
The Influence of Cement Layer Thickness on the Stress State of Metal Inlay Restorations—Photoelastic Analysis

 ,
,
Abstract
1. Introduction
- The change in cement volume does not affect shrinkage stress.
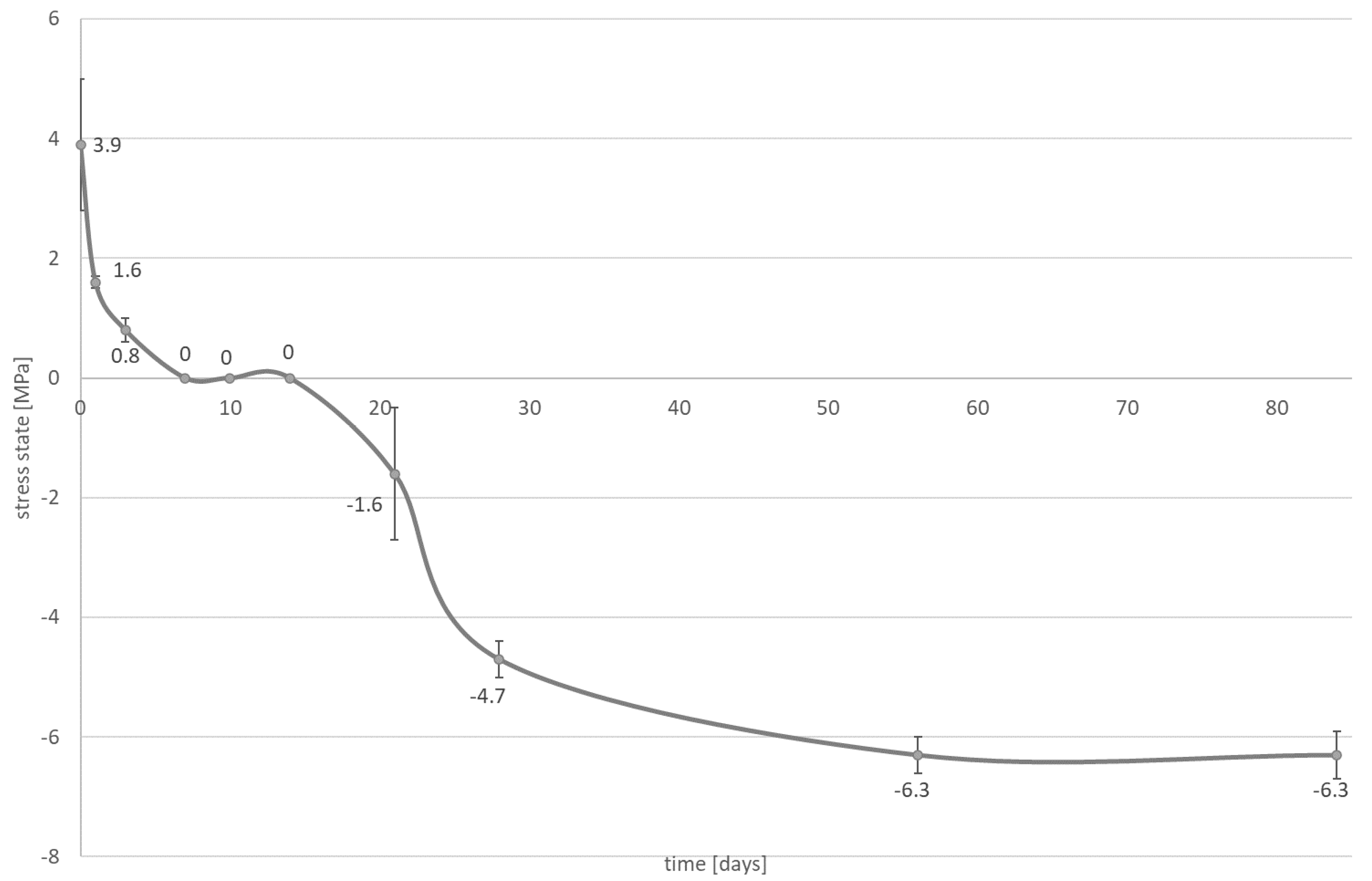
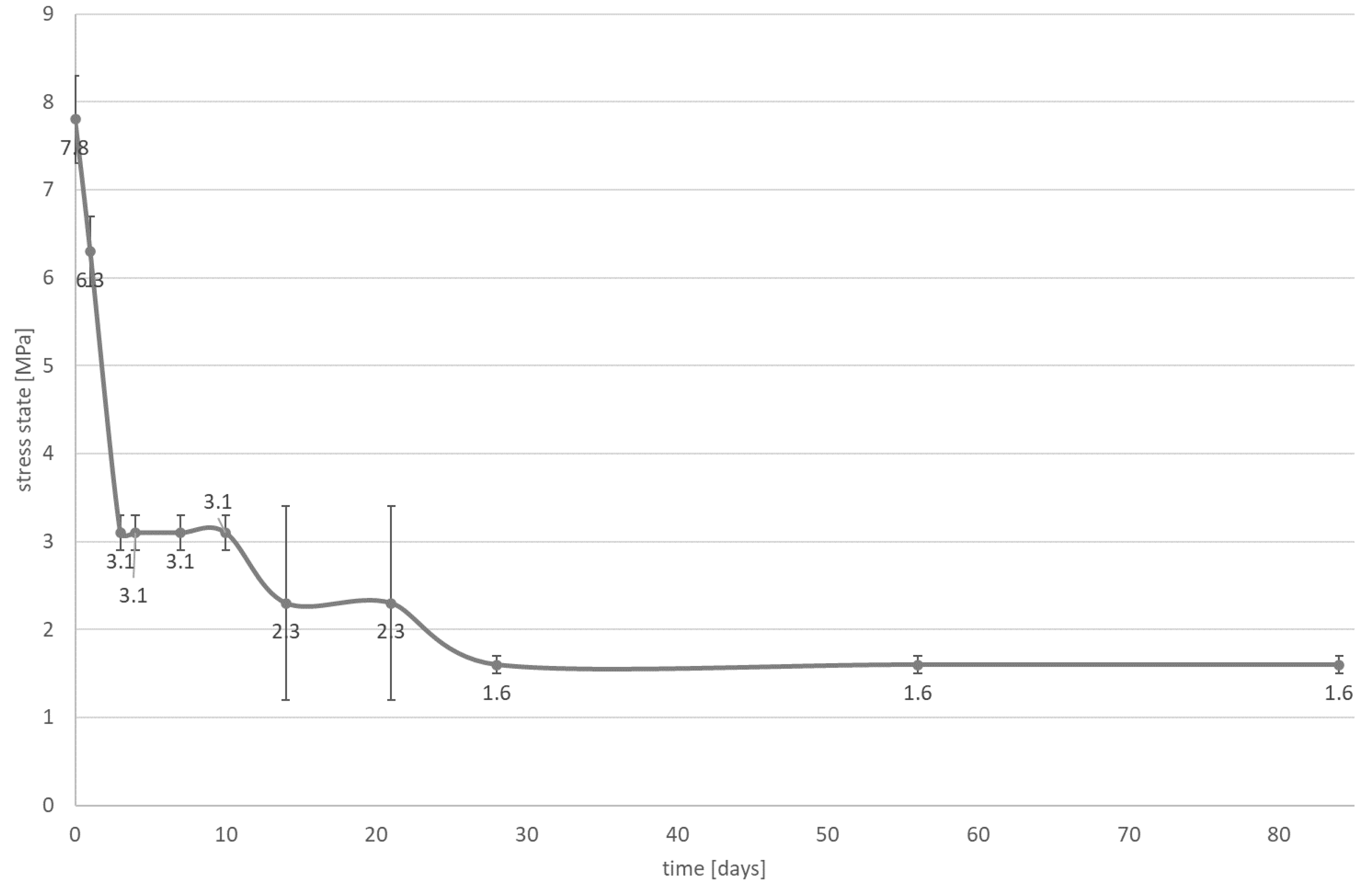
- Water absorption does not affect the state of stress.
2. Materials and Methods
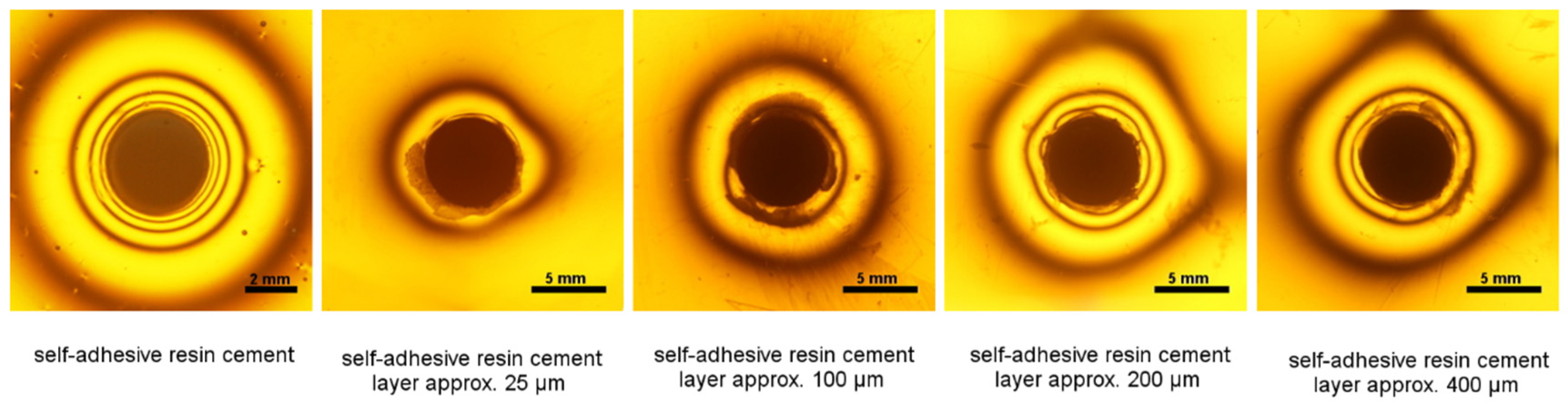
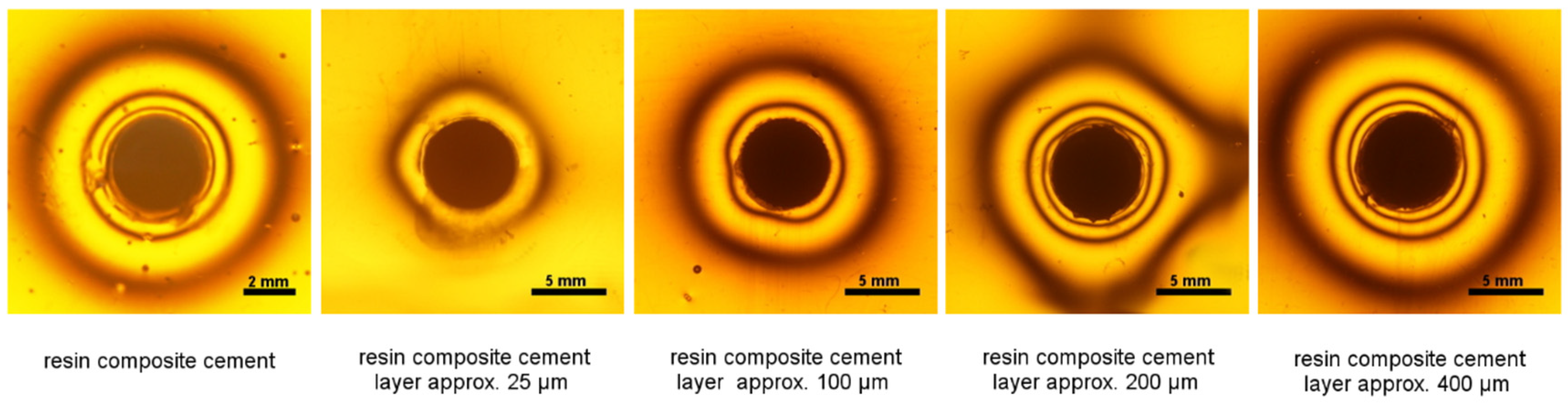
2.1. Photoelastic Study—The Dependence of the Cement Layer Thickness on Shrinkage Stress
2.2. Photoelastic Study—Influence of Water Absorption on Stress State
3. Results
3.1. Photoelastic Study—Dependence of Cement Layer Thickness on Shrinkage Stress
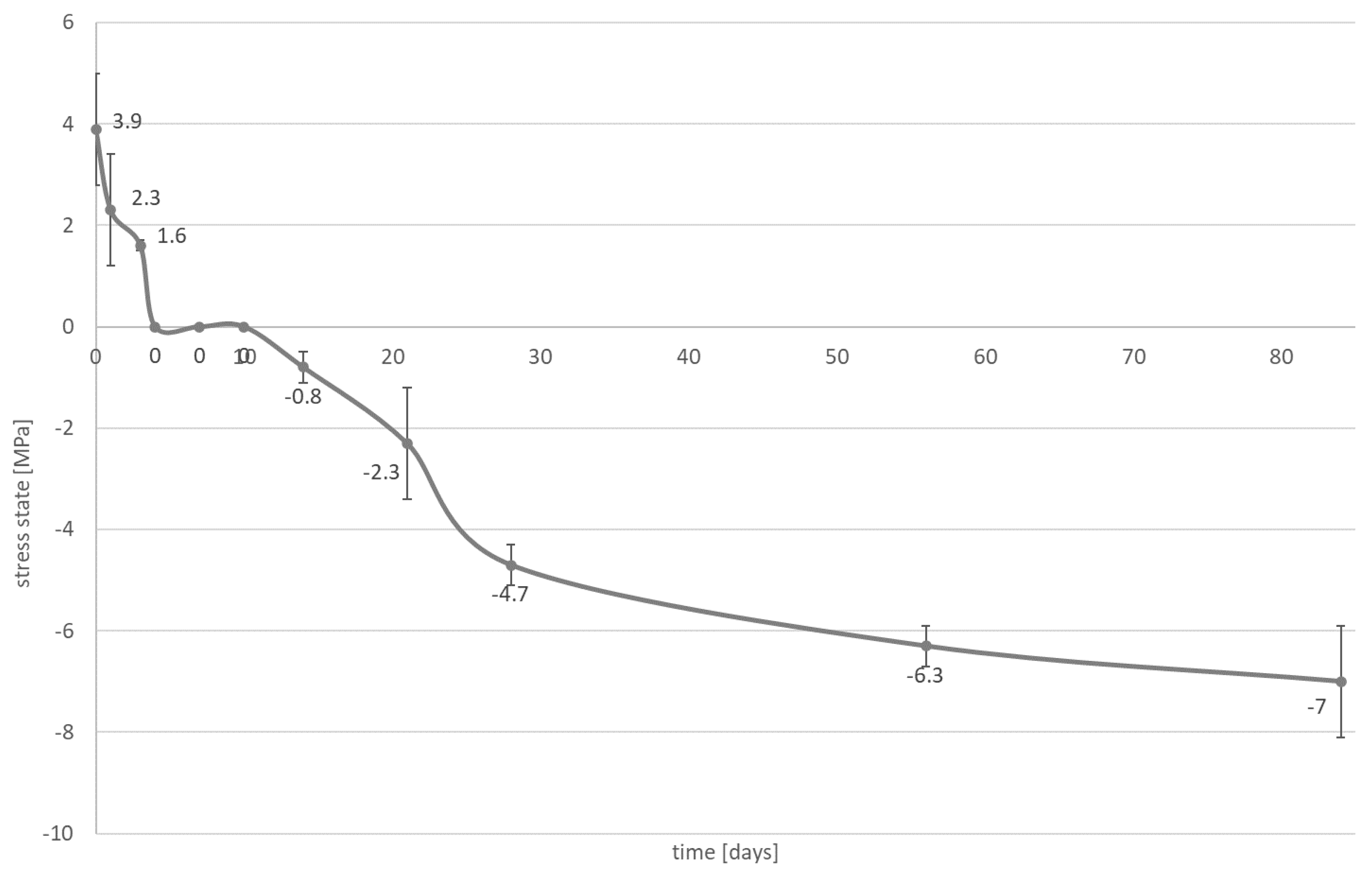
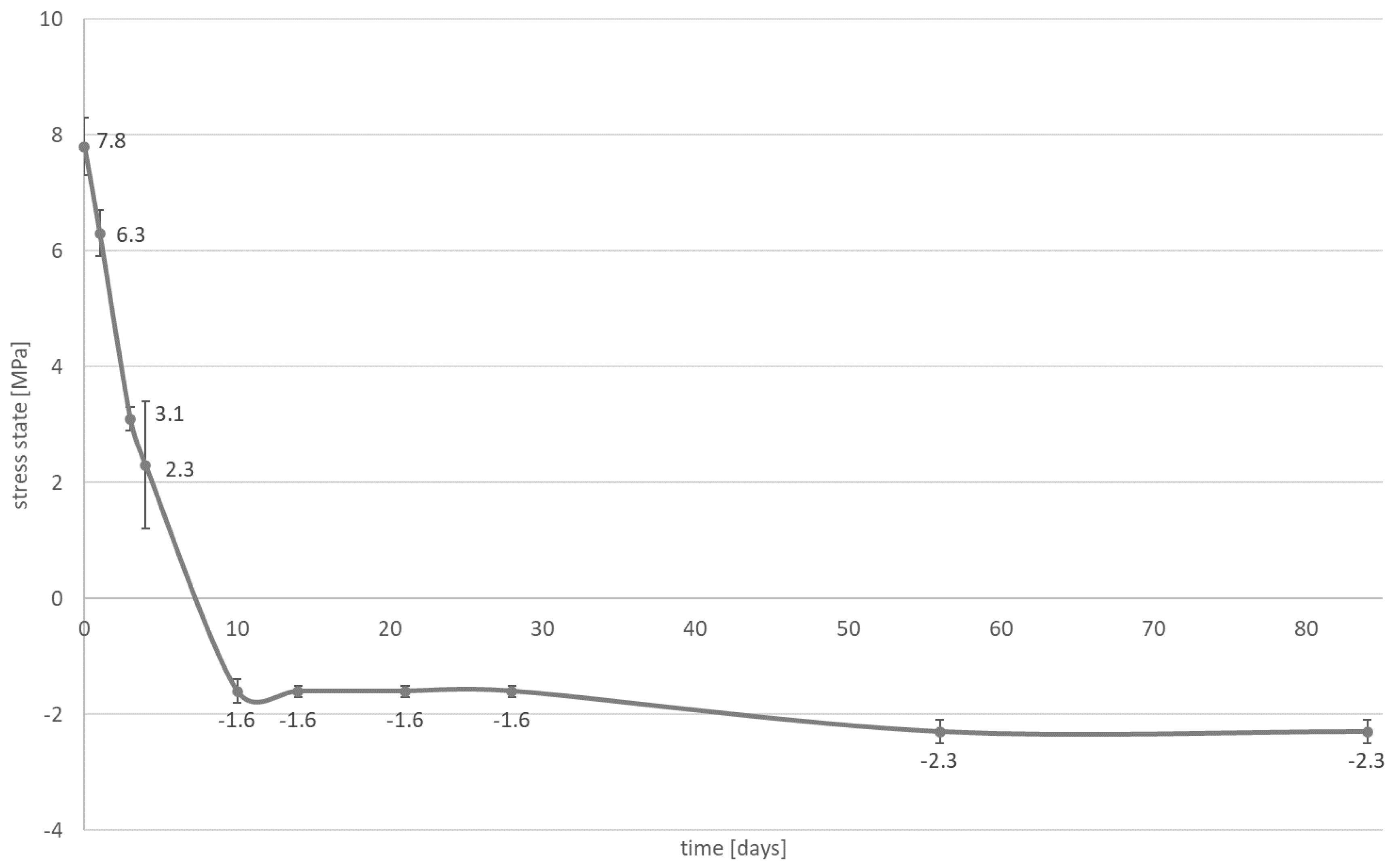
3.2. Photoelastic Study—Influence of Water Absorption on Stress State
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Clinical Significance
References
- Aspros, A. Inlays & Onlays Clinical Experiences and Literature Review. J. Dent. Health Oral Disord. Ther. 2015, 2, 26–31. [Google Scholar] [CrossRef]
- Edelhoff, D.; Spiekermann, H.; Yildirim, M. Metal-free inlay-retained fixed partial dentures. Quintessence Int. 2001, 2, 269–281. [Google Scholar]
- Alshiddi, I.F.; Aljinbaz, A. Fracture resistance of endodontically treated teeth restored with indirect composite inlay and onlay restorations—An in vitro study. Saudi Dent. J. 2016, 28, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Al-Fouzan, A.F. Gravimetric analysis of removed tooth structure associated with different preparation designs. Saudi J. Dent. Res. 2016, 7, 1–6. [Google Scholar] [CrossRef]
- Lutz, F.; Gohring, T.N. Fiber-reinforced inlay fixed partial dentures: Maximum preservation of dental hard tissue. J. Esthet. Dent. 2000, 12, 164–171. [Google Scholar] [CrossRef]
- Wolfart, S.; Kern, M. A new design for all-ceramic inlay-retained fixed partial dentures: A report of 2 cases. Quintessence Int. 2006, 37, 27–33. [Google Scholar]
