Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Dental Implants and Experimental Groups
2.2. Evaluation of the Implant Surface Roughness
2.2.1. Data Acquisition
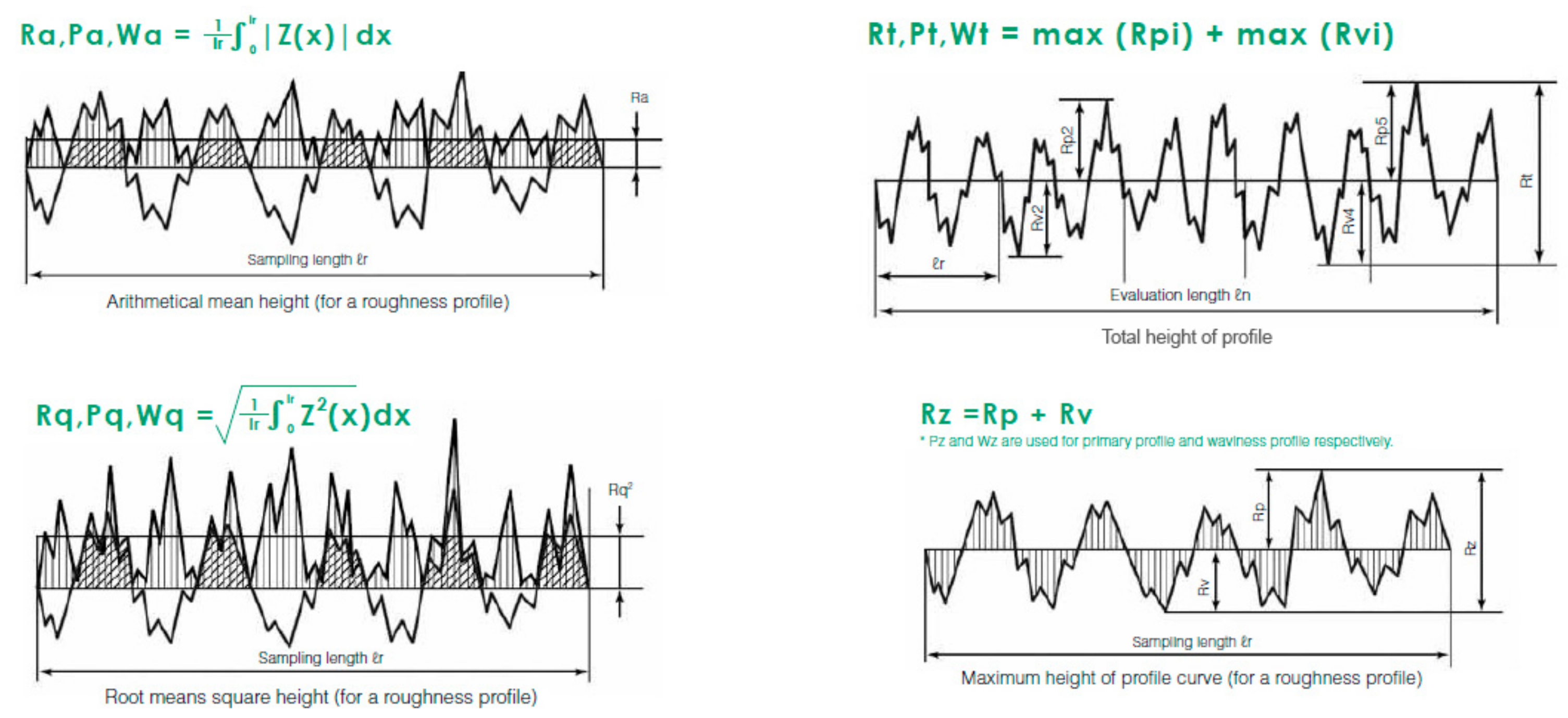
2.2.2. Roughness Parameters
- a.
- The arithmetical mean roughness (Ra): the arithmetical mean height indicates the average of the absolute value along the sampling length.
- b.
- Root mean square deviation (Rq): indicates the root mean square along the sampling length.
- c.
