
Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies


 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
Literature Review
2. Materials and Methods
2.1. Inclusion Criteria
- −
- Participants (P)—teeth that had undergone root canal preparation followed by endodontic obturation.
- −
- Intervention (I)—obturation done using heated gutta-percha techniques.
- −
- Comparison (C)—obturation of the root canal using the cold lateral condensation (CLC) technique.
- −
- Outcome (O)—assessment of root canal filling or voids on a micro-CT.
- −
- Studies (S)—studies that compared two or more techniques, one of which was cold lateral condensation and another which was a heated gutta-percha technique.
- −
- Those studies that objectively assessed and compared the obturation using micro-CT were included in this review.
2.2. Exclusion Criteria
2.3. Focus Question
2.4. Search Strategy
2.5. Risk of Bias
3. Results
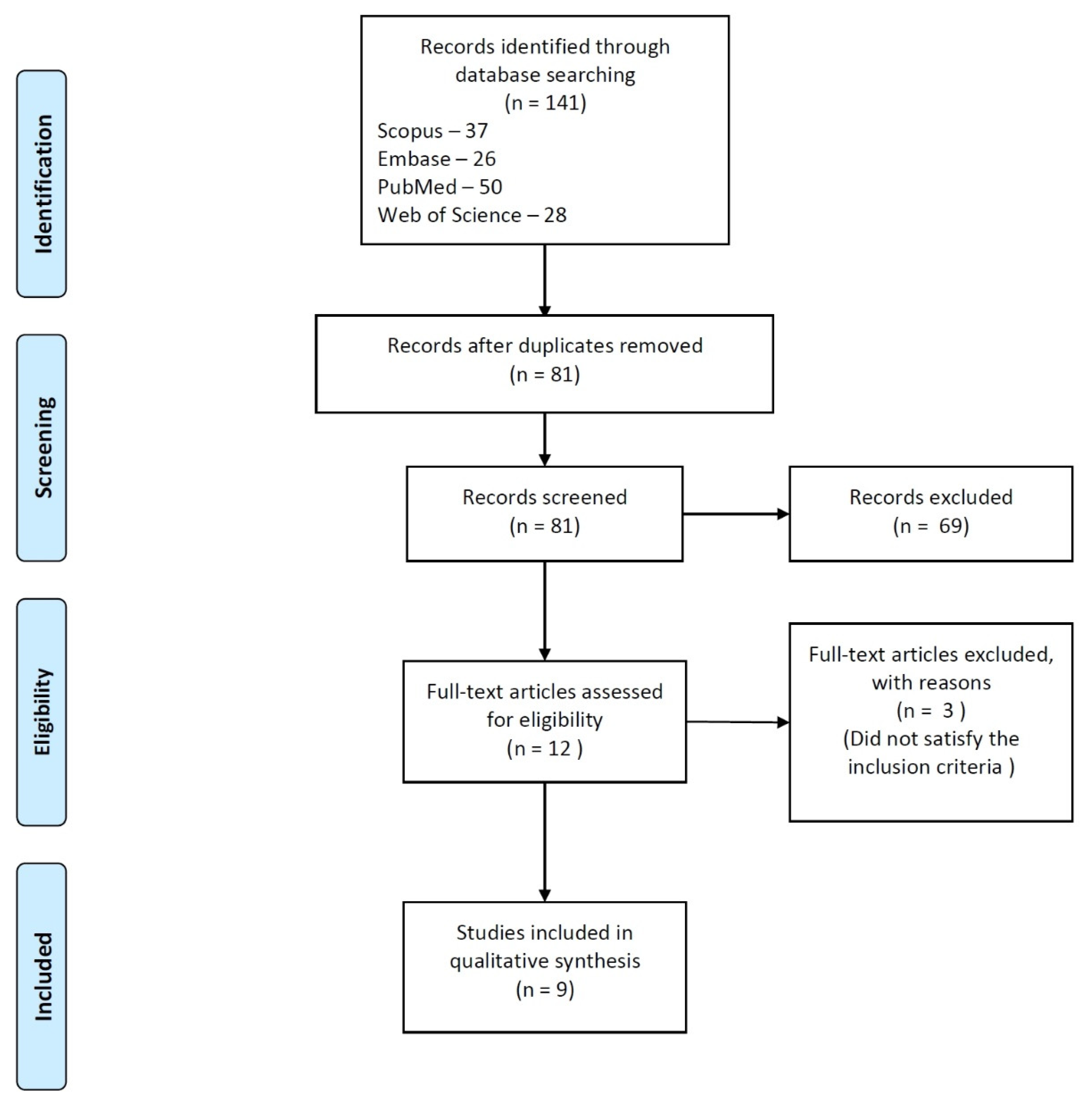
3.1. Identification of Studies
3.2. Assessment of Risk of Bias
3.3. Studies Examining the Completeness of Obturation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Epley, S.R.; Fleischman, J.; Hartwell, G.; Cicalese, C. Completeness of Root Canal Obturations: Epiphany Techniques versus Gutta-Percha Techniques. J. Endod. 2006, 32, 541–544. [Google Scholar] [CrossRef]
- Pedro, F.M.; Marques, A.; Pereira, T.M.; Bandeca, M.C.; Lima, S.; Kuga, M.C.; Tonetto, M.R.; Semenoff-Segundo, A.; Borges, A.H. Status of Endodontic Treatment and the Correlations to the Quality of Root Canal Filling and Coronal Restoration. J. Contemp. Dent. Pract. 2016, 17, 830–836. [Google Scholar] [CrossRef]
- Frisk, F. Epidemiological Aspects on Apical Periodontitis. Studies Based on the Prospective Population Study of Women in Göteborg and the Population Study on Oral Health in Jönköping, Sweden. Swed. Dent. J. 2007, 189, 11–78. [Google Scholar]
- Boucher, Y.; Matossian, L.; Rilliard, F.; Machtou, P. Radiographic Evaluation of the Prevalence and Technical Quality of Root Canal Treatment in a French Subpopulation. Int. Endod. J. 2002, 35, 229–238. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of Primary Root Canal Treatment: Systematic Review of the Literature—Part 2. Influence of Clinical Factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.M.; Rosenberg, P.A.; Lin, J. Do Procedural Errors Cause Endodontic Treatment Failure? J. Am. Dent. Assoc. 2005, 136, 187–193, quiz 231. [Google Scholar] [CrossRef] [PubMed]
- De Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment Outcome in Endodontics: The Toronto Study—Phases 3 and 4: Orthograde Retreatment. J. Endod. 2008, 34, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Kim, H.-C.; Lee, W.; Kim, E. Analysis of the Cause of Failure in Nonsurgical Endodontic Treatment by Microscopic Inspection during Endodontic Microsurgery. J. Endod. 2011, 37, 1516–1519. [Google Scholar] [CrossRef]
- Tennert, C.; Fuhrmann, M.; Wittmer, A.; Karygianni, L.; Altenburger, M.J.; Pelz, K.; Hellwig, E.; Al-Ahmad, A. New Bacterial Composition in Primary and Persistent/Secondary Endodontic Infections with Respect to Clinical and Radiographic Findings. J. Endod. 2014, 40, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, S.; Khan, F.R. Failure of Endodontic Treatment: The Usual Suspects. Eur. J. Dent. 2016, 10, 144–147. [Google Scholar] [CrossRef]
