Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface


 ,
,  and
and 
Abstract
1. Introduction
2. Material and Methods
2.1. Sample Description
2.1.1. Recruitment
2.1.2. Demographic Description
2.1.3. Inclusion and Exclusion Criteria
2.2. Diagnosis Records
2.3. Surgery Protocol
2.4. Follow-Up
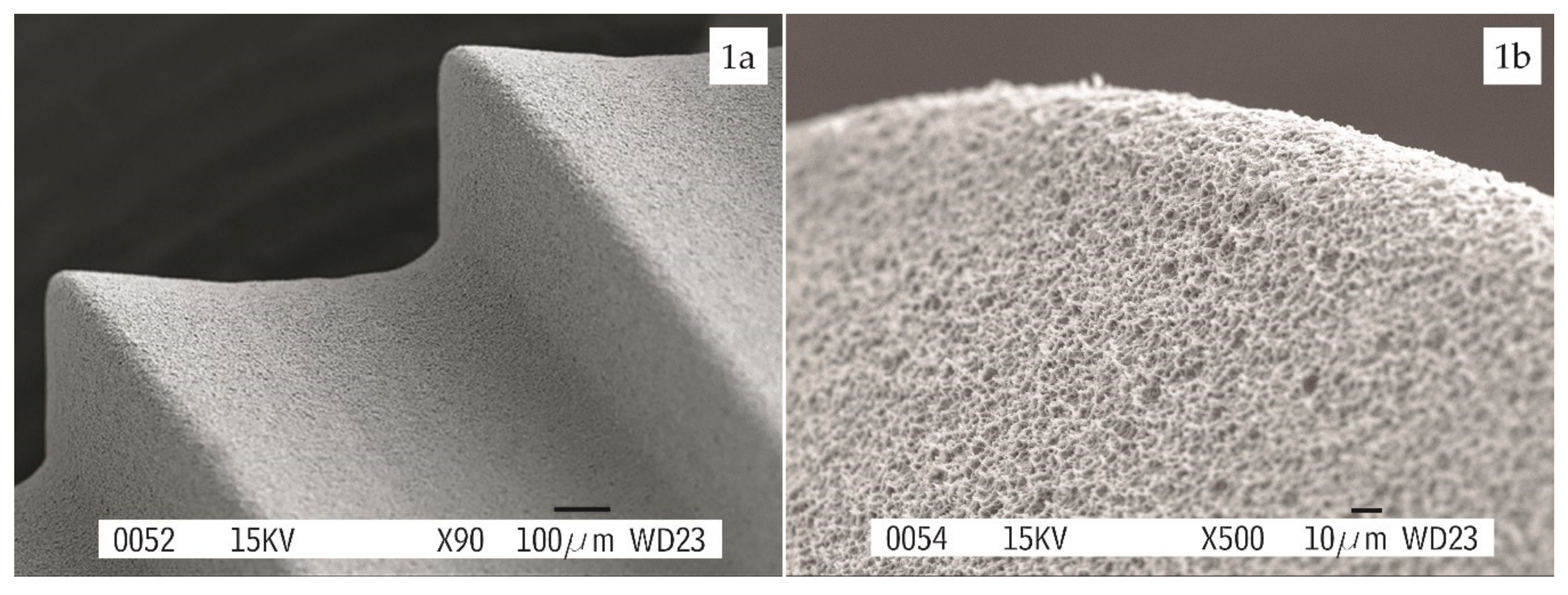
2.5. Implant Features
2.6. Success Criteria
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int J. Oral Maxillofac Implants. 1986, 1, 11–25. [Google Scholar]
- Del Fabbro, M.; Testori, T.; Kekovic, V.; Goker, F.; Tumedei, M.; Wang, H.L. Systematic review of survival rates of osseointegrated implants in fully and partially edentulous patients following immediate loading. J. Clin Med. 2019, 8, 2142. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Ortiz-García, I.; Jiménez-Guerra, J.; Monsalve-Guil, L.; Muñoz-Guzón, F.; Perez, R.A.; Gil, F.J. Comparison between sandblasted-acid etched and oxidized titanium dental implants: In vivo study. Int J. Mol Sci. 2019, 20, 3267. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Cavalcanti de Lima, J.H.; Rodriguez, F.; Calvo-Guirado, J.L.; Aramburú Júnior, J.; Pérez-Díaz, L.; Mazón, P.; Aragoneses, J.M.; De Aza, P.N. Microgrooves and microrugosities in titanium implant surfaces: An in vitro and in vivo evaluation. Materials 2019, 12, 1287. [Google Scholar] [CrossRef] [PubMed]
- Nicolas-Silvente, A.I.; Velasco-Ortega, E.; Ortiz-Garcia, I.; Monsalve-Guil, L.; Gil, J.; Jiménez-Guerra, A. Influence of the titanium implant surface treatment on the surface roughness and chemical composition. Materials 2020, 13, 314. [Google Scholar] [CrossRef] [PubMed]
- Blatt, S.; Max Pabst, A.M.; Schiegnitz, E.; Hosang, M.; Ziebart, T.; Walter, C.; Al-Nawas, B.; Klein, M.O. Early cell response of osteogenic cells on differently modified implant surfaces: Sequences of cell proliferation, adherence and differentiation. J. Cranio Maxillo Fac Sur. 2018, 46, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Ortega, E.; Alfonso-Rodriguez, C.; Monsalve-Guil, L.; España-López, A.; Jiménez-Guerra, A.; Garzón, I.; Alaminos, M.; Gil, F.J. Relevant aspects in the surface properties in titanium dental implants for the cellular viability. Mater. Sci Eng C Mater. Biol Appl. 2016, 64, 1–10. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1. Review focusing on topographic and chemical property surfaces and in vivo responses to them. Int J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 2. Review focusing on clinical knowledge of different surfaces. Int J. Prosthodont. 2004, 17, 544–564. [Google Scholar]
