
Comparison of Silane Heat Treatment by Laser and Various Surface Treatments on Microtensile Bond Strength of Composite Resin/Lithium Disilicate




Abstract
:1. Introduction
2. Materials and Experiments
- S group (silane): A silane coupling agent (Monobond S, Ivoclar Vivadent, Schaan, Liechtenstein) was applied to the surface specimens for 1 min and then air-dried for 30 s.
- SC group: Air abrasion was applied by 30 m aluminum oxide (Al2O3) particles modified with silica (Cojet Sand; Seefeld, Germany) at a pressure of 2.3 bar from a distance of 10 mm for 15 s (tribochemical silica coating). Then silane was applied.
- ALS (AL ± silane) group: Sandblasting was performed with 50 m Al2O3 particles (Korox 50; Bego Bremen, Germany) at a pressure of 0.3 MPa from a distance of 10 mm for 10 s [38]. Then silane was applied.
- SHT1 group (laser ± silane): Specimens were irradiated for 30 s with an Er:YAG laser using a non-contact head. The laser had a frequency of 20 Hz, a long pulse of 5 W, and a power of 250 mJ.
- SHT2 group (silane ± heat treatment): Silane was applied on the surface according to the same procedure and then heat treatment was performed in the furnace (100 °C, 1 min).
- HF group: The surface of the specimens was etched for 20s with 9.5 percent HF gel (Porcelain Etch; Ultradent Products Inc, South Jordan, UT, USA), washed for 1 min, and air-dried for 1 min.
- HFS group (HF ± silane): The acid-etching methodology was used. The technique was also followed by silanization.
2.1. Microtensile Bond Strength Test (µTBS)
2.2. Failure Mode
2.3. Scanning Electron Microscopi (SEM)
2.4. Statistical Analysis
3. Results
3.1. Microtensile Bond Strength Test (µTBS)
3.2. Failure Mode
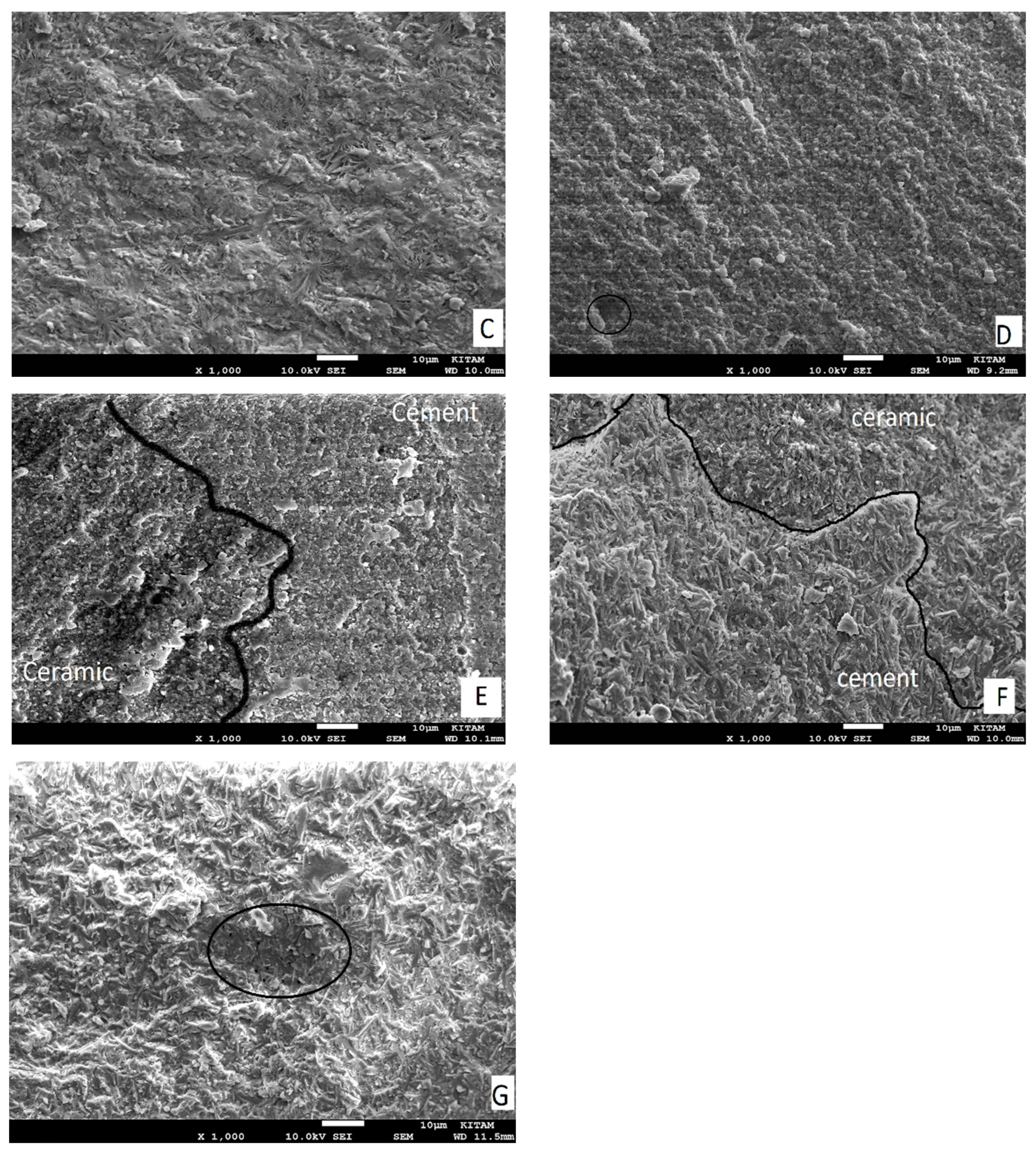
3.3. Scanning Electron Microscopi (SEM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tian, T.; Tsoi, J.K.H.; Matinlinna, J.P.; Burrow, M.F. Aspects of bonding between resin luting cements and glass-ceramic materials. Dent. Mater. 2014, 30, 147–162. [Google Scholar] [CrossRef]
- Marocho, S.M.S.; Özcan, M.; Amaral, R.; Bottino, M.A.; Valandro, L.F. Effect of resin cement type on the microtensile bond strength to lithium disilicate ceramic and dentin using different test assemblies. J. Adhes. Dent. 2013, 15, 361–368. [Google Scholar]
- Colares, R.C.R.; Neri, J.R.; de Souza, A.M.B.; Pontes, K.M.; Mendonça, J.S.; Santiago, S.L. Effect of surface preparements on the microtensile bond strength of lithium-disilicate ceramic repaired with composite resin. Braz. Dent. J. 2013, 24, 349–352. [Google Scholar] [CrossRef]
- Sundfeld, D.; Correr-Sobrinho, L.; Pini, N.I.P.; Costa, A.R.; Sundfeld, R.H.; Pfeifer, C.S.; Martins, L.R.M. Heat treatment-improved bond strength of resin cement to lithium disilicate glass-ceramic. Ceram. Int. 2016, 42, 10071–10078. [Google Scholar] [CrossRef] [Green Version]