- Mehl, C.J.; Ludwig, K.; Steiner, M.; Kern, M. Fracture strength of prefabricated all-ceramic posterior inlay-retained fixed dental prostheses. Dent. Mater. 2010, 26, 67–75. [Google Scholar] [CrossRef]
- Castillo-Oyagüe, R.; Sancho-Esper, R.; Lynch, C.D.; Suárez-García, M.-J. All-ceramic inlay-retained fixed dental prostheses for replacing posterior missing teeth: A systematic review. J. Prosthodont. Res. 2018, 62, 10–23. [Google Scholar] [CrossRef]
- Sabatini, C.; Patel, M.; D’Silva, E. In Vitro Shear Bond Strength of Three Self-adhesive Resin Cements and a Resin-Modified Glass Ionomer Cement to Various Prosthodontic Substrates. Oper. Dent. 2013, 38, 186–196. [Google Scholar] [CrossRef]
- Diaz-Arnold, A.M.; Vargas, M.A.; Haselton, D.R. Current status of luting agents for fixed prosthodontics. J. Prosthet. Dent. 1999, 81, 135–141. [Google Scholar] [CrossRef]
- Manso, A.P.; Carvalho, R.M. Dental Cements for Luting and Bonding Restorations. Dent. Clin. N. Am. 2017, 61, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Oyar, P. The effects of post-core and crown material and luting agents on stress distribution in tooth restorations. J. Prosthet. Dent. 2014, 112, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, I.K.C.S.; Lima-Arsati, Y.B.; Basting, R.T.; França, F.M.G. Waiting Time for Coronal Preparation and the Influence of Different Cements on Tensile Strength of Metal Posts. Int. J. Dent. 2012, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.J. Why use resin cements? J. Am. Dent. Assoc. 2010, 141, 204–206. [Google Scholar] [CrossRef] [PubMed]
- Vrochari, A.D.; Eliades, G.; Hellwig, E.; Wrbas, K.-T. Curing efficiency of four self-etching, self-adhesive resin cements. Dent. Mater. 2009, 25, 1104–1108. [Google Scholar] [CrossRef] [PubMed]
- Hikita, K.; Van Meerbeek, B.; De Munck, J.; Ikeda, T.; Van Landuyt, K.; Maida, T.; Lambrechts, P.; Peumans, M. Bonding effectiveness of adhesive luting agents to enamel and dentin. Dent. Mater. 2007, 23, 71–80. [Google Scholar] [CrossRef]
