
CKD Urine Metabolomics: Modern Concepts and Approaches

Abstract
1. Introduction
2. Analytical Methods in CKD Metabolomics Studies
2.1. NMR Spectroscopy
2.2. Mass Spectrometry-Based Methods
3. Biomarkers and Pathways
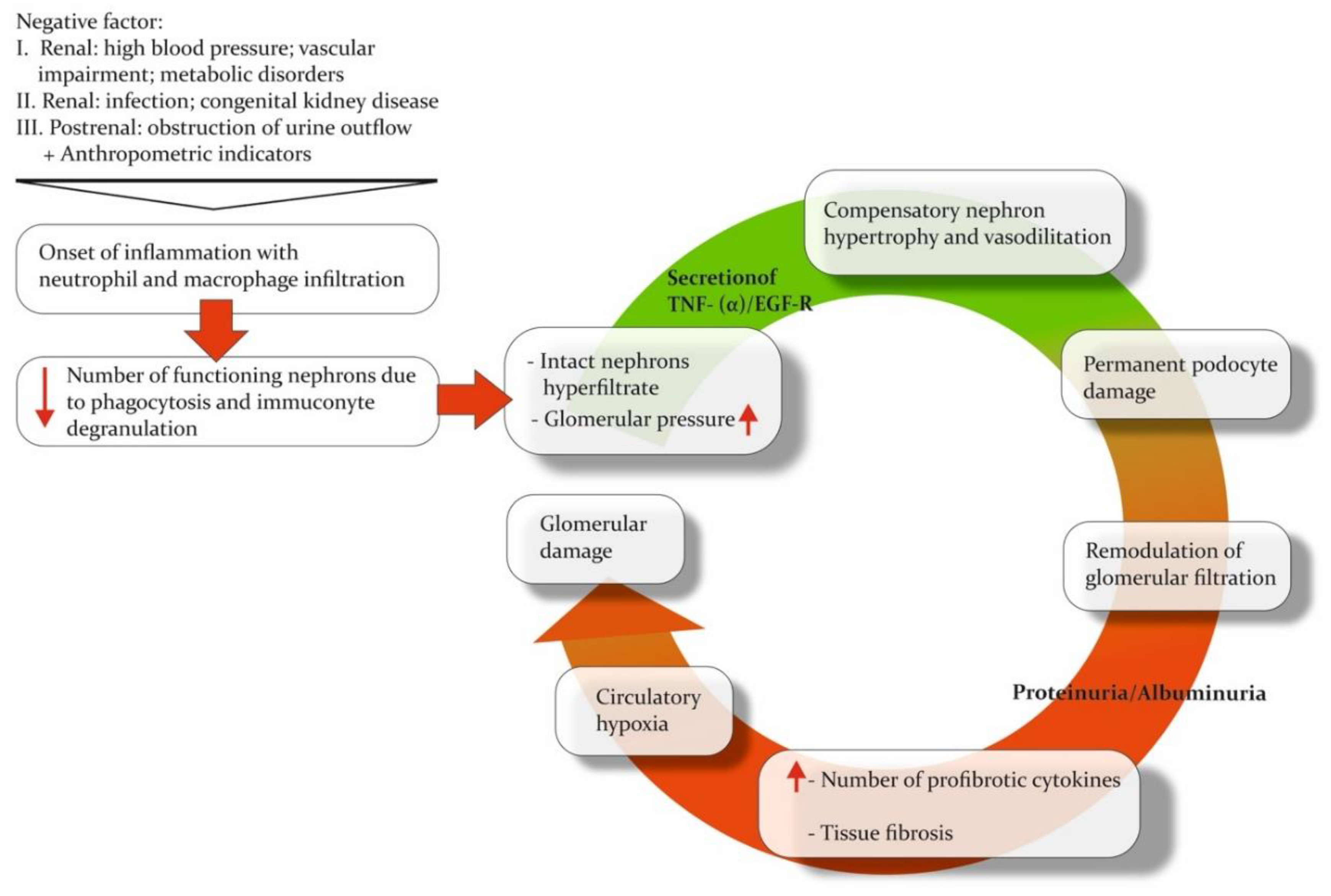
3.1. Pathogenesis of CKD
3.2. Markers of CKD

{kind=link}
| References | Type of Marker | Pathway | Main Markers | Main Findings | Method | Population |
|---|---|---|---|---|---|---|
| [57] | Secretory clearance of waste solutes relative to the GFR | Not annotated to the pathway in the original work | Phenylacetylglutamine, p-cresol sulfate, indoxyl sulfate, hippurate | The traditional GFR values were altered less dramatically than secretory clearances for solutes in advanced CKD stages. | LC-MS | Patients with advanced CKD (n = 16, eGFR,12 mL/min per 1.73 m2) and control participants (n = 16) |
| [28] | Markers related to eGFR | Not annotated to the pathway in the original work | Uracil ꜜ, formic acid ꜜ, glycolic acid ꜜ, hippuric acid ꜜ | Elevated concentrations of myo-inositol and betaine are believed to be associated with the impairment of protein binding for solutes. Despite the reason, the decline in uremic solutes binding indicates impairment of tubular secretion. | 1H-NMR | CKD patients (n = 227), a nested retrospective subgroup (n = 57) |
| TCA cycle | Citric acid ꜜ | |||||
| Amino acid metabolism | L-threonine ꜜ | |||||
| Lipid metabolism | Ethanolamine ꜜ | |||||
| The gut microbiome-derived uremic toxins | Indoxyl sulphate ꜜ, p-cresol sulphate ꜜ | |||||
| Osmolyte transport | Myo-inositol ꜛ, betaine ꜛ | |||||
| CKD prognostic markers | TCA cycle | Citric acid ꜜ | ||||
| Lipid metabolism | Ethanolamine ꜜ | |||||
| Not annotated to the pathway in the original work | Glycolic acid ꜜ, dimethylamine ꜜ, creatinine ꜜ, trimethylamine N-oxide ꜛ | |||||
| Osmolyte transport | Myo-inositol ꜛ, betaine ꜛ | |||||
| [45] | Markers of CKD progression | TCA cycle | Glucose ꜛ | Since choline is often metabolized into other compounds, its urinary excretion is minimal, making its presence in a sample a precise indicator of kidney dysfunction and poor prognosis. | NMR, LC-MS for validation | 789 patients with CKD (stage 1 = 340, stage 2 = 230, stage 3 = 219), 147 healthy control subjects |
| Carbohydrate metabolism | Fumarate ꜛ, citrate ꜜ | |||||
| Choline metabolism | Betaine ꜛ, choline ꜛ | |||||
| [69] | Markers related to eGFR | Not annotated to the pathway in the original work | Serotonin sulfate ꜛ, glycylprolylarginine, all-trans retinoic acid, methylarachidic acid | Both urinary and serum metabolomic profiles should be analyzed as dual variations in the metabolomic profile indicate both glomerular and tubular injury. | HPLC-QTOF- −MS (ESI+) | 88 patients with CKD, staged by eGFR in 6 subgroups and 20 healthy control subjects |
| Amino acid metabolism | Cysteine ꜛ, 5-methoxytryptohan ꜛ, phenylalanine ꜜ | |||||
| Alcylcarnitines | Propenoylcarnitine, butenoylcarnitine ꜛ | |||||
| Uremic toxins | Hippuric acid ꜛ, indoxyl sulfate ꜛ | |||||
| [71] | Markers of CKD during obesity | Uremic toxins | Hippuric acid ꜛ | High levels of hippuric acid found in the urine suggest an improved removal of uremic toxins after bariatric surgery. | GC-HRAM -MS | 11 obese patients with CKD, 14 obese patients without CKD |
| Amino acid metabolism | Valine ꜜ | |||||
| [35] | Markers of CKD and BEN | Uremic toxins | Phenolic compounds (including p-cresol ꜛ) | The presence of elevated p-cresol signals filtration injury, leading to p-cresol accumulation in the kidneys and, eventually, tissue inflammation. | GC-MS | 35 healthy volunteers (53.9%), 25 BEN patients (38.5%), 5 CKD patients (7.7%) |
3.3. Markers for CKD Subtypes
3.4. Markers of Acute Kidney Injury
3.5. Markers of Renal Impairment in Children
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| 3-HIBA | 3-hydroxyisobutyrate |
| 99mTc-DTPA | 99mTc-diethylenetriaminepentaacetic acid |
| ACR | urinary albumin/creatinine ratio |
| ADKD | albuminuria DKD |
| AKI | acute kidney injury |
| ATP | adenosine triphosphate |
| BCAA | branched-chain amino acid |
| BEN | Balkan Endemic Nephropathy |
| CE | capillary electrophoresis |
| CE-MS | capillary electrophoresis mass spectrometry |
| CI | chemical ionization |
| CKD | chronic kidney disease |
| CKD-EPI | chronic kidney disease epidemiology collaboration |
| CRIC | chronic renal insufficiency cohort |
| CPMG | Carr–Purcell–Meiboom–Gill |
| DI-MS | direct injection mass spectrometry |
| DKD | diabetic kidney disease |
| EI | electron ionization |
| eGFR | estimated glomerular filtration rate |
| ESI | electrospray ionization |
| ESKD | end-stage kidney disease |
| GC | gas chromatography |
| GC-MS | gas chromatography-mass spectrometry |
| GFR | glomerular filtration rate |
| HESI | heated electrospray ionization |
| HILIC-LC-MS | hydrophilic interaction liquid chromatography-mass spectrometry |
| ICU | intensive care unit |
| IL-18 | interleukin-18 |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| KIM-1 | kidney injury molecule 1 |
| LC | liquid chromatography |
| LC-MS | liquid chromatography-mass spectrometry |
| MS | mass spectrometry |
| NADKD | normoalbuminuric DKD |