- Total height of profile (Rt): indicates the vertical distance between the maximum profile peak height and the maximum profile valley depth along the evaluation length.
- d.
- Maximum height of profile (Rz): indicates the absolute vertical distance between the maximum profile peak height and the maximum profile valley depth along the sampling length [27].
2.2.3. Statistical Analysis
2.3. Evaluation of the Surface Chemical Composition
Data Acquisition
- Stage 1: as received by the manufacturer (AR), with a maximum time of two minutes of exposure to the air from the opening of the implant container until it was analyzed.
- Stage 2: After performing a 30-min sputter cleaning (SC) with an argon ion cannon, at an energy of 1 kV and a surface area of 1 mm2.
3. Results
3.1. Roughness of the Analyzed Surfaces. Quantitative Findings
3.2. Topography of the Analyzed Surfaces. Qualitative Findings
3.3. Surface Chemical Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Velasco-Ortega, E.; Alfonso-Rodríguez, C.A.; Monsalve-Guil, L.; España-López, A.; Jiménez-Guerra, A.; Garzón, I.; Alaminos, M.; Gil, F.J. Relevant aspects in the surface properties in titanium dental implants for the cellular viability. Mater. Sci. Eng. C 2016, 64, 1–10. [Google Scholar] [CrossRef]
- Deligianni, D.D.; Katsala, N.D.; Koutsoukos, P.G.; Missirlis, Y.F. Effect of surface roughness of hydroxyapatite on human bone marrow cell adhesion, proliferation, differentiation and detachment strength. Biomaterials 2000, 22, 87–96. [Google Scholar] [CrossRef]
- Sun, J.S.; Tsuang, Y.H.; Chang, W.H.; Li, J.; Liu, H.C.; Lin, F.H. Effect of hydroxyapatite particle size on myoblasts and fibroblasts. Biomaterials 1997, 18, 683–690. [Google Scholar] [CrossRef]
- Hanein, D.; Sabanay, H.; Addadi, L.; Geiger, B. Selective interactions of cells with crystal surfaces. J. Cell. Sci. 1993, 104, 275–288. [Google Scholar]
- De Bruijn, J.D.; van Blitterswijk, C.A.; Davies, J.E. Initial bone matrix formation at the hydroxyapatite interface in vitro. J. Biomed. Mater. Res. 1995, 29, 89–99. [Google Scholar] [CrossRef]
- Best, S.; Sim, B.; Kayser, M.; Downes, S. The dependence of osteoblastic response on variations in the chemical composition and physical properties of hydroxyapatite. J. Mater. Sci. Mater. Med. 1997, 8, 97–103. [Google Scholar] [CrossRef]
- Shin, Y.; Akao, M. Tissue reactions to various percutaneous materials with different surface properties and structures. Artif. Organs 1997, 21, 995–1001. [Google Scholar] [CrossRef]
- Kim, H.; Choi, S.; Ryu, J.; Koh, S.; Park, J.; Lee, I.S. The biocompatibility of SLA-treated titanium implants. Biomed. Mater. 2008, 3, 234–240. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Nakamura, T.; Kobayashi, M.; Kim, H.M.; Miyaji, F.; Kokubo, T. The effect of heat treatment on bone-bonding ability of alkali-treated titanium. Biomaterials 1999, 20, 491–500. [Google Scholar] [CrossRef]
- Aparicio, C.; Rodriguez, D.; Gil, F.J. Variation of roughness and adhesion strength of deposited apatite layers on titanium dental implants. Mater. Sci. Eng. C. 2011, 31, 320–324. [Google Scholar] [CrossRef]
- Von Wilmowsky, C.; Moest, T.; Nkenke, E.; Stelzle, F.; Schlegel, K.A. Implants in bone: Part I. A current overview about tissue response, surface modifications and future perspectives. Oral Maxillofac. Surg. 2014, 18, 243–257. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1-review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Albrektsson, T.; Branemark, P.I.; Hansson, H.A.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef]