- Turkistani, A.; Sadr, A.; Shimada, Y.; Nikaido, T.; Sumi, Y.; Tagami, J. Sealing performance of resin cements before and after thermal cycling: Evaluation by optical coherence tomography. Dent. Mater. 2014, 30, 993–1004. [Google Scholar] [CrossRef]
- Hitz, T.; Stawarczyk, B.; Fischer, J.; Hämmerle, C.H.F.; Sailer, I. Are self-adhesive resin cements a valid alternative to conventional resin cements? A laboratory study of the long-term bond strength. Dent. Mater. 2012, 28, 1183–1190. [Google Scholar] [CrossRef]
- Sokolowski, G.; Szczesio-Wlodarczyk, A.; Bociong, K.; Kaluzinska, K.; Lapinska, B.; Sokołowski, J.; Domarecka, M.; Lukomska-Szymanska, M. Dental Resin Cements—The Influence of Water Sorption on Contraction Stress Changes and Hydroscopic Expansion. Materials 2018, 11, 973. [Google Scholar] [CrossRef]
- Goujat, A.; Abouelleil, H.; Colon, P.; Jeannin, C.; Pradelle, N.; Seux, D.; Grosgogeat, B. Marginal and internal fit of CAD-CAM inlay/onlay restorations: A systematic review of in vitro studies. J. Prosthet. Dent. 2019, 121, 590–597.e3. [Google Scholar] [CrossRef]
- Rippe, M.P.; Monaco, C.; Missau, T.; Wandscher, V.F.; Volpe, L.; Scotti, R.; Bottino, M.A.; Valandro, L.F. Survival rate and load to failure of premolars restored with inlays: An evaluation of different inlay fabrication methods. J. Prosthet. Dent. 2019, 121, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Sokolowski, J.; Konieczny, B.; Krasowski, M.; Bociong, K.; Sokołowski, G.; Domarecka, M.; Lukomka-Szymanska, M. Stresses generated during the cementation of crown posts. In Proceedings of the 34th Scientific and Training Conference of the Prosthetics Section of the Polish Dental Society, Gdańsk, Poland, 1–3 June 2017. [Google Scholar]