| NAG | N-acetyl-beta-d-glucosaminidase |
| NGAL | neutrophil gelatinase-associated lipocalin |
| NIST | National Institute of Standards and Technology |
| NMR | nuclear magnetic resonance |
| NOESY | nuclear Overhauser effect spectroscopy |
| PAH | phenylalanine hydroxylase |
| Q-TOF-MS | quadrupole time-of-flight mass spectrometry |
| ROS | reactive oxygen species |
| RP | reverse phase |
| RP LC-MS | reverse-phase chromatography-mass spectrometry |
| RPD | renal pelvis dilatation |
| sCr | serum creatinine |
| SDM | simple diabetes mellitus group |
| SNR | signal-to-noise ratio |
| TCA cycle | tricarboxylic acid cycle |
| TCI | transmit coil decoupling using inverse detection |
| TMAO | trimethylamine N-oxide |
| TNF-a/EGF-R | tumor necrosis factor-alpha/epithelial growth factor receptor |
| TOF-MS | time-of-flight mass spectrometry |
| TQ-MS | triple quadrupole mass-spectrometer |
| UPJO | ureteropelvic junction obstruction |
| VOCs | volatile organic compounds |
References
- Cockwell, P.; Fisher, L.A. The global burden of chronic kidney disease. Lancet 2020, 395, 662–664. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Masson, Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Taherkhani, A.; Yekta, R.F.; Mohseni, M.; Saidijam, M.; Oskouie, A.A. Chronic kidney disease: A review of proteomic and metabolomic approaches to membranous glomerulonephritis, focal segmental glomerulosclerosis, and IgA nephropathy biomarkers. Proteome. Sci. 2019, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Lowe, K.M.; Cruz, J.B.; Jones, K.M. Complications in Patients with Chronic Kidney Disease. Crit. Care Nurs. Clin. North. Am. 2022, 34, 395–407. [Google Scholar] [CrossRef]
- Yan, M.T.; Chao, C.T.; Lin, S.H. Chronic Kidney Disease: Strategies to Retard Progression. Int. J. Mol. Sci. 2021, 22, 10084. [Google Scholar] [CrossRef]
- Sanchez-Niño, M.D.; Sanz, A.B.; Ramos, A.M.; Fernandez-Fernandez, B.; Ortiz, A. Clinical proteomics in kidney disease as an exponential technology: Heading towards the disruptive phase. Clin. Kidney. J. 2017, 10, 188–191. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Eckardt, K.U.; Coresh, J.; Devuyst, O.; Johnson, R.J.; Köttgen, A.; Levey, A.S.; Levin, A. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013, 382, 158–169. [Google Scholar] [CrossRef]
- George, J.A.; Gounden, V. Novel glomerular filtration markers. Adv. Clin. Chem. 2019, 88, 91–119. [Google Scholar] [CrossRef]
- Nickolas, T.L.; Barasch, J.; Devarajan, P. Biomarkers in acute and chronic kidney disease. Curr. Opin. Nephrol. Hypertens. 2008, 17, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Parikh, C.R. Biomarkers of Acute and Chronic Kidney Disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.-S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Kotsis, F.; Schultheiss, U.T.; Wuttke, M.; Schlosser, P.; Mielke, J.; Becker, M.S.; Oefner, P.J.; Karoly, E.D.; Mohney, R.P.; Eckardt, K.-U.; et al. on behalf of the G. Investigators, Self-Reported Medication Use and Urinary Drug Metabolites in the German Chronic Kidney Disease (GCKD) Study. J. Am. Soc. Nephrol. 2021, 32, 2315–2329. [Google Scholar] [CrossRef]
- Perez-Gomez, M.V.; Martin-Cleary, C.; Fernandez-Fernandez, B.; Ortiz, A. Meso-American nephropathy: What we have learned about the potential genetic influence on chronic kidney disease development. Clin. Kidney J. 2018, 11, 491–495. [Google Scholar] [CrossRef]
- Ko, G.J.; Grigoryev, D.N.; Linfert, D.; Jang, H.R.; Watkins, T.; Cheadle, C.; Racusen, L.; Rabb, H. Transcriptional analysis of kidneys during repair from AKI reveals possible roles for NGAL and KIM-1 as biomarkers of AKI-to-CKD transition. Am. J. Physiol. Renal. Physiol. 2010, 298, F1472–F1483. [Google Scholar] [CrossRef]
- Hsu, C.; Xie, D.; Waikar, S.S.; Bonventre, J.V.; Zhang, X.; Sabbisetti, V.; Mifflin, T.E.; Coresh, J.; Diamantidis, C.J.; He, J.; et al. Urine biomarkers of tubular injury do not improve on the clinical model predicting chronic kidney disease progression. Kidney Int. 2017, 91, 196–203. [Google Scholar] [CrossRef]
- Kim, K.; Aronov, P.; Zakharkin, S.O.; Anderson, D.; Perroud, B.; Thompson, I.M.; Weiss, R.H. Urine metabolomics analysis for kidney cancer detection and biomarker discovery. Mol. Cell Proteom. 2009, 8, 558–570. [Google Scholar] [CrossRef]
- Toyohara, T.; Akiyama, Y.; Suzuki, T.; Takeuchi, Y.; Mishima, E.; Tanemoto, M.; Momose, A.; Toki, N.; Sato, H.; Nakayama, M.; et al. Metabolomic profiling of uremic solutes in CKD patients. Hypertens. Res. 2010, 33, 944–952. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Laukkanen, J.A. Renal complications in COVID-19: A systematic review and meta-analysis. Ann. Med. 2020, 52, 345–353. [Google Scholar] [CrossRef]
- Karczewski, K.J.; Snyder, M.P. Integrative omics for health and disease. Nat. Rev. Genet. 2018, 19, 299–310. [Google Scholar] [CrossRef]
- Liu, J.-J.; Liu, S.; Gurung, R.L.; Ching, J.; Kovalik, J.-P.; Tan, T.Y.; Lim, S.C. Urine Tricarboxylic Acid Cycle Metabolites Predict Progressive Chronic Kidney Disease in Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2018, 103, 4357–4364. [Google Scholar] [CrossRef] [PubMed]
