

The Impact of Coping Strategies and Individual Resilience on Anxiety and Depression among Construction Supervisors



Abstract
1. Introduction
1.1. Literature Review
1.1.1. Coping
1.1.2. Resilience
1.1.3. Coping with Stress in the Construction Industry
1.1.4. Hypothesis of the Study
2. Methodology
2.1. Research Instruments
2.1.1. Patient Health Questionnaire-9 (PHQ-9)
2.1.2. Generalised Anxiety Disorder-2 (GAD-2)
2.1.3. Brief Resilience Scale (BRS)
2.1.4. Coping Strategies Instrument
2.1.5. Semi-Structured Interviews
2.1.6. Face and Content Validity
2.2. Sample Size
2.3. Data Collection
2.4. Statistical Analysis
2.4.1. Quantitative Data Analysis
- No depression or depression—a supervisor is categorised as “depression” if they had PHQ-9 scores ≥ 5.
- No anxiety or anxiety—a supervisor is categorised as having “anxiety” if he or she has GAD-2 scores ≥ 3.
- No suicidal ideation or suicidal ideation—a supervisor is categorised as having “suicidal ideation” if they ticked option two or above on item 9 of the PHQ-9, which indicates “a suicidal ideation experience”.
- Supervisors were categorised as “high resilience” if they had BRS score ≥ 4.31, “normal resilience”, and “low resilience” if their BRS score was 3.00–4.30 and 1.00–2.99, respectively.
- For coping strategies, “strongly disagree” was coded as 0 (i.e., No); “very little”, “moderately”, and “very great” were coded as 1 (i.e., Yes).
- For depression or anxiety symptoms, “not at all” was coded as 0; “several days”, “more than half the days”, and “nearly every day” were coded as 1.
- For resilience, BRS score 1.00–2.99 was coded as 0 (i.e., low); BRS 3.00–4.30 = 1 (i.e., normal); BRS ≥ 4.31 = 2 (i.e., high). The BRS scores were re-coded for moderation analysis, and to determine the reciprocal relationship between resilience and coping strategies, BRS 1.00–2.99 was coded as 0 (i.e., not resilient/low), and BRS scores ≥ 4.31 and 3.00–4.30” were re-coded as 1 (i.e., resilient/high).
2.4.2. Thematic Analysis
3. Results and Discussion
3.1. Profile of the Respondents
3.2. Mental Ill-Health Symptoms and Resilience Level among the Respondents
3.3. Association between Individual Resilience, Mental-Ill Health Symptoms, Suicidal Ideation, and Demographic Variables
3.4. Resilience and Mental Health
3.5. Coping Strategies Employed and Their Effects on Mental Health
3.6. Association between Individual Resilience, Coping Strategies and Mental Health
3.7. Discussion
4. Conclusions and Recommendations
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BRS QUESTIONNAIRE | |||||
|---|---|---|---|---|---|
| Respond to Each Statement Below by Ticking One Answer Per Row | Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree |
| I tend to bounce back quickly after a hard time of stress | 1 | 2 | 3 | 4 | 5 |
| I have a hard time making it through stressful events | 5 | 4 | 3 | 2 | 1 |
| It does not take me long to recover from a stressful event | 1 | 2 | 3 | 4 | 5 |
| It is hard for me to snap back when something bad happens | 5 | 4 | 3 | 2 | 1 |
| I come through difficult times with little trouble | 1 | 2 | 3 | 4 | 5 |
| It tend to take a long time to get over setbacks in my life | 5 | 4 | 3 | 2 | 1 |
| Correlations | ||||||
|---|---|---|---|---|---|---|
| Suicidal Ideation | Depression | Anxiety | Resilience | |||
| Spearman’s rho | Suicidal Ideation | Correlation Coefficient | 1.000 | 0.301 ** | 0.326 ** | −0.101 |
| Sig. (2-tailed) | . | 0.000 | 0.000 | 0.187 | ||
| N | 174 | 174 | 174 | 174 | ||
| Depression | Correlation Coefficient | 0.301 ** | 1.000 | 0.239** | −0.172 * | |
| Sig. (2-tailed) | 0.000 | . | 0.001 | 0.023 | ||
| N | 174 | 174 | 174 | 174 | ||
| Anxiety | Correlation Coefficient | 0.326 ** | 0.239 ** | 1.000 | −0.160 * | |
| Sig. (2-tailed) | 0.000 | 0.001 | . | 0.035 | ||
| N | 174 | 174 | 174 | 174 | ||
| Resilience | Correlation Coefficient | −0.101 | −0.172 * | −0.160 * | 1.000 | |
| Sig. (2-tailed) | 0.187 | 0.023 | 0.035 | . | ||
| N | 174 | 174 | 174 | 174 | ||
