Orbital blowout fractures (OBF) are among the most com- mon facial traumas requiring surgical intervention.[
1,
2,
3,
4] They are a frequent source of admission to trauma centers due to the increasing incidence of motor vehicle accidents and physical assault.[
5] There is ample investigation into the optimal timing and approach to OBF repair; however, much less attention has been directed toward the details of postoperative care. Isolated OBF repair may be performed as an outpatient surgery; however, some subspecialists still prefer overnight hospital admission following isolated OBF repair to monitor for retrobulbar hemorrhage (RBH).[
3,
6] While RBH is the most devastating potential sequelae after OBF repair, it is a rare complication with an incidence of 0 to 3.2%.[
3,
7,
8,
9] In addition, cases of delayed postoperative RBH occurring multiple days after surgery, beyond the overnight monitoring period, have been reported.[
6,
10,
11,
12] Therefore, it is important to consider whether overnight admission after isolated OBF repair is a necessary component of postopera- tive care and an appropriate use of healthcare resources.
Outpatient isolated OBF repair is an alternative to inpatient repair. Rather than admissionfor 23-hour observation, patients are examined 2 to 4 hours postoperatively to ensure that there are no exam findings concerning for orbital compartment syndrome due to RBH, such as loss of vision, significant restriction of eye movements, eye pain, or resistance to retro- pulsion. In a recent study by Shew and colleagues, a survey of AO North America Craniomaxillofacial faculty revealed that out of 105 craniomaxillofacial surgeons, 29% send patients home on the same dayof surgery. Outpatient management was significantly more common among those who performed 20 or more OBF repairs annually.[
13] Other authors have also argued in support ofoutpatient repair, although this is not yet considered standard of care in all settings.[
3,
14]
The rate of orbital fractures, and therefore the associated cost of surgical management, is on the rise.[
2,
7] It is thus becoming increasingly important to identify cost-saving opportunities within current practice patterns that do not sacrifice quality or safety of patient care. Koo and colleagues recently demonstrated that posttraumatic orbital recon- struction performed at a dedicated eye trauma center was associated with lower overall costs compared with orbital reconstruction performed at an academic hospital. They hypothesize that higher volume and specialization at the eye trauma center resulted in increased efficiency compared with academic centers.[
15] However, among oculoplastic sur- geons or other subspecialists who commonly manage OBF at academic centers, including otolaryngology, oral-maxillofa- cial surgery, and plastic surgery, postoperative management following isolated OBF repair is another factor that may be optimized for reducing the burden on both the patient and healthcare system. This is especially pertinent when hospital admission for polytrauma is not necessary.
To our knowledge, there are few studies evaluating the safety of inpatient versus outpatient isolated OBF repair and no studies comparing the associated costs. Both are key elements that should be more carefully examined considering the need for heightened cost and resource conscientiousness within medicine. The first aim of this multicenter, retrospective study is to compare the safety of inpatient versus outpatient repair of isolated OBFs, in terms of RBH recognition and feasibility of timely intervention. The secondary aim is to evaluate the cost of inpatient versus outpatient repair using unadjusted hospital charges. Lastly, we specifically consider the utility of an auto- matic postoperative computed tomographic (CT) scan of the orbits, which is often treated as a “fixed cost” associated with the procedure.
We hypothesize that outpatient management of isolated OBFs, which includes a delayed postoperative exam prior to discharge, will not preclude the recognition and appropriate treatment of RBH. We expect considerable reduction in estimates of costs associated with outpatient OBF repair compared with an inpatient approach. Finally, we predict that an automatic or reflexive CT scan following isolated OBF repair can be considered an added healthcare cost that does not impact patients’ postoperative care in cases that lack an associated change in clinical exam.
Methods
Study Design and Patient Characteristics
A multicenter IRB-approved retrospective review of electronic medical records of orbital fracture patients, based on Current Procedural Terminology (CPT) codes 21385–7, 21390, 21401, and 21406–8 presenting to our study sites (University of Maryland Medical Center, Baltimore, MD, University of Mary- land Midtown Hospital, Baltimore, MD and University of California San Francisco Medical Center, San Francisco, CA) between November 2008 and August 2016 was performed. Patients with isolated OBF were included in the study. Patients who were younger than 18 years, who had suffered poly- trauma in addition to an OBF or had incurred other associated intraocular trauma (e.g., retinal detachment, globe rupture, hyphema) were excluded from our study.