- Hancock, H.H.; Sigurdsson, A.; Trope, M.; Moiseiwitsch, J. Bacteria Isolated after Unsuccessful Endodontic Treatment in a North American Population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F. Microbial Causes of Endodontic Flare-Ups. Int. Endod. J. 2003, 36, 453–463. [Google Scholar] [CrossRef]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Arena, C.; Caponio, V.C.A.; Caloro, G.A.; Zhurakivska, K.; Adipietro, I.; Troiano, G.; Lo Muzio, L. Inspection of the Microbiota in Endodontic Lesions. Dent. J. 2019, 7, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assed, S.; Ito, I.Y.; Leonardo, M.R.; Silva, L.A.; Lopatin, D.E. Anaerobic Microorganisms in Root Canals of Human Teeth with Chronic Apical Periodontitis Detected by Indirect Immunofluorescence. Endod. Dent. Traumatol. 1996, 12, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.K.; R’oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and Extent of Long Oval Canals in the Apical Third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campello, A.F.; Marceliano-Alves, M.F.; Siqueira, J.F.; Fonseca, S.C.; Lopes, R.T.; Alves, F.R.F. Unprepared Surface Areas, Accumulated Hard Tissue Debris, and Dentinal Crack Formation after Preparation Using Reciprocating or Rotary Instruments: A Study in Human Cadavers. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Peters, O.A.; Paqué, F. Root Canal Preparation of Maxillary Molars with the Self-Adjusting File: A Micro-Computed Tomography Study. J. Endod. 2011, 37, 53–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, L.B.; Wesselink, P.R.; Moorer, W.R. The Fate and the Role of Bacteria Left in Root Dentinal Tubules. Int. Endod. J. 1995, 28, 95–99. [Google Scholar] [CrossRef]
- Bedier, M.M.; Hashem, A.A.R.; Hassan, Y.M. Improved Dentin Disinfection by Combining Different-Geometry Rotary Nickel-Titanium Files in Preparing Root Canals. Restor. Dent. Endod. 2018, 43, e46. [Google Scholar] [CrossRef]
- Pérez, A.R.; Ricucci, D.; Vieira, G.C.S.; Provenzano, J.C.; Alves, F.R.F.; Marceliano-Alves, M.F.; Rôças, I.N.; Siqueira, J.F. Cleaning, Shaping, and Disinfecting Abilities of 2 Instrument Systems as Evaluated by a Correlative Micro-Computed Tomographic and Histobacteriologic Approach. J. Endod. 2020, 46, 846–857. [Google Scholar] [CrossRef]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Laneve, E.; Cocco, A.; Troiano, G. Endodontic Irrigants: Different Methods to Improve Efficacy and Related Problems. Eur. J. Dent. 2018, 12, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Dubey, A.K.; Prasanna, S.R.M.; Dandapat, S. Sinusoidal Model-Based Hypernasality Detection in Cleft Palate Speech Using CVCV Sequence. Speech Commun. 2020, 124, 1–12. [Google Scholar] [CrossRef]
- Siqueira Junior, J.F.; Rôças, I.d.N.; Marceliano-Alves, M.F.; Pérez, A.R.; Ricucci, D. Unprepared Root Canal Surface Areas: Causes, Clinical Implications, and Therapeutic Strategies. Braz. Oral Res. 2018, 32, e65. [Google Scholar] [CrossRef] [Green Version]
- Van der Sluis, L.W.M.; Wu, M.-K.; Wesselink, P.R. An Evaluation of the Quality of Root Fillings in Mandibular Incisors and Maxillary and Mandibular Canines Using Different Methodologies. J. Dent. 2005, 33, 683–688. [Google Scholar] [CrossRef]
- Ducret, M.; Fabre, H.; Celle, A.; Mallein-Gerin, F.; Perrier-Groult, E.; Alliot-Licht, B.; Farges, J.-C. Current Challenges in Human Tooth Revitalization. Bio Med. Mater. Eng. 2017, 28, S159–S168. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kim, E. Antimicrobial Effect of Calcium Hydroxide as an Intracanal Medicament in Root Canal Treatment: A Literature Review—Part II. in Vivo Studies. Restor. Dent. Endod. 2015, 40, 97–103. [Google Scholar] [CrossRef]
