Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Drill Hole Defect Model
2.2. Surgery
2.3. Serum Concentration of Gentamicin
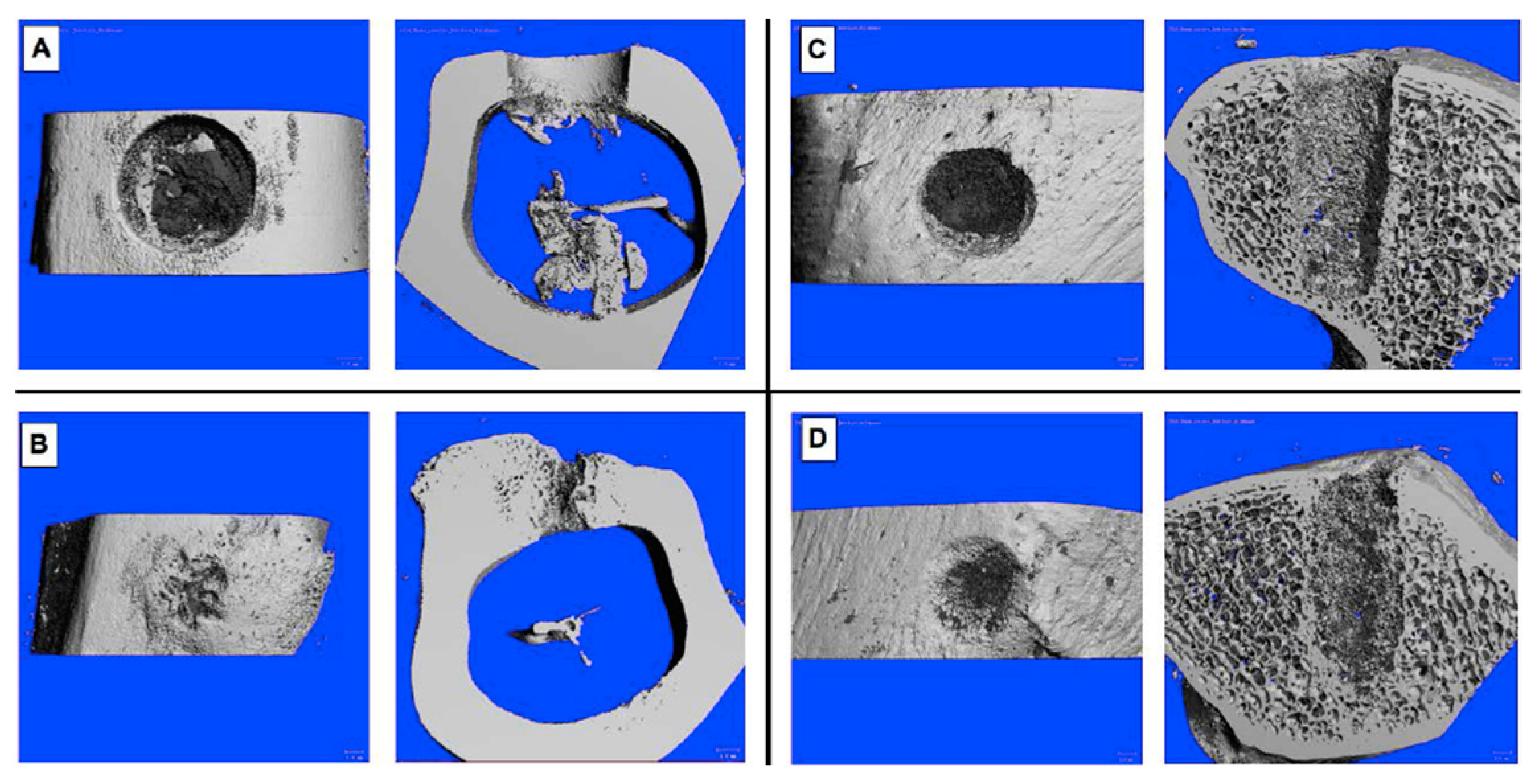
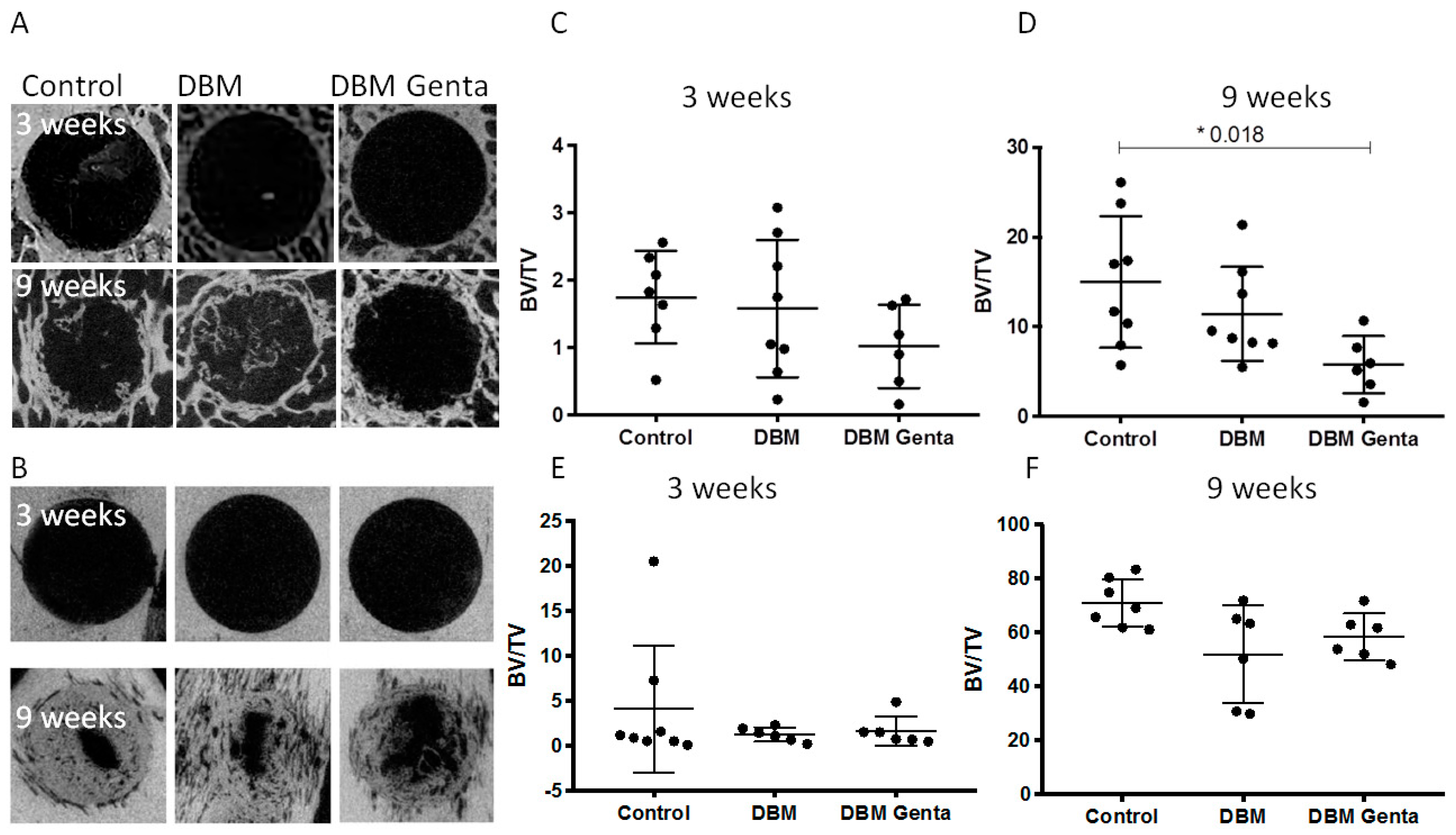
2.4. Micro-Computed Tomography (µCT)
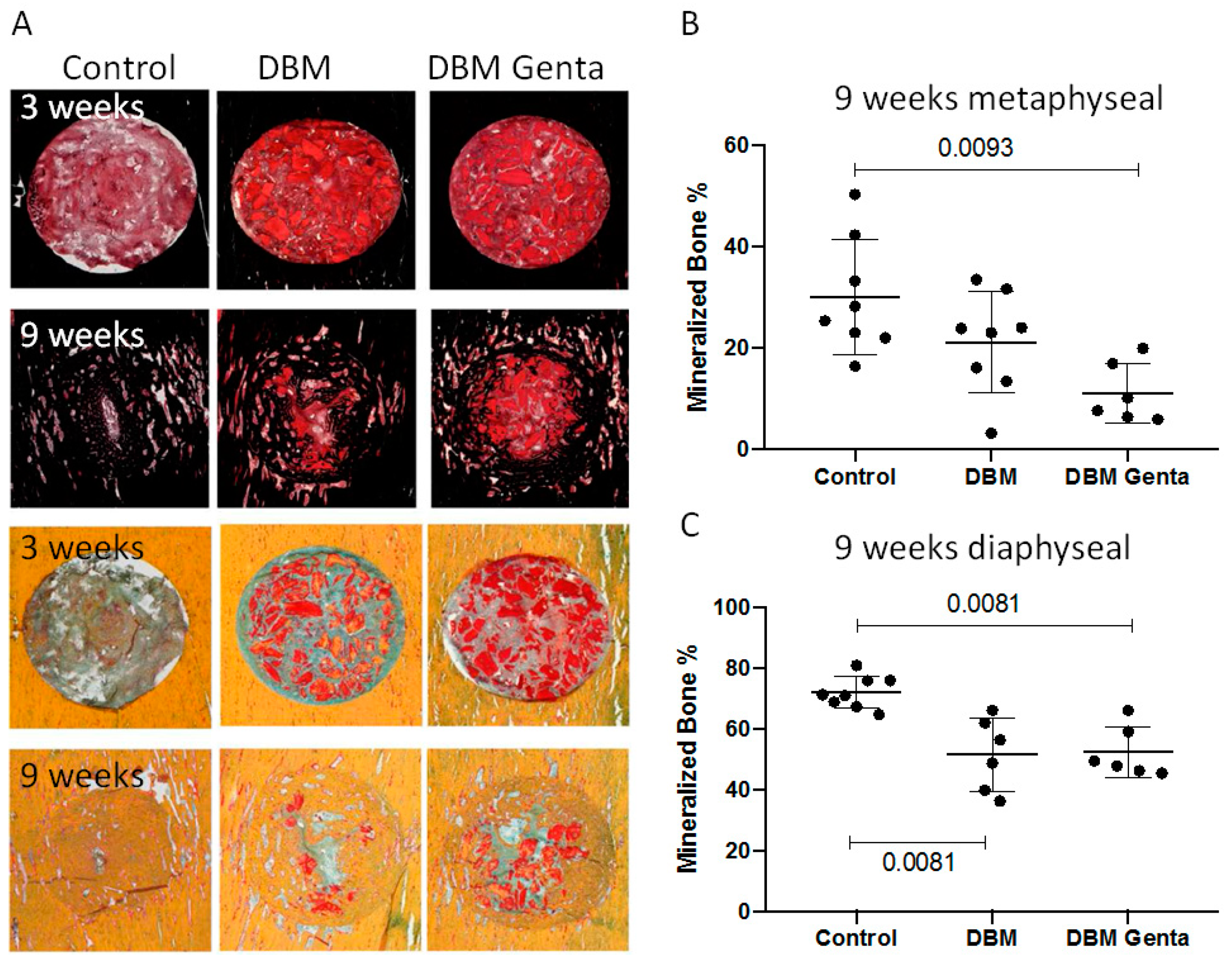
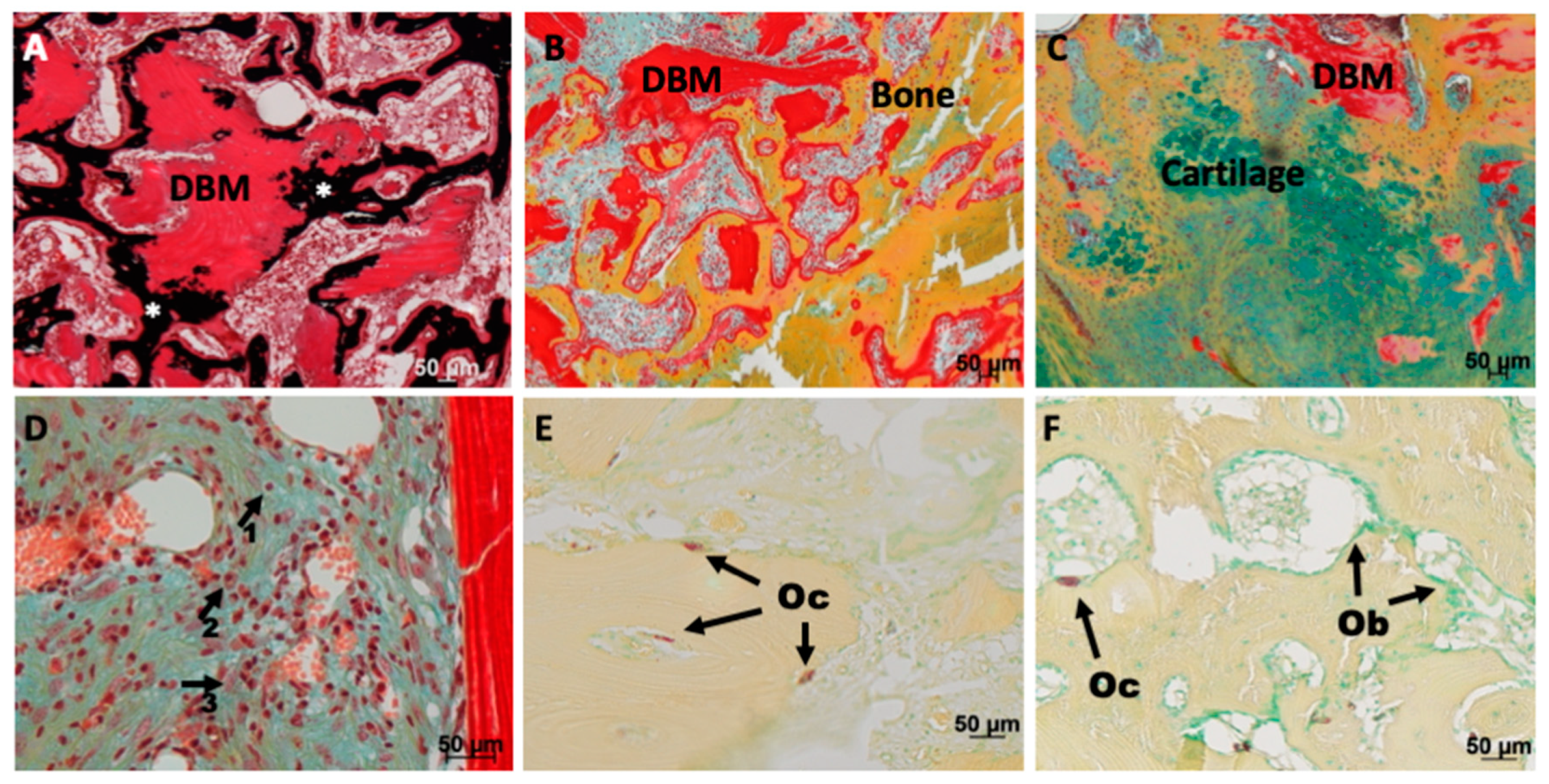
2.5. Histology and Histomorphometry
2.6. Statistical Analysis
3. Results
3.1. µCT Analysis of the Defect Healing
3.2. Histological Analysis of the Defect Healing
3.3. Serumconcentration of Gentamicin
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rao, N.; Ziran, B.H.; Lipsky, B.A. Treating osteomyelitis: Antibiotics and surgery. Plast. Reconstr. Surg. 2011, 127 (Suppl. 1), 177S–187S. [Google Scholar] [CrossRef] [PubMed]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications following autologous bone graft harvesting from the iliac crest and using the ria: A systematic review. Injury 2011, 42 (Suppl. 2), S3–S15. [Google Scholar]
- Calori, G.M.; Colombo, M.; Mazza, E.L.; Mazzola, S.; Malagoli, E.; Mineo, G.V. Incidence of donor site morbidity following harvesting from iliac crest or ria graft. Injury 2014, 45 (Suppl. 6), S116–S120. [Google Scholar] [CrossRef] [PubMed]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef] [PubMed]