- Rupp, F.; Lianga, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface characteristics of dental implants: A review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Monsalve-Guil, L.; Jiménez, A.; Ortiz, I.; Moreno-Muñoz, J.; Nuñez-Márquez, E.; Pegueroles, M.; Perez, R.; Gil, F.J. Importance of the surface roughness and residual stress of dental implants on fatigue and osseointegration behavior in rabbits. J. Oral Implantol. 2016, 42, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Abe, Y.; Yoshida, Y.; Nakayama, Y.; Okazaki, M.; Akagawa, Y. Acid pretreatment of titanium implants. Biomaterials 2003, 24, 1821–1827. [Google Scholar] [CrossRef]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface modifications and their effects on titanium dental implants. BioMed Res. Int. 2015, 791725. [Google Scholar] [CrossRef] [PubMed]
- Ban, S.; Iwaya, Y.; Kono, H.; Sato, H. Surface modification of titanium by etching in concentrated sulfuric acid. Dent. Mater. 2006, 22, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Klokkevold, P.R.; Nishimura, R.D.; Adachi, M.; Caputo, A. Osseointegration enhanced by chemical etching of the titanium surface: A torque removal study in the rabbit. Clin Oral Impl Res. 1997, 8, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Shayganpour, A.; Rebaudi, A.; Cortella, P.; Diaspro, A.; Salerno, M. Electrochemical coating of dental implants with anodic porous titania for enhanced osteointegration. Beilstein J. Nanotech. 2015, 6, 2183–2192. [Google Scholar] [CrossRef]
- Cho, S.A.; Park, K.T. The removal torque of titanium screw inserted in rabbit tibia treated by dual acid etching. Biomaterials 2003, 24, 3611–3617. [Google Scholar] [CrossRef]
- Mangano, F.G.; Pires, J.T.; Shibli, J.A.; Mijiritsky, E.; Iezzi, G.; Piattelli, A.; Mangano, C. Early bone response to dual acid-etched and machined dental implants placed in the posterior maxilla: A histologic and histomorphometric human study. Impl Dent. 2017, 26, 24–29. [Google Scholar] [CrossRef]
- Peñarrocha, M.; Carrillo, C.; Boronat, A.; Martí, E. Early loading of 642 Defcon implants: 1-year follow-up. J. Oral Maxillofac Surg. 2007, 65, 2317–2320. [Google Scholar] [CrossRef]
- Browaeys, H.; Defrancq, J.; Dierens, M.C.A.; Miremadi, R.; Vandeweghe, S.; van de Velde, T.; De Bruyn, H. A retrospective analysis of early and immediately loaded Osseotite implants in cross-arch rehabilitations in edentulous maxillas and mandibles up to 7 years. Clin Impl Dent. Relat Res. 2013, 15, 380–389. [Google Scholar] [CrossRef]
- Balshi, T.J.; Wolfinger, G.J.; Balshi, S.F.; Bidra, A.S. A 30-year follow-up of a patient with mandibular complete-arch fixed implant-supported prosthesis on 4 implants: A clinical report. J. Prosthodont. 2019, 28, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Simonis, P.; Dufour, T.; Tenenbaum, H. Long-term implant survival and success: A 10–16-year follow-up of non-submerged dental implants. Clin Oral Impl Res. 2010, 21, 772–777. [Google Scholar] [CrossRef]