Run MATRIX procedure: **************** PROCESS Procedure for SPSS Version 3.5.2 **************** Written by Andrew F. Hayes, Ph.D. www.afhayes.com (accessed on 20 August 2022) Documentation available in Hayes (2018). www.guilford.com/p/hayes3 (accessed on 20 August 2022) ************************************************************************** Model : 4 Y : Alogit X : nCP1 M : RES Sample Size: 174 ************************************************************************** OUTCOME VARIABLE: RES Model Summary R R-sq MSE F df1 df2 p 0.1582 0.0250 0.5572 4.4127 1.0000 172.0000 0.0371 Model coeff se t p LLCI ULCI constant 1.5000 0.2155 6.9608 0.0000 1.0747 1.9253 nCP1 0.4691 0.2233 2.1006 0.0371 0.0283 0.9100 ************************************************************************** OUTCOME VARIABLE: Alogit Coding of binary Y for logistic regression analysis: Alogit Analysis 0.00 0.00 1.00 1.00 Model Summary -2LL ModelLL df p McFadden CoxSnell Nagelkrk 126.8091 16.4223 2.0000 0.0003 0.1147 0.0901 0.1606 Model coeff se Z p LLCI ULCI constant 1.1162 0.7776 1.4355 0.1512 −0.4078 2.6402 nCP1 −2.2378 0.6461 −3.4639 0.0005 −3.5041 −0.9716 RES −0.5161 0.3326 −1.5516 0.1208 −1.1680 0.1358 |
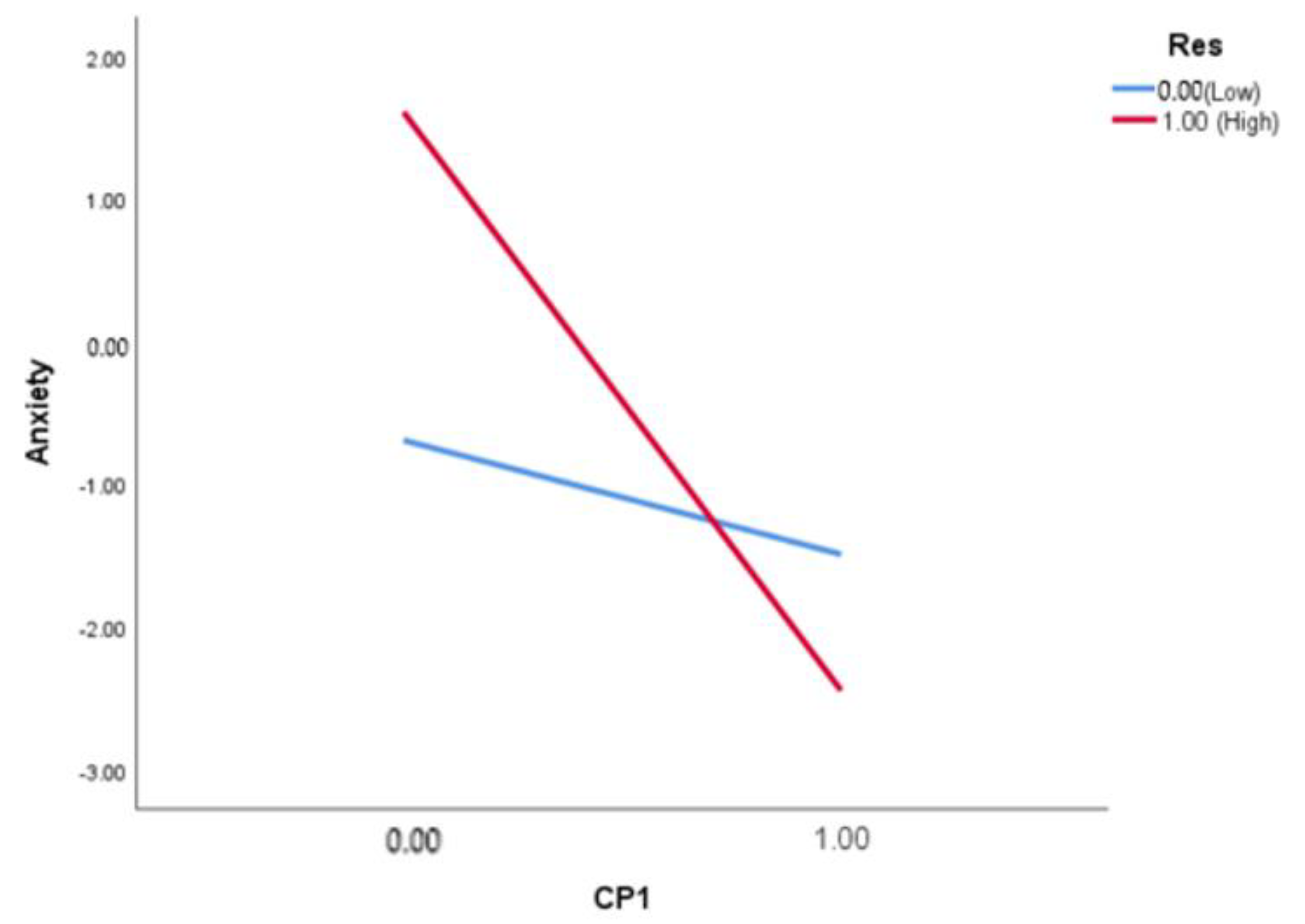
Run MATRIX procedure: **************** PROCESS Procedure for SPSS Version 3.5.2 **************** Written by Andrew F. Hayes, Ph.D. www.afhayes.com (accessed on 20 August 2022) Documentation available in Hayes (2018). www.guilford.com/p/hayes3 (accessed on 20 August 2022) ************************************************************************** Model : 1 Y : Alogit X : nCP1 W : DicotRES Sample Size: 174 ************************************************************************** OUTCOME VARIABLE: Alogit Coding of binary Y for logistic regression analysis: Alogit Analysis 0.00 0.00 1.00 1.00 Model Summary -2LL ModelLL df p McFadden CoxSnell Nagelkrk 122.5892 20.6423 3.0000 0.0001 0.1441 0.1119 0.1994 Model coeff se Z p LLCI ULCI constant −0.6931 0.8660 −0.8004 0.4235 −2.3905 1.0042 nCP1 −0.7985 0.9413 −0.8483 0.3963 −2.6435 1.0465 DicotRES 2.3026 1.3964 1.6489 0.0992 −0.4344 5.0395 Int_1 −3.2581 1.4855 −2.1932 0.0283 −6.1697 −0.3465 These results are expressed in a log-odds metric. Product terms key: Int_1 : nCP1 x DicotRES Likelihood ratio test(s) of highest order unconditional interactions(s): Chi-sq df p X*W 5.7393 1.0000 0.0166 ---------- Focal predict: nCP1 (X) Mod var: DicotRES (W) Conditional effects of the focal predictor at values of the moderator(s): DicotRES Effect se Z p LLCI ULCI 0.0000 −0.7985 0.9413 −0.8483 0.3963 −2.6435 1.0465 1.0000 −4.0566 1.1492 −3.5298 0.0004 −6.3091 −1.8042 Data for visualizing the conditional effect of the focal predictor: Paste text below into a SPSS syntax window and execute to produce plot. ------ END MATRIX ----- |
References
- Boschman, J.; Van Der Molen, H.; Sluiter, J.; Frings-Dresen, M. Psychosocial work environment and mental health among construction workers. Appl. Ergon. 2013, 44, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Haynes, N.S.; Love, P.E. Psychological adjustment and coping among construction project managers. Constr. Manag. Econ. 2004, 22, 129–140. [Google Scholar] [CrossRef]
- Cattell, K.; Bowen, P.; Edwards, P. Stress among South African construction professionals: A job demand-control-support survey. Constr. Manag. Econ. 2016, 34, 700–723. [Google Scholar] [CrossRef]
- Watson, R.; Deary, I.; Thompson, D.; Li, G. A study of stress and burnout in nursing students in Hong Kong: A questionnaire survey. Int. J. Nurs. Stud. 2008, 45, 1534–1542. [Google Scholar] [CrossRef] [PubMed]
- Hannigan, B.; Edwards, D.; Burnard, P. Stress and stress management in clinical psychology: Findings from a systematic review. J. Ment. Health 2004, 13, 235–245. [Google Scholar] [CrossRef]
- Liang, Q.; Leung, M.-Y.; Ahmed, K. How adoption of coping behaviors determines construction workers’ safety: A quantitative and qualitative investigation. Saf. Sci. 2021, 133, 105035. [Google Scholar] [CrossRef]
- Chan, A.P.C.; Nwaogu, J.M.; Naslund, J.A. Mental Ill-Health Risk Factors in the Construction Industry: Systematic Review. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- Campbell, F. Occupational Stress in the Construction Industry; Chartered Institute of Building: Berkshire, UK, 2006. [Google Scholar]