- Fukuda, A.; Takemoto, M.; Saito, T.; Fujibayashi, S.; Neo, M.; Pattanayak, D.K.; Sasaki, K.; Nishida, N.; Kokubo, T.; Nakamura, T. Osteoinduction of porous Ti implants with a channel structure fabricated by selective laser melting. Acta Biomater. 2011, 7, 2327–2336. [Google Scholar] [CrossRef]
- Takeuchi, K.; Saruwatari, L.; Nakamura, H.K.; Yang, J.M.; Ogawa, T. Enhanced intrinsic biomechanical properties of osteoblastic mineralized tissue on roughened titanium surface. J. Biomed. Mater. Res 2005, 72, 296–305. [Google Scholar] [CrossRef]
- Ferraris, S.; Spriano, S.; Pan, G.; Venturello, A.; Bianchi, C.L.; Chiesa, R.; Faga, M.G.; Maina, G.; Verne, E. Surface modification of Ti-6Al-4V alloy for biomineralization and specific biological response: Part I, inorganic modification. J. Mater. Sci. Mater. Med. 2011, 22, 533–545. [Google Scholar] [CrossRef]
- Ferraris, S.; Truffa Giachet, F.; Miola, M.; Bertone, E.; Varesano, A.; Vineis, C.; Cochis, A.; Sorrentino, R.; Rimondini, L.; Spriano, S. Nanogrooves and keratin nanofibers on titanium surfaces aimed at driving gingival fibroblasts alignment and proliferation without increasing bacterial adhesion. Mater. Sci. Eng. 2017, 76, 1–12. [Google Scholar] [CrossRef]
- Deppe, H.; Wolff, C.; Bauer, F.; Ruthenberg, R.; Sculean, A.; Mücke, T. Dental implant surfaces after insertion in bone: An in vitro study in four commercial implant systems. Clin. Oral. Invest. 2017, 22, 1593–1600. [Google Scholar] [CrossRef]
- Massaro, C.; Rotolo, P.; de Ricardis, F.; Milella, E.; Napoli, A.; Wieland, M. Comparative investigation of the surface properties of commercial titanium dental implants. Part I: Chemical composition. J. Mater. Sci. Mater. Med. 2002, 13, 535–548. [Google Scholar] [CrossRef]
- Marenzi, G.; Impero, F.; Scherillo, F.; Sammartino, J.C.; Squillace, A.; Spagnuolo, G. Effect of different surface treatments on titanium dental implant micro-morphology. Materials 2019, 12, 733. [Google Scholar] [CrossRef]
- Park, J.W.; Suh, J.Y.; Chung, H.J. Effects of calcium ion incorporation on osteoblast gene expression in MC3T3-E1 cells cultured on microstructured titanium surfaces. J. Biomed. Mat. Res. 2008, 86, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Lukaszewska-Kuskaa, M.; Wirstleinb, P.; Majchrowskic, R.; Dorocka-Bobkowskaa, B. Osteoblastic cell behaviour on modified titanium surfaces. Micron. 2018, 105, 55–63. [Google Scholar] [CrossRef]
- Vijayaraghavan, V.; Sabane, A.V. Hypersensitivity to titanium: A less explored area of research. J. Indian Prosthodont. Soc. 2012, 12, 201–207. [Google Scholar] [CrossRef]
- Mihara, I.; Havelund, R.; Gilmore, I.S. Embedding-free method for preparation of cross-sections of organic materials for micro chemical analysis using gas cluster ion beam sputtering. Anal. Chem. 2017, 89, 4781–4785. [Google Scholar] [CrossRef]
- Moharrami, M.; Perrotti, V.; Laculli, F.; Love, R.M.; Quaranta, A. Effects of air abrasive decontamination on titanium surfaces: A systematic review of in vitro studies. Clin. Impl. Dent. Relat. Res. 2019, 21, 398–421. [Google Scholar] [CrossRef]
- Saffarpour, A.; Nozari, A.; Fekrazad, R.; Saffarpour, A.; Heibati, M.N.; Iranparvar, K. Microstructural evaluation of contaminated implant surface treated by laser, photodynamic therapy, and chlorhexidine 2 percent. Int. J. Oral Maxillofac. Implants. 2018, 33, 1019–1026. [Google Scholar] [CrossRef]
- Keyence Surface Roughness Parameters. Available online: https://www.keyence.com/ss/products/microscope/roughness/line/parameters.jsp (accessed on 24 October 2019).