- Kvist, T.; Molander, A.; Dahlen, G.; Reit, C. Microbiological Evaluation of One- and Two-Visit Endodontic Treatment of Teeth with Apical Periodontitis: A Randomized, Clinical Trial. J. Endod. 2004, 30, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Gutmann, J.L. Adaptation of Injected Thermoplasticized Gutta-Percha in the Absence of the Dentinal Smear Layer. Int. Endod. J. 1993, 26, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F.; Favieri, A.; Gahyva, S.M.M.; Moraes, S.R.; Lima, K.C.; Lopes, H.P. Antimicrobial Activity and Flow Rate of Newer and Established Root Canal Sealers. J. Endod. 2000, 26, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Orstavik, D. Materials Used for Root Canal Obturation: Technical, Biological and Clinical Testing. Endod. Top. 2005, 12, 25–38. [Google Scholar] [CrossRef]
- Evans, J.T.; Simon, J.H. Evaluation of the Apical Seal Produced by Injected Thermoplasticized Gutta-Percha in the Absence of Smear Layer and Root Canal Sealer. J. Endod. 1986, 12, 100–107. [Google Scholar] [CrossRef]
- Balguerie, E.; van der Sluis, L.; Vallaeys, K.; Gurgel-Georgelin, M.; Diemer, F. Sealer Penetration and Adaptation in the Dentinal Tubules: A Scanning Electron Microscopic Study. J. Endod. 2011, 37, 1576–1579. [Google Scholar] [CrossRef]
- Saleh, I.M.; Ruyter, I.E.; Haapasalo, M.; Ørstavik, D. Survival of Enterococcus Faecalis in Infected Dentinal Tubules after Root Canal Filling with Different Root Canal Sealers in Vitro. Int. Endod. J. 2004, 37, 193–198. [Google Scholar] [CrossRef]
- De-Deus, G.; Brandão, M.C.; Leal, F.; Reis, C.; Souza, E.M.; Luna, A.S.; Paciornik, S.; Fidel, S. Lack of Correlation between Sealer Penetration into Dentinal Tubules and Sealability in Nonbonded Root Fillings. Int. Endod. J. 2012, 45, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Schilder, H. Cleaning and Shaping the Root Canal. Dent. Clin. N. Am. 1974, 18, 269–296. [Google Scholar]
- Metzger, Z.; Zary, R.; Cohen, R.; Teperovich, E.; Paqué, F. The Quality of Root Canal Preparation and Root Canal Obturation in Canals Treated with Rotary versus Self-Adjusting Files: A Three-Dimensional Micro-Computed Tomographic Study. J. Endod. 2010, 36, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- De-Deus, G.; Gurgel-Filho, E.D.; Magalhães, K.M.; Coutinho-Filho, T. A Laboratory Analysis of Gutta-Percha-Filled Area Obtained Using Thermafil, System B and Lateral Condensation. Int. Endod. J. 2006, 39, 378–383. [Google Scholar] [CrossRef]
- Cailleteau, J.G.; Mullaney, T.P. Prevalence of Teaching Apical Patency and Various Instrumentation and Obturation Techniques in United States Dental Schools. J. Endod. 1997, 23, 394–396. [Google Scholar] [CrossRef]
- Levitan, M.E.; Himel, V.T.; Luckey, J.B. The Effect of Insertion Rates on Fill Length and Adaptation of a Thermoplasticized Gutta-Percha Technique. J. Endod. 2003, 29, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Cueva-Goig, R.; Forner-Navarro, L.; Llena-Puy, M.C. Microscopic Assessment of the Sealing Ability of Three Endodontic Filling Techniques. J. Clin. Exp. Dent. 2016, 8, e27–e31. [Google Scholar] [CrossRef] [Green Version]
- Leduc, J.; Fishelberg, G. Endodontic Obturation: A Review. Gen. Dent. 2003, 51, 232–233. [Google Scholar]
- Budd, C.S.; Weller, R.N.; Kulild, J.C. A Comparison of Thermoplasticized Injectable Gutta-Percha Obturation Techniques. J. Endod. 1991, 17, 260–264. [Google Scholar] [CrossRef]
- Schilder, H. Filling Root Canals in Three Dimensions. 1967. J. Endod. 2006, 32, 281–290. [Google Scholar] [CrossRef]
- Buchanan, L.S. Continuous Wave of Condensation Technique. Endod. Pract. 1998, 1, 7–10, 13–16, 18 passim. [Google Scholar]
- Canal Preparation and Obturation Clinical Newsletter. Available online: https://www.aae.org/specialty/communique/newsletter/canal-preparation-obturation-updated-view-two-pillars-nonsurgical-endodontics (accessed on 9 April 2021).