- Abduljabbar, T.; AlQahtani, M.A.; Jeaidi, Z.A.; Vohra, F. Influence of silane and heated silane on the bond strength of lithium disilicate ceramics-an in vitro study. Pak. J. Med. Sci. 2016, 32, 550–554. [Google Scholar] [CrossRef]
- Araujo, N.S.; Moda, M.D.; Silva, E.A.; Zavanelli, A.C.; Mazaro, J.V.Q.; Pellizzer, E.P. Survival of all-ceramic restorations after a minimum follow-up of five years: A systematic review. Quintessence Int. 2016, 47, 395–405. [Google Scholar]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.F.A.; Bonfante, E.A. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Cappare, P.; Ferrini, F.; Mariani, G.; Nagni, M.; Cattoni, F. Implant rehabilitation of edentulous jaws with predominantly monolithic zirconia compared to metal-acrylic prostheses: A 2-year retrospective clinical study. J. Biol. Regul. Homeost. Agents 2021, 35, 99–112. [Google Scholar]
- Ritter, R.G. Multifunctional uses of a novel ceramic-lithium disilicate. J. Esthet. Restor. Dent. 2010, 22, 332–341. [Google Scholar] [CrossRef]
- Huang, S.; Li, Y.; Wei, S.; Huang, Z.; Gao, W.; Cao, P. A novel high-strength lithium disilicate glass-ceramic featuring a highly intertwined microstructure. J. Eur. Ceram. Soc. 2017, 37, 1083–1094. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Sleem, D. Microtensile bond strength of lithium disilicate ceramics to resin adhesives. J. Adhes. Dent. 2014, 16, 547–552. [Google Scholar]
- Campaner, L.M.; Silveira, M.P.M.; de Andrade, G.S.; Borges, A.L.S.; Bottino, M.A.; Dal Piva, A.M.O.; Giudice, R.L.; Ausiello, P.; Tribst, J.P.M. Influence of polymeric restorative materials on the stress distribution in posterior fixed partial dentures: 3D finite element analysis. Polymers 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Tetè, G.; Sacchi, L.; Camerano, C.; Nagni, M.; Capelli, O.; Vercellin, S.C.; La Rocca, G.; Polizzi, E. Management of the delicate phase of the temporary crown: An in vitro study. J. Biol. Regul. Homeost. Agents 2020, 34, 69–80. [Google Scholar] [PubMed]
- Conrad, H.J.; Seong, W.J.; Pesun, I.J. Current ceramic materials and systems with clinical recommendations: A systematic review. J. Prosthet. Dent. 2007, 98, 389–404. [Google Scholar] [CrossRef]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef]
- Pollington, S.; Fabianelli, A.; van Noort, R. Microtensile bond strength of a resin cement to a novel fluorcanasite glass-ceramic following different surface treatments. Dent. Mater. 2010, 26, 864–872. [Google Scholar] [CrossRef]
- Lung, C.Y.K.; Matinlinna, J.P. Aspects of silane coupling agents and surface conditioning in dentistry: An overview. Dent. Mater. 2012, 28, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Hakimaneh, M.S.; Sayed-Shojaedin, S.; Ghavami-Lahiji, M.; Chokr, A.; Moraditalab, A. Effect of Silane Heat Treatment by Laser on the Bond Strength of a Repair Composite to Feldspathic Porcelain. J. Prosthodont. 