- Su, M.Y.; Shi, B.; Zhu, Y.; Guo, Y.I.; Zhang, Y.; Xia, H.; Zhao, L. Comparison of implant success rates with different loading protocols: A meta-analysis. Int J. Oral Maxillofac Implants. 2014, 29, 344–352. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Papaspyridakos, P.; Mokti, M.; Chen, C.J.; Benic, G.I.; Gallucci, G.O.; Chronopoulos, V. Implant and prosthodontic survival rates with implant fixed complete dental prostheses in the edentulous mandible after at least 5 years:a systematic review. Clin Impl Dent. Relat Res. 2014, 16, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Wittneben, J.G.; Millen, C.; Brägger, U. Clinical performance of screw-versus cement-retained fixed implant-supported reconstructions- a systematic review. Int J. Oral Maxillofac Implant. 2014, 29, 84–98. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Carrascal, N.; Salomó-Coll, O.; Gilabert-Cerdà, M.; Farré-Pagés, N.; Gargallo-Albiol, J.; Hernández-Alfaro, F. Effect of implant macro-design on primary stability: A prospective clinical study. Med. Oral Patol Oral Cir. Bucal. 2016, 21, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.V.; Vandamme, K.; Chaudhari, A.; De Rycker, J.; Van Meerbeek, B.; Naert, I.; Duyck, J. Dental implant macro-design features can impact the dynamics of osseointegration. Clin Implant. Dent. Relat Res. 2015, 17, 639–645. [Google Scholar] [CrossRef]
- Martínez-González, J.M.; Barona-Dorado, C.; Cano-Sánchez, J.; Fernández-Cáliz, F.; Sánchez-Turrión, A. Evaluation of 80 implants subjected to immediate loading in edentulous mandibles after two years of follow-up. Med. Oral Patol Oral Cir. Bucal. 2006, 11, 165–170. [Google Scholar]
- Lazzara, R.J.; Porter, S.S.; Testori, T.; Galante, J.; Zetterqvist, L. A prospective multicenter study evaluating loading of Osseotite implants two months after placement: One year results. J. Esthet Dent. 1998, 10, 280–289. [Google Scholar] [CrossRef]
- Sullivan, D.; Vincenzi, G.; Feldman, S. Early loading of Osseotite implants 2 months after placement in the maxilla and mandible: A 5-year report. Int J. Oral Maxillofac Implant. 2005, 20, 905–912. [Google Scholar]
- Peñarrocha, M.; Boronat, A.; García, B. Immediate loading of immediate mandibular implants with a full-arch fixed prosthesis: A preliminary study. J. Oral Maxillofac Surg. 2009, 67, 1286–1293. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Gómez-Moreno, G.; Delgado-Ruiz, R.A.; Maté Sánchez de Val, J.E.; Negri, B.; Ramírez-Fernández, M.P. Clinical and radiographic evaluation of osseotite-expanded platform implants related to crestal bone loss: A 10-year study. Clin Oral Implant. Res. 2014, 25, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, J.M.; García-Sabán, F.; Ferrándiz-Bernal, J.; Gonzalo-Lafuente, J.C.; Cano-Sánchez, J.; Barona-Dorado, C. Removal torque and physico-chemical characteristics of dental implants etched with hydro-fluoric and nitric acid. An experimental study in Beagle dogs. Med. Oral Patol Oral Cir. Bucal. 2006, 11, 281–285. [Google Scholar]