- Clinton, K.; Van Himel, T. Comparison of a Warm Gutta-Percha Obturation Technique and Lateral Condensation. J. Endod. 2001, 27, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.; Walker, M.P.; Kulild, J.; Lee, C. A Comparison of Three Gutta-Percha Obturation Techniques to Replicate Canal Irregularities. J. Endod. 2006, 32, 762–765. [Google Scholar] [CrossRef]
- Lea, C.S.; Apicella, M.J.; Mines, P.; Yancich, P.P.; Parker, M.H. Comparison of the Obturation Density of Cold Lateral Compaction Versus Warm Vertical Compaction Using the Continuous Wave of Condensation Technique. J. Endod. 2005, 31, 37–39. [Google Scholar] [CrossRef]
- Williamson, A.E.; Dawson, D.V.; Drake, D.R.; Walton, R.E.; Rivera, E.M. Effect of Root Canal Filling/Sealer Systems on Apical Endotoxin Penetration: A Coronal Leakage Evaluation. J. Endod. 2005, 31, 599–604. [Google Scholar] [CrossRef]
- Cattoni, F.; Teté, G.; Calloni, A.M.; Manazza, F.; Gastaldi, G.; Capparè, P. Milled versus Moulded Mock-Ups Based on the Superimposition of 3D Meshes from Digital Oral Impressions: A Comparative in Vitro Study in the Aesthetic Area. BMC Oral Health 2019, 19, 230. [Google Scholar] [CrossRef]
- Tetè, G.; D’Orto, B.; Nagni, M.; Agostinacchio, M.; Polizzi, E.; Agliardi, E. Role of Induced Pluripotent Stem Cells (IPSCS) in Bone Tissue Regeneration in Dentistry: A Narrative Review. J. Biol. Regul. Homeost. Agents 2020, 34, 1–10. [Google Scholar]
- Lucchese, A.; Gherlone, E.; Portelli, M.; Bertossi, D. Tooth Orthodontic Movement after Maxillofacial Surgery. Eur. J. Inflamm. 2012, 10, 227–232. [Google Scholar] [CrossRef] [Green Version]
- European Society of Endodontology; Patel, S.; Durack, C.; Abella, F.; Roig, M.; Shemesh, H.; Lambrechts, P.; Lemberg, K. European Society of Endodontology Position Statement: The Use of CBCT in Endodontics. Int. Endod. J. 2014, 47, 502–504. [Google Scholar] [CrossRef]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology Position Statement: Use of Cone Beam Computed Tomography in Endodontics: European Society of Endodontology (ESE) Developed By. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helvacioglu-Yigit, D.; Kocasarac, H.D.; Bechara, B.; Noujeim, M. Evaluation and Reduction of Artifacts Generated by 4 Different Root-End Filling Materials by Using Multiple Cone-Beam Computed Tomography Imaging Settings. J. Endod. 2016, 42, 307–314. [Google Scholar] [CrossRef]
- Naranjo, V.; Lloréns, R.; Alcañiz, M.; López-Mir, F. Metal Artifact Reduction in Dental CT Images Using Polar Mathematical Morphology. Comput. Methods Programs Biomed. 2011, 102, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Mazzi-Chaves, J.F.; de Faria Vasconcelos, K.; Pauwels, R.; Jacobs, R.; Sousa-Neto, M.D. Cone-Beam Computed Tomographic–Based Assessment of Filled C-Shaped Canals: Artifact Expression of Cone-Beam Computed Tomography as Opposed to Micro–Computed Tomography and Nano–Computed Tomography. J. Endod. 2020, 46, 1702–1711. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.T.; Jacobs, R.; Vasconcelos, K.F.; Lambrechts, P.; Rubira-Bullen, I.R.F.; Gaêta-Araujo, H.; Oliveira-Santos, C.; Duarte, M.A.H. Influence of CBCT-Based Volumetric Distortion and Beam Hardening Artefacts on the Assessment of Root Canal Filling Quality in Isthmus-Containing Molars. Dento Maxillo Facial Radiol. 2021, 20200503. [Google Scholar] [CrossRef] [PubMed]
- Reda, R.; Zanza, A.; Mazzoni, A.; Cicconetti, A.; Testarelli, L.; Di Nardo, D. An Update of the Possible Applications of Magnetic Resonance Imaging (MRI) in Dentistry: A Literature Review. J. Imaging 2021, 7, 75. [Google Scholar] [CrossRef]
- Kim, I.; Paik, K.-S.; Lee, S.-P. Quantitative Evaluation of the Accuracy of Micro-Computed Tomography in Tooth Measurement. Clin. Anat. 2007, 20, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.C.; Tam, A.; Schilder, H. Root Canal Anatomy Illustrated by Microcomputed Tomography and Clinical Cases. Gen. Dent. 2006, 54, 331–335. [Google Scholar]
- Gutmann, J.; Rigsby, S.; Endo, C.; Abe, D. Meeting Age Old Challenges in Root Canal Procedures with Contemporary Technological Assessments. ENDO 2015, 9, 107–110. [Google Scholar]
- Peters, O.A.; Boessler, C.; Paqué, F. Root Canal Preparation with a Novel Nickel-Titanium Instrument Evaluated with Micro-Computed Tomography: Canal Surface Preparation over Time. J. Endod. 2010, 36, 1068–1072. [Google Scholar] [CrossRef]
- Jung, M.; Lommel, D.; Klimek, J. The Imaging of Root Canal Obturation Using Micro-CT. Int. Endod. J. 2005, 38, 617–626. [Google Scholar] [CrossRef]