- Love PE, D.; Edwards, D.J.; Irani, Z. Work Stress, Support, and Mental Health in Construction. J. Constr. Eng. Manag. 2010, 136, 650–658. [Google Scholar] [CrossRef]
- Lingard, H.; Brown, K.; Bradley, L.; Bailey, C.; Townsend, K. Improving employees’ work-life balance in the construction industry: Project alliance case study. J. Constr. Eng. Manag. 2007, 133, 807–815. [Google Scholar] [CrossRef]
- Langdon, R.; Sawang, S. Construction Workers’ Well-Being: What Leads to Depression, Anxiety, and Stress? J. Constr. Eng. Manag. 2018, 144, 04017100. [Google Scholar] [CrossRef]
- Chen, Y.; Mccabe, B.; Hyatt, D. Relationship between Individual Resilience, Interpersonal Conflicts at Work, and Safety Outcomes of Construction Workers. J. Constr. Eng. Manag. 2017, 143, 04017042. [Google Scholar] [CrossRef]
- Kamardeen, I.; Sunindijo, R.Y. Personal Characteristics Moderate Work Stress in Construction Professionals. J. Constr. Eng. Manag. 2017, 143, 04017072. [Google Scholar] [CrossRef]
- Liang, S.-Y.; Liu, H.-C.; Lu, Y.-Y.; Wu, S.-F.; Chien, C.-H.; Tsay, S.-L. The Influence of Resilience on the Coping Strategies in Patients with Primary Brain Tumors. Asian Nurs. Res. 2020, 14, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Townsend, J.A.; Wells, M.H. 24—Behavior Guidance of the Pediatric Dental Patient. In Pediatric Dentistry (Sixth Edition); Nowak, A.J., Christensen, J.R., Mabry, T.R., Townsend, J.A., Wells, M.H., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 352–370.e352. [Google Scholar]
- Sunindijo, R.Y.; Kamardeen, I. Work Stress Is a Threat to Gender Diversity in the Construction Industry. J. Constr. Eng. Manag. 2017, 143, 04017073. [Google Scholar] [CrossRef]
- Cheung, T.; Yip, P.S. Depression, anxiety and symptoms of stress among Hong Kong nurses: A cross-sectional study. Int. J. Environ. Res. Public Health 2015, 12, 11072–11100. [Google Scholar] [CrossRef]
- Olanipekun, A.O.; Saka, N. Response of the Nigerian construction sector to economic shocks. Constr. Econ. Build. 2019, 19, 160–180. [Google Scholar] [CrossRef]
- Ibem, E.O.; Anosike, N.; Azuh, D.E.; Mosaku, T.O. Work stress among professionals in the building construction industry in Nigeria. Australas. J. Constr. Econ. Build. 2011, 11, 45–57. [Google Scholar] [CrossRef]
- Ojo, G.K.; Adeyeye, G.M.; Opawole, A.; Kajimo-Shakantu, K. Gender differences in workplace stress response strategies of quantity surveyors in Southwestern Nigeria. Int. J. Build. Pathol. Adapt. 2019, 37, 718–732. [Google Scholar] [CrossRef]
- Oladinrin, T.; Adeniyi, O.; Udi, M. Analysis of stress management among professionals in the Nigerian construction industry. Int. J. Multidiscip. Curr. Res. 2014, 2, 22–33. [Google Scholar]
- Oyewunmi, A.E.; Oyewunmi, O.A.; Iyiola, O.O.; Ojo, A.Y. Mental health and the Nigerian workplace: Fallacies, facts and the way forward. Int. J. Psychol. 2015, 7, 106–111. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Rabenu, E.; Yaniv, E. Psychological resources and strategies to cope with stress at work. Int. J. Psychol. Res. 2017, 10, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Yip, B.; Rowlinson, S. Job burnout among construction engineers working within consulting and contracting organizations. J. Manag. Eng. 2009, 25, 122–130. [Google Scholar] [CrossRef]
- Abramson, D.M.; Grattan, L.M.; Mayer, B.; Colten, C.E.; Arosemena, F.A.; Bedimo-Rung, A.; Lichtveld, M. The resilience activation framework: A conceptual model of how access to social resources promotes adaptation and rapid recovery in post-disaster settings. J. Behav. Health Serv. Res. 2015, 42, 42–57. [Google Scholar] [CrossRef]
- Wu, M.; Yang, Y.; Zhang, D.; Zhao, X.; Sun, Y.; Xie, H.; Jia, J.; Su, Y.; Li, Y. Association between social support and health-related quality of life among Chinese rural elders in nursing homes: The mediating role of resilience. Qual. Life Res. 2018, 27, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Biggs, A.; Brough, P.; Drummond, S. Lazarus and Folkman’s psychological stress and coping theory. Handb. Stress Health 2017, 349–364. [Google Scholar] [CrossRef]