2020, 29, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, T.; Eraslan, O. The effect of silane applied to glass-ceramics on surface structure and bonding strength at different temperatures. J. Adv. Prosthodont. 2016, 8, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarda, G.B.; Correr, A.B.; Gonçalves, L.S.; Costa, A.R.; Borges, G.A.; Sinhoreti, M.A.C.; Correr-Sobrinho, L. Effects of surface treatments, thermocycling, and cyclic loading on the bond strength of a resin cement bonded to a lithium disilicate glass-ceramic. Oper. Dent. 2013, 38, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Spohr, A.M.; Sobrinho, L.C.; Consani, S.; Sinhoretti, M.A.C.; Knowles, J.C. Influence of surface conditioning and silane agent on the bond of resin to IPS Empress 2 ceramic. Int. J. Prosthodont. 2003, 16, 277–282. [Google Scholar] [PubMed]
- Kim, B.K.; Bae, H.E.K.; Shim, J.S.; Lee, K.W. The influence of ceramic surface treatments on the tensile bond strength of composite resin to all-ceramic coping materials. J. Prosthet. Dent. 2005, 94, 357–362. [Google Scholar] [CrossRef]
- Bottino, M.C.; Özcan, M.; Coelho, P.G.; Valandro, L.F.; Bresciani, J.C.; Bresciani, A.H.A. Micro-morphological changes prior to adhesive bonding: High-alumina and glassy-matrix ceramics. Braz. Oral Res. 2008, 22, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yavuz, T. Özyılmaz, Ö.Y.; Dilber, E.; Tobi, E.S.; Kiliç, H.Ş. Effect of different surface treatments on porcelain-resin bond strength. J. Prosthodont. 2017, 26, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, T.; Dilber, E.; Kara, H.B.; Tuncdemir, A.R.; Ozturk, A.N. Effects of different surface treatments on shear bond strength in two different ceramic systems. Lasers Med. Sci. 2013, 28, 1233–1239. [Google Scholar] [CrossRef]
- Özcan, M.; Vallittu, P.K. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent. Mater. 2003, 19, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Özcan, M.; Allahbeickaraghi, A.; Dündar, M. Possible hazardous effects of hydrofluoric acid and recommendations for treatment approach: A review. Clin. Oral Investig. 2012, 16, 15–23. [Google Scholar] [CrossRef]
- Helbling, F.; Özcan, M. Adhesion of resin cement to contemporary hybrid ceramic and polymeric CAD/CAM materials: Effect of conditioning methods and aging. J. Adhes. Sci. Technol. 2019, 33, 886–902. [Google Scholar] [CrossRef] [Green Version]
- de Paula Eduardo, P.; Bello-Silva, M.S.; Moretto, S.G.; Cesar, P.F.; de Freitas, P.M. Microtensile bond strength of composite resin to glass-infiltrated alumina composite conditioned with Er,Cr:YSGG laser. Lasers Med. Sci. 2012, 27, 7–14. [Google Scholar] [CrossRef]
- Corazza, P.H.; Cavalcanti, S.C.M.; Queiroz, J.R.C.; Bottino, M.A.; Valandro, L.F. Effect of post silanization heat treatments of silanized feldspathic ceramic on adhesion to resin cement. J. Adhes. Dent. 2013, 15, 473–479. [Google Scholar]