- Celikten, B.; Jacobs, R.; deFaria Vasconcelos, K.; Huang, Y.; Nicolielo, L.F.P.; Orhan, K. Assessment of Volumetric Distortion Artifact in Filled Root Canals Using Different Cone-Beam Computed Tomographic Devices. J. Endod. 2017, 43, 1517–1521. [Google Scholar] [CrossRef]
- Celikten, B.; Jacobs, R.; de Faria Vasconcelos, K.; Huang, Y.; Shaheen, E.; Nicolielo, L.F.P.; Orhan, K. Comparative Evaluation of Cone Beam CT and Micro-CT on Blooming Artifacts in Human Teeth Filled with Bioceramic Sealers. Clin. Oral Investig. 2019, 23, 3267–3273. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Fardi, A.; Kodonas, K.; Gogos, C.; Economides, N. Top-Cited Articles in Endodontic Journals. J. Endod. 2011, 37, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Estrela, C.; Holland, R.; Estrela, C.R.d.A.; Alencar, A.H.G.; Sousa-Neto, M.D.; Pécora, J.D. Characterization of Successful Root Canal Treatment. Braz. Dent. J. 2014, 25, 3–11. [Google Scholar] [CrossRef]
- Sarkis-Onofre, R.; Skupien, J.; Cenci, M.; Moraes, R.; Pereira-Cenci, T. The Role of Resin Cement on Bond Strength of Glass-Fiber Posts Luted Into Root Canals: A Systematic Review and Meta-Analysis of In Vitro Studies. Oper. Dent. 2014, 39, E31–E44. [Google Scholar] [CrossRef]
- Abdo, S.B.; Darrat, A.A.; Masudi, S.M.; Luddin, N.; Husien, A. Sealing Ability of Gutta-Percha/Nano HA versus Resilon/Epiphany after 20 Months Using an Electrochemical Model: An in Vitro Study. Braz. J. Oral Sci. 2012, 11, 387–391. [Google Scholar]
- Küçükkaya Eren, S.; Askerbeyli Örs, S.; Yılmaz, Z. Effect of Post Space Preparation on Apical Obturation Quality of Teeth Obturated with Different Techniques: A Micro-Computed Tomographic Study. J. Endod. 2017, 43, 1152–1156. [Google Scholar] [CrossRef] [PubMed]
- Athkuri, S.; Mandava, J.; Chalasani, U.; Ravi, R.C.; Munagapati, V.K.; Chennareddy, A.R. Effect of Different Obturating Techniques and Sealers on the Removal of Filling Materials during Endodontic Retreatment. J. Conserv. Dent. 2019, 22, 578–582. [Google Scholar] [CrossRef]
- Şımşek, N.; Keleş, A.; Ahmetoğlu, F.; Akinci, L.; Er, K. 3D Micro-CT Analysis of Void and Gap Formation in Curved Root Canals. Eur. Endod. J. 2017, 2, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, S.; Perinpanayagam, H.; Kum, D.J.W.; Lim, S.-M.; Yoo, Y.-J.; Chang, S.W.; Lee, W.; Baek, S.-H.; Zhu, Q.; Kum, K.Y. Evaluation of Three Obturation Techniques in the Apical Third of Mandibular First Molar Mesial Root Canals Using Micro-Computed Tomography. J. Dent. Sci. 2016, 11, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Ho, E.S.S.; Chang, J.W.W.; Cheung, G.S.P. Quality of Root Canal Fillings Using Three Gutta-Percha Obturation Techniques. Restor. Dent. Endod. 2016, 41, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Celikten, B.; F Uzuntas, C.; I Orhan, A.; Tufenkci, P.; Misirli, M.; O Demiralp, K.; Orhan, K. Micro-CT Assessment of the Sealing Ability of Three Root Canal Filling Techniques. J. Oral Sci. 2015, 57, 361–366. [Google Scholar] [CrossRef] [Green Version]
- Kierklo, A.; Tabor, Z.; Pawińska, M.; Jaworska, M. A Microcomputed Tomography-Based Comparison of Root Canal Filling Quality Following Different Instrumentation and Obturation Techniques. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2015, 24, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Nhata, J.; Machado, R.; Vansan, L.P.; Batista, A.; Sidney, G.; Rosa, T.P.; Leal Silva, E.J.N. Micro-Computed Tomography and Bond Strength Analysis of Different Root Canal Filling Techniques. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2014, 25, 698–701. [Google Scholar] [CrossRef]
- Keleş, A.; Alcin, H.; Kamalak, A.; Versiani, M.A. Micro-CT Evaluation of Root Filling Quality in Oval-Shaped Canals. Int. Endod. J. 2014, 47, 1177–1184. [Google Scholar] [CrossRef]
- Naseri, M.; Kangarlou, A.; Khavid, A.; Goodini, M. Evaluation of the Quality of Four Root Canal Obturation Techniques Using Micro-Computed Tomography. Iran. Endod. J. 2013, 8, 89–93. [Google Scholar] [PubMed]
- Moeller, L.; Wenzel, A.; Wegge-Larsen, A.M.; Ding, M.; Kirkevang, L.L. Quality of Root Fillings Performed with Two Root Filling Techniques. An in Vitro Study Using Micro-CT. Acta Odontol. Scand. 2013, 71, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Versiani, M.A.; Keleș, A. Applications of Micro-CT Technology in Endodontics. In Micro-Computed Tomography (micro-CT) in Medicine and Engineering; Orhan, K., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 183–211. ISBN 978-3-030-16640-3. [Google Scholar]