- Nwaogu, J.M.; Chan AP, C.; Tetteh, M.O. Staff resilience and coping behavior as protective factors for mental health among construction tradesmen. J. Eng. Des. Technol. 2022, 20, 671–695. [Google Scholar] [CrossRef]
- Tsaras, K.; Daglas, A.; Mitsi, D.; Papathanasiou, I.V.; Tzavella, F.; Zyga, S.; Fradelos, E.C. A cross-sectional study for the impact of coping strategies on mental health disorders among psychiatric nurses. Health Psychol. Res. 2018, 6, 7466. [Google Scholar] [CrossRef]
- Enshassi, A.; Al-Swaity, E.; Abdul Aziz Abdul, R.; Choudhry, R. Coping behaviors to deal with stress and stressor consequences among construction professionals: A case study at the Gaza Strip, Palestine. J. Financ. Manag. Prop. Constr. 2018, 23, 40–56. [Google Scholar] [CrossRef]
- Thompson, N.J.; Fiorillo, D.; Rothbaum, B.O.; Ressler, K.J.; Michopoulos, V. Coping strategies as mediators in relation to resilience and posttraumatic stress disorder. J. Affect. Disord. 2018, 225, 153–159. [Google Scholar] [CrossRef]
- Wu, Y.; Yu, W.; Wu, X.; Wan, H.; Wang, Y.; Lu, G. Psychological resilience and positive coping styles among Chinese undergraduate students: A cross-sectional study. BMC Psychol. 2020, 8, 79. [Google Scholar] [CrossRef]
- Kimhi, S. Levels of resilience: Associations among individual, community, and national resilience. J. Health Psychol. 2014, 21, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M.; Saklofske, D.H.; Keefer, K.V.; Tremblay, P.F. Coping Strategies and Psychological Outcomes: The Moderating Effects of Personal Resiliency. J. Psychol. 2016, 150, 318–332. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Zhou, Y.; Wang, S.; Luo, T.; Huang, M.; Zeng, Y. Exploratory study on resilience and its influencing factors among hospital nurses in Guangzhou, China. Int. J. Nurs. Sci. 2018, 5, 57–62. [Google Scholar] [CrossRef]
- Chen, Y.; Mccabe, B.; Hyatt, D. Impact of individual resilience and safety climate on safety performance and psychological stress of construction workers: A case study of the Ontario construction industry. J. Saf. Res. 2017, 61, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Matos, P.S.; Neushotz, L.A.; Griffin MT, Q.; Fitzpatrick, J.J. An exploratory study of resilience and job satisfaction among psychiatric nurses working in inpatient units. Int. J. Ment. Health Nurs. 2010, 19, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Youssef, C.M.; Luthans, F. Positive organizational behavior in the workplace: The impact of hope, optimism, and resilience. J. Manag. 2007, 33, 774–800. [Google Scholar] [CrossRef]
- Gloria, C.T.; Steinhardt, M.A. Relationships among positive emotions, coping, resilience and mental health. Stress Health 2016, 32, 145–156. [Google Scholar] [CrossRef]
- Li, W.W.; Miller, D.J. The impact of coping and resilience on anxiety among older Australians. Aust. J. Psychol. 2017, 69, 263–272. [Google Scholar] [CrossRef]
- Chen, H.; Xu, J.; Mao, Y.; Sun, L.; Sun, Y.; Zhou, Y. Positive Coping and Resilience as Mediators between Negative Symptoms and Disability Among Patients with Schizophrenia. Front. Psychiatry 2019, 10, 641. [Google Scholar] [CrossRef]
- Nwaogu, J.M. An Integrated Approach to Improve Mental Health Among Construction Personnel in Nigeria. Ph.D. Thesis, The Hong Kong Polytechnic University, Hong Kong, China, 2021. [Google Scholar]
- Leung, M.Y.; Liu, A.M.; Wong, M.M.K. Impact of stress-coping behaviour on estimation performance. Constr. Manag. Econ. 2006, 24, 55–67. [Google Scholar] [CrossRef]
- Chan, I.; Leung, M.-Y.; Liang, Q. The roles of motivation and coping behaviours in managing stress: Qualitative interview study of Hong Kong expatriate construction professionals in mainland China. Int. J. Environ. Res. Public Health 2018, 15, 561. [Google Scholar] [CrossRef] [PubMed]
- Palaniappan, K.; Rajaraman, N.; Ghosh, S. Effectiveness of peer support to reduce depression, anxiety and stress among migrant construction workers in Singapore. Eng. Constr. Archit. Manag. 2022. [Google Scholar] [CrossRef]
- Secades, X.G.; Molinero, O.; Salguero, A.; Barqu, N.R.R.; De La Vega, R.; Rquez, S.M. Relationship between resilience and coping strategies in competitive sport. Percept. Mot. Ski. 2016, 122, 336–349. [Google Scholar] [CrossRef] [PubMed]