- Wennerberg, A.; Albrektsson, T. Suggested guidelines for the topographic evaluation of implant surfaces. Int. J. Oral Maxillofac. Imp. 2000, 15, 331–344. [Google Scholar]
- Mendonça, G.; Mendonça, D.B.S.; Aragao, F.J.L.; Cooper, L.F. Advancing dental implant surface technology-from micron-to nanotopography. Biomaterials 2008, 29, 3822–3835. [Google Scholar] [CrossRef]
- Webster, T.J.; Ejiofor, J.U. Increased osteoblast adhesion on nano phase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials 2004, 25, 4731–4739. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Monsalve-Guil, L.; Jiménez-Guerra, A.; Ortiz, I.; Moreno-Muñoz, J.; Nuñez-Marquez, E.; Pequeroles, M.; Perez, R.A.; Gil, F.J. Importance of the roughness and residual stresses of dental implants on fatigue and osseointegration behavior. In vivo study in rabbits. J. Oral Impl. 2016, 42, 469–476. [Google Scholar] [CrossRef]
- Elias, C.N.; Meirelles, L. Improving osseointegration of dental implants. Expert. Rev. Med. Devices 2010, 7, 241–256. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. On implant surfaces: A review of current knowledge and opinions. Int. J. Oral Maxillofac. Imp. 2010, 25, 63–74. [Google Scholar]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implants Res. 2009, 20, 172–184. [Google Scholar] [CrossRef]
- Rosa, M.B.; Albrektsson, T.; Francischone, C.E.; Schwartz Filho, H.O.; Wennerberg, A. The influence of surface treatment on the implant roughness pattern. J. App. Oral Sci. 2012, 20, 550–555. [Google Scholar] [CrossRef]
- Velasco-Ortega, E.; Ortiz-Garcia, I.; Jimenez-Guerra, A.; Monsalve-Guil, L.; Muñoz-Guzon, F.; Perez, R.A.; Gil, F.J. Comparison between sandblasted acid-etched and oxidized titanium dental implants: In vivo study. Int. J. Mol. Sci. 2019, 20, 3267. [Google Scholar] [CrossRef]
- Duddeck, D.U.; Albrektsson, T.; Wennerberg, A.; Larsson, C.; Beuer, F. On the cleanliness of different oral implant systems: A pilot study. J. Clin. Med. 2019, 8, 1280. [Google Scholar] [CrossRef]
- Naauman, Z.; Bin Rajion, Z.A.; Maliha, S.; Hariy, P.; Muhammad, Q.S.; Razak Noor, H.A. Ultraviolet A and Ultraviolet C Light–Induced reduction of surface hydrocarbons on titanium implants. Eur. J. Dent. 2019, 13, 114–118. [Google Scholar] [CrossRef]
- Ferraris, S.; Cazzola, M.; Peretti, V.; Stella, B.; Spriano, S. Zeta potential measurements on solid surfaces for in vitro biomaterials testing: Surface charge, reactivity upon contact with fluids and protein absorption. Front. Bioeng. Biotechnol. 2018, 6, 60. [Google Scholar] [CrossRef]
- Ferraris, S.; Cochis, A.; Cazzola, M.; Tortello, M.; Scalia, A.; Spriano, S.; Rimondini, L. Cytocompatible and Anti-bacterial Adhesion Nanotextured Titanium Oxide Layer on Titanium Surfaces for Dental and Orthopedic Implants. Front. Bioeng. Biotechnol. 2019, 7, 1–12. [Google Scholar] [CrossRef]
