; Al-Aql, Z.S.; AlGhamdi, M.; AlJeraisy, A.; Alagl, A.S. Effect of CAD/CAM Ceramic Thickness on Shade Masking Ability of Discolored Teeth: In Vitro Study. Int. J. Environ. Res. Public. Health 2021, 18, 13359. [Google Scholar] [CrossRef]
- Tennert, C.; Suárez Machado, L.; Jaeggi, T.; Meyer-Lueckel, H.; Wierichs, R.J. Posterior Ceramic versus Metal Restorations: A Systematic Review and Meta-Analysis. Dent. Mater. 2022, 38, 1623–1632. [Google Scholar] [CrossRef]
- Goto, M.; Oki, K.; Koyano, K.; Ayukawa, Y. The 3-Year Cumulative Survival Rates of Posterior Monolithic Zirconia Crowns and Their Antagonist Teeth, and Their Influencing Factors. J. Oral Sci. 2022, 64, 286–289. [Google Scholar] [CrossRef]
- Jin, H.; Teng, M.; Wang, Z.; Li, X.; Liang, J.; Wang, W.; Jiang, S.; Zhao, B. Comparative Evaluation of BioHPP and Titanium as a Framework Veneered with Composite Resin for Implant-Supported Fixed Dental Prostheses. J. Prosthet. Dent. 2019, 122, 383–388. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Galli, M.; De Biase, A.; Testarelli, L.; Di Nardo, D. Applications and Clinical Behavior of BioHPP in Prosthetic Dentistry: A Short Review. J. Compos. Sci. 2022, 6, 90. [Google Scholar] [CrossRef]
- Jovanović, M.; Živić, M.; Milosavljević, M. A Potential Application of Materials Based on a Polymer and CAD/CAM Composite Resins in Prosthetic Dentistry. J. Prosthodont. Res. 2021, 65, 137–147. [Google Scholar] [CrossRef]
- Shetty, R.; Shenoy, K.; Dandekeri, S.; Suhaim, K.S.; Ragher, M.; Francis, J. Resin-matrix ceramics—An overview. Int. J. Recent. Sci. Res. 2015, 6, 7414–7417. [Google Scholar]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.; Bonfante, E.A. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef]
- Shi, H.Y.; Pang, R.; Yang, J.; Fan, D.; Cai, H.; Jiang, H.B.; Han, J.; Lee, E.-S.; Sun, Y. Overview of Several Typical Ceramic Materials for Restorative Dentistry. Bio. Med. Res. Int. 2022, 2022, e8451445. [Google Scholar] [CrossRef]
- Campos, F.; Almeida, C.; Rippe, M.; De Melo, R.; Valandro, L.; Bottino, M. Resin Bonding to a Hybrid Ceramic: Effects of Surface Treatments and Aging. Oper. Dent. 2016, 41, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Coldea, A.; Swain, M.V.; Thiel, N. Mechanical Properties of Polymer-Infiltrated-Ceramic-Network Materials. Dent. Mater. 2013, 29, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Bajraktarova-Valjakova, E.; Korunoska-Stevkovska, V.; Kapusevska, B.; Gigovski, N.; Bajraktarova-Misevska, C.; Grozdanov, A. Contemporary Dental Ceramic Materials, a Review:Chemical Composition, Physical and Mechanical Properties, Indication for Use. Open Access Maced. J. Med. Sci. 2018, 6, 1742–1755. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ruggiero, G.; Leone, R.; Breschi, L.; Leuci, S.; Sorrentino, R. Zirconia-Reinforced Lithium Silicate (ZLS) Mechanical and Biological Properties: A Literature Review. J. Dent. 2021, 109, 103661. [Google Scholar] [CrossRef] [PubMed]