- De La Fuente, J.; Fern Ndez-Cabezas, M.; Cambil, M.; Vera, M.M.; Gonz Lez-Torres, M.C.; Artuch-Garde, R. Linear Relationship between Resilience, Learning Approaches, and Coping Strategies to Predict Achievement in Undergraduate Students. Front. Psychol. 2017, 8, 1039. [Google Scholar] [CrossRef] [PubMed]
- Adewuya, A.O.; Atilola, O.; Ola, B.A.; Coker, O.A.; Zachariah, M.P.; Olugbile, O.; Fasawe, A.; Idris, O. Current prevalence, comorbidity and associated factors for symptoms of depression and generalised anxiety in the Lagos State Mental Health Survey (LSMHS), Nigeria. Compr. Psychiatry 2018, 81, 60–65. [Google Scholar] [CrossRef]
- Obadeji, A.; Oluwole, L.O.; Dada, M.U.; Ajiboye, A.S.; Kumolalo, B.F.; Solomon, O.A. Assessment of depression in a primary care setting in Nigeria using the PHQ-9. J. Fam. Med. Prim. Care 2015, 4, 30. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Ola, B.A.; Afolabi, O.O. Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J. Affect. Disord. 2006, 96, 89–93. [Google Scholar] [CrossRef]
- Folayan, M.O.; Harrison, A.; Brown, B.; Odetoyinbo, M.; Stockman, J.K.; Ajuwon, A.J.; Caceres, C.F. Associations between forced sexual initiation, HIV status, sexual risk behavior, life stressors, and coping strategies among adolescents in Nigeria. PLoS ONE 2016, 11, e0155210. [Google Scholar] [CrossRef]
- Arroll, B.; Goodyear-Smith, F.; Crengle, S.; Gunn, J.; Kerse, N.; Fishman, T.; Falloon, K.; Hatcher, S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann. Fam. Med. 2010, 8, 348–353. [Google Scholar] [CrossRef]
- Tomitaka, S.; Kawasaki, Y.; Ide, K.; Akutagawa, M.; Yamada, H.; Ono, Y.; Furukawa, T.A. Distributional patterns of item responses and total scores on the PHQ-9 in the general population: Data from the National Health and Nutrition Examination Survey. BMC Psychiatry 2018, 18, 108. [Google Scholar] [CrossRef]
- Li, H.; Luo, X.; Ke, X.; Dai, Q.; Zheng, W.; Zhang, C.; Cassidy, R.M.; Soares, J.C.; Zhang, X.; Ning, Y. Major depressive disorder and suicide risk among adult outpatients at several general hospitals in a Chinese Han population. PLoS ONE 2017, 12, e0186143. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef] [PubMed]
- Fils, J.M.; Penick, E.C.; Nickel, E.J.; Othmer, E.; Desouza, C.; Gabrielli, W.F.; Hunter, E.E. Minor versus major depression: A comparative clinical study. Prim. Care Companion J. Clin. Psychiatry 2010, 12, 27496. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hughes, A.J.; Dunn, K.M.; Chaffee, T.; Bhattarai, J.J.; Beier, M. Diagnostic and Clinical Utility of the GAD-2 for Screening Anxiety Symptoms in Individuals with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2018, 99, 2045–2049. [Google Scholar] [CrossRef] [PubMed]
- Rodr Guez-Rey, R.; Alonso-Tapia, J.; Hernansaiz-Garrido, H. Reliability and validity of the Brief Resilience Scale (BRS) Spanish Version. Psychol. Assess. 2016, 28, e101. [Google Scholar] [CrossRef]
- Smith, B.W.; Epstein, E.M.; Ortiz, J.A.; Christopher, P.J.; Tooley, E.M. The Foundations of Resilience: What Are the Critical Resources for Bouncing Back from Stress? In Resilience in Children, Adolescents, and Adults: Translating Research into Practice; Prince-Embury, S., Saklofske, D.H., Eds.; Springer: New York, NY, USA, 2013; pp. 167–187. [Google Scholar]
- Liang, Q.; Leung, M.-Y.; Cooper, C. Focus group study to explore critical factors for managing stress of construction workers. J. Constr. Eng. Manag. 2018, 144, 04018023. [Google Scholar] [CrossRef]
- Chan YS, I.; Leung, M.-Y.; Yuan, T. Structural relationships between cultural values and coping behaviors of professionals in the stressful construction industry. Eng. Constr. Archit. Manag. 2014, 21, 133–151. [Google Scholar] [CrossRef]
- Scherer, R.F.; Brodzinski, J.D. An Analysis of the Ways of Coping Questionnaire. Manag. Commun. Q. 1990, 3, 401–418. [Google Scholar] [CrossRef]
- Cochran, W.G. Sampling Techniques; John Wiley & Sons: Hoboken, NJ, USA, 1977. [Google Scholar]
- Kroonenberg, P.M.; Verbeek, A. The Tale of Cochran’s Rule: My Contingency Table has so Many Expected Values Smaller than 5, What Am I to Do? Am. Stat. 2018, 72, 175–183. [Google Scholar] [CrossRef]