- Marenzi, G.; Impero, F.; Scherillo, F.; Sammartino, J.C.; Squillace, A.; Spagnuolo, G. Effect of different surface treatments on titanium dental implant micro-morphology. Materials 2019, 12, 733. [Google Scholar] [CrossRef] [PubMed]
- Shah, F.A.; Stenlund, P.; Martinelli, A.; Thomsen, P.; Palmquist, A. Direct communication between osteocytes and acid-etched titanium implants with a sub-micron topography. J. Mater. Sci. Mater. Med. 2016, 27, 167. [Google Scholar] [CrossRef]
- Carmo Filho, L.C.; Marcello-Machado, R.M.; Castilhos, E.D.; del bel Cury, A.A.; Faot, F. Can implant surfaces affect implant stability during osseointegration? A randomized clinical trial. Braz Oral Res. 2018, 32, 110. [Google Scholar] [CrossRef]
- Khang, W.; Feldman, S.; Hawley, C.E.; Gunsolley, J. A multi-center study comparing dual acid-etched and machined-surfaced implants in various bone qualities. J. Periodontol. 2001, 72, 1384–1390. [Google Scholar] [CrossRef]
- Nicoli, L.G.; de Oliveira, G.J.P.L.; Lopes, B.M.V.; Marcantonio, C.; Zandim-Barcelos, D.L.; Marcantonio Jr., E. Survival/success of dental implants with acid-etched surfaces: A retrospective evaluation after 8 to 10 years. Braz Dent. J. 2017, 28, 330–336. [Google Scholar] [CrossRef]
- Montero, J.; Fernández-Ruiz, J.; Pardal-Peláez, B.; Jiménez-Guerra, A.; Velasco-Ortega, E.; Nicolas-Silvente, A.I.; Monsalve-Guil, L. Effect of rough surface platforms on the mucosal attachment and the marginal bone loss of implants: A dog study. Materials 2020, 13, 802. [Google Scholar] [CrossRef]
- Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone loss in implants placed at subcrestal and crestal level: A systematic review and meta-analysis. Materials 2019, 12, 154. [Google Scholar] [CrossRef]
- Barona-Dorado, C.; Martínez-Rodríguez, N.; Torres-Lear, F.; Martínez- González, J.M. Observational study of 67 wide platform implants treated with avantblast surface. Results at three years. Med. Oral Patol Oral Cir. Bucal. 2009, 14, 183–187. [Google Scholar]
- Nobre, M.A.; Maló, P. Prevalence of periodontitis, dental caries, and peri-implant pathology and their relation with systemic status and smoking habits: Results of an open cohort study with 22009 patients in a private rehabilitation center. J. Dent. 2017, 67, 36–42. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Patients | n = 48 (100%) | Age | 52.4 yrs (Ranged 30–72) |
|---|---|---|---|
| Gender | Male | Female | |
| n = 48 (100%) | n = 26 (51.4%) | n = 22 (48.6%) | |