- Hamza, T.A.; Sherif, R.M. Fracture Resistance of Monolithic Glass-Ceramics Versus Bilayered Zirconia-Based Restorations. J. Prosthodont. 2019, 28, e259–e264. [Google Scholar] [CrossRef]
- Sen, N.; Us, Y.O. Mechanical and Optical Properties of Monolithic CAD-CAM Restorative Materials. J. Prosthet. Dent. 2018, 119, 593–599. [Google Scholar] [CrossRef]
- Rosentritt, M.; Schmid, A.; Huber, C.; Strasser, T. In Vitro Mastication Simulation and Wear Test of Virgilite and Advanced Lithium Disilicate Ceramics. Int. J. Prosthodont. 2022. [Google Scholar] [CrossRef]
- Gunal, B.; Ulusoy, M.M. Optical Properties of Contemporary Monolithic CAD-CAM Restorative Materials at Different Thicknesses. J. Esthet. Restor. Dent. 2018, 30, 434–441. [Google Scholar] [CrossRef]
- Marchesi, G.; Camurri Piloni, A.; Nicolin, V.; Turco, G.; Di Lenarda, R. Chairside CAD/CAM Materials: Current Trends of Clinical Uses. Biology. 2021, 10, 1170. [Google Scholar] [CrossRef]
- Gierthmuehlen, P.C.; Jerg, A.; Fischer, J.B.; Bonfante, E.A.; Spitznagel, F.A. Posterior minimally invasive full-veneers: Effect of ceramic thicknesses, bonding substrate, and preparation designs on failure-load and -mode after fatigue. J. Esthet. Restor. Dent. 2022, 34, 145–153. [Google Scholar] [CrossRef]
- Zimmermann, M.; Egli, G.; Zaruba, M.; Mehl, A. Influence of material thickness on fractural strength of CAD/CAM fabricated ceramic crowns. Dent. Mater. J. 2017, 36, 778–783. [Google Scholar] [CrossRef]
- Abdulazeez, M.I.; Majeed, M.A. Fracture Strength of Monolithic Zirconia Crowns with Modified Vertical Preparation: A Comparative In Vitro Study. Eur. J. Dent. 2022, 16, 209–214. [Google Scholar] [CrossRef]
- Haddad, C.; Azzi, K. Influence of the Type and Thickness of Cervical Margins on the Strength of Posterior Monolithic Zirconia Crowns: A Review. Eur. J. Gen. Dent. 2022, 11, 73–80. [Google Scholar] [CrossRef]
- Subaşı, M.G.; Çakmak, G.; Sert, M.; Yilmaz, B. Effect of Multiple Firings on Surface Roughness and Flexural Strength of CAD-CAM Ceramics. J. Prosthet. Dent. 2022, 128, 216.e1–216.e8. [Google Scholar] [CrossRef]
- Mota, E.G.; Smidt, L.N.; Fracasso, L.M.; Burnett, L.H., Jr.; Spohr, A.M. The Effect of Milling and Postmilling Procedures on the Surface Roughness of CAD/CAM Materials. J. Esthet. Restor. Dent. 2017, 29, 450–458. [Google Scholar] [CrossRef]
- Reich, S.; Wichmann, M.; Nkenke, E.; Proeschel, P. Clinical Fit of All-Ceramic Three-Unit Fixed Partial Dentures, Generated with Three Different CAD/CAM Systems. Eur. J. Oral Sci. 2005, 113, 174–179. [Google Scholar] [CrossRef]
- Di Fiore, A.; Stellini, E.; Basilicata, M.; Bollero, P.; Monaco, C. Effect of Toothpaste on the Surface Roughness of the Resin-Contained CAD/CAM Dental Materials: A Systematic Review. J. Clin. Med. 2022, 11, 767. [Google Scholar] [CrossRef]
