
Elevated Zinc and Potassium Levels in Renal Calculi Indicate Distinct Pathophysiological Mechanisms in Urolithiasis

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Material and Methods
- (1)
- Approximately 0.2 g of the sample was weighed into a test tube made of borosilicate glass. Two independent repetitions were made for each sample. The number of analytical repetitions and the mass of the samples for analysis were limited by the mass of the material obtained from patients.
- (2)
- A volume of 4 mL of HNO3 (J.T. Baker, Radnor, PA, USA) was added to each sample.
- (3)
- Mineralization was performed using microwave energy (parameters in Table 1).
- (4)
- Dissolved kidney stones were transferred to volumetric flasks made of borosilicate glass and diluted with deionized water to a volume of 25 mL. An internal standard PlasmaCAL Yb 10 mg/L (Analytichem, Quebec, QC, Canada) was added to each sample to monitor the stability of the analytical signal. Limit of detection (3.3 σ/S), limit of qualification (10 σ/S), and calibration curve range of selected elements are provided in Table 1.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stamatelou, K.; Goldfarb, D.S. Epidemiology of Kidney Stones. Healthcare 2023, 11, 424. [Google Scholar] [CrossRef] [PubMed]
- Gillams, K.; Juliebø-Jones, P.; Juliebø, S.Ø.; Somani, B.K. Gender Differences in Kidney Stone Disease (KSD): Findings from a Systematic Review. Curr. Urol. Rep. 2021, 22, 50. [Google Scholar] [CrossRef]