- Macioszek, S.; Wawrzyniak, R.; Kranz, A.; Kordalewska, M.; Struck-Lewicka, W.; Dudzik, D.; Biesemans, M.; Maternik, M.; Żurowska, A.M.; Markuszewski, M.J. Comprehensive Metabolic Signature of Renal Dysplasia in Children. A Multiplatform Metabolomics Concept. Front. Mol. Biosci. 2021, 8, 665661. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Hu, J.; Xu, Y.; Abraham, A.G.; Xiao, R.; Coresh, J.; Rebholz, C.; Chen, J.; Rhee, E.P.; Feldman, H.I.; et al. Using Machine Learning to Identify Metabolomic Signatures of Pediatric Chronic Kidney Disease Etiology. J. Am. Soc. Nephrol. 2022, 33, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.; Lopata, A.L.; Dasouki, M.; Rahman, A.M.A. Metabolomics toward personalized medicine. Mass Spectrom. Rev. 2019, 38, 221–238. [Google Scholar] [CrossRef] [PubMed]
- Al-Ismaili, Z.; Palijan, A.; Zappitelli, M. Biomarkers of acute kidney injury in children: Discovery, evaluation, and clinical application. Pediatr. Nephrol. 2011, 26, 29–40. [Google Scholar] [CrossRef]
- Bell, J.D.; Lee, J.A.; Lee, H.A.; Sadler, P.J.; Wilkie, D.R.; Woodham, R.H. Nuclear magnetic resonance studies of blood plasma and urine from subjects with chronic renal failure: Identification of trimethylamine-N-oxide. Biochim. Biophys. Acta 1991, 1096, 101–107. [Google Scholar] [CrossRef]
- Gil, R.B.; Ortiz, A.; Sanchez-Niño, M.D.; Markoska, K.; Schepers, E.; Vanholder, R.; Glorieux, G.; Schmitt-Kopplin, P.; Heinzmann, S.S. Increased urinary osmolyte excretion indicates chronic kidney disease severity and progression rate. Nephrol. Dial. Transplant. 2018, 33, 2156–2164. [Google Scholar] [CrossRef]
- Dalili, N.; Chashmniam, S.; Khoormizi, S.M.H.; Salehi, L.; Jamalian, S.A.; Nafar, M.; Kalantari, S. Urine and serum NMR-based metabolomics in pre-procedural prediction of contrast-induced nephropathy. Intern. Emerg. Med. 2020, 15, 95–103. [Google Scholar] [CrossRef]
- Chasapi, S.A.; Karagkouni, E.; Kalavrizioti, D.; Vamvakas, S.; Zompra, A.; Takis, P.G.; Goumenos, D.S.; Spyroulias, G.A. NMR-Based Metabolomics in Differential Diagnosis of Chronic Kidney Disease (CKD) Subtypes. Metabolites 2022, 12, 490. [Google Scholar] [CrossRef]
- Mutter, S.; Valo, E.; Aittomäki, V.; Nybo, K.; Raivonen, L.; Thorn, L.M.; Forsblom, C.; Sandholm, N.; Würtz, P.; Groop, P.H. Urinary metabolite profiling and risk of progression of diabetic nephropathy in 2670 individuals with type 1 diabetes. Diabetologia 2022, 65, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Lucio-Gutiérrez, J.R.; Cordero-Pérez, P.; Farías-Navarro, I.C.; Tijerina-Marquez, R.; Sánchez-Martínez, C.; Ávila-Velázquez, J.L.; García-Hernández, P.A.; Náñez-Terreros, H.; Coello-Bonilla, J.; Pérez-Trujillo, M.; et al. Using nuclear magnetic resonance urine metabolomics to develop a prediction model of early stages of renal disease in subjects with type 2 diabetes. J. Pharm. Biomed. Anal. 2022, 219, 114885. [Google Scholar] [CrossRef] [PubMed]
- Muhle-goll, C.; Eisenmann, P.; Luy, B.; Kölker, S.; Tönshoff, B.; Fichtner, A.; Westhoff, J.H. Urinary NMR Profiling in Pediatric Acute Kidney Injury—A Pilot Study. Int. J. Mol. Sci. 2020, 21, 1187. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Wang, L.; Chen, B.; Wang, C.; Wang, M.; Li, J.; Gao, X.; Zhang, Z.; Han, L. A multiple-metabolites model to predict preliminary renal injury induced by iodixanol based on UHPLC/Q-Orbitrap-MS and 1H-NMR. Metabolomics 2022, 18, 85. [Google Scholar] [CrossRef]
- Ordodi, V.L.; Hădărugă, N.G.; Hădărugă, D.I.; Lukinich-Gruia, A.T.; Mărgineanu, M.; Tatu, C.A.; Păunescu, V. Urine Metabolomic Signature of People Diagnosed with Balkan Endemic Nephropathy and Other Types of Chronic Kidney Disease Compared with Healthy Subjects in Romania. Metabolites 2023, 13, 609. [Google Scholar] [CrossRef]
- Ligor, T.; Zawadzka, J.; Strączyński, G.; Paredes, R.M.G.; Wenda-Piesik, A.; Ratiu, I.A.; Muszytowski, M. Searching for Potential Markers of Glomerulopathy in Urine by HS-SPME-GC × GC TOFMS. Molecules 2021, 26, 1817. [Google Scholar] [CrossRef]
- Shao, M.; Lu, H.; Yang, M.; Liu, Y.; Yin, P.; Li, G.; Wang, Y.; Chen, L.; Chen, Q.; Zhao, C.; et al. Serum, and urine metabolomics reveal potential biomarkers of T2DM patients with nephropathy. Ann. Transl. Med. 2020, 8, 199. [Google Scholar] [CrossRef]
- Taherkhani, A.; Nafar, M.; Arefi-Oskouei, A.; Broumandnia, N.; Parvin, M.; Mahmoudieh, L.; Kalantari, S. Metabolomic Analysis of Membranous Glomerulonephritis: Identification of a Diagnostic Panel and Pathogenic Pathways. Arch. Med. Res. 2019, 50, 159–169. [Google Scholar] [CrossRef]
- Hirakawa, Y.; Yoshioka, K.; Kojima, K.; Yamashita, Y.; Shibahara, T.; Wada, T.; Nangaku, M.; Inagi, R. Potential progression biomarkers of diabetic kidney disease determined using comprehensive machine learning analysis of non-targeted metabolomics. Sci. Rep. 2022, 12, 16287. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, P.; Bao, G.; Fang, Y.; Chen, W. Discovery of potential biomarkers in acute kidney injury by ultra-high-performance liquid chromatography-tandem quadrupole time-of-flight mass spectrometry (UPLC-Q/TOF–MS). Int. Urol. Nephrol. 2021, 53, 2635–2643. [Google Scholar] [CrossRef]