- Domarecka, M.; Sokołowski, K.; Krasowski, M.; Lukomska-Szymanska, M.; Sokołowski, J. The Shrinkage Stress of Modified Flowable Dental Composites. Dent. Med. Probl. 2015, 52, 424–433. [Google Scholar] [CrossRef]
- Domarecka, M.; Sokołowski, K.; Krasowski, M.; Szczesio, A.; Bociong, K.; Sokołowski, J.; Łukomska-Szymańska, M.M. Influence of water sorption on the shrinkage stresses of dental composites. J. Stoma 2016, 64, 476–483. [Google Scholar]
- Bociong, K.; Szczesio, A.; Sokolowski, K.; Domarecka, M.; Sokolowski, J.; Krasowski, M.; Lukomska-Szymanska, M. The influence of water sorption of dental light-cured composites on shrinkage stress. Materials 2017, 10, 1142. [Google Scholar] [CrossRef] [PubMed]
- Muris, J.; Feilzer, A.J. Polymerization shrinkage and contraction stress of dental resin composites. Dent. Mater. 2005, 21, 1150–1157. [Google Scholar] [CrossRef]
- Domarecka, M. Some properties of flowable low-shrinkage dental composites. Wybrane właściwości materiałów kompozytowych typu flow o niskim skurczu polimeryzacyjnym. Przem. Chem. 2014, 93, 1000–1003. [Google Scholar] [CrossRef]
- Bociong, K.; Krasowski, M.; Domarecka, M.; Sokołowski, J. Effect of the method of photopolymerization of dental composites based on dimethacrylate resin on the shrinkage stresses and selected properties of the cured material. Polimery 2016, 61, 499–508. [Google Scholar] [CrossRef]
- Al Sunbul, H.; Silikas, N.; Watts, D.C. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent. Mater. 2016, 32, 998–1006. [Google Scholar] [CrossRef]
- Spinell, T.; Schedle, A.; Watts, D.C. Polymerization shrinkage kinetics of dimethacrylate resin-cements. Dent. Mater. 2009, 25, 1058–1066. [Google Scholar] [CrossRef]
- Feilzer, A.; De Gee, A.; Davidson, C. Increased Wall-to-Wall Curing Contraction in Thin Bonded Resin Layers. J. Dent. Res. 1989, 68, 48–50. [Google Scholar] [CrossRef]