Outcomes
Demographic, medical, and surgical information was gath- ered from the electronic medical records, including age, date of injury, mechanism of injury, involved orbital wall(s), use of oral anticoagulants, and number of days to repair. Preopera- tive data were collected including visual acuity (VA), motility, presence of gross globe displacement (enophthalmos, hypo- globus, etc.), and the presence of diplopia. The same para- meters were recorded from the postoperative examination. Completion of a postoperative CT scan of the orbits without contrast was recorded, as well as inpatient versus outpatient status of the surgery. Lastly, the need for reoperation and associated indication was documented.
Information regarding costs at our institution associated with inpatient and outpatient surgical repair of isolated OBFs including the surgeon’s fee, facility fee, anesthesia fee, cost of admission for one night, and cost of a postoperative CT scan of the orbits without contrast were obtained by referring to publicly available cost estimates from the Department of Human Resources of our local community hospital and study site, at the University of Maryland Midtown Hospital. The purpose of obtaining these data was to provide a represen- tative example of inpatient versus outpatient costs rather than a formal cost analysis.
Lastly, postoperative orbital CT scans of patients within the defined cohort were reviewed. Indication for obtaining a CT scan, other than reflexive postoperative imaging, was recorded. Cases in which postoperative CT imaging altered the course of patient management were identified including details of the patient’s postoperative course.
Statistical Analysis
Patient characteristics among the inpatient and outpatient cohorts were compared using an analysis of variance for the continuous variables, including age and time to OBF repair. Chi-square analysis was used to evaluate the categorical variables, including gender, mechanism of injury, preopera- tive characteristics, and postoperative characteristics. For the inpatient and outpatient settings, unadjusted hospital charges were calculated. Statistical significance in this study is reported as p < 0.005. Data analysis was performed using GraphPad Prism software version 6.05 (La Jolla, CA).
Results
Baseline Characteristics and Safety Outcomes
Using the previously listed CPT codes, 264 cases of OBF treated at our study sites between November 2008 and August 2016 were identified. Of these, therewere 126 patients with isolated OBFs who met our inclusion criteria. Just less than half of our cohort had isolated OBF repaired on an outpatient basis (
n = 53, 42.1%), while the remaining 73 (57.9%) were admitted for overnight monitoring after surgery. Gender and age dis- tribution was comparable between the two groups. Blunt trauma, including assault, was the most common mechanism of injury in both the inpatient (
n = 39; 53%) and outpatient (
n = 29; 54%) cohorts accounting for over half of cases in each group. Motor vehicle accident, fall, and unknown were the remaining causes of injury (
Table 1).
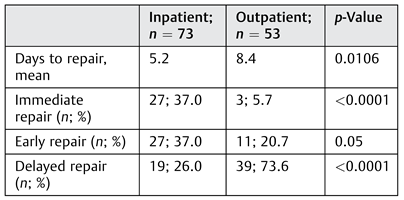
Time elapsed prior to repair differed between the two groups at a mean of 8.4 days versus 5.2 days for outpatient and inpatient cohorts, respectively (
p = 0.01). Repair was considered “immediate” if performed within 1 day of injury, “early” if within 2 weeks of injury, and “delayed” if greater than 2 weeks out from injury. A majority of the inpatient cases underwent immediate repair (
n = 27, 37.0%) compared with only 5.7% of outpatient cases (
n = 3;
p ≤ 0.0001). A majority of outpatient repairs were delayed (
n = 39, 73.6%). This is in contrast to only 26.0% (
n = 19) of inpatient cases that under- went delayed repair (
p ≤ 0.0001); 37.0% (
n = 27) of inpatient cases and 20.7% (
n = 11) of outpatient cases were early repairs (
p = 0.05) (
Table 2).