- Piedrafita, A.; Balayssac, S.; Mayeur, N.; Gazut, S.; Grossac, J.; Buleon, M.; Alves, M.; Klein, J.; Minville, V.; Marcheix, B.; et al. The tryptophan pathway and nicotinamide supplementation in ischaemic acute kidney injury. Clin. Kidney J. 2021, 14, 2490–2496. [Google Scholar] [CrossRef] [PubMed]
- Saito, R.; Hirayama, A.; Akiba, A.; Kamei, Y.; Kato, Y.; Ikeda, S.; Kwan, B.; Pu, M.; Natarajan, L.; Shinjo, H.; et al. Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry. Metabolites 2021, 11, 671. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xiao, C.; Liu, C.; Li, J.; Fang, F.; Lu, X.; Zhang, C.; Xu, F. Identification of Biomarkers of Sepsis-Associated Acute Kidney Injury in Pediatric Patients Based on UPLC-QTOF/MS. Inflammation 2020, 43, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Kwan, B.; Fuhrer, T.; Zhang, J.; Darshi, M.; Van Espen, B.; Montemayor, D.; de Boer, I.H.; Dobre, M.; Hsu, C.Y.; Kelly, T.N.; et al. Metabolomic Markers of Kidney Function Decline in Patients with Diabetes: Evidence from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 2020, 76, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, J.; Kang, M.S.; Song, J.; Kim, S.G.; Cho, S.; Huh, H.; Lee, S.; Park, S.; Jo, H.A.; et al. Urinary metabolite profile predicting the progression of chronic kidney disease. Kidney 2023, 4, 1048–1057. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, K.; Hirakawa, Y.; Kurano, M.; Ube, Y.; Ono, Y.; Kojima, K.; Iwama, T.; Kano, K.; Hasegawa, S.; Inoue, T.; et al. Lysophosphatidylcholine mediates fast decline in kidney function in diabetic kidney disease. Kidney Int. 2022, 101, 510–526. [Google Scholar] [CrossRef]
- Feng, Q.; Li, Y.; Yang, Y.; Feng, J. Urine Metabolomics Analysis in Patients with Normoalbuminuric Diabetic Kidney Disease. Front. Physiol. 2020, 11, 578799. [Google Scholar] [CrossRef]
- Bai, Y.; Zhang, H.; Wu, Z.; Huang, S.; Luo, Z.; Wu, K.; Hu, L.; Chen, C. Use of ultra high-performance liquid chromatography with high resolution mass spectrometry to analyze urinary metabolome alterations following acute kidney injury in post-cardiac surgery patients. J. Mass Spectrom. Adv. Clin. Lab. 2022, 24, 31–40. [Google Scholar] [CrossRef]
- Masania, J.; Faustmann, G.; Anwar, A.; Hafner-Giessauf, H.; Rajpoot, N.; Grabher, J.; Rajpoot, K.; Tiran, B.; Obermayer-Pietsch, B.; Winklhofer-Roob, B.M.; et al. Urinary Metabolomic Markers of Protein Glycation, Oxidation, and Nitration in Early-Stage Decline in Metabolic, Vascular, and Renal Health. Oxid. Med. Cell Longev. 2019, 2019, 4851323. [Google Scholar] [CrossRef]
- Zhang, J.; Fuhrer, T.; Ye, H.; Kwan, B.; Montemayor, D.; Tumova, J.; Darshi, M.; Afshinnia, F.; Scialla, J.J.; Anderson, A.; et al. High-Throughput Metabolomics and Diabetic Kidney Disease Progression: Evidence from the Chronic Renal Insufficiency (CRIC) Study. Am. J. Nephrol. 2022, 53, 215–225. [Google Scholar] [CrossRef]
- Lv, W.; Booz, G.W.; Wang, Y.; Fan, F.; Roman, R.J. Inflammation and renal fibrosis: Recent developments on key signaling molecules as potential therapeutic targets. Eur. J. Pharmacol. 2018, 820, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Chagnac, A.; Zingerman, B.; Rozen-Zvi, B.; Herman-Edelstein, M. Consequences of Glomerular Hyperfiltration: The Role of Physical Forces in the Pathogenesis of Chronic Kidney Disease in Diabetes and Obesity. Nephron 2019, 143, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Lindhardt, M.; Persson, F.; Currie, G.; Pontillo, C.; Beige, J.; Delles, C.; Von Der Leyen, H.; Mischak, H.; Navis, G.; Noutsou, M.; et al. Proteomic prediction and Renin angiotensin aldosterone system Inhibition prevention of early diabetic nephropathy in TYpe 2 diabetic patients with normoalbuminuria (PRIORITY): Essential study design and rationale of a randomised clinical multicentre trial. BMJ Open 2016, 6, e010310. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.J. Chronic kidney disease. Nat. Rev. Dis. Primers 2017, 3, 17088. [Google Scholar] [CrossRef]
- Humphreys, B.D. Mechanisms of Renal Fibrosis. Annu. Rev. Physiol. 2018, 80, 309–326. [Google Scholar] [CrossRef]
- Wang, Y.N.; Ma, S.X.; Chen, Y.Y.; Chen, L.; Liu, B.L.; Liu, Q.Q.; Zhao, Y.Y. Chronic kidney disease: Biomarker diagnosis to therapeutic targets. Clin. Chim. Acta 2019, 499, 54–63. [Google Scholar] [CrossRef]
- Schnaper, H.W. The Tubulointerstitial Pathophysiology of Progressive Kidney Disease. Adv. Chronic. Kidney Dis. 2017, 24, 107–116. [Google Scholar] [CrossRef]
- Duffield, J.S. Cellular and molecular mechanisms in kidney fibrosis. J. Clin. Investig. 2014, 124, 2299–2306. [Google Scholar] [CrossRef]
- Fu, Q.; Colgan, S.P.; Shelley, C.S. Hypoxia: The Force that Drives Chronic Kidney Disease. Clin. Med. Res. 2016, 14, 15–39. [Google Scholar] [CrossRef]
- Tanaka, S.; Tanaka, T.; Nangaku, M. Hypoxia and Dysregulated Angiogenesis in Kidney Disease. Kidney Dis. 2015, 1, 80–89. [Google Scholar] [CrossRef]
- Carbonare, L.D.; Valenti, M.T.; Giannini, S.; Gallieni, M.; Stefani, F.; Ciresa, R.; Politi, C.; Fusaro, M. Bone Biopsy for Histomorphometry in Chronic Kidney Disease (CKD): State-of-the-Art and New Perspectives. J. Clin. Med. 2021, 10, 4617. [Google Scholar] [CrossRef] [PubMed]