- Bressan, E.; Tessarolo, F.; Sbricoli, L.; Caola, I.; Nollo, G.; Di Fiore, A. Effect of chlorhexidine in preventing plaque biofilm on healing abutment: A crossover controlled study. Implant. Dent. 2014, 23, 64–68. [Google Scholar] [CrossRef]
- Pawar, R.O.; Narote, P.S.; Gawai, K.T.; Amte, M.P.; Singh, S.; Sonkesriya, S. Comparative Analysis of Biofilm Formation on Materials Used for the Fabrication of Implant Supported Prostheses. J. Pharm. Bioallied. Sci. 2022, 14 (Suppl. 1), S812–S815. [Google Scholar] [CrossRef]
- De Andrade, G.S.; Augusto, M.G.; Simões, B.V.; Pagani, C.; Saavedra, G.D.S.F.A.; Bresciani, E. Impact of Simulated Toothbrushing on Surface Properties of Chairside CAD-CAM Materials: An in Vitro Study. J. Prosthet. Dent. 2021, 125, 469.e1–469.e6. [Google Scholar] [CrossRef]
- Şen, N.; Tuncelli, B.; Göller, G. Surface Deterioration of Monolithic CAD/CAM Restorative Materials after Artificial Abrasive Toothbrushing. J. Adv. Prosthodont. 2018, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Majumder, A.; Giri, T.K.; Mukherjee, S. An in Vitro Study to Compare the Influence of Different All-Ceramic Systems on the Polymerization of Dual-Cure Resin Cement. J. Indian Prosthodont. Soc. 2019, 19, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Corado, H.P.R.; Da Silveira, P.H.P.M.; Ortega, V.L.; Ramos, G.G.; Elias, C.N. Flexural Strength of Vitreous Ceramics Based on Lithium Disilicate and Lithium Silicate Reinforced with Zirconia for CAD/CAM. Int. J. Biomater. 2022, 2022, e5896511. [Google Scholar] [CrossRef] [PubMed]
- Ellakany, P.; Fouda, S.M.; Mahrous, A.A.; AlGhamdi, M.A.; Aly, N.M. Influence of CAD/CAM Milling and 3D-Printing Fabrication Methods on the Mechanical Properties of 3-Unit Interim Fixed Dental Prosthesis after Thermo-Mechanical Aging Process. Polymers 2022, 14, 4103. [Google Scholar] [CrossRef] [PubMed]
- Nam, N.-E.; Shin, S.-H.; Lim, J.-H.; Shim, J.-S.; Kim, J.-E. Effects of Artificial Tooth Brushing and Hydrothermal Aging on the Mechanical Properties and Color Stability of Dental 3D Printed and CAD/CAM Materials. Materials 2021, 14, 6207. [Google Scholar] [CrossRef] [PubMed]
- Rosentritt, M.; Sawaljanow, A.; Behr, M.; Kolbeck, C.; Preis, V. Effect of tooth brush abrasion and thermo-mechanical loading on direct and indirect veneer restorations. Clin. Oral. Investig. 2015, 19, 53–60. [Google Scholar] [CrossRef]
- Dal Piva, A.M.d.O.; Bottino, M.A.; Anami, L.C.; Werner, A.; Kleverlaan, C.J.; Lo Giudice, R.; Famà, F.; Da Silva-Concilio, L.R.; Tribst, J.P.M. Toothbrushing Wear Resistance of Stained CAD/CAM Ceramics. Coatings 2021, 11, 224. [Google Scholar] [CrossRef]
- Yuan, J.C.-C.; Barão, V.A.R.; Wee, A.G.; Alfaro, M.F.; Afshari, F.S.; Sukotjo, C. Effect of Brushing and Thermocycling on the Shade and Surface Roughness of CAD-CAM Ceramic Restorations. J. Prosthet. Dent. 2018, 119, 1000–1006. [Google Scholar] [CrossRef]
- 14:00-17:00. ISO 11609:2010. ISO. Available online: https://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/03/80/38010.html (accessed on 13 November 2022).