- Fabianelli, A.; Pollington, S.; Papacchini, F.; Goracci, C.; Cantoro, A.; Ferrari, M.; van Noort, R. The effect of different surface treatments on bond strength between leucite reinforced feldspathic ceramic and composite resin. J. Dent. 2010, 38, 39–43. [Google Scholar] [CrossRef] [PubMed]
- de Figueiredo, V.M.G.; Corazza, P.H.; Lepesqueur, L.S.S.; Miranda, G.M.; Pagani, C.; de Melo, R.M.; Valandro, L.F. Heat treatment of silanized feldspathic ceramics: Effect on the bond strength to resin after thermocycling. Int. J. Adhes. Adhes. 2015, 63, 96–101. [Google Scholar] [CrossRef] [Green Version]
- de Carvalho, R.F.; Martins, M.E.M.N.; de Queiroz, J.R.C.; Leite, F.P.P.; Özcan, M. Influence of silane heat treatment on bond strength of resin cement to a feldspathic ceramic. Dent. Mater. 2011, 30, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Monticelli, F.; Toledano, M.; Osorio, R.; Ferrari, M. Effect of temperature on the silane coupling agents when bonding core resin to quartz fiber posts. Dent. Mater. 2006, 22, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.; Breschi, L.; Özcan, M.; Pfefferkorn, F.; Ferrari, M.; Van Meerbeek, B. Academy of Dental Materials guidance on in vitro testing of dental composite bonding effectiveness to dentin/enamel using micro-tensile bond strength (μTBS) approach. Dent. Mater. 2017, 33, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Sano, H.; Chowdhury, A.F.M.A.; Saikaew, P.; Matsumoto, M.; Hoshika, S.; Yamauti, M. The microtensile bond strength test: Its historical background and application to bond testing. Jpn. Dent. Sci. Rev. 2020, 56, 24–31. [Google Scholar] [CrossRef]
- Nagarkar, S.; Theis-Mahon, N.; Perdigão, J. Universal dental adhesives: Current status, laboratory testing, and clinical performance. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 107, 2121–2131. [Google Scholar] [CrossRef] [PubMed]
- Sasany, R.; Sarac, D.; Kunt, G.E. Effect of various veneering techniques on bond strength and colour stability of zirconia / veneering ceramic after hydrothermal aging. J. Evolution. Med. Dent. Sci. 2021, 10, 3474–3479. [Google Scholar] [CrossRef]
- Sasany, R.; Saraç, D.; Özcan, M. Effect of different liner techniques and argon plasma treatment of zirconia base on the adhesion and colour change of veneering ceramic. J. Adhes. Sci. Technol. 2021, 35, 1981–1994. [Google Scholar] [CrossRef]
- Della Bona, A.; Anusavice, K.J.; Mecholsky, J.J., Jr. Failure analysis of resin composite bonded to ceramic. Dent. Mater. 2003, 19, 693–699. [Google Scholar] [CrossRef]
- Ramakrishnaiah, R.; Alkheraif, A.A.; Divakar, D.D.; Matinlinna, J.P.; Vallittu, P.K. The Effect of Hydrofluoric Acid Etching Duration on the Surface Micromorphology, Roughness, and Wettability of Dental Ceramics. Int. J. Mol. Sci. 2016, 17, 822. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Material | Composition | Manufacturer |
|---|---|---|
| IPS e. max Press | Lithium disilicate glass-ceramic | Ivoclar Vivadent, Schaan, Liechtenstein |