The inpatient and outpatient groups also differed signifi- cantly in terms of preoperative characteristics. Motility restriction was documented in 26.0% (
n = 19) of the inpa- tient cohort compared with 77.3% (41) of outpatient cases (
p ≤ 0.0001). Preoperative diplopia was present in a majority of outpatient cases (77.3%,
n = 41) compared with 30.1% (
n = 22) of inpatient cases (
p ≤ 0.0001). Enophthalmos was noted in about half (50.9%,
n = 27) of outpatient cases and only 17.8% (
n = 13) of inpatient cases (
p ≤ 0.0001;
Table 3). In almost half of inpatient cases (
n = 32; 44%), the sole documented indication for isolated OBF repair was fracture size greater than 50% of the floor.
Postoperative Complications
In the entire study population, there were two cases of RBH resulting in a rate of 1.6%. Both cases occurred within the outpatient cohort and neither patient was taking anticoa- gulation medication. The first patient with RBH developed decreased VA, diplopia, and eye pain 3 hours following surgery while being monitored in the postoperative anesthe- sia care unit (PACU). He was promptly taken to the operating room (OR) for hematoma evacuation. Discharge was com- pleted the following morning. The second patient presented to the emergency department 2 days after surgery with eye pain and periorbital swelling. VA was normal but intraocular pressure (IOP) was elevated. An emergent CT scan confirmed RBH, which necessitated return to the OR. Following hema- toma evacuation, both patients were admitted for overnight monitoring and then discharged the next morning. At the following postoperative clinic visit, VA was at baseline for both patients and no additional complications were noted.
There were four inpatient cases (5.4%) requiring reopera- tion during the 24-hour postoperative period. One patient experienced acute and unexplained loss of vision at the immediate postoperative evaluation and was taken back to the OR for implant removal. In two cases, revision was performed due to concerns for poor implant positioning based on immediate, reflexive postoperative CT imaging alone. There was not a documented change in clinical exam (e.g., eye pain, increased IOP, restricted motility) in either case. In the fourth case, the patient had been admitted overnight due to intractable postoperative pain, which per- sisted into the morning prompting repeat imaging. CT was concerning for possible muscle impingement; therefore, reoperation was performed for implant repositioning.
Cost Analysis
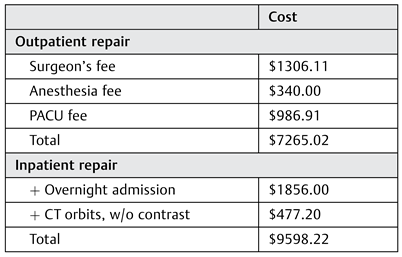
Hospital charges to the patient’s insurance for key compo- nents of an inpatient versus outpatient isolated OBF repair were obtained from the billing department at our local community hospital and study site, the University of Mary- land Midtown Hospital, and are as follows: average sur- geon’s fee for OBF,
$1306.11; OR fee,
$4632; anesthesia fee,
$340; PACU fee,
$986.91; overnight admission,
$1856; and a CT scan of the orbits without contrast,
$477.20. Costs associated with procedure-specific supplies or medications were not included in this analysis. These estimates amount to a total cost of
$9,598.22 for inpatient management,
$7,742.22 for outpatient management, and
$7,265.02 for outpatient management without reflexive postoperative imaging (
Table 4). This amounts to a difference of
$1,856.00 and
$2,333.20 with and without postoperative imaging, respectively. A formal cost analysis with adjust- ments for patient factors, such as demographics and comor- bidities, was not included, given that this calculation was meant to be a representative comparison.
CT Imaging
Out of the inpatient cohort, 76.7% (n = 56) of patients received an automatic, reflexive postoperative CT scan. Within this group, two patients (3.6%) were taken back to the OR for revision based on CT appearance of the implant alone. Of note, neither patient had a documented concomi- tant change in clinical status.