- Matzinger, M.; Hahnel, S.; Preis, V.; Rosentritt, M. Polishing Effects and Wear Performance of Chairside CAD/CAM Materials. Clin. Oral. Investig. 2019, 23, 725–737. [Google Scholar] [CrossRef]
- Turker, I.; Kursoglu, P. Wear Evaluation of CAD-CAM Dental Ceramic Materials by Chewing Simulation. J. Adv. Prosthodont. 2021, 13, 281–291. [Google Scholar] [CrossRef]
- Duarte, S.; Sartori, N.; Phark, J.-H. Ceramic-Reinforced Polymers: CAD/CAM Hybrid Restorative Materials. Curr. Oral Health Rep. 2016, 3, 198–202. [Google Scholar] [CrossRef]
- Silva, T.M.; Salvia, A.C.; Carvalho, R.F.; Pagani, C.; Rocha, D.M.; Silva, E.G. Polishing for glass ceramics: Which protocol? J. Prosthodont. Res. 2014, 58, 160–170. [Google Scholar] [CrossRef]
- Sasany, R.; Ergün Kunt, G.; Koca, M.F. Influence different polishing systems on roughness and colour stability of chairside CAD/CAM blocks with laminate veneer thickness. J. Appl. Biomater. Funct. Mater. 2022, 20, 22808000221086493. [Google Scholar] [CrossRef]
- Garza, L.A.; Thompson, G.; Cho, S.-H.; Berzins, D.W. Effect of Toothbrushing on Shade and Surface Roughness of Extrinsically Stained Pressable Ceramics. J. Prosthet. Dent. 2016, 115, 489–494. [Google Scholar] [CrossRef]
- Flury, S.; Diebold, E.; Peutzfeldt, A.; Lussi, A. Effect of Artificial Toothbrushing and Water Storage on the Surface Roughness and Micromechanical Properties of Tooth-Colored CAD-CAM Materials. J. Prosthet. Dent. 2017, 117, 767–774. [Google Scholar] [CrossRef]
- Steiner, R.; Beier, U.S.; Heiss-Kisielewsky, I.; Engelmeier, R.; Dumfahrt, H.; Dhima, M. Adjusting Dental Ceramics: An in Vitro Evaluation of the Ability of Various Ceramic Polishing Kits to Mimic Glazed Dental Ceramic Surface. J. Prosthet. Dent. 2015, 113, 616–622. [Google Scholar] [CrossRef]