- Xu, J.Z.; Li, C.; Xia, Q.D.; Lu, J.L.; Wan, Z.C.; Hu, L.; Lv, Y.M.; Lei, X.M.; Guan, W.; Xun, Y.; et al. Sex disparities and the risk of urolithiasis: A large cross-sectional study. Ann. Med. 2022, 54, 1627–1635. [Google Scholar] [CrossRef]
- Romero, V.; Akpinar, H.; Assimos, D.G. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev. Urol. 2010, 12, e86–e96. [Google Scholar] [PubMed] [PubMed Central]
- Ferraro, P.M.; Taylor, E.N.; Curhan, G.C. Factors associated with sex differences in the risk of kidney stones. Nephrol. Dial. Transplant. 2023, 38, 177–183. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, Y.; Zhang, J.; Deng, Q.; Liang, H. Recent advances on the mechanisms of kidney stone formation (Review). Int. J. Mol. Med. 2021, 48, 149. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.R.; Pearle, M.S.; Robertson, W.G.; Gambaro, G.; Canales, B.K.; Doizi, S.; Traxer, O.; Tiselius, H.G. Kidney stones. Nat. Rev. Dis. Primers 2016, 2, 16008. [Google Scholar] [CrossRef] [PubMed]
- Ratkalkar, V.N.; Kleinman, J.G. Mechanisms of Stone Formation. Clin. Rev. Bone Miner. Metab. 2011, 9, 187–197. [Google Scholar] [CrossRef]
- Duan, L.Q.; Li, X.Y.; Li, Q.; Zhao, J.F.; Zhao, L.; Zhang, J.; Wang, Z.H.; Han, Q.H. Study on the Correlation between Urinary Sodium and Potassium Excretion and Blood Pressure in Adult Hypertensive Inpatients of Different Sexes. Int. J. Clin. Pract. 2022, 2022, 1854475. [Google Scholar] [CrossRef]