- Cicciu, M. Real opportunity for the present and a forward step for the future of bone tissue engineering. J. Craniofac. Surg. 2017, 28, 592–593. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, H.W.; Engelbrecht, H. Depot effects of various antibiotics mixed with palacos resins. Chirurg 1970, 41, 511–515. [Google Scholar]
- Parvizi, J.; Saleh, K.J.; Ragland, P.S.; Pour, A.E.; Mont, M.A. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008, 79, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, K.D.; Renz, N.; Trampuz, A. Local antibiotic therapy. Unfallchirurg 2017, 120, 561–572. [Google Scholar]
- Levack, A.E.; Cyphert, E.L.; Bostrom, M.P.; Hernandez, C.J.; von Recum, H.A.; Carli, A.V. Current options and emerging biomaterials for periprosthetic joint infection. Curr. Rheumatol. Rep. 2018, 20, 33. [Google Scholar]
- Fleischman, A.N.; Austin, M.S. Local intra-wound administration of powdered antibiotics in orthopaedic surgery. J. Bone Jt. Infect. 2017, 2, 23–28. [Google Scholar]
- Coraca-Huber, D.C.; Ammann, C.G.; Nogler, M.; Fille, M.; Frommelt, L.; Kuhn, K.D.; Folsch, C. Lyophilized allogeneic bone tissue as an antibiotic carrier. Cell Tissue Bank. 2016, 17, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.; Diefenbeck, M.; McNally, M. Ceramic biocomposites as biodegradable antibiotic carriers in the treatment of bone infections. J. Bone Jt. Infect. 2017, 2, 38–51. [Google Scholar] [CrossRef]