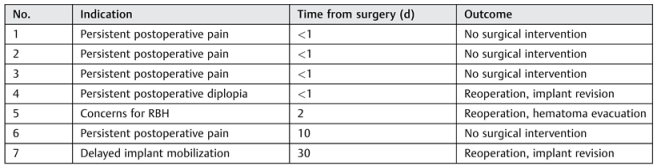
Conversely, in the outpatient group, no patients received a reflexive postoperative CT scan following surgery. Delayed postoperative imaging was obtained in seven cases (13.2%) due to a concerning change in clinical exam, almost half of which (
n = 3; 42.8%) led to reoperation. In four cases, repeat imaging was obtained for persistent postoperative pain. One case of enophthalmos due to implant displacement 30 days after the original operation and one case of postoperative diplopia also prompted imaging. In another patient, post- operative imaging was obtained due to concerns for RBH based on clinical exam when the patient presented to the emergency department 2 days after the surgery with eye pain and periorbital swelling. RBH was confirmed prompting a return to the OR for hematoma evacuation. Characteristics of the outpatient cases requiring postoperative imaging and their outcomes are listed in
Table 5.
Discussion
Outpatient isolated OBF repair is an attractive alternative to inpatient management considering the associated decreased consumption of healthcare resources as well as reduced patient burden by avoiding hospital admission. Almost half of isolated OBF repairs in this study (
n = 53, 42%) were managed on an outpatient basis. The overall rate of post-operative RBH was low at 1.6% (
n = 2), consistent with previously reported numbers.[
6,
7,
8,
9,
10,
11,
12] One case of RBH was detected at the immediate postoperative exam while the patient was still in the PACU. After hematoma evacuation in the OR, the patient was observed overnight rather than being discharged the same day as was originally planned. The second case of RBH occurred following outpatient OBF repair; however, it did not develop until postoperative day 2. Eye pain prompted presentation to the emergency depart- ment where RBH was quickly diagnosed and treated. Even if the original OBF in this case had been performed on an inpatient basis, RBH onset would have fallen outside of the 23-hour inpatient observation period. In neither case, did inpatient management contribute to RBH detection. The two cases highlight both the severity of RBH presenting signs and symptoms and the importance of appropriate patient coun- seling. Neither is dependent on a formal ophthalmologic assessment, thus allowing for a multidisciplinary approach to OBF repair and postoperative management.
Overnight admission is not required for recognition of immediate postoperative RBH. Some subspecialists who per- form OBF repairs may have an inherent bias toward inpatient observation based on the amount of inpatient versus out- patient surgery performed during their training. However, there are no data to suggest that OBF repair as an inpatient surgery is safer. In addition, overnight monitoring does not necessarily guarantee RBH identification in cases of delayed onset, as was demonstrated in this study and has been described previously in the literature. Valsalva, uncontrolled hypertension, blood dyscrasia, vascular disease, and restarting oral anticoagulant medication are several hypothesized etiologies for delayed RBH.[
6,
8,
11] Careful post-operative examination within 90 minutes of surgery and prolonged PACU monitoring for 2 to 6 hours after surgery are both critical for detecting immediate RBH and should remain standard of care. Hemorrhage resulting from continued or new bleeding at the conclusion of a surgical case would likely be identified in this time window. However, for delayed RBH, detailed counseling of patients, family members, and care- takers regarding risk factors, warning signs, and symptoms that necessitate immediate return to the hospital is paramount.[
16]
Our inpatient and outpatient cohorts differed in terms of the number of days to repair with more outpatient repairs done on a delayed basis. Despite most inpatient repairs being performed immediately or early, common indications for isolated OBF repair including functionally limiting diplopia and significant enophthalmos were present in only a min- ority of cases compared with the vast majority of outpatient repairs. In almost half of inpatient cases, the documented indication for OBF repair was fracture size greater than 50% of the orbital floor. There has been considerable debate in the literature regarding the prognostic implication of fracture size with a concern that larger fractures (>50% of the floor) will lead to subsequent enophthalmos if repair is delayed. There is, however, adequate evidence to support observation of isolated OBF in the absence of EOM restriction and gross diplopia and thus proceed with delayed repair only if sig-nificant sequelae develop.[
17,
18,
19] In addition, delaying surgery provides time for tissue edema from acute injury to resolve, thus allowing for easier visualization and manipulation intraoperatively. In the presence of intraorbital hemorrhage associated with the OBF, delaying repair may even help protect against an orbital compartment syndrome as the fracture plane serves as an opening for orbital contents that may otherwise put unwanted pressure on the optic nerve.