- Meyer, H.E.; Johansson, L.; Eggen, A.E.; Johansen, H.; Holvik, K. Sodium and Potassium Intake Assessed by Spot and 24-h Urine in the Population-Based Tromsø Study 2015–2016. Nutrients 2019, 11, 1619. [Google Scholar] [CrossRef]
- Liu, Z.; Man, Q.; Li, Y.; Yang, X.; Ding, G.; Zhang, J.; Zhao, W. Estimation of 24-hour urinary sodium and potassium excretion among Chinese adults: A cross-sectional study from the China National Nutrition Survey. Am. J. Clin. Nutr. 2024, 119, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Graham, L.A.; Padmanabhan, S.; Fraser, N.J.; Kumar, S.; Bates, J.M.; Raffi, H.S.; Welsh, P.; Beattie, W.; Hao, S.; Leh, S.; et al. Validation of uromodulin as a candidate gene for human essential hypertension. Hypertension 2014, 63, 551–558. [Google Scholar] [CrossRef] [PubMed]
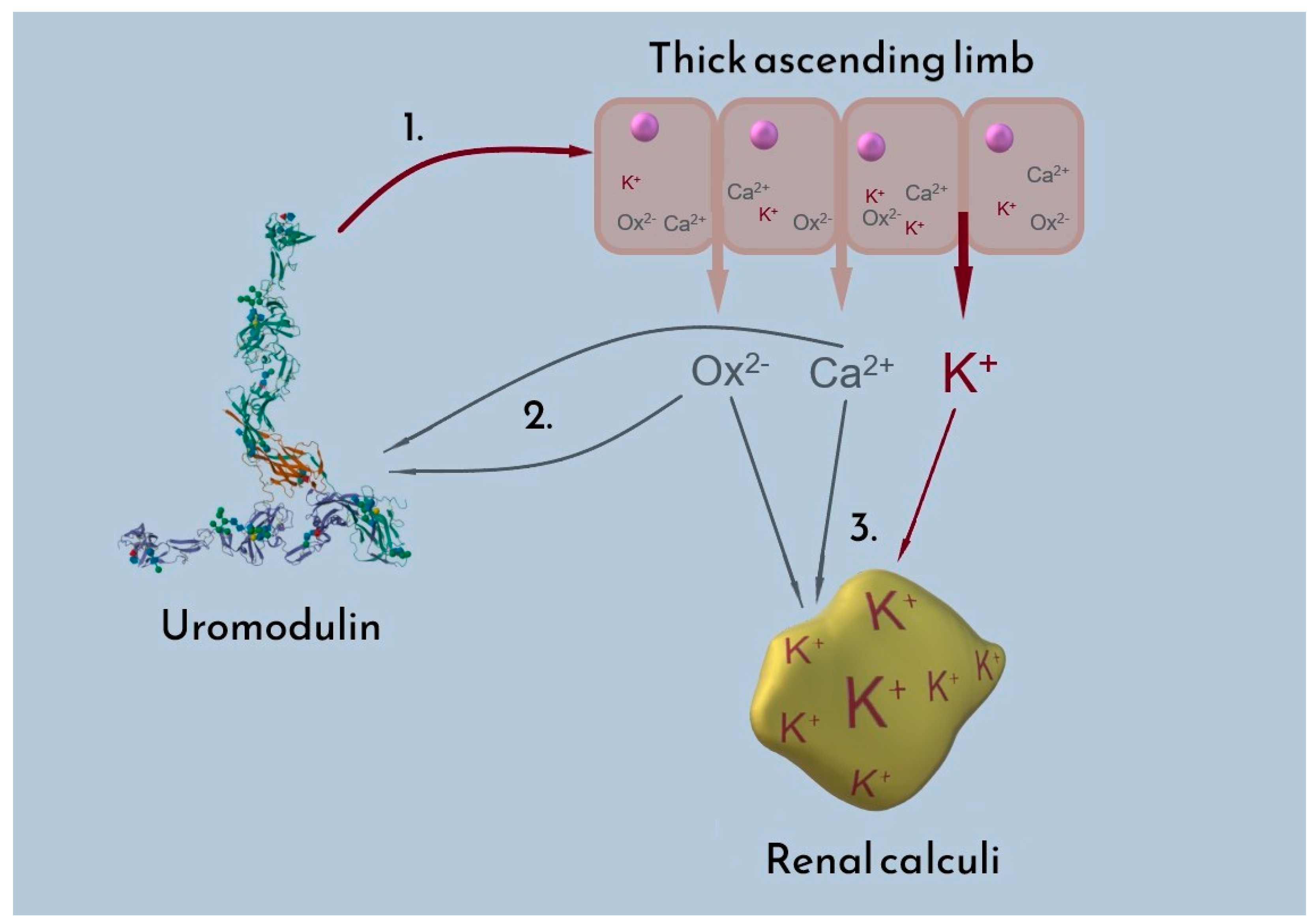
- Wolf, M.T.F.; Zhang, J.; Nie, M. Uromodulin in mineral metabolism. Curr. Opin. Nephrol. Hypertens. 2019, 28, 481–489. [Google Scholar] [CrossRef]
- Renigunta, A.; Renigunta, V.; Saritas, T.; Decher, N.; Mutig, K.; Waldegger, S. Tamm-Horsfall glycoprotein interacts with renal outer medullary potassium channel ROMK2 and regulates its function. J. Biol. Chem. 2011, 286, 2224–2235. [Google Scholar] [CrossRef]
- Noonin, C.; Peerapen, P.; Yoodee, S.; Kapincharanon, C.; Kanlaya, R.; Thongboonkerd, V. Systematic analysis of modulating activities of native human urinary Tamm-Horsfall protein on calcium oxalate crystallization, growth, aggregation, crystal-cell adhesion and invasion through extracellular matrix. Chem.-Biol. Interact. 2022, 357, 109879. [Google Scholar] [CrossRef] [PubMed]