- Frassetto, A.; Navarra, C.O.; Marchesi, G.; Turco, G.; Di Lenarda, R.; Breschi, L.; Ferracane, J.L.; Cadenaro, M. Kinetics of polymerization and contraction stress development in self-adhesive resin cements. Dent. Mater. 2012, 28, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Feilzer, A.; De Gee, A.; Davidson, C. Relaxation of Polymerization Contraction Shear Stress by Hygroscopic Expansion. J. Dent. Res. 1990, 69, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Szczesio-Wlodarczyk, A.; Sokołowski, J.; Kleczewska, J.; Bociong, K. Ageing of Dental Composites Based on Methacrylate Resins—A Critical Review of the Causes and Method of Assessment. Polymer 2020, 12, 882. [Google Scholar] [CrossRef] [PubMed]
- Sahebalam, R.; Boruziniat, A.; Mohammadzadeh, F.; Rangrazi, A. Effect of the Time of Salivary Contamination during Light Curing on Degree of Conversion and Microhardness of a Restorative Composite Resin. Biomimetics 2018, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Malacarne, J.; Carvalho, R.M.; De Goes, M.F.; Svizero, N.; Pashley, D.H.; Tay, F.R.; Yiu, C.K.; Carrilho, M.R.D.O. Water sorption/solubility of dental adhesive resins. Dent. Mater. 2006, 22, 973–980. [Google Scholar] [CrossRef]
- Park, J.; Eslick, J.; Ye, Q.; Misra, A.; Spencer, P. The influence of chemical structure on the properties in methacrylate-based dentin adhesives. Dent. Mater. 2011, 27, 1086–1093. [Google Scholar] [CrossRef]
- Wei, Y.-J.; Silikas, N.; Zhang, Z.-T.; Watts, D.C. Hygroscopic dimensional changes of self-adhering and new resin-matrix composites during water sorption/desorption cycles. Dent. Mater. 2011, 27, 259–266. [Google Scholar] [CrossRef]
- Braga, R.R.; Boaro, L.C.C.; Kuroe, T.; Azevedo, C.L.N.; Singer, J.M. Influence of cavity dimensions and their derivatives (volume and ‘C’ factor) on shrinkage stress development and microleakage of composite restorations. Dent. Mater. 2006, 22, 818–823. [Google Scholar] [CrossRef]
- Spazzin, A.O.; Galafassi, D.; De Meira-Júnior, A.D.; Braz, R.; Garbin, C.A. Influence of Post and Resin Cement on Stress Distribution of Maxillary Central Incisors Restored with Direct Resin Composite. Oper. Dent. 2009, 34, 223–229. [Google Scholar] [CrossRef]