- Bebsh, M.; Haimeur, A.; França, R. The Effect of Different Surface Treatments on the Micromorphology and the Roughness of Four Dental CAD/CAM Lithium Silicate-Based Glass. Ceramics 2021, 4, 467–475. [Google Scholar] [CrossRef]
- Colombo, M.; Poggio, C.; Lasagna, A.; Chiesa, M.; Scribante, A. Vickers Micro-Hardness of New Restorative CAD/CAM Dental Materials: Evaluation and Comparison after Exposure to Acidic Drink. Materials 2019, 12, 1246. [Google Scholar] [CrossRef] [PubMed]
- Hölken, F.; Dietrich, H. Restoring Teeth with an Advanced Lithium Disilicate Ceramic: A Case Report and 1-Year Follow-Up. Case Rep. Dent. 2022, 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Timepoints | Thickness | LD (n = 10) | ZLS (n = 10) | ALD (n = 10) | LE (n = 10) | p Value |
|---|---|---|---|---|---|---|
| Mean (SD) | ||||||
| T1 | 0.5 mm | 0.61 (0.04) a, A | 0.68 (0.05) b | 0.51 (0.05) c | 0.58 (0.04) a | <0.001 * |
| 1 mm | 0.65 (0.06) ac, AB | 0.70 (0.05) a | 0.53 (0.07) bc | 0.58 (0.05) c | <0.001 * | |
| 1.5 mm | 0.67 (0.05) a, B | 0.71 (0.07) a | 0.56 (0.06) b | 0.59 (0.04) b | <0.001 * | |
| pvalue | 0.04 * | 0.41 | 0.22 | 0.72 | ||
| T2 | 0.5 mm | 0.77 (0.06) a, A | 0.95 (0.06) b, A | 0.65 (0.08) c | 0.76 (0.08) a | <0.001 * |
| 1 mm | 0.83 (0.07) a, AB | 1.01 (0.04) b, B | 0.70 (0.09) c | 0.79 (0.08) ac | <0.001 * | |
| 1.5 mm | 0.87 (0.04) a, B | 1.02 (0.06) b, B | 0.73 (0.08) c | 0.81 (0.07) a | <0.001 * | |
| pvalue | 0.003 * | 0.007 * | 0.12 | 0.47 | ||
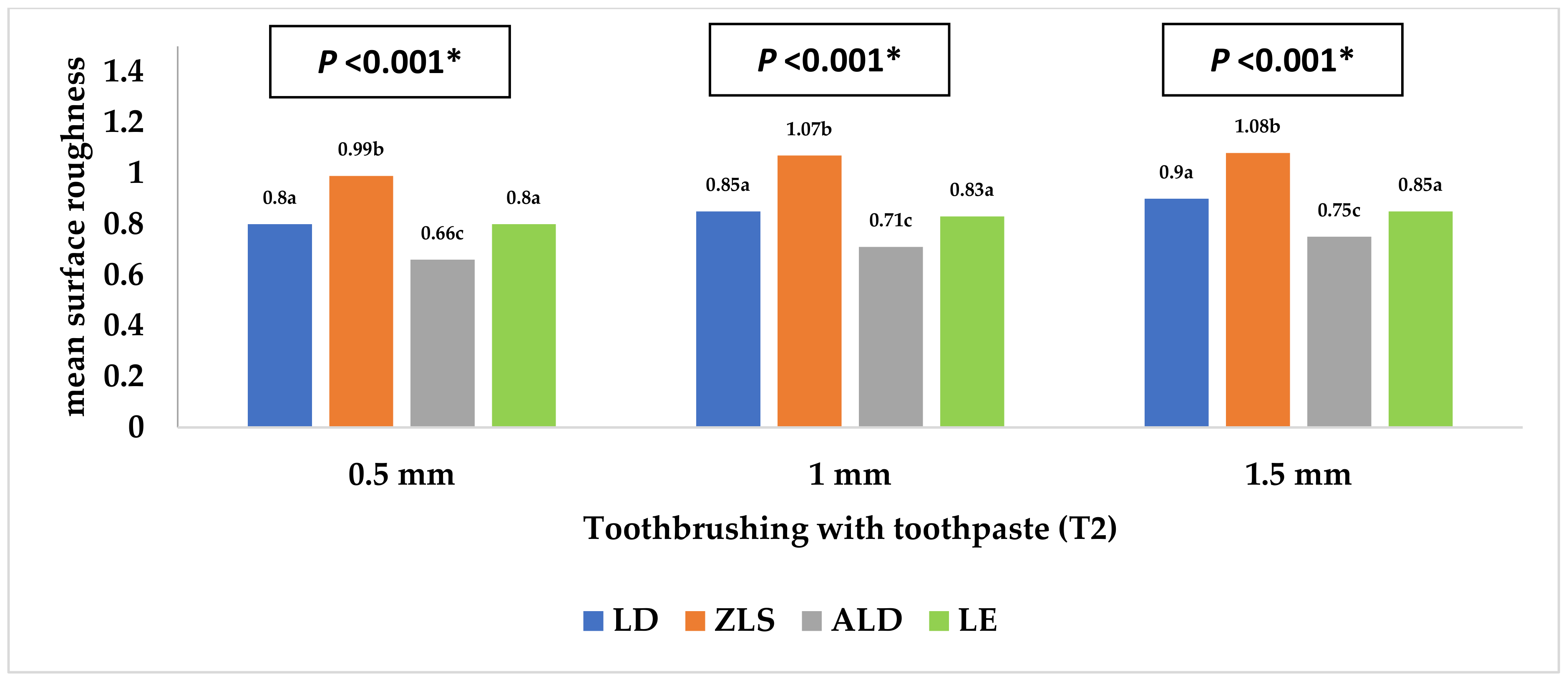
| T3 | 0.5 mm | 0.80 (0.07) a, A | 0.99 (0.09) b | 0.66 (0.09) c | 0.80 (0.06) a | <0.001 * |
| 1 mm | 0.85 (0.06) a, AB | 1.07 (0.09) b | 0.71 (0.07) c | 0.83 (0.06) a | <0.001 * | |
| 1.5 mm | 0.90 (0.06) a, B | 1.08 (0.09) b | 0.75 (0.07) c | 0.85 (0.07) a | <0.001 * | |
| pvalue | 0.003 * | 0.08 | 0.06 | 0.15 | ||