- Mo, B.; Scharf, B.; Gutheil, C.; Letzel, M.C.; Hensel, A. Tamm-Horsfall protein in humane urine: Sex-dependent differences in the excretion and N-glycosylation pattern. Sci. Rep. 2023, 13, 17815. [Google Scholar] [CrossRef]
- van Duijl, T.T.; Ruhaak, L.R.; Hoogeveen, E.K.; de Mutsert, R.; Rosendaal, F.R.; le Cessie, S.; de Fijter, J.W.; Cobbaert, C.M. Reference intervals of urinary kidney injury biomarkers for middle-aged men and women determined by quantitative protein mass spectrometry. Ann. Clin. Biochem. 2022, 59, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Tamborino, F.; Cicchetti, R.; Mascitti, M.; Litterio, G.; Orsini, A.; Ferretti, S.; Basconi, M.; De Palma, A.; Ferro, M.; Marchioni, M.; et al. Pathophysiology and Main Molecular Mechanisms of Urinary Stone Formation and Recurrence. Int. J. Mol. Sci. 2024, 25, 3075. [Google Scholar] [CrossRef] [PubMed]
- Yen, Y.; Cheng, B.; Chan, C.; Lin, C.; Chen, H. Heavy Metal Components in Blood and Urinary Stones of Urolithiasis Patients. Biol. Trace Elem. Res. 2018, 185, 266–274. [Google Scholar] [CrossRef]
- Tian, Y.; Han, G.; Qu, R.; Xiao, C. Major and Trace Elements in Human Kidney Stones: A Preliminary Investigation in Beijing, China. Minerals 2022, 12, 512. [Google Scholar] [CrossRef]