In the outpatient cohort of this study, enophthalmos occurred in 50.9% (n = 27) of cases that proceeded to frac- ture repair. This difference in preoperative characteristics (functionally limiting diplopia, EOM restriction, and enophthalmos) reflects the fact that for many patients in the inpatient cohort, surgery was pursued immediately following the injury with less emphasis placed on the pre-sence or absence of persistent sequelae after several weeks of healing. While the authors’ study did not examine the rate at which isolated OBF repair was deemed unnecessary and thus avoided, it can be hypothesized that monitoring OBF patients before deciding whether to pursue surgery may result in fewer fractures being managed operatively, which would in turn provide some cost relief.
Our cost analysis provides a general comparison of the expense associated with an inpatient versus outpatient approach to isolated OBF repair. Based on our estimates, the total cost of an inpatient repair at our local community hospital would be approximately $9,598.22 compared with $7,742.22 for outpatient management and $7,265.02 if a reflexive postoperative CT scan is deferred. While this was not an all-cost analysis and many additional variables con- tribute to the overall cost of care, such as OR surgeon’s time and implant material, it seems clear to reason that outpatient management, when possible, would be more economical.
An additional variable to consider, independent of out- patient versus inpatient care, is the utility of a postoperative CT scan. In our cohort, reflexive postoperative imaging in the absence of clinical symptoms led to a change in management only in two patients (3.6%). In these cases, it is uncertain whether a return to the OR for implant revision was abso- lutely necessary given the lack of correlation between CT appearance and concerning exam findings. In addition, 96.4% of reflexive postoperative CTs led to no change in manage- ment, suggesting that perhaps it should not be viewed as a requisite component of isolated OBF postoperative manage- ment, but reserved for situations where the postoperative exam changes or causes concern. A similar question has been raised in regard to other facial fractures with the conclusion that postreduction imaging may not be necessary, especially in the hands of experienced surgeons. Various authors have demonstrated that reflexive postreduction imaging rarely alters clinical management.[
2,
20,
21] Although a single post- operative CT scan is only a minor component of the entire OBF repair, it is an easily identifiable source of radiation exposure and healthcare costs that may be obviated in lieu of careful postoperative clinical examination. Further delinea- tion of reflexive postoperative CT findings after isolated OBF repair is needed to help more clearly define its role, if any, at all.
Limitations of this study include the rare occurrence of RBH and other earlycomplications fromisolated OBF repair, which is logistically prohibitive for powering the study to determine a statistically significant difference in RBH incidence between inpatient and outpatient groups. In certain cases, follow-up data in the form of clinic notes could not be obtained due to loss of patient contact or may have been inaccurate due to recall bias. Therefore, it is possible that cases of postoperative com- plications could have been missed. Sampling bias was intro- ducedby the inherently more complexorbital traumatriaged to academic medical centers, which represented our study sites. While the results and observations in this study are general- izable to other medical facilities withexperienced surgeons and well-trained ancillary support staff who can detect concerning changes in the delayed postoperative period, our conclusions may not be as applicable to more resource-poor settings where personnel for close postoperative monitoring are limited.
Lastly, our cost analysis was a simplified comparison of inpatient versus outpatient OBF repair and did not include a formal analysis. Additional factors that impact healthcare costs, such as OR surgeon’s time, specific OR setting, and implant choice, were not analyzed. Detailed calculations by a health economist would need to be pursued to draw more quantitative conclusions regarding the cost differences between inpatient versus outpatient management.
Conclusion
In this study, wehave provided strong evidence that outpatient isolated OBF management, which includes a postoperative examination within 90 minutes of surgery, as well as pro- longed PACU surveillance for 4 to 6 hours, is a safe and economical alternative to inpatient management with 23- hour overnight monitoring. Cases of RBH present with sig- nificant clinical signs and symptoms that will either be noted in the PACU or prompt the patient, who has been educated on concerning signs and symptoms, to return for evaluation in cases of delayed RBH. It is the authors’ opinion that a reflexive postoperative CT scan is not a cost-effective adjunct to the surgical management of isolated OBFs. Lastly, the potential cost savings of outpatient management, which do not detract from quality or safety of patient care, should not be ignored.