- Rack, A.; Stiller, M.; Dalügge, O.; Rack, T.; Riesemeier, H.; Knabe, C. 3.304—Developments in High-Resolution CT: Studying Bioregeneration by Hard X-ray Synchrotron-Based Microtomography. In Comprehensive Biomaterials; Ducheyne, P., Ed.; Elsevier: Oxford, UK, 2011; pp. 47–62. ISBN 978-0-08-055294-1. [Google Scholar]
- Zaslansky, P.; Fratzl, P.; Rack, A.; Wu, M.-K.; Wesselink, P.R.; Shemesh, H. Identification of Root Filling Interfaces by Microscopy and Tomography Methods: Microtomography and Microscopy Observations of Root Fillings. Int. Endod. J. 2011, 44, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Shahravan, A.; Haghdoost, A.-A.; Adl, A.; Rahimi, H.; Shadifar, F. Effect of Smear Layer on Sealing Ability of Canal Obturation: A Systematic Review and Meta-Analysis. J. Endod. 2007, 33, 96–105. [Google Scholar] [CrossRef]
- Dummer, P.M.; Lyle, L.; Rawle, J.; Kennedy, J.K. A Laboratory Study of Root Fillings in Teeth Obturated by Lateral Condensation of Gutta-Percha or Thermafil Obturators. Int. Endod. J. 1994, 27, 32–38. [Google Scholar] [CrossRef]
- Schäfer, E.; Olthoff, G. Effect of Three Different Sealers on the Sealing Ability of Both Thermafil Obturators and Cold Laterally Compacted Gutta-Percha. J. Endod. 2002, 28, 638–642. [Google Scholar] [CrossRef]
- Jaju, K.K.; Sandhya, R. Mahalakshmi Jayaraman Frequency, Distribution and Obturation Technique of Root Canal Retreatment among Patients Attending a Teaching Dental Hospital in Chennai—A Retrospective Study. Int. J. Res. Pharm. Sci. 2020, 11, 230–236. [Google Scholar] [CrossRef]
- AlRahabi, M. Attitudes of General Practice Dentists in Private Dental Clinics in Almadinah Almunawarah toward Novel Endodontic Technologies. G. Ital. Endod. 2016, 30, 10–13. [Google Scholar] [CrossRef] [Green Version]
- Savani, G.M.; Sabbah, W.; Sedgley, C.M.; Whitten, B. Current Trends in Endodontic Treatment by General Dental Practitioners: Report of a United States National Survey. J. Endod. 2014, 40, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.-Y.; Zhang, S.; Li, S.K.-Y.; Zhang, C.; Chu, C.-H. Clinical Studies on Core-Carrier Obturation: A Systematic Review and Meta-Analysis. BMC Oral Health 2017, 17, 167. [Google Scholar] [CrossRef] [Green Version]
- Gulabivala, K.; Abdo, S.; Sherriff, M.; Regan, J.D. The Influence of Interfacial Forces and Duration of Filing on Root Canal Shaping. Endod. Dent. Traumatol. 2000, 16, 166–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abarca, A.M.; Bustos, A.; Navia, M. A Comparison of Apical Sealing and Extrusion between Thermafil and Lateral Condensation Techniques. J. Endod. 2001, 27, 670–672. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Ye, L.; Tan, H.; Zhou, X. Outcome of Root Canal Obturation by Warm Gutta-Percha versus Cold Lateral Condensation: A Meta-Analysis. J. Endod. 2007, 33, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Augusto, C.M.; Barbosa, A.F.A.; Guimarães, C.C.; Lima, C.O.; Ferreira, C.M.; Sassone, L.M.; Silva, E.J.N.L. A Laboratory Study of the Impact of Ultraconservative Access Cavities and Minimal Root Canal Tapers on the Ability to Shape Canals in Extracted Mandibular Molars and Their Fracture Resistance. Int. Endod. J. 2020, 53, 1516–1529. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Query |
|---|---|
| PubMed | (quality) AND (((root canal) AND ((obturation) OR (filling))) AND (technique)) AND (micro-CT) Details: (“qualities”[All Fields] OR “quality”[All Fields] OR “quality s”[All Fields]) AND ((“dental pulp cavity”[MeSH Terms] OR (“dental”[All Fields] AND “pulp”[All Fields] AND “cavity”[All Fields]) OR “dental pulp cavity”[All Fields] OR (“root”[All Fields] AND “canal”[All Fields]) OR “root canal”[All Fields]) AND (“obturate”[All Fields] OR “obturated”[All Fields] OR “obturating”[All Fields] OR “obturation”[All Fields] OR “obturations”[All Fields] OR “obturator”[All Fields] OR “obturators”[All Fields] OR “obturing”[All Fields] OR (“filled”[All Fields] OR “filling”[All Fields] OR “fillings”[All Fields] OR “fills”[All Fields])) AND (“methods”[MeSH Subheading] OR “methods”[All Fields] OR “techniques”[All Fields] OR “methods”[MeSH Terms] OR “technique”[All Fields] OR “technique s”[All Fields])) AND (“X-ray microtomography”[MeSH Terms] OR (“X-ray”[All Fields] AND “microtomography”[All Fields]) OR “X-ray microtomography”[All Fields] OR (“micro”[All Fields] AND “ct”[All Fields]) OR “micro-CT”[All Fields]) |