- Turgut, M.; Unal, I.; Berber, A.; Demir, T.A.; Mutlu, F.; Aydar, Y. The concentration of Zn, Mg and Mn in calcium oxalate monohydrate stones appears to interfere with their fragility in ESWL therapy. Urol. Res. 2008, 36, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Taha, S.A.Y.; Shokeir, A.A.; Mortada, W.I.; Awadalla, A.; Barakat, L.A.A. Effect of Copper and Zinc Ions on Biochemical and Molecular Characteristics of Calcium Oxalate Renal Stones: A Controlled Clinical Study. Biol. Trace Elem. Res. 2024, 202, 410–422. [Google Scholar] [CrossRef] [PubMed]
- LeGeros, R.Z.; Bleiwas, C.B.; Retino, M.; Rohanizadeh, R.; LeGeros, J.P. Zinc effect on the in-vitro formation of calcium phosphates: Relevance to clinical inhibition of calculus formation. Am. J. Dent. 1999, 12, 65–71. [Google Scholar] [PubMed]
- Boanini, E.; Gazzano, M.; Nervi, C.; Chierotti, M.R.; Rubini, K.; Gobetto, R.; Bigi, A. Strontium and Zinc Substitution in β-Tricalcium Phosphate: An X-ray Diffraction, Solid State NMR and ATR-FTIR Study. J. Funct. Biomater. 2019, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Hyuga, H.; Kondo, N.; Kita, H.; Sasaki, M.; Mitamura, M.; Hashimoto, K.; Toda, Y. Substitution Model of Monovalent (Li, Na, and K), Divalent (Mg), and Trivalent (Al) Metal Ions for β-Tricalcium Phosphate. J. Am. Ceram. Soc. 2005, 89, 688–690. [Google Scholar] [CrossRef]
- Sun, Y.; Zhou, Q.; Zheng, J. Nephrotoxic metals of cadmium, lead, mercury and arsenic and the odds of kidney stones in adults: An exposure-response analysis of NHANES 2007–2016. Environ. Int. 2019, 132, 105115. [Google Scholar] [CrossRef]