- May, L.G.; Kelly, J.R. Influence of resin cement polymerization shrinkage on stresses in porcelain crowns. Dent. Mater. 2013, 29, 1073–1079. [Google Scholar] [CrossRef]
- Stomatologia—Materiały Polimerowe do Odbudowy; PN-EN ISO 4049:2010; Polski Komitet Normalizacyjny: Warszawa, Poland, 2010.
- Neppelenbroek, K.H. The clinical challenge of achieving marginal adaptation in direct and indirect restorations. J. Appl. Oral Sci. 2015, 23, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, K.; Mierzwińska-Nastalska, E.; Molak, R.; Kożuchowski, M.; Pakieła, Z. Strength and thickness of the layer of materials used for ceramic veneers bonding. Acta Bioeng. Biomech. 2012, 14, 75–78. [Google Scholar] [PubMed]
- Versluis, A.; Tantbirojn, D.; Lee, M.S.; Tu, L.S.; Delong, R. Can hygroscopic expansion compensate polymerization shrinkage? Part I. Deformation of restored teeth. Dent. Mater. 2011, 27, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.R.; Ferracane, J.L.; Condon, J.R. Polymerization contraction stress in dual-cure cements and its effect on interfacial integrity of bonded inlays. J. Dent. 2002, 30, 333–340. [Google Scholar] [CrossRef]
- Alrahlah, A.; Silikas, N.; Watts, D.C. Hygroscopic expansion kinetics of dental resin-composites. Dent. Mater. 2014, 30, 143–148. [Google Scholar] [CrossRef]
- Sindel, J.; Frankenberger, R.; Krämer, N.; Petschelt, A. Crack formation of all-ceramic crowns dependent on different core build-up and luting materials. J. Dent. 1999, 27, 175–181. [Google Scholar] [CrossRef]
- Sokołowski, G.; Szczesio-Wlodarczyk, A.; Konieczny, B.; Bociong, K.; Sokołowski, J. Comparative evaluation of the mechanical properties of resin, self-adhesive and adhesive cements. Prosthodontics 2018, 68, 415–424. [Google Scholar] [CrossRef]