- Park, H. An introduction to logistic regression: From basic concepts to interpretation with particular attention to nursing domain. J. Korean Acad. Nurs. 2013, 43, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Szumilas, M. Explaining odds ratios. J. Can. Acad. Child Adolesc. Psychiatry 2010, 19, 227. [Google Scholar]
- Hayes, A.F.; Rockwood, N.J. Conditional Process Analysis: Concepts, Computation, and Advances in the Modeling of the Contingencies of Mechanisms. Am. Behav. Sci. 2019, 64, 19–54. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, Second Edition: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Folkman, S.; Lazarus, R.S.; Dunkel-Schetter, C.; Delongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Personal. Soc. Psychol. 1986, 50, 992. [Google Scholar] [CrossRef] [PubMed]
- Aitken, A.; Crawford, L. Coping with stress: Dispositional coping strategies of project managers. Int. J. Proj. Manag. 2007, 25, 666–673. [Google Scholar] [CrossRef]
- Nakamura, Y.M.; Orth, U. Acceptance as a coping reaction: Adaptive or not? Swiss J. Psychol./Schweiz. Z. Psychol./Rev. Suisse Psychol. 2005, 64, 281–292. [Google Scholar] [CrossRef]
- Yikealo, D.; Tareke, W. Stress Coping Strategies among College Students: A Case in the College of Education, Eritrea Institute of Technology. Open Sci. J. 2018, 3, 1–17. [Google Scholar] [CrossRef]
- Miyata, A.; Arai, H.; Suga, S. Nurse managers stress and coping. Open J. Nurs. 2015, 5, 957. [Google Scholar] [CrossRef]
- Fatima, H.; Oyetunji, T.P.; Mishra, S.; Sinha, K.; Olorunsogbon, O.F.; Akande, O.S.; Srinivasan; Kar, S.K. Religious coping in the time of COVID-19 Pandemic in India and Nigeria: Finding of a cross-national community survey. Int. J. Soc. Psychiatry 2022, 68, 309–315. [Google Scholar] [CrossRef]




| Variable | Categories | Frequency (%) | Mean (SD) |
|---|---|---|---|
| Demographics Characteristics | |||
| Sex | Male | 158 (90.8) | |
| Female | 16 (9.2) | ||
| Type of firm | Micro | 37 (21.3) | |
| Small | 59 (33.9) | ||
| Medium | 46 (26.4) | ||
| Large | 32 (18.4) | ||
| Years of Experience | 1–5 years | 46 (26.4) | |
| 6–10 years | 66 (37.9) | ||
| 11–15 years | 41 (23.6) | ||
| 16–20 years | 10 (5.7) | ||
| 21–25 years | 4 (2.3) | ||
| over 25 years | 7 (4.0) | ||
| Position | Project Manager | 62 (35.6) | |
| Site Engineer/Supervisor | 73 (41.9) | ||
| Asst. Site Engineer/Supervisor | 39 (22.4) | ||
| Education | HND | 43 (24.7) | |
| PGD | 19 (10.9) | ||
| BSc./B.Tech. | 67 (38.5) | ||
| MSc./M. Tech. | 45 (25.9) | ||
| Professional Affiliation | |||
| NIOB | 93 (53.4) | ||
| NICE | 74 (42.5) | ||
| NIQS | 5 (2.9) | ||
| NIA | 2 (1.1) | ||
| Mental ill-health symptoms | |||
| Depression (0, 17) | 5.33 (3.80) | ||
| None-Minimal (0–4) | 79 (45.4) | ||
| Mild (5–9) | 65 (37.4) | ||
| Moderate (10–14) | 27 (15.5) | ||
| Moderately severe (15–19) | 3 (1.7) | ||
| Suicide ideation | 16 (9.2) | ||
| Anxiety (0, 6) | 1.20 (1.39) | ||
| None-minimal (0–2) | 149 (85.6) | ||
| Mild-moderate (≥3) | 25 (14.4) | ||
| Resilience | Low resilience (≥2.99) | 55 (31.6) | |
| Normal resilience (3.00–4.30) | 75 (43.1) | ||
| High resilience (4.31–5.00) | 44 (25.3) | ||
| Depression | No Depression | χ2 or F | p | COR | Anxiety | No Anxiety | χ2 or F | p | COR | Resilience | No Resilience | χ2 or F | p | COR | |
| Personnel (n = 174) | 95 (55.1) | 79 (44.9) | 25 (14.8) | 149 (85.2) | 119 (68.4) | 55 (31.6) | |||||||||
| Gender | 2.08 | 0.19 | 1.62 | 0.25 | 1.35 | 0.28 | |||||||||
| Male (n = 158) | 89 (56.3) | 69 (43.7) | 21 (13.3) | 137 (86.7) | 106 (67.1) | 52 (32.9) | |||||||||
| Female (n = 16) | 6 (37.5) | 10 (62.5) | 4 (25.0) | 12 (75.0) | 13 (81.3) | 3 (18.8) | |||||||||
| Years of experience | 2.54 F | 0.79 | 7.03 F | 0.16 | 5.81 F | 0.31 | |||||||||
| 1–5 year (n = 46) | 24 (52.2) | 22 (47.8) | 4 (8.7) | 42 (91.3) | 35 (76.1) | 11 (23.9) | |||||||||
| 6–10 year (n = 66) | 38 (57.6) | 28 (41.8) | 11 (16.7) | 55 (83.3) | 42 (63.6) | 24 (36.4) | |||||||||
| 11–15 year (n = 41) | 24 (58.5) | 17 (41.5) | 7 (17.1) | 34 (82.9) | 27 (65.9) | 14 (34.1) | |||||||||