| Tetric N-Ceram | dimethacrylates (19–20 wt %) | Ivoclar Vivadent, Schaan, Liechtenstein |
| Silane coupling agent | 3-glycidoxypropyltrimethoxysilane | Ivoclar Vivadent, Schaan, Liechtenstein |
| CoJet-System | Sand (CoJet®® Sand): Silicatized sand (particle size 30 μm); Silane (ESPE Sil®®): Silane with an attached methacrylic group; and Ethanol Bonding agent (Visio-Bond®®): Bisacrylate, Aminodiolmethacrylate, Camphor quinine, Benzyldimethylketale, and Stabilizers | 3M ESPE, Seefeld, Germany |
| Korox 50 | Al2O3 particles | Bego, Bremen, Germany |
| Porcelain Etch | Hydrofluoric acid | Ultraden Products Inc. South Jordan, UT, USA |
| Variolink-N | BISGMA, Barium, Glass filler, Di-methacrylates, Pigments, Initiators, Stabilizers, Silica | Ivoclar Vivadent, Schaan, Liechtenstein |
| Group | Mean ± SD | Min | Max |
|---|---|---|---|
| S | 20.12 a ± 1.71 | 12 | 29 |
| SC | 20.78 a ± 1.85 | 14 | 28 |
| ALS | 15.62 b ± 1.79 | 10 | 19 |
| SHT1 | 27.46 c ± 0.97 | 16 | 36 |
| SHT2 | 26.74 c ± 0.82 | 16 | 35 |
| HF | 25.77 c ± 1.21 | 20 | 32 |
| HFS | 26.06 d ± 1.41 | 31 | 43 |
| Group | CS | ALS | SHT1 | SHT2 | HF | HFS |
|---|---|---|---|---|---|---|
| S | p = 1 | p = 0.001 | p < 0.001 | p < 0.001 | p = 0.001 | p < 0.001 |
| SC | p < 0.001 | p < 0.001 | p < 0.001 | p = 0.008 | p < 0.001 | |
| ALS | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | ||
| SHT1 | p < 0.001 | p < 0.001 | p < 0.001 | |||
| SHT2 | p < 0.001 | p = 1 | ||||
| HF | p < 0.001 |
| Group | Adhesive * | Cohesive * | Mixed * |
|---|---|---|---|
| S | 8 (80) | - | 2 (20) |
| SC | 7 (70) | - | 3 (30) |
| ALS | 9 (90) | - | 1 (10) |
| SHT1 | 5 (50) | - | 5 (50) |
| SHT2 | 6 (60) | - | 4 (40) |
| HF | 8 (80) | - | 2 (20) |
| HFS | 4 (40) | - | 6 (60) |
| Total | 47 (67.1) | 23 (32.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ergun-Kunt, G.; Sasany, R.; Koca, M.F.; Özcan, M. Comparison of Silane Heat Treatment by Laser and Various Surface Treatments on Microtensile Bond Strength of Composite Resin/Lithium Disilicate. Materials 2021, 14, 7808. https://doi.org/10.3390/ma14247808
Ergun-Kunt G, Sasany R, Koca MF, Özcan M. Comparison of Silane Heat Treatment by Laser and Various Surface Treatments on Microtensile Bond Strength of Composite Resin/Lithium Disilicate. Materials. 2021; 14(24):7808. https://doi.org/10.3390/ma14247808
Chicago/Turabian StyleErgun-Kunt, Goknil, Rafat Sasany, Mehmet Faruk Koca, and Mutlu Özcan. 2021. "Comparison of Silane Heat Treatment by Laser and Various Surface Treatments on Microtensile Bond Strength of Composite Resin/Lithium Disilicate" Materials 14, no. 24: 7808. https://doi.org/10.3390/ma14247808
APA StyleErgun-Kunt, G., Sasany, R., Koca, M. F., & Özcan, M. (2021). Comparison of Silane Heat Treatment by Laser and Various Surface Treatments on Microtensile Bond Strength of Composite Resin/Lithium Disilicate. Materials, 14(24), 7808. https://doi.org/10.3390/ma14247808