- Huang, J.L.; Mo, Z.Y.; Li, Z.Y.; Liang, G.Y.; Liu, H.L.; Aschner, M.; Ou, S.Y.; Zhou, B.; Chen, Z.M.; Jiang, Y.M. Association of lead and cadmium exposure with kidney stone incidence: A study on the non-occupational population in Nandan of China. J. Trace Elem. Med. Biol. 2021, 68, 126852. [Google Scholar] [CrossRef] [PubMed]
- Day, P.L.; Wermers, M.; Pazdernik, V.; Jannetto, P.J.; Bornhorst, J.A. Detection of Cadmium and Lead in Kidney Stones. Associations with Patient Demographics, Stone Composition, and Smoking. J. Appl. Lab. Med. 2023, 8, 330–340. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Element | Cu | Fe | K | Ni | Pb | Zn |
|---|---|---|---|---|---|---|
| Limit of quantification [mg/kg] | 0.013 | 0.031 | 0.087 | 0.004 | 0.008 | 0.027 |
| Limit of detection [mg/kg] | 0.004 | 0.010 | 0.029 | 0.001 | 0.003 | 0.009 |
| Calibration curve range [mg/L] | 0.005–5.000 | 0.005–2.000 | 0.500–10.00 | 0.005–2.000 | 0.005–2.000 | 0.020–2.000 |
| Female Group | Male Group | p-Value | |
|---|---|---|---|
| Number of participants | n = 24 | n = 20 | |
| Mean age (years) | 63.5 (SD = 13.9) | 62.7 (SD = 10.4) | 0.58 |
| Blood potassium (mmol/L) | 4.31 (SD = 0.34) | 4.41 (SD = 0.33) | 0.33 |
| Blood sodium (mmol/L) | 138.6 (SD = 1.7) | 138.0 (SD = 1.9) | 0.31 |
| Urine specific gravity | 1.014 (SD = 0.005) | 1.016 (SD = 0.004) | 0.42 |
| Present microscopic hematuria | 18 | 12 | - |