- Misra, B.B.; Upadhayay, R.P.; Cox, L.A.; Olivier, M. Optimized GC–MS metabolomics for the analysis of kidney tissue metabolites. Metabolomics 2018, 14, 75. [Google Scholar] [CrossRef]
- Hanifa, M.A.; Skott, M.; Maltesen, R.G.; Rasmussen, B.S.; Nielsen, S.; Frøkiær, J.; Ring, T.; Wimmer, R. Tissue, urine and blood metabolite signatures of chronic kidney disease in the 5/6 nephrectomy rat model. Metabolomics 2019, 15, 112. [Google Scholar] [CrossRef] [PubMed]
- Mussap, M.; Noto, A.; Fanos, V.; Van Den Anker, J.N. Emerging Biomarkers and Metabolomics for Assessing Toxic Nephropathy and Acute Kidney Injury (AKI) in Neonatology. Biomed. Res. Int. 2014, 2014, 602526. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M.; et al. Association between albuminuria; kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef] [PubMed]
- Nkuipou-Kenfack, E.; Duranton, F.; Gayrard, N.; Argilés, À.; Lundin, U.; Weinberger, K.M.; Dakna, M.; Delles, C.; Mullen, W.; Husi, H.; et al. Assessment of metabolomic and proteomic biomarkers in detection and prognosis of progression of renal function in chronic kidney disease. PLoS ONE 2014, 9, e96955. [Google Scholar] [CrossRef]
- Uwaezuoke, S.N.; Ayuk, A.C.; Muoneke, V.U.; Mbanefo, N.R. Chronic kidney disease in children: Using novel biomarkers as predictors of disease. Saudi. J. Kidney Dis. Transpl. 2018, 29, 775–784. [Google Scholar] [CrossRef]
- Mair, R.D.; Lee, S.; Plummer, N.S.; Sirich, T.L.; Meyer, T.W. Impaired tubular secretion of organic solutes in advanced chronic kidney disease. J. Am. Soc. Nephrology 2021, 32, 2877. [Google Scholar] [CrossRef]
- Glavan, M.R.; Socaciu, C.; Socaciu, A.I.; Gadalean, F.; Cretu, O.M.; Vlad, A.; Muntean, D.M.; Bob, F.; Milas, O.; Suteanu, A.; et al. Untargeted Metabolomics by Ultra-High-Performance Liquid Chromatography Coupled with Electrospray Ionization-Quadrupole-Time of Flight-Mass Spectrometry Analysis Identifies a Specific Metabolomic Profile in Patients with Early Chronic Kidney Disease. Biomedicines 2023, 11, 1057. [Google Scholar] [CrossRef]
- Kim, S.; Kang, C.; Park, J.; Han, S.S.; Koh, Y.; Yoon, S.-S. Abstract 672: A genetic defect in phenylalanine hydroxylase (PAH) affects the immune system in kidney. Cancer Res. 2023, 83, 672. [Google Scholar] [CrossRef]
- Lanzon, B.; Martin-taboada, M.; Castro-alves, V.; Vila-bedmar, R.; de Pablos, I.G.; Duberg, D.; Gomez, P.; Rodriguez, E.; Orešič, M.; Hyötyläinen, T.; et al. Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity. Metabolites 2021, 11, 836. [Google Scholar] [CrossRef] [PubMed]
- Vanweert, F.; Schrauwen, P.; Phielix, E. Role of branched-chain amino acid metabolism in the pathogenesis of obesity and type 2 diabetes-related metabolic disturbances BCAA metabolism in type 2 diabetes. Nutr. Diabetes 2022, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.L.; Kelly, B.; Logan, A.; Costa, A.S.H.; Varma, M.; Bryant, C.E.; Tourlomousis, P.; Däbritz, J.H.M.; Gottlieb, E.; Latorre, I.; et al. Succinate Dehydrogenase Supports Metabolic Repurposing of Mitochondria to Drive Inflammatory Macrophages. Cell 2016, 167, 457–470.e13. [Google Scholar] [CrossRef] [PubMed]
- Chouchani, E.T.; Pell, V.R.; Gaude, E.; Aksentijević, D.; Sundier, S.Y.; Robb, E.L.; Logan, A.; Nadtochiy, S.M.; Ord, E.N.J.; Smith, A.C.; et al. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature 2014, 515, 431–435. [Google Scholar] [CrossRef]
- Ye, Z.; Wang, S.; Zhang, C.; Zhao, Y. Coordinated Modulation of Energy Metabolism and Inflammation by Branched-Chain Amino Acids and Fatty Acids. Front. Endocrinol. 2020, 11, 559087. [Google Scholar] [CrossRef]
- Kwon, S.; Hyeon, J.S.; Jung, Y.; Li, L.; An, J.N.; Kim, Y.C.; Yang, S.H.; Kim, T.; Kim, D.K.; Lim, C.S.; et al. Urine myo-inositol as a novel prognostic biomarker for diabetic kidney disease: A targeted metabolomics study using nuclear magnetic resonance. Kidney Res. Clin. Pract. 2023, 42, 445–459. [Google Scholar] [CrossRef]
- Reiss, A.B.; De Leon, J.; Pan, X. The Roles of Fatty Acids and Apolipoproteins in the Kidneys. Metabolites 2022, 12, 462. [Google Scholar] [CrossRef]
- Sun, Y.; Zhou, C.; Chen, Y.; He, X.; Gao, F.; Xue, D. Quantitative increase in short-chain fatty acids, especially butyrate protects kidney from ischemia/reperfusion injury. J. Investig. Med. 2022, 70, 29–35. [Google Scholar] [CrossRef]
- Cui, F.Q.; Wang, Y.F.; Gao, Y.B.; Meng, Y.; Cai, Z.; Shen, C.; Liu, Z.Q.; Jiang, X.C.; Zhao, W.J.; Zhao, R. Effects of BSF on Podocyte Apoptosis via Regulating the ROS-Mediated PI3K/AKT Pathway in DN. J. Diabetes Res. 2019, 2019, 9512406. [Google Scholar] [CrossRef]
- Abdelsattar, S.; Kasemy, Z.A.; Elsayed, M.; Elrahem, T.A.; Zewain, S.K. Targeted metabolomics as a tool for the diagnosis of kidney disease in Type II diabetes mellitus. N. Pub. Front. 2021, 78, 184–190. [Google Scholar] [CrossRef]
- Jeon, Y.H.; Lee, S.; Kim, D.W.; Kim, S.; Bae, S.S.; Han, M.; Seong, E.Y.; Song, S.H. Serum and urine metabolomic biomarkers for predicting prognosis in patients with immunoglobulin A nephropathy. Kidney Res. Clin. Pract. 2023. [Google Scholar] [CrossRef]