- Sansone, V.; Pagani, D.; Melato, M. The effect on bone cells of metal ion released from orthopaedic implants. A review. Clin. Cases Miner. Bone Metab. 2013, 10, 34–40. [Google Scholar] [CrossRef]
- Vermes, C.; Chandrasekaran, R.; Jacobs, J.J.; Galante, J.O.; Roebuck, K.A.; Glant, T.T. The effects of particulate wear debris, cytokines, and growth factors on the functions of MG-63 osteoblasts. J. Bone Joint Surg. Am. 2001, 83, 201–211. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | Implant Manufacturer | Implant System | Surface Name | Surface Treatment | Treatment Code |
|---|---|---|---|---|---|
| Group I | Straumann | BL | SLA® | large-grit sandblasting + | SB + AE |
| (n = 10) | acid-etching | ||||
| Group II | Microdent | Genius | ATEC® | Alumina sandblasting | SB (Al2O3) |
| (n = 10) | |||||
| Group III | Dentsply-Sirona | Astra Tech | OsseoSpeed® | Titanium Oxide sandblasting + | SB (TiO2) + F |
| (n = 10) | Fluoride treatment | ||||
| Group IV | Avinent | OCEAN® | Biomimetic® | Sandblasting + | SB + Ca + P |
| (n = 10) | Addition of calcium and Phosphorous | ||||
| Group V | Zimmer Biomet | Biomet 3i | Osseotite® | Double acid-etching | 2AE |
| (n = 10) | |||||
| Group VI | Klockner | Vega® | Vega® | Alumina sandblasting + | SB (Al2O3) + TCT |
| (n = 10) | thermochemical treatment | ||||
| Group VII | Ticare | inHex® | RBM TC® | Resorbable particles sandblasting + | SB (res) + 2AE |
| (n = 10) | Double acid-etching | ||||
| Group VIII | Nobel Biocare | NobelReplace® | TiUnite® | TiO2 layer | TiO2 |
| (n = 10) | |||||
| Group IX | Galimplant | IPX® | Nanoblast® | Sandblasting + | SB + 3AE |
| (n = 10) | Triple acid-etching |
| Implant System | Ra (µm) | Rq (µm) | Rt (µm) | Rz (µm) | Roughness Type |
|---|---|---|---|---|---|
| STRAUMANN® | 2.49 | 3.16 | 22.86 | 25.49 | highly rough |
| MICRODENT® | 1.07 | 1.37 | 15.01 | 28.09 | moderately rough |
| ASTRATECH® | 1.97 | 2.51 | 24.71 | 35.05 | moderately rough |
| AVINENT® | 2.39 | 3.07 | 27.58 | 35.95 | highly rough |
| BIOMET 3i® | 0.79 | 0.99 | 17.07 | 29.74 | minimally rough |
| KLOCKNER® | 2.89 | 3.74 | 29.32 | 34.52 | highly rough |
| MOZOGRAU® | 1.31 | 1.73 | 36.71 | 59.30 | moderately rough |
| NOBELBIOCARE® | 1.10 | 1.50 | 24.21 | 32.12 | moderately rough |
| GALIMPLANT® | 1.45 | 1.94 | 14.98 | 16.38 | moderately rough |
| Implant System | n | Minimum Ra | Maximum Ra | Mean Ra | Ra Standard Deviation |
|---|---|---|---|---|---|
| STRAUMANN® | 10 | 1.99 | 3.34 | 2.49 | 0.43126 |
| MICRODENT® | 10 | 0.95 | 1.13 | 1.07 | 0.05959 |
| ASTRATECH® | 10 | 1.80 | 2.14 | 1.97 | 0.10692 |
| AVINENT® | 10 | 1.99 | 2.78 | 2.39 | 0.27727 |
| BIOMET 3i® | 10 | 0.73 | 0.93 | 0.79 | 0.06567 |
| KLOCKNER® | 10 | 2.48 | 3.33 | 2.89 | 0.29578 |