| Present leucocyturia | 19 | 18 | - |
| Prior interventions | 8 | 5 | - |
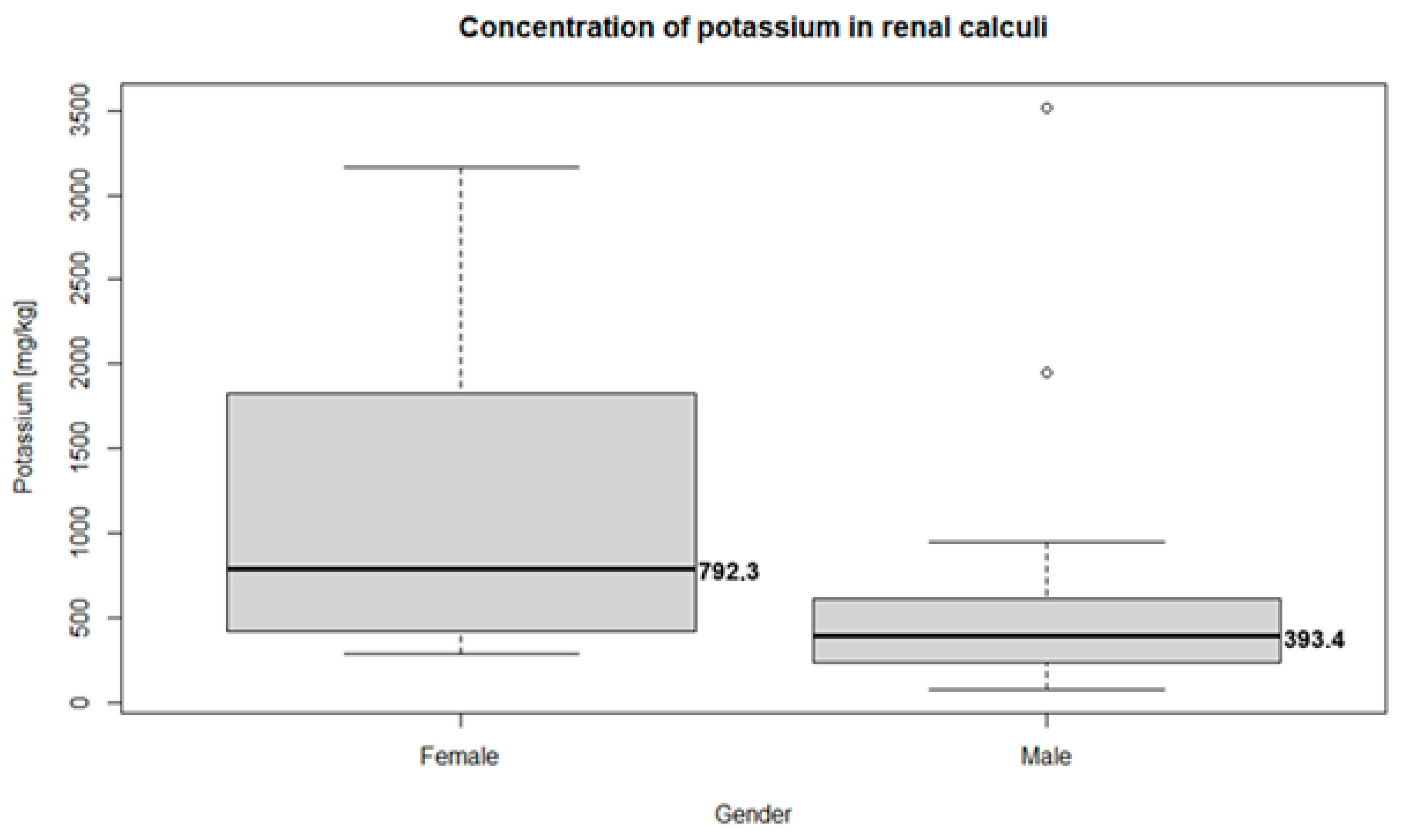
| Median potassium concentration (mg/kg) | 792.3 (95% CI = 297.12–2749.30 | 393.4 (95% CI = 109.82–2773.05) | 0.007 |
| Median copper concentration (mg/kg) | 1.82 (95% CI = 0.64–8.73) | 1.42 (95% CI = 0.75–5.47) | 0.49 |
| Median iron concentration (mg/kg) | 23 (95% CI = 6.80–65.56) | 24.52 (95% CI = 2.52–95.50) | 0.41 |
| Median lead concentration (mg/kg) | 5.23 (95% CI = 1.99–19.69) | 5.48 (95% CI = 0.58–18.41) | 0.45 |
| Median zinc concentration (mg/kg) | 320.05 (95% CI = 15.25–955.59) | 235.8 (95% CI = 7.20–948.46) | 0.62 |
| Median nickel concentration (mg/kg) | 15.68 (95% CI = 1.41–107.00) | 4.01 (95% CI = 0.81–18.33) | 0.19 |
| CaP | CaOx | p-Value | |
|---|---|---|---|
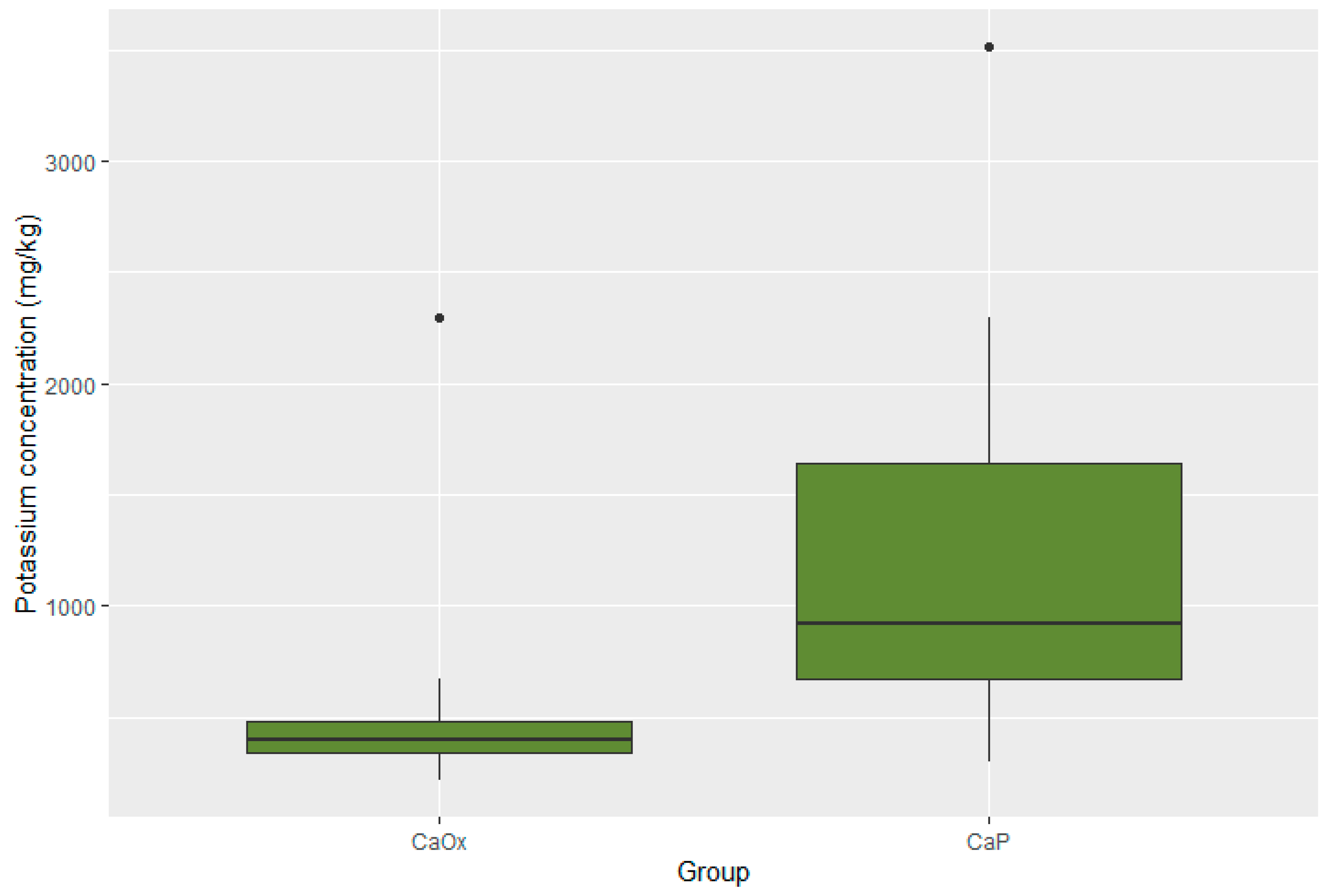
| Median potassium (mg/kg) | 918.4 95% CI 338.02–3026.20 | 400.75 95% CI 222.28–1606.03 | 0.001 |
| Median copper (mg/kg) | 1.56 95% CI 0.72–5.66 | 1.44 95% CI 0.70–7.16 | 0.68 |
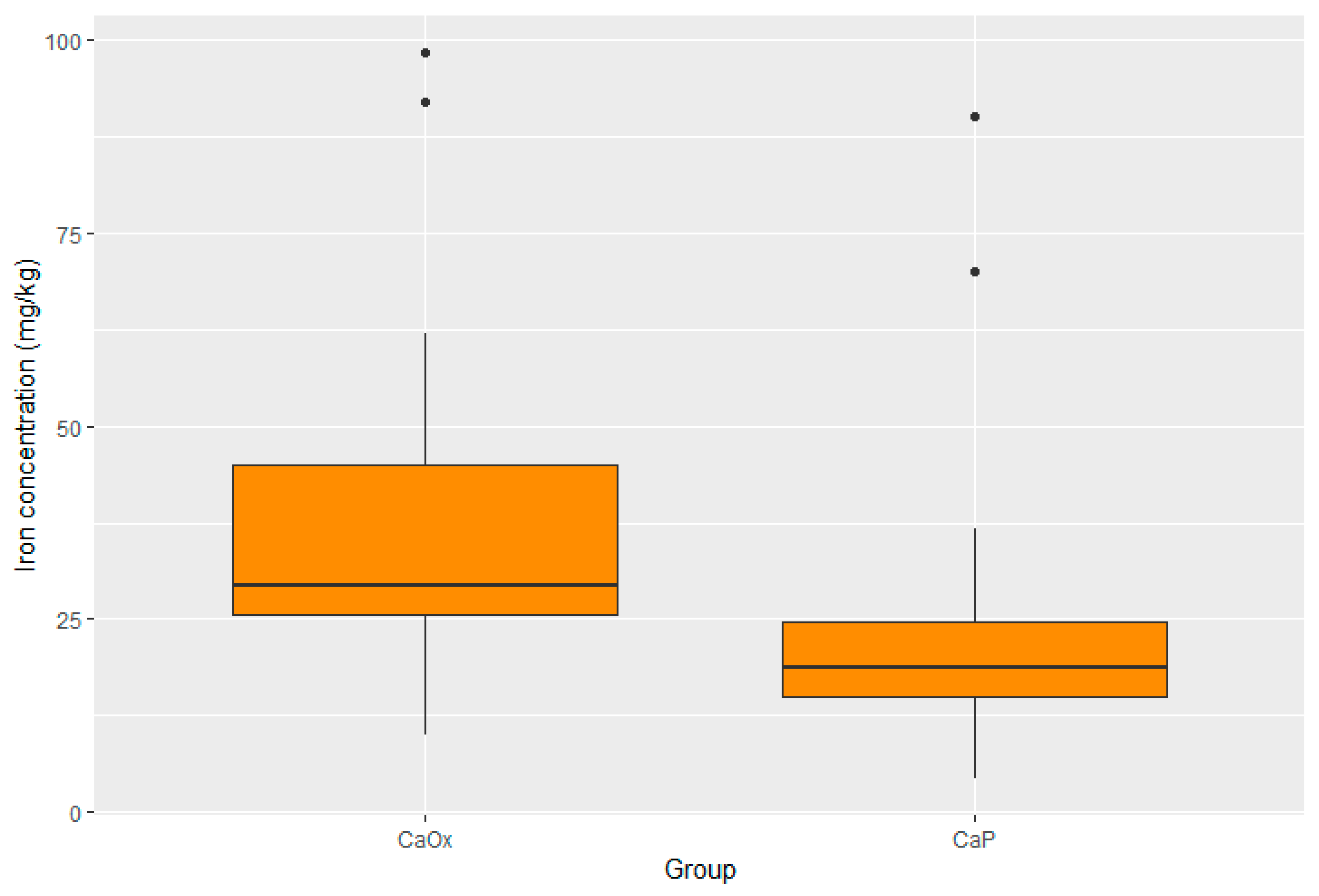
| Median iron (mg/kg) | 18.72 95% CI 6.12–81.94 | 29.47 95% CI 11.27–95.66 | 0.003 |
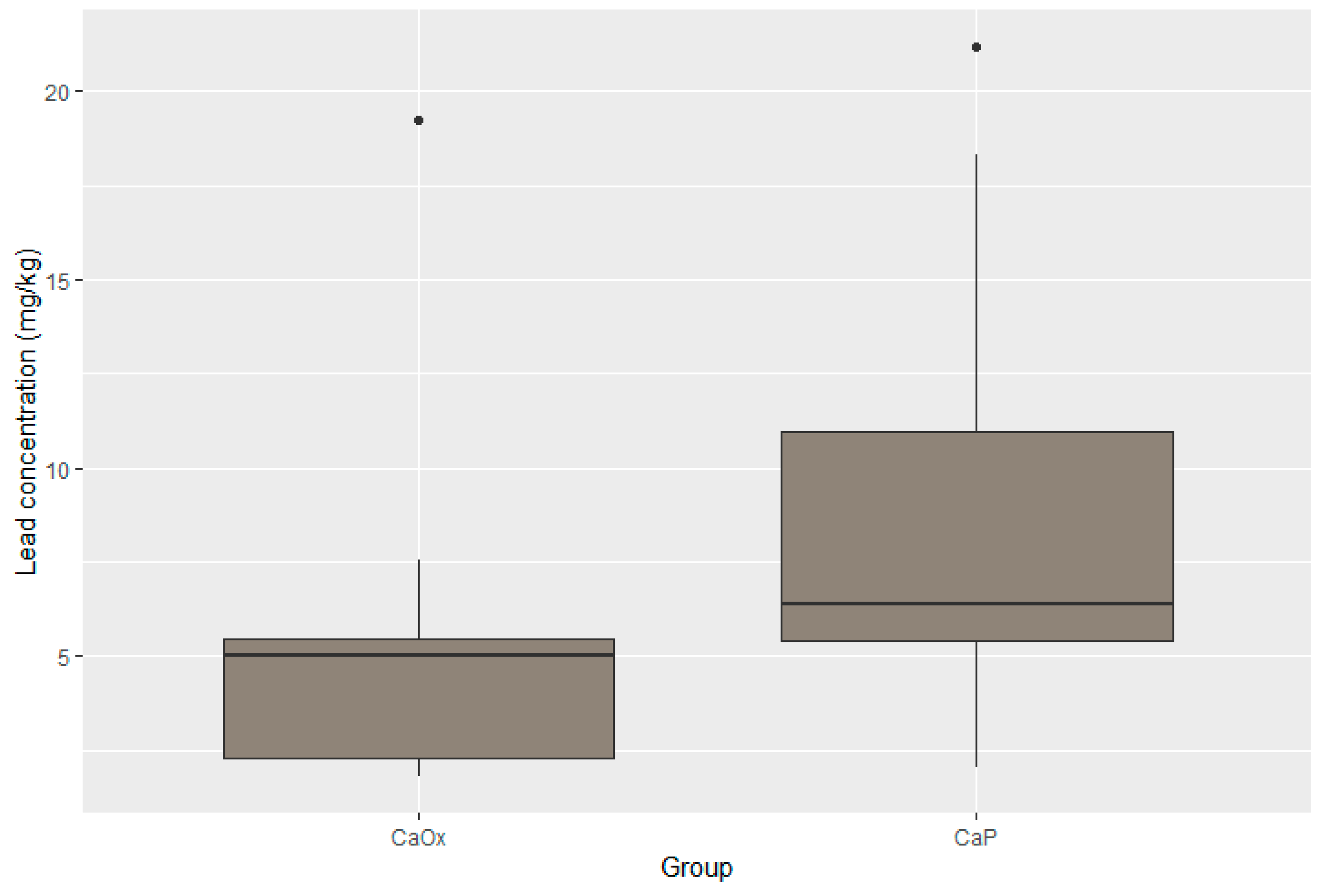
| Median lead (mg/kg) | 6.39 95% CI 2.37–20.12 | 5.03 95% CI 1.85–15.14 | 0.017 |
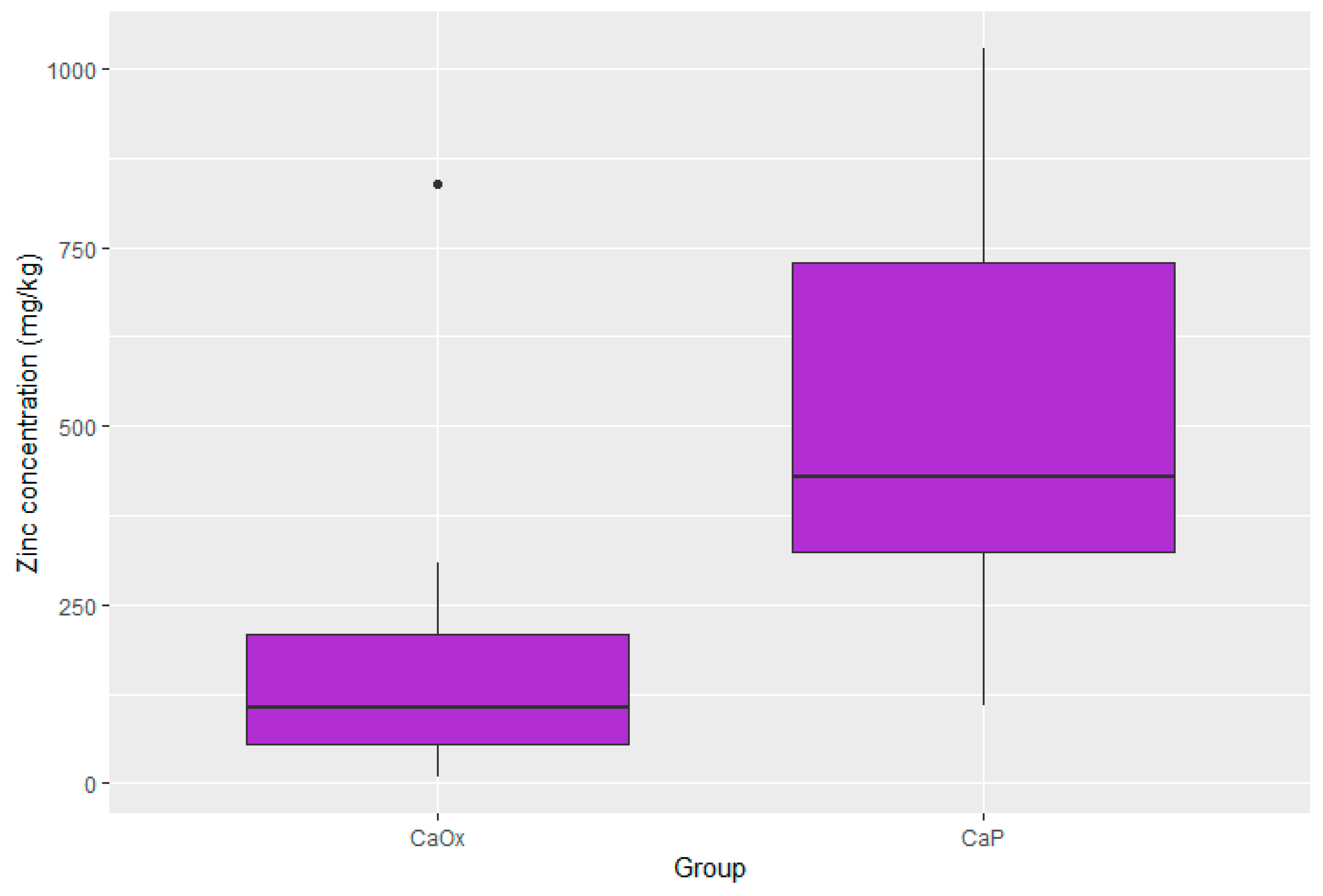
| Median zinc (mg/kg) | 428.41 95% CI 111.64–1020.20 | 106.90 95% CI 10.94–614.37 | 0.001 |