- Schmidmaier, G.; Lucke, M.; Wildemann, B.; Haas, N.P.; Raschke, M. Prophylaxis and treatment of implant-related infections by antibiotic-coated implants: A review. Injury 2006, 37 (Suppl. 2), S105–S112. [Google Scholar] [CrossRef] [PubMed]
- Isefuku, S.; Joyner, C.J.; Simpson, A.H. Gentamicin may have an adverse effect on osteogenesis. J. Orthop. Trauma 2003, 17, 212–216. [Google Scholar] [CrossRef]
- Bormann, N.; Schwabe, P.; Smith, M.D.; Wildemann, B. Analysis of parameters influencing the release of antibiotics mixed with bone grafting material using a reliable mixing procedure. Bone 2014, 59, 162–172. [Google Scholar] [CrossRef]
- Pobloth, A.M.; Johnson, K.A.; Schell, H.; Kolarczik, N.; Wulsten, D.; Duda, G.N.; Schmidt-Bleek, K. Establishment of a preclinical ovine screening model for the investigation of bone tissue engineering strategies in cancellous and cortical bone defects. BMC Musculoskelet. Disord. 2016, 17, 111. [Google Scholar] [CrossRef]
- Huber, E.; Pobloth, A.M.; Bormann, N.; Kolarczik, N.; Schmidt-Bleek, K.; Schell, H.; Schwabe, P.; Duda, G.N.; Wildemann, B. (*) demineralized bone matrix as a carrier for bone morphogenetic protein-2: Burst release combined with long-term binding and osteoinductive activity evaluated in vitro and in vivo. Tissue Eng. Part A 2017, 23, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Goldberg, V.M.; Caplan, A.I. Toxic effects of gentamicin on marrow-derived human mesenchymal stem cells. Clin. Orthop. Relat. Res. 2006, 452, 242–249. [Google Scholar] [CrossRef]