| Ceramic Thicknesses | Thickness | LD (n = 10) | ZLS (n = 10) | ALD (n = 10) | LE (n = 10) | p Value |
|---|---|---|---|---|---|---|
| Mean (SD) | ||||||
| 0.5 mm | T2-T1 | 0.16 (0.10) | 0.18 (0.11) | 0.21 (0.06) | 0.27 (0.08) | 0.07 |
| T3-T1 | 0.19 (0.06) a | 0.20 (0.07) a, b | 0.23 (0.08) a, b | 0.31 (0.10) b | 0.02 * | |
| T3-T2 | 0.03 (0.10) | 0.02 (0.10) | 0.03 (0.07) | 0.04 (0.13) | 0.99 | |
| 1 mm | T2-T1 | 0.32 (0.06) a | 0.31 (0.08) a | 0.14 (0.08) b | 0.17 (0.10) b | <0.001 * |
| T3-T1 | 0.37 (0.11) a | 0.36 (0.12) a | 0.16 (0.13) b | 0.18 (0.11) b | <0.001 * | |
| T3-T2 | 0.05 (0.08) | 0.05 (0.07) | 0.01 (0.13) | 0.02 (0.13) | 0.62 | |
| 1.5 mm | T2-T1 | 0.17 (0.10) | 0.19 (0.05) | 0.21 (0.08) | 0.21 (0.09) | 0.74 |
| T3-T1 | 0.20 (0.10) | 0.22 (0.06) | 0.25 (0.05) | 0.26 (0.06) | 0.31 | |
| T3-T2 | 0.02 (0.09) | 0.03 (0.10) | 0.04 (0.11) | 0.05 (0.11) | 0.92 | |
| Thickness | LD (n = 10) | ZLS (n = 10) | ALD (n = 10) | LE (n = 10) | p Value |
|---|---|---|---|---|---|
| Mean (SD) | |||||
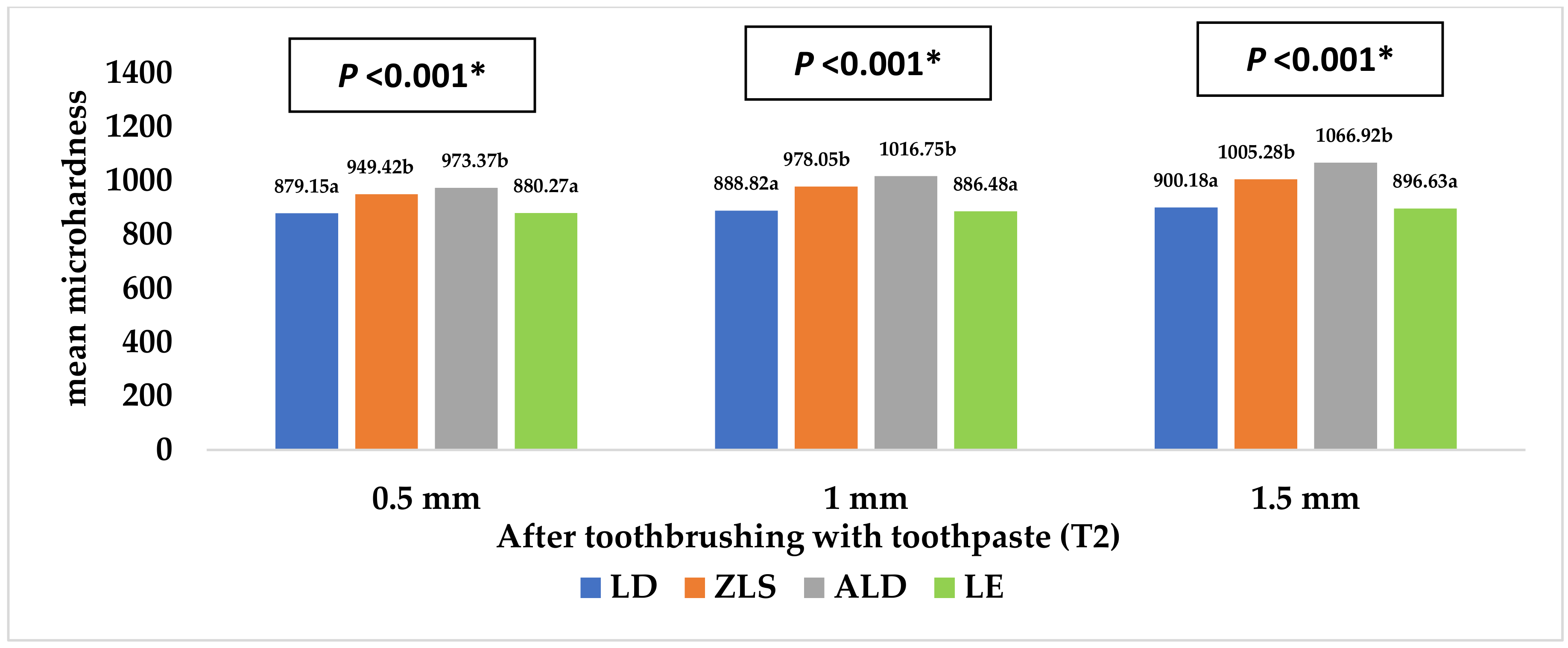
| 0.5 mm | 879.15 (29.57) a | 949.42 (37.96) b, A | 973.37 (67.29) b, A | 880.27 (40.61) a | <0.001 * |
| 1 mm | 888.82 (29.70) a | 978.05 (37.60) b, AB | 1016.75 (42.77) b, AB | 886.48 (58.99) a | <0.001 * |
| 1.5 mm | 900.18 (48.85) a | 1005.28 (34.43) b, B | 1066.92 (69.54) b, B | 896.63 (41.13) a | <0.001 * |
| pvalue | 0.46 | 0.008 * | 0.008 * | 0.74 | |
| Adjusted Mean (SE) | 95% CI | p Value | ||
|---|---|---|---|---|
| Group | LD | 0.77 (0.007) a | 0.76, 0.79 | <0.001 * |
| ZLS | 0.91 (0.007) b | 0.90, 0.93 | ||
| ALD | 0.64 (0.007) c | 0.63, 0.66 | ||
| LE | 0.73 (0.007) d | 0.72, 0.75 | ||
| Thickness | 0.5 mm | 0.73 (0.006) a | 780.48, 811.34 | <0.001 * |
| 1 mm | 0.77 (0.006) b | 777.55, 808.41 | ||
| 1.5 mm | 0.80 (0.006) c | 805.56, 836.42 | ||