| Scopus | TITLE-ABS -KEY ((quality) AND (((root AND canal) AND ((obturation) OR (filling))) AND (technique)) AND (micro AND ct)) |
| Embase | quality AND root AND canal AND (obturation OR filling) AND technique AND micro AND ct |
| Web of Science | ALL FIELDS: ((quality) AND (((root canal) AND ((obturation) OR (filling))) AND (technique)) AND (micro-CT)) |
| S. No | Author, Year, (Country) | Samples Used (Size per Group) | Thermoplastic Technique Used | Sealer | Final Irrigants | Measurement Method | Values Obtained | Results | |
|---|---|---|---|---|---|---|---|---|---|
| Cold Lateral Condensation (CLC) | Thermoplastic Technique | ||||||||
| 1 | Simsek et al., 2017 (Turkey) | Mesial root canals of mandibular first molars (10) | Thermoplasticized injectable gutta-percha (TIGP) | AH plus | 17% EDTA, 2.5% NaOCl | Volume of voids and filling (in mm3) calculated for both techniques using micro-CT for canals instrumented using self-adjusting files (SAF) and rotary files. | 3.11 ± 2.06 mm3 (SAF) 2.78 ± 1.20 mm3 (Rotary) | 3.81 ± 1.87 mm3 (SAF) 3.43 ± 0.90 mm3 (Rotary) | No significant differences were observed between techniques of preparation and obturation. In the filling techniques, independent of the instrumentation, more voids were in the thermoplastic GP technique, but the differences were not statistically significant. |
| 2 | Oh et al., 2016 (Korea) | Permanent mandibular first molars (20) | Continuous wave of condensation (CWC) | AH plus | 17 % EDTA, 3.5% NaOCl | The interface void volume ratio of the main canal was also calculated as a percentage of the main canal volume for the apical 5 mm. | 0.77 ± 0.16% | 0.27 ± 0.12% * | Filling density and adaptation was inferior in CLC filled canals with significantly higher interface void volume ratios. The gutta-percha volume ratio was also significantly lower in CLC than in CWC, but the sealer volume ratio was significantly higher in CLC than in CWC. |
| 3 | Ho et al., 2016 (China) | Permanent mandibular first molars (11) | Warm Vertical Compaction (WVC) with Thermoplasticized injectable gutta-percha (TIGP) | None | 3% NaOCl, 17% EDTA | The overall mean fraction of the root canal volume filled with gutta-percha for each group was determined | 68.51 ± 6.75% filled | 88.91 ± 5.16% filled * | The overall gutta-percha volume was significantly lower in the CL group than in the other groups. Within the CL group, the volume fraction was the same in all segments while in WVC, it increased towards the coronal aspect |
| 4 | Celikten et al., 2015 (Turkey) | First mandibular premolars (10) | Core carrier technique (Thermafil) | Endo-Sequence BC | 2.5% NaOCl, 17% EDTA, distilled water | Using 2D slices, the root filling volume percentages, the volume of internal, external and combined voids in materials was calculated. | 0.5 ± 0.2 (internal) 0.8 0.5 (external) 0.6 ± 0.3 (combined) | 0.4 ± 0.2 (internal) 0.7 ± 0.4 (external) 0.6 ± 0.3 (combined) | Thermafil had the smallest void volumes (both types) but significantly differed at the apical level only when compared to CLC. The overall volumes were not significantly different for both techniques. |
| 5 | Kiekerlo, 2015, Poland | Mandibular premolars (10) | Continuous Wave of Condensation | ZOE-based sealer (Tubli-seal) | 17% EDTA, 2% NaOCl and saline solution | The number, size, percentage of volume and distribution of voids-internal (I) and external (E) was measured for groups instrumented with hand (H) and rotary (R) instruments | 0.21 ± 0.18% (HI) 0.69 ± 0.41% (HE) 0.27 ± 0.28% (RI) 0.52 ± 0.38% (RE) | 0.11 ± 0.12% (HI) ** 0.14 ± 0.13% (HE) 0.20 ± 0.30% (RI) * 0.55 ± 0.48% (RE) | CLC produced voids mainly between the canal wall and the filling. With thermal compaction, the internal voids were more common, except for the apical third of the canal where mostly parietal voids were present. |
| 6 | Nhata et al., 2014 (Brazil) | Mandibular incisors (10) | Continuous wave of condensation | AH plus | 17% EDTA, Distilled water | The presence of voids at the interface between the root canal dentin and the filling material in all filling techniques investigated | 0.019 ± 0.005% | 0.004 ± 0.003% * | Less empty spaces were observed when GP was heated within the root canal on continuous wave of condensation compared to CLC. |