- Mogos, M.; Socaciu, C.; Socaciu, A.I.; Vlad, A.; Gadalean, F.; Bob, F.; Milas, O.; Cretu, O.M.; Suteanu-Simulescu, A.; Glavan, M.; et al. Metabolomic Investigation of Blood and Urinary Amino Acids and Derivatives in Patients with Type 2 Diabetes Mellitus and Early Diabetic Kidney Disease. Biomedicines 2023, 11, 1527. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, J.; Yang, S.H.; Lee, H.; Kim, J.Y.; Park, M.; Kim, K.H.; Moon, J.J.; Cho, S.; Lee, S.; et al. Comprehensive metabolomic profiling in early IgA nephropathy patients reveals urine glycine as a prognostic biomarker. J. Cell Mol. Med. 2021, 25, 5177. [Google Scholar] [CrossRef] [PubMed]
- Franiek, A.; Sharma, A.; Cockovski, V.; Wishart, D.S.; Zappitelli, M.; Blydt-Hansen, T.D. Urinary metabolomics to develop predictors for pediatric acute kidney injury. Pediatr. Nephrol. 2022, 37, 2079–2090. [Google Scholar] [CrossRef] [PubMed]
- Scalabre, A.; Clément, Y.; Guillière, F.; Ayciriex, S.; Gaillard, S.; Demède, D.; Bouty, A.; Lanteri, P.; Mure, P.Y. Early detection of ureteropelvic junction obstruction in neonates with prenatal diagnosis of renal pelvis dilatation using 1H NMR urinary metabolomics. Sci. Rep. 2022, 12, 13406. [Google Scholar] [CrossRef] [PubMed]

| References | Type of Markers | Pathway | Main Markers | Main Findings | Method | Population |
|---|---|---|---|---|---|---|
| [34] | Markers of rapid decline in DKD | Not annotated to the pathway in the original work | 1-methyl pyridine-1-ium (NMP), retinol-1, trigonelline, threonic acid, ethanolamine, choline, 4-(trimethylammonio) but-2-enoate (CE-C-0218) | Non-targeted metabolomics and comprehensive machine learning analysis allowed us to reveal important features in DKD progression prediction. | CE-TOF–MS, LC-TOF–MS | Group 1 (n = 46) eGFR change rate was above 0%; group 2 (n = 34) below 0% and above −3.3%; group 3 (n = 39) below −3.3% and above −10%; group 4 (n = 14) <10% (rapid decliner) |
| [39] | DKD progression prospectively for a median of 8 (range: 2–10) years | TCA | Citric acid, aconitic acid | Obtained an extended panel of progression markers correlated with previous studies. Metabolites of TCA and BCAA catabolism are linked to the deterioration of mitochondrial functions and angiogenesis or insulin resistance and ketoacidosis. | FI-MS (Q-TOF) | 1001 Chronic Renal Insufficiency Cohort (CRIC) participants with diabetes |
| Catabolic intermediate of branched-chain amino acid (BCAA) | 3-hydroxyisobutyrate (3-HIBA), tiglylglycine | |||||
| Not annotated to the pathway in the original work | Uracil, glycolic acid, 3-methyladipic acid, homovanillic acid, aconitic acid, 3-hydroxypropionate, 2-methylacetoacetate, 2-ethyl-3-hydroxypropionate | |||||
| [43] | Metabolomic profiles and markers of progression | Not annotated to the pathway in the original work | C10:3, acyl-carnitine | The study found that higher levels of tryptophan were associated with higher end-stage kidney disease (ESKD) risk in both untargeted and targeted analyses, and the tryptophan pathway was significantly enriched in a set of ESKD-related metabolites. | FI-Q-TOF-MS (untargeted), CE-MS (target) | 995 randomly selected CRIC participants with diabetes across CKD |
| Amino acid metabolism | Tryptophan, valine, asparaginyl-hydroxyproline, arginyl glutamine | |||||
| Food or drug derivatives | 3-(4-methyl-3-pentenyl) thiophene | |||||
| [40] | Albuminuria DKD (ADKD) difference from normoalbuminuric DKD (NADKD) | TCA cycle | L-malic acid ꜜ | Metabolites related to the linoleic acid metabolism, citrate cycle, and arginine and proline metabolism allowed differentiating the ADKD group from the SDM and NADKD groups but not between the SDM and NADKD groups. | UPLC–MS/MS | SDM group (UACR < 30 mg/g and eGFR ≥ 90 mL/min/1.73 m2, n = 30); ADKD (30 ≤ UACR < 300 mg/g and eGFR ≥ 45 mL/min/1.73 m2, n = 30); NADKD (DKD patients with UACR < 30 mg/g and 45 ≤ eGFR < 90 mL/min/1.73 m2, n = 35) |
| Arginine and proline metabolism | L-proline ꜜ, L-erythro-4-hydroxyglutamate ꜜ, spermidine ꜜ | |||||
| Linoleic acid metabolism | Linoleic acid ꜛ, γ-linolenic acid ꜛ | |||||
| Albuminuria DKD (ADKD) difference from simple diabetes mellitus group (SDM) | TCA cycle | Succinic acid ꜜ, cis-aconitic acid ꜜ, citric acid ꜜ | ||||
| Arginine and proline metabolism | L-proline ꜜ, L-erythro-4-hydroxyglutamate ꜜ, N-methylhydantoin ꜜ, N-carbamoyl putrescine ꜜ, spermidine ꜜ, 5-aminopentanoic acid ꜜ | |||||
| Linoleic acid metabolism | γ-linolenic acid ꜛ | |||||
| [29] | DM2-CKD mild | Not annotated to the pathway in the original work | Alanine ꜛ, 2-hydroxybutyrate ꜛ | The groups of metabolites were significantly different in patients with mild, moderate, and severe CKD. An increase in trigonelline in DM2 patients due to creatinine depletion was found for the first time. 2-hydroxybutyrate urinary consent correlated with the body mass index. | 1D NOESY 1H -NMR | Control (n = 17), DM2 (n = 6), DM2-CKD mild (n = 13), DM2-CKD moderate (n = 10), DM2-CKD severe (n = 14) |
| DM2-CKD mild | Glyoxylate, dicarboxylate metabolism | Citrate ꜛ | ||||
| DM2-CKD moderate | Amino acid metabolism | Hippurate ꜛ | ||||
| DM2-CKD severe | Glycolysis and gluconeogenesis, pyruvate metabolism | Lactate ꜛ | ||||
| DM2-CKD severe | Glyoxylate and dicarboxylate metabolism | Glycolate ꜜ | ||||
| DM2-CKD moderate and severe | Amino acid metabolism and biosynthesis | Phenylalanine ꜛ | ||||