- Jiranek, W.A.; Hanssen, A.D.; Greenwald, A.S. Antibiotic-loaded bone cement for infection prophylaxis in total joint replacement. J. Bone Jt. Surg. Am. 2006, 88, 2487–2500. [Google Scholar] [CrossRef] [PubMed]
- Wahlig, H.; Dingeldein, E. Antibiotics and bone cements. Experimental and clinical long-term observations. Acta Orthop. Scand. 1980, 51, 49–56. [Google Scholar] [CrossRef]
- Shiels, S.M.; Raut, V.P.; Patterson, P.B.; Barnes, B.R.; Wenke, J.C. Antibiotic-loaded bone graft for reduction of surgical site infection in spinal fusion. Spine J. 2017, 17, 1917–1925. [Google Scholar] [CrossRef]
- Lewis, C.S.; Supronowicz, P.R.; Zhukauskas, R.M.; Gill, E.; Cobb, R.R. Local antibiotic delivery with demineralized bone matrix. Cell Tissue Bank. 2012, 13, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Shiels, S.M.; Cobb, R.R.; Bedigrew, K.M.; Ritter, G.; Kirk, J.F.; Kimbler, A.; Finger Baker, I.; Wenke, J.C. Antibiotic-loaded bone void filler accelerates healing in a femoral condylar rat model. Bone Jt. J. 2016, 98-B, 1126–1131. [Google Scholar] [CrossRef]