| SmokingHabit | Smoker | Nonsmoker | |
| n = 48 (100%) | n = 26 (51.4%) | n = 26 (51.4%) | |
| Periodontitis History | Yes | No | |
| n = 48 (100%) | n = 11 (22.9%) | n = 37 (77.1%) | |
| Edentulism | Totally | Partially | |
| n = 48 (100%) | n = 11 (22.9%) | n = 37 (77.1%) |
| Implant Characteristics | N = 169 (100%) | |
|---|---|---|
| Diameter | 4 mm | 3.4 mm |
| 99 implants (58.7%) | 70 implants (41.3%) | |
| Length | 13 mm | 10 mm |
| 50 implants (29.6%) | 119 implants (70.4%) | |
| Location | Maxilla | Mandible |
| 79 implants (46.7%) | 90 implants (53.3%) | |
| Area | Anterior | Posterior |
| 82 implants (48.5%) | 87 implants (51.5%) | |
| Percentage of Failure/Success | Failure | Success |
| 12 implants (7.1%) | 157 implants (92.9%) | |
| Number of Implants | Single Crown | Fixed Bridge | Overdenture | Fixed Full-Arch |
|---|---|---|---|---|
| 1 | 30 (46.1%) | -- | -- | -- |
| 2 | -- | 13 (20.0%) | -- | -- |
| 3 | -- | 7 (10.7%) | 1 (1.5%) | -- |
| 4 | -- | 1 (1.5%) | 8 (12.3%) | -- |
| 9 | -- | -- | -- | 2 (3.1%) |
| 10 | -- | -- | -- | 3 (4.6%) |
| Total Prostheses | ||||
| 65 (100%) | 30 (46.1%) | 21 (32.3%) | 9 (13.8%) | 5 (87.6%) |
| Screwed /Cemented | ||||
| 65 (100%) | 44 (67.6%) Screwed | 21 (32.4%) Cemented | ||
| Complications | + | - |
|---|---|---|
| Patients Showing Complications | 22 patients (48.6%) | 26 patients (51.4%) |
| Early Implant Loss | 3 patients (6.2%) | 45 patients (93.8%) |
| Delayed Implant Loss | 5 patients (10.4%) | 43 patients (89.6%) |
| Peri-Implantitis | 10 patients (22.8%) | 38 patients (77.2%) |
| Technical Complications | 12 patients (26.6%) | 36 patients (73.4%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velasco-Ortega, E.; Jimenez-Guerra, A.; Monsalve-Guil, L.; Ortiz-Garcia, I.; Nicolas-Silvente, A.I.; Segura-Egea, J.J.; Lopez-Lopez, J. Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface. Materials 2020, 13, 1553. https://doi.org/10.3390/ma13071553
Velasco-Ortega E, Jimenez-Guerra A, Monsalve-Guil L, Ortiz-Garcia I, Nicolas-Silvente AI, Segura-Egea JJ, Lopez-Lopez J. Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface. Materials. 2020; 13(7):1553. https://doi.org/10.3390/ma13071553
Chicago/Turabian StyleVelasco-Ortega, Eugenio, Alvaro Jimenez-Guerra, Loreto Monsalve-Guil, Ivan Ortiz-Garcia, Ana I. Nicolas-Silvente, Juan J. Segura-Egea, and Jose Lopez-Lopez. 2020. "Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface" Materials 13, no. 7: 1553. https://doi.org/10.3390/ma13071553
APA StyleVelasco-Ortega, E., Jimenez-Guerra, A., Monsalve-Guil, L., Ortiz-Garcia, I., Nicolas-Silvente, A. I., Segura-Egea, J. J., & Lopez-Lopez, J. (2020). Long-Term Clinical Outcomes of Treatment with Dental Implants with Acid Etched Surface. Materials, 13(7), 1553. https://doi.org/10.3390/ma13071553