| DM2-CKD moderate and severe | Not annotated to the pathway in the original work | Trigonelline ꜛ | ||||
| [76] | Markers of DKD | Monosaccharide and TCA cycle | Citrate, mannose ꜛ | Based on our multidisciplinary analysis, urinary myo-inositol concentration can increase predictive power when used in combination with serum creatinine and UPCR in ESRD progression. | Targeted NMR | Patients with DKD stages 1–5 (n = 208) and healthy controls (n = 26) |
| Not annotated to the pathway in the original work | Myo-inositol ꜛ, choline | |||||
| [80] | Markers of DKD | Amino acid metabolism | Arginine ꜛ, citrulline ꜛ, ornithine ꜛ | Acylcarnitines are more sensitive markers of early diabetic kidney failure in type 2 diabetes in patients with normoalbuminuria and microalbuminuria than Hb1Ac. They interact with NF-Kβ, initiating inflammation and insulin resistance. | Targeted GC/MS | 232 patients with type 2 diabetes mellitus and 150 healthy controls |
| Alcylcarnitines | Dodecanoylcarnitines C12, triglylcarnitine C5:1, isovalerylcarnitine C5 | |||||
| [81] | Markers related to Immunoglobulin A nephropathy progression | Aminoacyl-transfer RNA biosynthesis | Glutamine Valine Leucine Tyrosine | The prediction of IgAN progression improved significantly when proteinuria was combined with serum glycerol/threonine or urine leucine-valine. | NMR | Non-progressors, progressors, healthy control (n = 10 for each group) |
| Valine, leucine, and isoleucine biosynthesis | Leucine, valine ꜛ | |||||
| TCA cycle intermediates | D-glucose ꜛ, sucrose ꜛ, gluconic acid ꜛ, l-xylonate-2, oxalic acid | |||||
| [82] | Markers of early DKD stages | Not annotated to the pathway in the original work | o-phosphothreonine, aspartic acid, 5-hydroxy lysine, uric acid, methoxytryptophan | The discovery of these candidate biomarkers implies their contribution to early DKD and 2DM advancement. This is because, even in the early stages of DKD, it can indicate kidney damage at specific sites along the nephron. | UPLC-QTOF-ESI* MS | 90 patients with type 2 DM, classified into three subgroups according to albuminuria stage from P1 to P3 (30 normo-, 30 micro-, and 30 macroalbuminuric) and 20 healthy controls |
| [83] | Markers related to early immunoglobulin A nephropathy | Amino acid metabolism | Glycine ꜛ | A high glycine concentration could potentially ameliorate the inflammatory damage induced by TNF-alpha. The activation of the tubules in IgAN due to glomerulotubular communication could be addressed by glycine. Physiological changes in renal tubular metabolism could increase glycine levels. IgAN patients have a significant reduction in protein H, which forms the glycine cleavage system, but without reduced eGFR. | NMR | Membranous nephropathy (MN) patients (n = 81), minimal change disease (MCD) (n = 49), lupus nephritis (LN) (n = 38) patients, and healthy controls (n = 146) |
| [46] | Markers of DKD’s fast decline | Phospholipid metabolism | Lysophosphatidylcholine ꜛ (16:0 and 18:0) | The accumulation of these compounds results from impaired lipid metabolism and leads to oxidative stress of organelles and apoptosis through the PPARd-PLIN2 pathway. | MS | 150 patients with stage G3 DKD |
| [18] | Risk prediction of CKD progression in individuals with type 2 diabetes mellitus (T2DM) | TCA | Lactate ꜛ, malate ꜛ, fumarate ꜛ, citrate ꜜ | Oxidative stress in CKD progression is connected with fumarate production. Fumarate and malate could be predictors of CKD progression independent of traditional cardio-renal risk factors. | GC-MS (selected ion monitoring) | Discovery study: progressors (n = 116), non-progressors (n = 271); validation study: progressors (n = 96), non-progressors (n = 402) |
| References | Type of Markers | Pathway | Main Markers | Main Findings | Method | Population |
|---|---|---|---|---|---|---|
| [35] | AKI diagnostic markers | Metabolism of xenobiotics by cytochrome P450 | 2-S-glutathionyl acetate | Characteristic AKI metabolomic markers were mainly related to xenobiotic, taurine, and hypotaurine metabolism. | UPLC–MS (Q/TOF) | AKI (n = 30) and healthy controls (n = 20) |
| Taurine and hypotaurine metabolism | 5-l-glutamyl-taurine | |||||
| Metabolism of xenobiotics by arginine and proline metabolism | l-phosphoarginine | |||||
| [37] | AKI after invasive surgery. Model 1 | Not annotated to the pathway in the original work | Ethanolamine ꜜ, glutamine ꜜ, glycine ꜜ, 2-hydroxypentanoate, serine, succinate | The study identified AKI-specific metabolites and time points, which may lead to improved biomarker development. | CE-TOF-MS | Non-AKI: 23, mild AKI: 24, severe AKI: 14 were measured, followed by the measurement of urine samples from 60 additional patients (non-AKI: 40, mild AKI: 20) |
| AKI after invasive surgery. Model 2 | Glycine ꜜ, urea, urate, ethanolamine ꜜ, glutamine, N, N-dimethylglycine | |||||
| AKI after invasive surgery. Model 3 | Piperidine, taurine, methanesulfonate, 3-hydroxykynurenine |
| References | Type of Markers | Pathway | Main Markers | Main Findings | Method | Population |
|---|---|---|---|---|---|---|