- Coraca-Huber, D.C.; Hausdorfer, J.; Fille, M.; Nogler, M. Effect of storage temperature on gentamicin release from antibiotic-coated bone chips. Cell Tissue Bank. 2013, 14, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Coraca-Huber, D.C.; Hausdorfer, J.; Fille, M.; Steidl, M.; Nogler, M. Effect of two cleaning processes for bone allografts on gentamicin impregnation and in vitro antibiotic release. Cell Tissue Bank. 2013, 14, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Coraca-Huber, D.C.; Putzer, D.; Fille, M.; Hausdorfer, J.; Nogler, M.; Kuhn, K.D. Gentamicin palmitate as a new antibiotic formulation for mixing with bone tissue and local release. Cell Tissue Bank. 2014, 15, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Coraca-Huber, D.C.; Wurm, A.; Fille, M.; Hausdorfer, J.; Nogler, M.; Kuhn, K.D. Effect of freezing on the release rate of gentamicin palmitate and gentamicin sulfate from bone tissue. J. Orthop. Res. 2014, 32, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Pforringer, D.; Harrasser, N.; Muhlhofer, H.; Kiokekli, M.; Stemberger, A.; van Griensven, M.; Lucke, M.; Burgkart, R.; Obermeier, A. Osteoinduction and -conduction through absorbable bone substitute materials based on calcium sulfate: In vivo biological behavior in a rabbit model. J. Mater. Sci. Mater. Med. 2018, 29, 17. [Google Scholar] [CrossRef]
- Pforringer, D.; Obermeier, A.; Kiokekli, M.; Buchner, H.; Vogt, S.; Stemberger, A.; Burgkart, R.; Lucke, M. Antimicrobial formulations of absorbable bone substitute materials as drug carriers based on calcium sulfate. Antimicrob. Agents Chemother. 2016, 60, 3897–3905. [Google Scholar] [CrossRef]
- Pforringer, D.; Harrasser, N.; Beirer, M.; Cronlein, M.; Stemberger, A.; van Griensven, M.; Lucke, M.; Burgkart, R.; Obermeier, A. Influence of absorbable calcium sulfate-based bone substitute materials on human haemostasis-in vitro biological behavior of antibiotic loaded implants. Materials 2018, 11, 935. [Google Scholar] [CrossRef]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cell Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beuttel, E.; Bormann, N.; Pobloth, A.-M.; Duda, G.N.; Wildemann, B. Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model. Materials 2019, 12, 1116. https://doi.org/10.3390/ma12071116
Beuttel E, Bormann N, Pobloth A-M, Duda GN, Wildemann B. Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model. Materials. 2019; 12(7):1116. https://doi.org/10.3390/ma12071116
Chicago/Turabian StyleBeuttel, Elisabeth, Nicole Bormann, Anne-Marie Pobloth, Georg N. Duda, and Britt Wildemann. 2019. "Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model" Materials 12, no. 7: 1116. https://doi.org/10.3390/ma12071116
APA StyleBeuttel, E., Bormann, N., Pobloth, A.-M., Duda, G. N., & Wildemann, B. (2019). Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model. Materials, 12(7), 1116. https://doi.org/10.3390/ma12071116