| Median nickel (mg/kg) | 3.71 95% CI 1.64–25.01 | 5.60 95% CI 1.30–123.78 | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaromin, M.; Cichocki, M.; Konecki, T.; Kutwin, P.; Maniukiewicz, W.; Wysocki, P.; Gajek, M.; Szynkowska-Jóźwik, M.I.; Moczulski, D. Elevated Zinc and Potassium Levels in Renal Calculi Indicate Distinct Pathophysiological Mechanisms in Urolithiasis. Pathophysiology 2025, 32, 23. https://doi.org/10.3390/pathophysiology32020023
Jaromin M, Cichocki M, Konecki T, Kutwin P, Maniukiewicz W, Wysocki P, Gajek M, Szynkowska-Jóźwik MI, Moczulski D. Elevated Zinc and Potassium Levels in Renal Calculi Indicate Distinct Pathophysiological Mechanisms in Urolithiasis. Pathophysiology. 2025; 32(2):23. https://doi.org/10.3390/pathophysiology32020023
Chicago/Turabian StyleJaromin, Maciej, Marcin Cichocki, Tomasz Konecki, Piotr Kutwin, Waldemar Maniukiewicz, Piotr Wysocki, Magdalena Gajek, Małgorzata Iwona Szynkowska-Jóźwik, and Dariusz Moczulski. 2025. "Elevated Zinc and Potassium Levels in Renal Calculi Indicate Distinct Pathophysiological Mechanisms in Urolithiasis" Pathophysiology 32, no. 2: 23. https://doi.org/10.3390/pathophysiology32020023
APA StyleJaromin, M., Cichocki, M., Konecki, T., Kutwin, P., Maniukiewicz, W., Wysocki, P., Gajek, M., Szynkowska-Jóźwik, M. I., & Moczulski, D. (2025). Elevated Zinc and Potassium Levels in Renal Calculi Indicate Distinct Pathophysiological Mechanisms in Urolithiasis. Pathophysiology, 32(2), 23. https://doi.org/10.3390/pathophysiology32020023