| [66] | Metabolites overlapped between the pre-AKI and AKI panels | Amino acid metabolism | Taurine, glutamine, methionine, aspartic acid, histidine, kynurenine ꜛ | Inflammation of renal cells leads to disruption of membrane integrity and tubule apoptosis in AKI, activation of compensatory functions, and loss of maintaining an osmotic balance. Renoprotective biomarkers are clusterin and cystatin C. Impaired renal function also affects kidney blood flow and vascular endothelial function. | GC-MS, direct flow injection MS (DI-MS) | Pre-AKI (n = 15), AKI (n = 22), and respective controls (n = 30) |
| Amino acid metabolism, catecholamine metabolism | Homovanillic acid | |||||
| Components of the lipid bilayer | Phosphatidylcholine (PC.aa.C34.1), sphingolipid (SM.C16.0) | |||||
| Pre-AKI | Not annotated to the pathway in the original work | Acylcarnitines (C5.DC.C6.OH., C2,C7.DC,C9,C3.DC.C4.OH.), phosphatidylcholine (PC.aa.C36.1) | ||||
| Not annotated to the pathway in the original work | Acetylornithine, serotonin, arginine, methylmalonic acid | |||||
| [38] | Acute kidney injury 24 h after the diagnosis of sepsis | Amino acid metabolism | Histidine | An effective diagnostic panel of markers for SA-AKI was demonstrated. Glycerophospholipid metabolism is related to the pathophysiology of septic AKI. | UPLC HILIC -QTOF/MS, Triple TOF | Septic children with AKI (n = 27) and septic children without AKI (n = 30) |
| Tyrosine metabolism, ascorbate and aldarate metabolism | Gentisaldehyde, 3-ureidopropionate, N4-acetylcytidine, and 3-methoxy-4-hydroxyphenylglycol sulfate | |||||
| Acute kidney injury 12 h ALL after the diagnosis of sepsis | N-galactose metabolism, fructose and mannose metabolism, glyoxylate and dicarboxylate metabolism, β -alanine metabolism, and glycerophospholipid metabolism | L-histidine, DL-indole-3-lactic ac id, trimethylamine N-oxide, and caprylic acid | ||||
| TCA compensation | L-glutamine | |||||
| [67] | Biomarkers for ureteropelvic junction obstruction (UPJO) | Amino acid metabolism | Alanine ꜜ, arginine ꜜ, lysine ꜜ, threonine ꜜ, N,N-dimethylaniline ꜜ, taurine ꜜ, ornithine ꜜ | Found diagnostic biomarkers of UPJO and an early-stage transient dilatation demonstrated promising results and allowed differentiating all groups. | 1H-NMR | Newborns with prenatally diagnosed RPD (n = 50), healthy newborn controls (n = 90) |
| Betaine metabolism | Betaine ꜜ | |||||
| Not annotated to the pathway in the original work | Creatine ꜜ, threitol ꜜ, glucoronate ꜜ | |||||
| [30] | Differentiating metabolites of established AKI patients, healthy and hospitalized patients without AKI | Amino acid metabolism | Leucine ꜛ, valine ꜛ | The decrease in the concentration of TCAs suggests that the observed effect originates from tubular cell membrane dysfunction connected with the transcellular transport of dicarbonic acids. | 1H-NMR | 65 neonatal and pediatric patients with established AKI of heterogeneous etiology; healthy children (n = 53); group of critically ill children without AKI (n = 31) |
| TCA cycle | Citrate ꜜ | |||||
| Not annotated to the pathway in the original work | Bile acid ꜛ | |||||
| [19] | Metabolic signature of renal dysplasia, unrelated to eGFR value | Amino acid metabolism | Indoxyl sulfate ꜜ, glutamine ꜜ, glyceric acid ꜛ | The authors suggested that decreased acylcarnitine concentrations could indirectly indicate impaired mitochondrial function. This may also cause abnormalities in oxidative phosphorylation and fatty acid oxidation. These findings are consistent with cellular processes characteristic of CKD, such as ATP depletion, apoptosis, cell dedifferentiation, and intracellular lipid deposition. | GC-MS (GC-QQQ/MS), LC-TOF-MS (RP; HILIC) | 72 children: renal dysplasia (n = 39, mean age of 5.68 years (range: 0.08–17.40)) and healthy controls (n = 33, mean age of 7.28 years (range: 0.09–17.69)) |
| Purine metabolism | Xanthine ꜜ | |||||
| Fatty acid metabolism and biosynthesis | Acylcarnitines, hexadecanoic acid ꜛ | |||||
| TCA | Aconitate ꜜ | |||||
| Carbohydrates metabolism and biosynthesis | Arabitol ꜛ, lactose ꜛ, lactic acid ꜛ | |||||
| Microbial metabolism | Furoic acid ꜛ | |||||
| Ascorbate and aldarate metabolism | Threonic acid ꜛ | |||||
| tRNA degradation | Dimethylguanosine ꜛ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danilova, E.Y.; Maslova, A.O.; Stavrianidi, A.N.; Nosyrev, A.E.; Maltseva, L.D.; Morozova, O.L. CKD Urine Metabolomics: Modern Concepts and Approaches. Pathophysiology 2023, 30, 443-466. https://doi.org/10.3390/pathophysiology30040033
Danilova EY, Maslova AO, Stavrianidi AN, Nosyrev AE, Maltseva LD, Morozova OL. CKD Urine Metabolomics: Modern Concepts and Approaches. Pathophysiology. 2023; 30(4):443-466. https://doi.org/10.3390/pathophysiology30040033
Chicago/Turabian StyleDanilova, Elena Y., Anna O. Maslova, Andrey N. Stavrianidi, Alexander E. Nosyrev, Larisa D. Maltseva, and Olga L. Morozova. 2023. "CKD Urine Metabolomics: Modern Concepts and Approaches" Pathophysiology 30, no. 4: 443-466. https://doi.org/10.3390/pathophysiology30040033
APA StyleDanilova, E. Y., Maslova, A. O., Stavrianidi, A. N., Nosyrev, A. E., Maltseva, L. D., & Morozova, O. L. (2023). CKD Urine Metabolomics: Modern Concepts and Approaches. Pathophysiology, 30(4), 443-466. https://doi.org/10.3390/pathophysiology30040033