- Pishevar, L.; Ghavam, M.; Pishevar, A. Stress analysis of two methods of ceramic inlay preparation by finite element. Indian J. Dent. Res. 2014, 25, 364. [Google Scholar] [CrossRef]
- Rees, J.; Jacobsen, P.H. Stress generated by lutting resins during cementation of composite and ceramic inlays. J. Oral Rehabil. 1992, 19, 115–122. [Google Scholar] [CrossRef]
- Watts, D. Composite inlay systems: Material properties and design. J. Dent. 1990, 18, 67–70. [Google Scholar]
- Alster, D.; Feilzer, A.J.; De Gee, A.J.; Davidson, C.L. Polymerization contraction stress in thin resin composite layers as a function of layer thickness. Dent. Mater. 1997, 13, 146–150. [Google Scholar] [CrossRef]
- Hübsch, P.F.; Middleton, J.; Knox, J. A finite element analysis of the stress at the restoration-tooth interface, comparing inlays and bulk fillings. Biomaterials 2000, 21, 1015–1019. [Google Scholar] [CrossRef]
- Dejak, B.; Młotkowski, A. A comparison of stresses in molar teeth restored with inlays and direct restorations, including polymerization shrinkage of composite resin and tooth loading during mastication. Dent. Mater. 2015, 31, e77–e87. [Google Scholar] [CrossRef] [PubMed]
- Angker, L.; Swain, M.V.; Kilpatrick, N. Micro-mechanical characterisation of the properties of primary tooth dentine. J. Dent. 2003, 31, 261–267. [Google Scholar] [CrossRef]
- Kinney, J.; Balooch, M.; Marshall, G.; Marshall, S. A micromechanics model of the elastic properties of human dentine. Arch. Oral Biol. 1999, 44, 813–822. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Type | Composition | Curing Time (s) | Manufacturer |
|---|---|---|---|---|
| NX3 | Resin composite cement | TEGDMA, bis-GMA, fluoro-aluminosilicate glass (67.5% wt./47% vol.), activators, stabilizers, radiopaque agent | 20 | Kerr |
| Maxcem Elite Chroma | Self-adhesive resin cement | HEMA, GDM, UDMA, 1,1,3,3-tetramethylbutyl hydroperoxide TEGDMA, fluoro-aluminosilicate glass, GPDM, barium glass filler, fumed silica (69% wt.) | 10 | Kerr |