| MOZOGRAU® | 10 | 1.06 | 1.47 | 1.31 | 0.11657 |
| NOBELBIOCARE® | 10 | 0.76 | 1.37 | 1.10 | 0.17735 |
| GALIMPLANT® | 10 | 1.07 | 1.72 | 1.45 | 0.24501 |
| System and Treat CODE | Stage | C | O | N | Ti | Al | Si | Ca | Na | Cl | Mg | P | Zn |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| STRAUMANN® | AR | 58.4 | 28.4 | 1.2 | 7.0 | X | 3.5 | 0.8 | 0.8 | X | X | X | X |
| SB+AE | SC | 23.8 | 47.8 | 0.9 | 25.5 | X | 1.8 | 0.2 | X | X | X | X | X |
| MICRODENT® | AR | 54.7 | 28.0 | 2.5 | 4.8 | 5.1 | 1.8 | 0.5 | 1.3 | 0.7 | 0.7 | X | X |
| SB (Al2O3) | SC | 23.9 | 41.6 | 0.9 | 17.5 | 15.3 | X | 0.1 | X | X | X | X | X |
| ASTRATECH® | AR | 81.9 | 13.8 | X | 1.8 | X | 1.0 | 1.4 | X | X | X | X | X |
| SB (TiO2)+F- | SC | 47.7 | 21.3 | 2.2 | 28.6 | X | X | 0.0 | X | X | X | X | X |
| AVINENT® | AR | 45.5 | 36.5 | 1.1 | 9.7 | 3.3 | 1.6 | 1.7 | X | X | X | 0.6 | X |
| SB+Ca+P | SC | 41.4 | 38.8 | 1.1 | 11.2 | 1.4 | 2.6 | 2.8 | X | X | X | 0.7 | X |
| BIOMET 3i® | AR | 40.2 | 39.6 | 1.2 | 11.8 | X | 7.2 | X | X | X | X | X | X |
| 2AE | SC | 38.2 | 27.5 | 2.3 | 32.1 | X | X | X | X | X | X | X | X |
| KLOCKNER® | AR | 62.6 | 23.6 | 1.1 | 2.9 | 4.3 | 4.8 | 0.4 | X | X | X | 0.5 | X |
| SB (Al2O3)+TCT | SC | 64.1 | 18.3 | X | 7.3 | 8.5 | 1.7 | X | X | X | X | X | X |
| MOZOGRAU® | AR | 73.5 | 18.2 | 0.4 | 2.7 | X | 2.3 | 1.3 | 0.7 | X | X | 1.0 | X |
| SB (res)+2AE | SC | 47.7 | 21.3 | 2.2 | 28.6 | X | X | 0.2 | X | X | X | X | X |
| NOBELBIOCARE® | AR | 82.4 | 12.2 | X | 0.7 | X | 2.0 | 1.9 | X | X | X | 0.8 | X |
| TiO2 | SC | 69.9 | 18.8 | X | 8.5 | X | 1.7 | 0.8 | X | X | X | 2.0 | X |
| GALIMPLANT® | AR | 53.1 | 31.2 | 1.0 | 8.4 | X | 3.7 | 1.2 | X | X | X | X | 0.50 |
| SB+3AE | SC | 33.7 | 27.1 | 3.7 | 31.5 | X | X | X | X | X | X | X | X |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolas-Silvente, A.I.; Velasco-Ortega, E.; Ortiz-Garcia, I.; Monsalve-Guil, L.; Gil, J.; Jimenez-Guerra, A. Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition. Materials 2020, 13, 314. https://doi.org/10.3390/ma13020314
Nicolas-Silvente AI, Velasco-Ortega E, Ortiz-Garcia I, Monsalve-Guil L, Gil J, Jimenez-Guerra A. Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition. Materials. 2020; 13(2):314. https://doi.org/10.3390/ma13020314
Chicago/Turabian StyleNicolas-Silvente, Ana Isabel, Eugenio Velasco-Ortega, Ivan Ortiz-Garcia, Loreto Monsalve-Guil, Javier Gil, and Alvaro Jimenez-Guerra. 2020. "Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition" Materials 13, no. 2: 314. https://doi.org/10.3390/ma13020314
APA StyleNicolas-Silvente, A. I., Velasco-Ortega, E., Ortiz-Garcia, I., Monsalve-Guil, L., Gil, J., & Jimenez-Guerra, A. (2020). Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition. Materials, 13(2), 314. https://doi.org/10.3390/ma13020314