| 16–20 year (n =10) | 5 (50.0) | 5 (50.0) | - | 10 (100) | 5 (50.0) | 5 (50.0) | |||||||||
| 21–25 year (n = 4) | 1 (25.0) | 3 (75.0) | - | 4 (100.0) | 4 (100) | - | |||||||||
| >25 year (n = 7) | 3 (42.9) | 4 (57.1) | 3 (42.9) | 4 (57.1) | 6 (85.7) | 1 (14.3) | |||||||||
| Suicidal Ideation | 10.90 | 0.00 | 0.30 a | 18.18 | 0.00 | 0.33 a | 1.20 | 0.40 | −0.10 | ||||||
| No (n = 158) | 80 (50.6) | 78 (49.4) | 17 (10.8) | 141 (89.2) | 110 (69.6) | 48 (30.4) | |||||||||
| Yes (n = 16) | 15 (93.8) | 1 (6.3) | 8 (50.0) | 8 (50.0) | 9 (56.3) | 7 (43.8) |
| Code | Suicidal Ideation | Depression | Anxiety | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | ||
| R | Resilience | |||||||||
| Low resilience | - | - | - | - | - | - | ||||
| Normal resilience | 0.54 | 0.71 | 0.23–2.14 | 0.51 | 0.79 | 0.39–1.60 | 0.56 | 0.76 | 0.31–1.88 | |
| High resilience | 0.18 | 0.33 | 0.64–1.66 | 0.66 | 0.47 | 0.21–1.05 | 0.03 | 0.19 | 0.04–0.91 | |
| MIL | Mental ill-health symptoms | |||||||||
| Depression | 0.01 | 14.63 | 1.89–113.39 | |||||||
| Anxiety | 0.00 | 8.29 | 2.76–24.96 | |||||||
| Code | Coping Strategies | Descriptive Statistics | Univariate Logistic Regression | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Depression | Anxiety | ||||||||
| Mean | R | p | OR | 95% CI | p | OR | 95% CI | ||
| Problem-focused coping | |||||||||
| Planful problem-solving (α = 0.76) | |||||||||
| C1 | Knew what had to be done, so I doubled my efforts to make the thing work | 3.11 | 8 | 0.74 | 1.22 | 0.38–3.94 | 0.00 | 0.09 | 0.03–0.31 |
| C2 | Came out with a couple of different solutions to the problem | 3.22 | 5 | 0.99 | - | - | 0.99 | 0.00 | - |
| C3 | Made a plan of action and followed it | 3.14 | 7 | 0.79 | 1.21 | 0.29–5.02 | 0.39 | 0.48 | 0.09–2.54 |
| Positive reappraisal (α = 0.71) | |||||||||
| C4 | Came out of the experience better than when I went in | 3.28 | 4 | 0.53 | 1.54 | 0.40–5.93 | 0.78 | 1.36 | 0.16–11.38 |
| C5 | Changed or grew as a person in a good way | 3.28 | 3 | 0.68 | 0.60 | 0.53–6.70 | 0.37 | 0.33 | 0.03–3.74 |
| C6 | Rediscovered what is important in life | 3.29 | 2 | 0.51 | 1.84 | 0.30–11.27 | 0.13 | 0.24 | 0.04–1.49 |
| C7 | Found a new faith | 2.57 | 18 | 0.80 | 1.09 | 0.56–2.11 | 0.15 | 2.27 | 0.74–7.00 |
| C8 | Prayed to withstand or succeed | 3.35 | 1 | 0.99 | 1.00 | 0.29–3.42 | 0.00 | 0.17 | 0.05–0.60 |
| Seeking social support (α = 0.78) | |||||||||
| C9 | Talk to someone who could do something concrete about the problem | 2.83 | 13 | 0.79 | 0.85 | 0.26–2.79 | 0.29 | 0.47 | 0.12–1.88 |
| C10 | Talk to someone to find out more about the situation | 2.77 | 14 | 0.07 | 0.79 | 0.85–5.31 | 0.04 | 0.29 | 0.09–0.93 |
| C11 | Talk to someone about how I was feeling | 2.62 | 16 | 0.16 | 2.15 | 0.75–6.20 | 0.35 | 2.69 | 0.34–21.30 |
| Confrontive coping (α = 0.69) | |||||||||
| C12 | Expressed anger toward the person who caused the problem | 2.05 | 22 | 0.26 | 1.45 | 0.75–2.79 | 0.49 | 1.41 | 0.53–3.77 |
| C13 | Tried to get the person responsible to change his or her mind | 2.59 | 17 | 0.36 | 1.50 | 0.63–3.57 | 0.16 | 4.38 | 0.56–34.00 |
| Emotion-focused coping | |||||||||
| Accept responsibility (α = 0.72) | |||||||||
| C14 | Realised I had brought the problem on myself | 2.11 | 21 | 0.02 | 2.28 | 1.17–4.41 | 0.47 | 0.72 | 0.30–1.76 |
| C15 | Criticised or lectured myself | 2.84 | 11 | 0.66 | 1.23 | 0.49–3.13 | 0.23 | 3.51 | 0.45–27.45 |
| C16 | I made a promise to myself that things would be different next time | 3.16 | 6 | 0.99 | 0.00 | 0.00 | 0.72 | 0.66 | 0.07–6.18 |
| Escape-Avoidance (α = 0.75) | |||||||||
| C17 | Wished that the situation would go away or somehow be over | 2.99 | 9 | 0.99 | 0.29 | 1.03–3.48 | 0.99 | - | - |
| C18 | I had fantasies about how things might turn out | 2.83 | 12 | 0.25 | 1.76 | 0.67–4.62 | 0.99 | - | - |
| C20 | Tried to lose myself for a while by smoking | 1.39 | 25 | 0.67 | 0.85 | 0.41–1.79 | 0.12 | 2.13 | 0.83–5.43 |
| C21 | Used alcohol to make myself feel better | 1.35 | 26 | 0.18 | 1.66 | 0.79–3.46 | 0.22 | 1.79 | 0.71–4.53 |
| C22 | Tried to make myself feel better by eating | 2.01 | 23 | 0.08 | 1.73 | 0.94–3.20 | 0.01 | 4.06 | 1.33–12.42 |