| 7 | Keleş et al., 2014 (Turkey) | Single rooted maxillary premolars (12) | Thermoplasticized injectable gutta-percha (TIGP) | AH plus | Saline solution | The volume of gutta-percha, sealer and voids was expressed as the percentage of the root canal volume | 4.26 ± 0.74% | 0.57 ± 0.44% * | The WVC group had a significantly lower percentage volume range of voids (p < 0.05) overall but the difference was insignificant for the techniques in the apical thirds |
| 8 | Naseri et al., 2013 (Iran) | Maxillary first molars (5) | Warm vertical condensation, Thermoplasticized injectable gutta-percha (TIGP) | AH26 sealer | 17% EDTA, 2.5% NaOCl | Expressed as the percentage of the root canal volume | 80.4 ± 1.6% | 84.8 ± 6.0%—WVC 92.7 ± 2.4% *—TIGP | The TIGP group had the least volume of voids, which was significantly less than both CLC and WVC. Both thermal techniques showed better fill volumes than CLC, which also had a higher percentage of sealer than any other technique. |
| 9 | Moeller et al., 2013 (Denmark) | Mandibular molars, premolars, and canines (34—CL and 33 in TH) | Hybrid Thermafil Technique (HT) | AH plus | 17% EDTA, 0.5% NaOCl | 2D slices were compared for the presence of voids in root fillings by assessing each section (672 µm apart) using a binary value—void present/void not present | 65.9% of the sections had voids | 66.9% of the sections had voids | A high frequency of voids was found for both techniques, increasing coronally. CLC resulted in fewer voids in the apical part of the root filling. The opposite was true for HT which had more voids cervically. Overall, the two techniques did not differ significantly in the percentage of voids. |
| S No. | Author, Year (Country) | Were Human Teeth Used as Specimens? | Was the Morphology Same for All Root Canals and without Any Root Perforation or Fracture? | Were the Groups Matched? | Was the Rationale for the Sample Size Mentioned? | Was a Standardized Root Canal Preparation and Disinfection Protocol Followed for Both Groups? | Did a Single Operator Perform All Procedures? | Was the Operator Skilled in Both Techniques? | Was the Observer/Evaluator Blind to the Groups? | Was the Entire Root Canal Volume Considered? | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Simsek et al., 2017 (Turkey) | Yes | Yes | Yes | Not mentioned | Yes | Yes | Not mentioned | Not mentioned | Yes | Moderate |
| 2 | Oh et al., 2016 (Korea) | Yes | Yes | Yes | Not mentioned | Yes | Yes | Not mentioned | Not mentioned | No | High |
| 3 | Ho et al., 2016 (China) | Yes | Yes | Yes | Not mentioned | Yes | Not mentioned | Not mentioned | Not mentioned | Yes | Moderate |
| 4 | Celikten et al., 2015 (Turkey) | Yes | Yes | Not mentioned | Not mentioned | Yes | Yes | Not mentioned | Yes | Yes | Moderate |
| 5 | Kiekerlo, 2015, Poland | Yes | Yes | Not mentioned | Not mentioned | Yes | Yes | Not mentioned | Not mentioned | Yes | Moderate |
| 6 | Nhata et al., 2014 (Brazil) | Yes | Not mentioned | Not mentioned | Not mentioned | Yes | Yes | Not mentioned | Not mentioned | Yes | High |
| 7 | Keleş et al., 2014 (Turkey) | Yes | Yes | Yes | Yes | Yes | Yes | Not mentioned | Not mentioned | Yes | Low |
| 8 | Naseri et al., 2013 (Iran) | Yes | Yes | Yes | Not mentioned | Yes | Yes | Not mentioned | Not mentioned | Yes | Moderate |
| 9 | Moeller et al., 2013 (Denmark) | Yes | Yes | Yes | Not mentioned | Yes | 2 operators alternated between techniques | Yes | Yes | No | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhandi, S.; Mashyakhy, M.; Abumelha, A.S.; Alkahtany, M.F.; Jamal, M.; Chohan, H.; Raj, A.T.; Testarelli, L.; Reda, R.; Patil, S. Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies. Materials 2021, 14, 4013. https://doi.org/10.3390/ma14144013
Bhandi S, Mashyakhy M, Abumelha AS, Alkahtany MF, Jamal M, Chohan H, Raj AT, Testarelli L, Reda R, Patil S. Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies. Materials. 2021; 14(14):4013. https://doi.org/10.3390/ma14144013
Chicago/Turabian StyleBhandi, Shilpa, Mohammed Mashyakhy, Abdulaziz S. Abumelha, Mazen F. Alkahtany, Mohamed Jamal, Hitesh Chohan, A. Thirumal Raj, Luca Testarelli, Rodolfo Reda, and Shankargouda Patil. 2021. "Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies" Materials 14, no. 14: 4013. https://doi.org/10.3390/ma14144013
APA StyleBhandi, S., Mashyakhy, M., Abumelha, A. S., Alkahtany, M. F., Jamal, M., Chohan, H., Raj, A. T., Testarelli, L., Reda, R., & Patil, S. (2021). Complete Obturation—Cold Lateral Condensation vs. Thermoplastic Techniques: A Systematic Review of Micro-CT Studies. Materials, 14(14), 4013. https://doi.org/10.3390/ma14144013