| Cement Layer Thickness | σr MPa | σθ MPa | Shrinkage Stress MPa |
|---|---|---|---|
| the cement itself | 6.6 ± 0.1 | −7.9 ± 0.1 | 14.5 ± 0.1 |
| approximately 25 µm | 0.9 ± 0.1 | −2.1 ± 0.2 | 3.1 ± 0.3 |
| approximately 100 µm | 2.8 ± 0.4 | −4.2 ± 0.7 | 7.0 ± 0.5 |
| approximately 200 µm | 3.8 ± 0.2 | −5.4 ± 0.3 | 9.2 ± 0.5 |
| approximately 400 µm | 3.8 ± 0.2 | −5.4 ± 0.3 | 9.2 ± 0.5 |
| Cement Layer Thickness | σr MPa | σθ MPa | Shrinkage Stress MPa |
|---|---|---|---|
| the cement itself | 3.9 ± 0.4 | −5.2 ± 0.5 | 9.1 ± 0.9 |
| approximately 25 µm | 0.7 ± 0.1 | −1.8 ± 0.2 | 2.6 ± 0.3 |
| approximately 100 µm | 3.0 ± 0.2 | −4.6 ± 0.2 | 7.6 ± 0.4 |
| approximately 200 µm | 3.9 ± 0.2 | −5.4 ± 0.2 | 9.3 ± 0.4 |
| approximately 400 µm | 4.8 ± 0.2 | −5.9 ± 0.3 | 10.7 ± 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sokolowski, G.; Krasowski, M.; Szczesio-Wlodarczyk, A.; Konieczny, B.; Sokolowski, J.; Bociong, K. The Influence of Cement Layer Thickness on the Stress State of Metal Inlay Restorations—Photoelastic Analysis. Materials 2021, 14, 599. https://doi.org/10.3390/ma14030599
Sokolowski G, Krasowski M, Szczesio-Wlodarczyk A, Konieczny B, Sokolowski J, Bociong K. The Influence of Cement Layer Thickness on the Stress State of Metal Inlay Restorations—Photoelastic Analysis. Materials. 2021; 14(3):599. https://doi.org/10.3390/ma14030599
Chicago/Turabian StyleSokolowski, Grzegorz, Michal Krasowski, Agata Szczesio-Wlodarczyk, Bartlomiej Konieczny, Jerzy Sokolowski, and Kinga Bociong. 2021. "The Influence of Cement Layer Thickness on the Stress State of Metal Inlay Restorations—Photoelastic Analysis" Materials 14, no. 3: 599. https://doi.org/10.3390/ma14030599
APA StyleSokolowski, G., Krasowski, M., Szczesio-Wlodarczyk, A., Konieczny, B., Sokolowski, J., & Bociong, K. (2021). The Influence of Cement Layer Thickness on the Stress State of Metal Inlay Restorations—Photoelastic Analysis. Materials, 14(3), 599. https://doi.org/10.3390/ma14030599