| C23 | Let my feelings out, like crying or venting my emotions | 1.76 | 24 | 0.00 | 2.69 | 1.44–4.99 | 0.83 | 0.91 | 0.39–2.14 |
| Self-controlling | |||||||||
| C19 | Kept others from knowing how bad things were | 2.43 | 20 | 0.25 | 1.59 | 0.73–3.46 | 0.80 | 1.16 | 0.37–3.66 |
| Distancing (α = 0.73) | |||||||||
| C24 | Didn’t let it get to me and refused to think about it too much | 2.52 | 19 | 0.61 | 1.24 | 0.54–2.86 | 0.99 | - | - |
| C25 | Went on as if nothing had happened | 2.75 | 15 | 0.99 | 1.00 | 0.41–2.46 | 0.19 | 3.94 | 0.51–30.68 |
| C26 | Made light of the situation and refused to get too serious about it | 2.87 | 10 | 0.96 | 1.03 | 0.33–3.21 | 0.91 | 0.92 | 0.19–4.41 |
| Code | Coping Skills | Frequency | Percentage |
|---|---|---|---|
| Problem-Focused Coping | |||
| Planful problem-solving | |||
| C3 | Made a plan of action and followed it | 5 | 38.46 |
| C2 | Came out with a different solution to the problem | 2 | 15.38 |
| Positive reappraisal | |||
| C8 | Prayed to withstand or succeed | 8 | 61.54 |
| C7 | Explore other faith | 3 | 23.08 |
| Seeking social support | |||
| C11 | Speak to someone about the problem | 11 | 84.62 |
| Confrontive coping | |||
| C12 | Expressed anger toward the person who caused the problem | 3 | 23.08 |
| Stress-reducing activity | |||
| NC1 | Take some rest | 4 | 30.77 |
| Emotion-focused coping | |||
| Accept responsibility | |||
| C16 | I made a promise to myself that things would be different next | 1 | 7.69 |
| Escape-Avoidance | |||
| C22 | Tried to make myself feel better by eating | 3 | 23.08 |
| NC2 | Transfer aggression to my family (i.e., took it out on other people) | 1 | 7.69 |
| Documents with code(s) | 13 | 100.00 | |
| Documents without code(s) | 0 | 0.00 | |
| Analysed documents | 13 | 100.00 | |
| Resilience | Emotion-Focused | Problem-Focused | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Escape-Avoidance | Planful Problem-Solving | Positive Reappraisal | |||||||
| p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | |
| Low * | |||||||||
| High | 0.047 | 0.46 | 0.22, 0.99 | 0.01 | 17.21 | 2.06, 143.6 | 0.01 | 20.09 | 2.44, 165.0 |
| Overall model | |||||||||
| R → CP | R2 = 0.035, 2 LI = 170.835 | R2 = 0.204, 2 LI = 53.478 | R2 = 0.226, 2 LI = 57.172 | ||||||
| CP → R | R2 = 0.031, 2 LI = 213.255 | R2 = 0.089, 2 LI = 205.691 | R2 = 0.106, 2 LI = 203.446 | ||||||
| Model summary | ||||||
| −2 LL | ModelLL | df | p | McFadden | CoxSnell | Nagelkrk |
| 122.5892 | 20.6423 | 3.0000 | 0.0001 | 0.1441 | 0.1119 | 0.1994 |
| Coeff | se | z | p | LLCI | UPCI | |
| Constant | −0.693 | 0.866 | −0.800 | 0.424 | −2.391 | 1.004 |
| CP1 | −0.799 | 0.941 | −0.848 | 0.396 | −2.644 | 1.047 |
| Res | 2.303 | 1.396 | 1.649 | 0.099 | −0.434 | 5.040 |
| Int_1 | −3.258 | 1.486 | −2.193 | 0.028 | −6.170 | −0.347 |
| Likelihood ratio test(s) of highest order unconditional interactions(s): | ||||||
| Chi-sq | df | p | ||||
| X*W | 5.7393 | 1.0000 | 0.0166 | |||
| Conditional effects of the focal predictor at values of the moderator(s): | ||||||
| Res | Effect | se | Z | p | LLCI | ULCI |
| 0.0000 | −0.7985 | 0.9413 | −0.8483 | 0.3963 | −2.6435 | 1.0465 |
| 1.0000 | −4.0566 | 1.1492 | −3.5298 | 0.0004 | −6.3091 | −1.8042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nwaogu, J.M.; Chan, A.P.C. The Impact of Coping Strategies and Individual Resilience on Anxiety and Depression among Construction Supervisors. Buildings 2022, 12, 2148. https://doi.org/10.3390/buildings12122148
Nwaogu JM, Chan APC. The Impact of Coping Strategies and Individual Resilience on Anxiety and Depression among Construction Supervisors. Buildings. 2022; 12(12):2148. https://doi.org/10.3390/buildings12122148
Chicago/Turabian StyleNwaogu, Janet M., and Albert P. C. Chan. 2022. "The Impact of Coping Strategies and Individual Resilience on Anxiety and Depression among Construction Supervisors" Buildings 12, no. 12: 2148. https://doi.org/10.3390/buildings12122148
APA StyleNwaogu, J. M., & Chan, A. P. C. (2022). The Impact of Coping Strategies and Individual Resilience on Anxiety and Depression among Construction Supervisors. Buildings, 12(12), 2148. https://doi.org/10.3390/buildings12122148