| Toothbrushing | T0 | 0.61 (0.006) a | 664.95, 695.81 | <0.001 * |
| T1 | 0.83 (0.006) b | 850.13, 880.99 | ||
| T2 | 0.86 (0.006) c | 848.51, 879.36 | ||
| Adjusted Mean (SE) | 95% CI | p Value | ||
|---|---|---|---|---|
| Group | LD | 889.38 (8.64) a | 872.27, 906.49 | <0.001 * |
| ZLS | 977.58 (8.64) b | 960.47, 994.69 | ||
| ALD | 1019.01 (8.64) c | 1001.90, 1036.12 | ||
| LE | 887.79 (8.64) a | 870.68, 904.90 | ||
| Thickness | 0.5 mm | 920.55 (7.48) a | 905.74, 935.37 | <0.001 * |
| 1 mm | 942.53 (7.48) ab | 927.71, 957.34 | ||
| 1.5 mm | 967.25 (7.48) b | 952.43, 982.07 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ellakany, P.; Madi, M.; Aly, N.M.; Alshehri, T.; Alameer, S.T.; Al-Harbi, F.A. Influences of Different CAD/CAM Ceramic Compositions and Thicknesses on the Mechanical Properties of Ceramic Restorations: An In Vitro Study. Materials 2023, 16, 646. https://doi.org/10.3390/ma16020646
Ellakany P, Madi M, Aly NM, Alshehri T, Alameer ST, Al-Harbi FA. Influences of Different CAD/CAM Ceramic Compositions and Thicknesses on the Mechanical Properties of Ceramic Restorations: An In Vitro Study. Materials. 2023; 16(2):646. https://doi.org/10.3390/ma16020646
Chicago/Turabian StyleEllakany, Passent, Marwa Madi, Nourhan M. Aly, Turki Alshehri, Shahad T. Alameer, and Fahad A. Al-Harbi. 2023. "Influences of Different CAD/CAM Ceramic Compositions and Thicknesses on the Mechanical Properties of Ceramic Restorations: An In Vitro Study" Materials 16, no. 2: 646. https://doi.org/10.3390/ma16020646
APA StyleEllakany, P., Madi, M., Aly, N. M., Alshehri, T., Alameer, S. T., & Al-Harbi, F. A. (2023). Influences of Different CAD/CAM Ceramic Compositions and Thicknesses on the Mechanical Properties of Ceramic Restorations: An In Vitro Study. Materials, 16(2), 646. https://doi.org/10.3390/ma16020646